
Abstract
Exposure to intimate partner violence (IPV) is a common feature of women living in low- and middle-income countries. Several studies have shown a significant association between IPV against women and mental health in both developed and in low- and middle-income countries. In postconflict settings, the relationship between IPV and mental health is likely more complex, given the high levels of violence experienced by the population as a whole. In this cross-sectional study the authors explore the association between IPV and common mental health disorders (CMD), and more specifically, suicidal ideation, among inhabitants of postgenocide Rwanda. The authors use the concept of “mutual partner violence,” thereby exploring the association between IPV and CMD in victims, perpetrators, and those who state they are both. Data of 241 married men and women were used. Symptoms suggestive of CMD were established by use of the Self-Reporting Questionnaire (SRQ-20), and physical intimate partner violence was measured using the Conflict Tactics Scale, Short Version (CTS2S). The authors applied multivariate logistic regressions with total SRQ-20 scores (above/below cutoff) and suicidal ideation as the outcome measures and corrected for age and gender. The study findings suggest that reported IPV is associated with CMD (odds ratio [OR] = 1.7, 95% confidence interval [95% CI] = 0.92-3.15) and suicidal ideation (OR = 1.6, 95% CI = 0.70-3.53). Those who state to be both victim and perpetrator (OR = 1.75, 95% CI = 0.82-3.72), or only perpetrator (OR = 3.13, 95% CI = 0.49-20.0), are more likely to report mental health problems than victims and people who do not report IPV. In a postconflict situation, perpetrators of IPV may suffer from mental health problems as much as, or even more than, victims. Longitudinal data are needed to clarify the complex relationship between CMD and IPV, especially if outcomes may also be related to other forms of violence experienced in the past.
Introduction
Intimate partner violence (IPV) refers to any behaviour within an intimate relationship that causes physical, psychological, or sexual harm to those in the relationship. Such behaviour includes acts of physical aggression, such as slapping, kicking, and beating; psychological abuse, such as intimidation and humiliation; and forced intercourse and other forms of sexual coercion (WHO’s World Report on Violence and Health, 2002). The WHO studied the prevalences of IPV in women in 10 high-, middle-, and low-income countries (Garcia-Moreno et al., 2006). Fifteen percent to 71% reported having been a victim of partner violence at least once in their life. Between 4% and 54% of these women reported partner violence in the preceding year. The prevalence of IPV appeared to be especially high in low-income countries. A cross-sectional study in four low-income countries found lifetime prevalence rates of physical IPV of 24.9% in Chile, 11.1% in Egypt, 21.1% in the Philippines, and up to 43.1% in Indian cities (Jeyaseelan et al., 2004). The same study found proportions of women reporting being victims of psychological IPV ranging from 10.5% to 50.7% (Ramiro, Hassan, & Peedicayil, 2004).
In a review of studies in low- and middle-income countries, Ribeiro and colleagues demonstrated that exposure to partner violence is consistently associated with mental disorders (Ribeiro, Andreoli, Ferri, Prince, & Mari, 2009). A study in India showed that women who reported physically violent behavior by their spouse were at increased risk of poor mental health (Kumar, Jeyaseelan, Suresh, & Ahuja, 2005). In Paraguay, Ishida et al. found that IPV is independently associated with an increased risk of common mental health disorders (CMD) and suicidal ideation (Ishida, Stupp, Melian, Serbanescu, & Goodwin, 2010). In Ethiopia, physical violence, emotional violence, and high spousal control of women by their partners were independently associated with depressive episodes, after adjusting for socioeconomic factors (Deyessa et al., 2009).
In these studies, little attention has been paid to the mental health status of the perpetrators, who are mostly men. They are likely to have an increased risk of mental health problems as well, especially in light of studies that suggest that a considerable proportion of IPV is mutual, when both partners report committing violence. For this the term “mutual intimate partner violence” has been introduced. A study of mutual partner violence in 767 residents of the United States from four racial and ethnic groups suggested that 35% of victims of IPV also reported perpetration of violence against their partner (Próspero & Ki, 2009). Mental health problems have been associated with IPV perpetration (often called battering) in a number of cross-sectional studies, including depressive symptomatology, anxiety, hostility, borderline personality disorder, antisocial personality disorder, psychotic experiences, posttraumatic stress disorder (PTSD), suicidality, and impulsive behaviors including violence (Lipsky, Caetano, & Roy-Byrne, 2011). Men disclosing both victimization and perpetration seemed to have the highest frequency and severity of adverse mental health symptoms (Próspero & Ki, 2009; Rhodes et al., 2009).
It is generally known that mental health symptoms or disorders are highly prevalent in postconflict settings (De Jong, Komproe, & Van Ommeren, 2003; Steel et al., 2009). This may relate to a variety of factors, including war-related trauma, poverty, drug abuse, ongoing political turbulence, and the impact of HIV/AIDS.
To date, few studies have investigated the association between IPV and mental health in a postconflict setting. In Lebanon, women’s self-reported mental ill health scores were positively correlated with both domestic violence and the violence associated with the conflict during and after the conflict (Usta, Farver, & Zein, 2008). Refugees from Darfur show symptoms of depression and trauma, as well as elevated levels of both domestic violence and community conflict, relative to pregenocide measurements (Meffert & Marmar, 2009). In specific territories of Eastern Democratic Republic of Congo, self-reported sexual violence was associated with physical and mental health outcomes (Johnson et al., 2010). These studies, however, do not report on mental health problems among perpetrators, while a higher risk of mental health problems likely applies to both victims and perpetrators of IPV, who all have been exposed to collective violence (De Jong et al., 2003; Steel et al., 2009).
This article explores the mental health status of victims as well as perpetrators of IPV in a postconflict setting. More specifically, we focus on Rwanda, where the prevalence of IPV is high. The Rwandan 2005 Demographic and Health Survey (DHS; Institut National de la Statistique du Rwanda [INSR] & ORC Macro, 2006) reported a national prevalence of IPV among 30% of women. Thirty-seven percent of married or cohabiting women have experienced physical violence since age 15, and 26% experienced it in the 12 months preceding the survey (Rwanda Demographic and Health Survey, 2005). Three studies on IPV in Rwanda considered the prevalence and determinants (not CMD) of IPV against pregnant women (Ntaganira, Muula, Siziya, Stoskopf, & Rudatsikira, 2008), factors associated with IPV among these pregnant women (alcohol use by partners and level of education for women; Ntaganira et al., 2009), and the association between IPV and HIV and other sexually transmitted diseases (Dude, 2011). No information is known about IPV against men or about perpetrators of IPV (batterers) in Rwanda, or their association with mental health problems.
We explored the association between IPV and the risk of CMD, more specifically suicidal ideation, among inhabitants of Byumba (Gicumbi), a northern province of Rwanda, where people are still suffering from the consequences of systematic violence. We used the concept of “mutual partner violence” to explore the association between IPV and CMD in victims, perpetrators, and those who state they are both. We hypothesized that both victims and perpetrators of IPV show an increased risk of CMD.
The work described in this article was part of a larger study to determine the effect of a community-based therapeutic group approach called sociotherapy in Rwanda. (Richters, Dekker, & Scholte, 2008; Scholte, Verduin, Kamperman et al., 2011).
The baseline measurement of this study took place in October 2007. Approval was gained from the Medical Ethics Committee of the Academic Medical Center in Amsterdam (Trial Registration: Nederlands Trial Register NTR1120).
Method
For this cross-sectional study, data of 241 men and women were used. These people were all married participants of the larger quasi-experimental study at baseline (October 2007; Richters et al., 2008; Scholte, Verduin, Kamperman et al., 2011). The husbands and wives of these participants were not necessarily included in the study, but each interviewee reported on victimization and perpetration within their marriage. Participants were all inhabitants of Byumba province in Rwanda. They were part of either the experimental or control group for the quasi-experimental study on sociotherapy. For participation in a sociotherapy group, no inclusion criteria were applied; the program was open to any adult (≥16 years) willing to participate.
Instruments
Sociodemographics of each participant were documented: gender, age, level of education, profession, and socioeconomic status (SES). Two instruments were administered: the Self-Reporting Questionnaire 20 items (SRQ-20) and the Revised Conflict Tactics Scale, Short version (CTS2S).
Self-Reporting Questionnaire—20 Items (SRQ-20)
The SRQ-20 was developed by the World Health Organization (WHO) in the 1980s as a screening tool for common mental disorders (CMD) in primary care settings. When patients are literate it can be self-administered, but in developing countries it is often administered by lay interviewers. It consists of 20 yes/no questions about mood, thinking capacity, feelings of anxiety and physical well-being. “Yes” answers result in a higher score, indicating a poorer mental health condition. Cutoff points vary considerably depending on setting and culture. A cutoff point of 7/8 is widely used (Harpham et al., 2003).
We back-translated the WHO version of SRQ-20 to the local language, Kinyarwanda, and validated it for the local context in a pilot study. The capacity of the Kinyarwanda version of the SRQ-20 to identify probable psychopathology proved to be sufficient for men (AUC = 0.74) and women (AUC = 0.76). Its reliability was considered to be good (α = .83). In this validation study, cutoff scores for women and men were ≥10 and ≥8, respectively (Scholte, Verduin, Van Lammeren, Rutayisire, & Kamperman, 2011). We used the validated, Kinyarwanda SRQ-20 for the present study.
In addition to participants’ CMD risk, we considered their suicidal ideation, captured by a single question in the SRQ-20 (Question 17): “Has the thought of ending your life been on your mind?” While SRQ-20 is intended to capture poor general mental health status across multiple dimensions, suicidal ideation alone captures a potentially severe and distinct mental health problem and indicates risk for actual self-harm. For this study, the SRQ-20 offered two outcome variables: a total score above or below cut-off, and the occurrence of suicidal ideation.
Revised Conflict Tactics Scale, Short Version (CTS2S)
We assessed the presence of IPV with the Revised Conflict Tactics Scale, Short form (CTS2S). The revised Conflict Tactics Scale (CTS) was developed in 1979 and is the most widely used instrument for measuring IPV (Straus, 2004). The instrument includes three scales to measure tactics used when there is a conflict in a relationship: Negotiation, Physical Assault, and Psychological Aggression. In addition, there are two supplemental scales: Injury from Assault and Sexual Coercion. We made use of the short version, the CTS2S, that can be administered in 3 minutes. The validity of the CTS2S is comparable to the CTS2 (Straus, 2004). The CTS2S consists of 10 items, each of which is first asked concerning the behavior of the respondent and then repeated for the behavior of the respondent’s partner. This permits classifying couples into three mutuality types, despite only one partner responding. For example, according to the Physical Assault scale, the three mutuality types are 1 = male partner only, 2 = female partner only, 3 = both. For this study, the CTS2S was not validated locally but adapted to the context in three ways. First, we omitted the questions about sexual violence because we thought it would be inappropriate to ask such questions in this particular setting—relatively short interviews by lay interviewers in a culture where sexuality is considered a very private matter.
Second, we changed the Likert scale of the CTS2S. In its original form it consists of eight possible options. We narrowed it down to three options, to make it more understandable for our respondents and interviewers (see Appendix 1). Third, the CTS2S asks about conflicts that happened in the past year. As our version of the CTS2S was used in a longitudinal design, with more than one measurement in one year, we asked about conflicts that occurred over the past 3 months.
For this study all participants were divided into four categories: only victim, victim and perpetrator, only perpetrator, and no partner violence. Respondents were considered victims if they scored more than zero on questions 5, 10, 12, 14, and 15 and were considered perpetrators if they scored more than zero on questions 6, 9, 11, 13, and 16 (see Appendix 1). With this in mind, we present IPV as physical violence.
Interviews
The questionnaires were administered by trained interviewers. Eight local interviewers were recruited; all were sociology students at the “Institut Polytechnique de Byumba” in Gicumbi. Their 1-week training addressed the principles of the study design, interviewing techniques, and measuring instruments. They were involved in making the wording of the questions acceptable and understandable for people in Byumba (Gicumbi; Verduin, Scholte, Rutayisire, & Richters, 2010). Informed consent was obtained by use of an explanatory text, which was read aloud because of the high rate of illiteracy. In case of refusal, demographic data and reasons for refusal would be requested and documented, but no one refused.
For determination of SES (socioeconomic status) our interviewers approached respondents of the control group at or near their homes and scored respondents’ SES by judging the state of the houses. Participants of the experimental group, however, were interviewed at the spot of their meetings and were asked to describe the state of their houses themselves.
Statistical Analysis
For all analyses, we used SPSS (Version 18). First, we described the prevalence of IPV and risk of CMD. Subsequently, we presented bivariate associations between IPV and the two indicators of mental health —CMD risk and suicidal ideation—with odds ratios. We distinguished three groups within the research population: participants who reported victimization only, participants who reported both victimization and perpetration, and those who reported only perpetration of IPV.
Last, we applied multivariate logistic regressions with total SRQ-20 scores (above/below cutoff) and suicidal ideation as the outcome measures and corrected for estimated confounders (age and gender).
Results
Sociodemographics
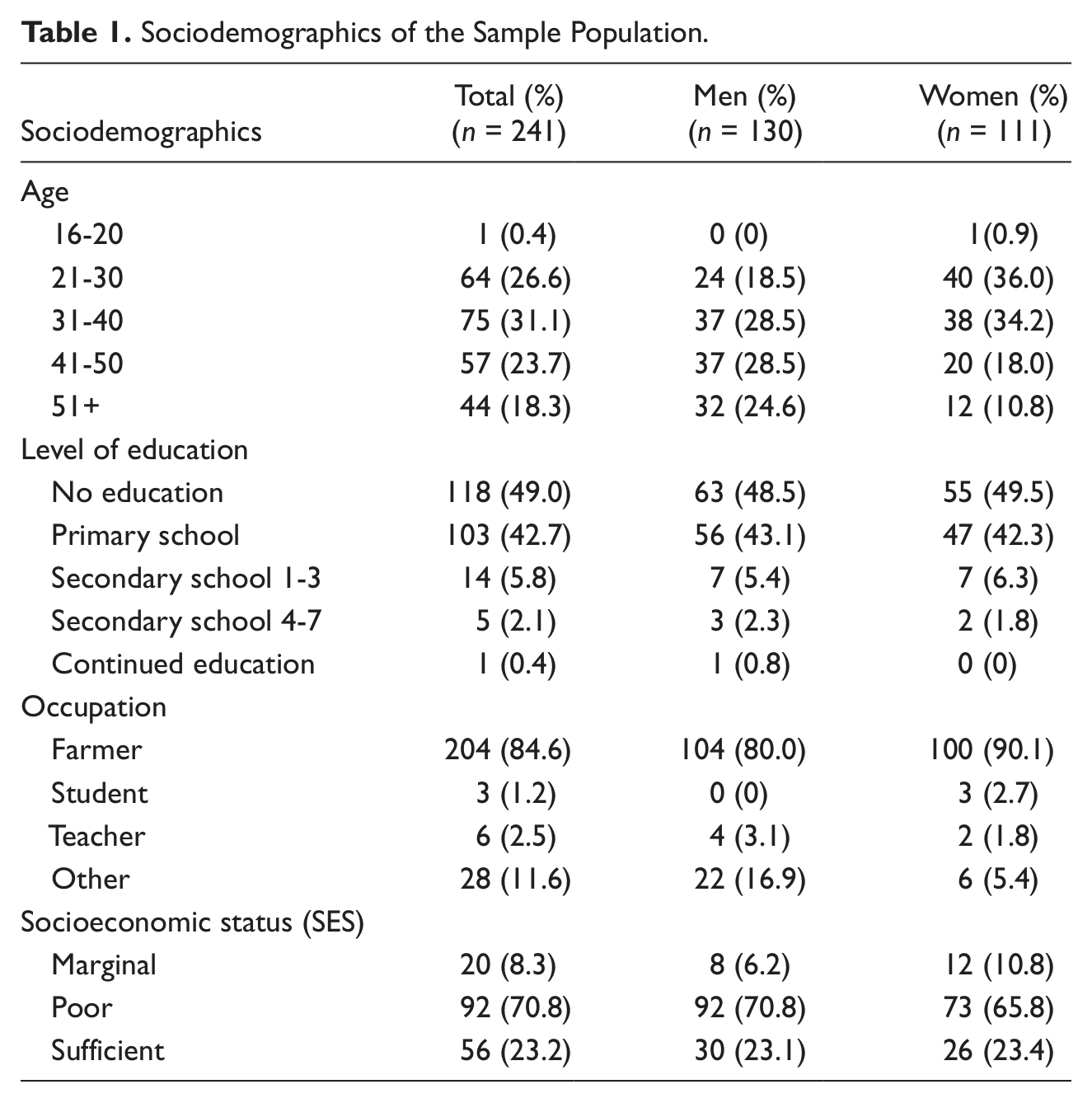
Table 1 shows that the average age of our research population was 40.2 (SD ± 12.7). Almost half of the participants had no formal education and 42.7% had primary school education only. The majority of the participants were farmers (agriculturalists; 84.6%) and their SES was low (71%).
Sociodemographics of the Sample Population.
Mental Health (CMD)
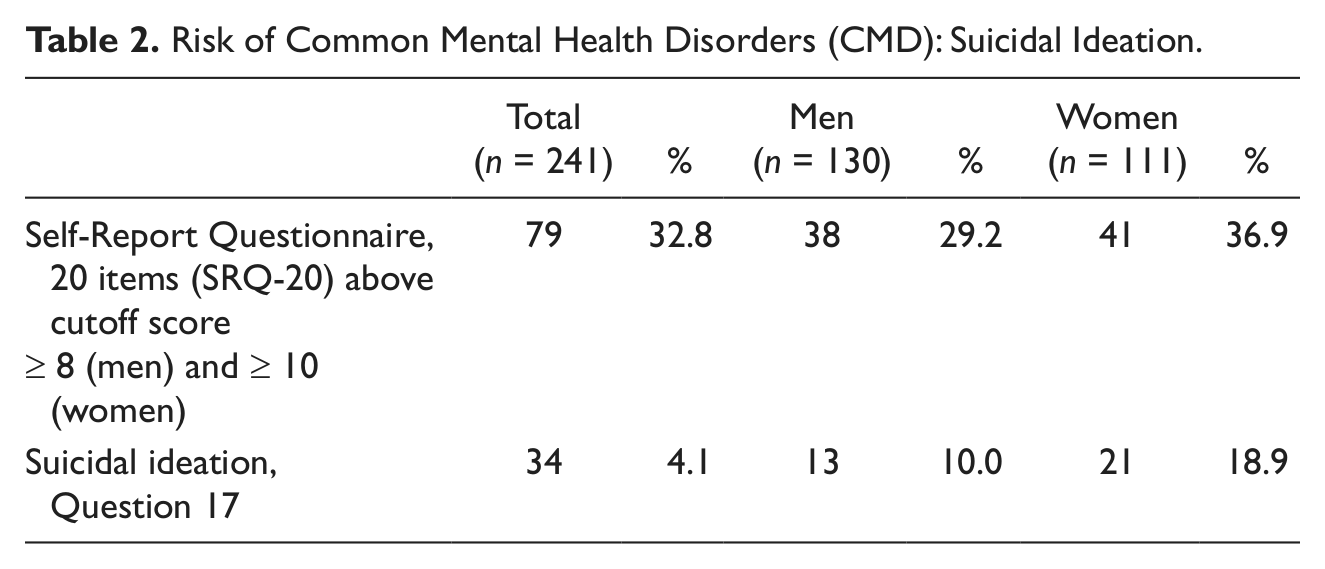
Thirty-three percent of participants scored above cutoff on the SRQ-20 and so were considered at risk of CMD (see Table 2). More women than men scored above cutoff (37% vs. 29%). Of the women, 19.8% reported suicidal ideation, compared to 10% of men.
Risk of Common Mental Health Disorders (CMD): Suicidal Ideation.
Intimate Partner Violence
Twenty-five percent of the study population reported involvement in IPV in the preceding 3 months (see Table 3). Seventeen percent of men and 29.7% of women indicated they were victims of IPV in the past 3 months. The majority of women who reported IPV indicated they were only victim, but 12.6% reported victimization and perpetration. No women indicated perpetration only. Fifteen percent of men said they were both victims and perpetrators. Five men (3.8%) reported perpetration only, and two men (1.5%) reported being a victim of IPV without perpetrating.
Prevalence Intimate Partner Violence.

Intimate Partner Violence and Mental Health
Table 4 shows the association between IPV and risk of CMD, as well as the association between IPV and suicidal ideation, as assessed by logistic regression models.
Percentage Risk for Common Mental Health Disorders (CMD), Percentage Suicidal Ideation, Odds Ratio (OR), Corrected OR, and 95% Confidence Intervals (95 % CI; Corrected for Gender and Age).
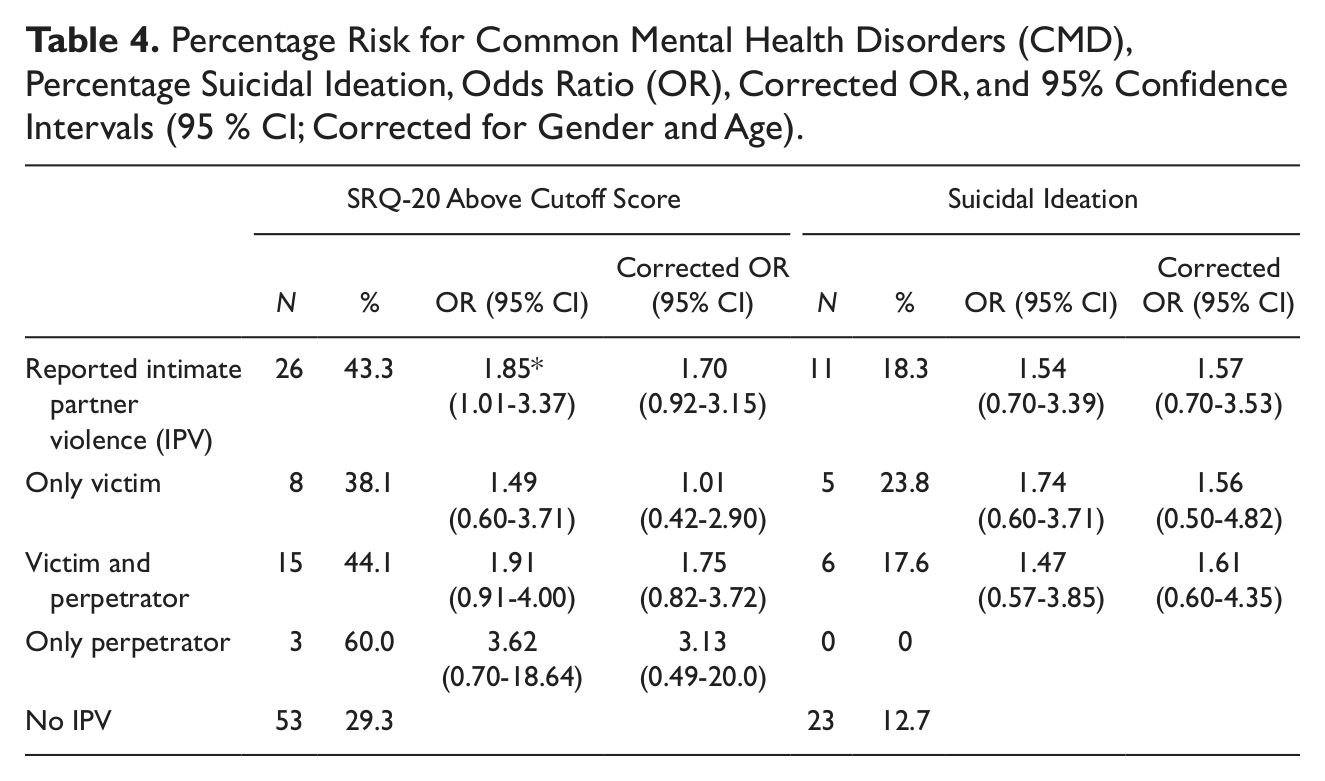
Reporting IPV is associated with CMD (odds ratio [OR] = 1.85, p < .05, 95% confidence interval [CI] = 1.01-3.37; corrected OR = 1.7, 95% CI = 0.92-3.15) and suicidal ideation (corrected OR= 1.6, 95% CI= 0.70-3.53). For those who state to be only victims of IPV, we find no association with CMD (corrected OR = 1.01, 95% CI = 0.42-2.90). Those who state to be victim and perpetrator (corrected OR = 1.75, 95% CI = 0.82-3.72) or only perpetrator (corrected or = 3.13, 95% CI = 0.49-20.0) are more likely to have mental health problems, especially more than people who do not report IPV. However, none of our corrected associations are significant.
Discussion
This explorative study indicates that reporting IPV may be associated with CMD and suicidal ideation in a postconflict area such as Rwanda. Those who state to be either perpetrator or both victim and perpetrator report more mental health problems than victims and more than people who do not report IPV. Although our study sample is small and we cannot provide strong evidence, our findings suggest that IPV may be associated with adverse mental health outcomes for both victims and perpetrators in a postconflict area. The causal direction of this association, however, remains unclear.
Most existing studies concerning the association between IPV and mental health do not explicitly address the issue of the direction of this association. If any, the assumption seems to have been made that IPV preceded a decline in mental health. Several studies, most from developed countries, have shown a significant association between IPV against women and women’s mental health (Campbell, 2002; Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Escribà-Agüir et al., 2010; Ishida et al., 2010; Krug, Mercy, Dahlberg, & Zwi, 2002). A review in 2002 states that depression and PTSD, conditions that frequently coincide, are the most prevalent mental health sequelae of IPV (Krug et al., 2002). In the WHO’s multicountry study on women’s health and domestic violence, women who reported partner violence at least once in their life reported significantly more emotional distress, suicidal thoughts, and suicidal attempts than nonabused women (Ellsberg et al., 2008; Garcia-Moreno et al., 2006). In a recent study in Australia among a nationally representative sample of women, gender-based violence was significantly associated with adverse mental health effects such as anxiety, mood disorder, PTSD, and suicide attempts (Rees et al., 2011). A review by Marshall et al. showed that in veterans, PTSD is an important correlate that largely accounts for the relationship between combat exposure and IPV perpetration (Marshall, Panuzio, & Taft, 2005).
One may argue, however, that an association in the opposite direction is plausible as well. Poor mental health could be a risk factor for becoming involved in IPV, either as victim or perpetrator. A recent study examined partner aggression among male veterans from the United States who served in Afghanistan or Iraq and compared this aggression to that reported by Vietnam veterans with PTSD. Though only a few comparisons reached significance, odds ratios suggested that male Iraq and Afghanistan veterans with PTSD were 1.9 to 3.1 times more likely to perpetrate aggression toward their female partners than veterans without PTSD and Vietnam veterans with PTSD (Teten et al., 2009).
While the direction of the association between IPV and mental disorder has yet to be clarified, the relationship seems to be even more complex in postconflict settings, as both IPV and CMD are probably more prevalent after the previous experience of any form of violence. This includes trauma of recent genocide and war, the impact of HIV/AIDS, poverty, drug abuse, and ongoing political turbulence.
It has been suggested that collective violence raises the risk of IPV. In Palestine, Clark et al. have shown increased odds of IPV in a sample of married women whose husbands had been exposed to political violence (Clark et al., 2010). Findings from studies in civilian populations in Sri Lanka, Afghanistan, Lebanon, and the West Bank suggest that exposure to violent conflict is associated with IPV and other forms of domestic violence (Al-Krenawi, Graham, & Sehwail, 2007; Catani, Jacob, Schauer, Kohila, & Neuner, 2008; Catani et al., 2009; Catani, Schauer, & Neuner, 2008; Haj-Yahia & Abdo-Kaloti, 2003; Usta et al., 2008). A study conducted among internally displaced persons in postconflict Uganda produced estimates of IPV in the past year of 51.7% (Stark et al., 2010). Women’s narratives from a qualitative study in northern Uganda illustrate the multiple levels of violence that women may experience in war, including violence from an armed group, abuse from extended family members, and IPV (Annan & Brier, 2010).
For the population of postgenocide Rwanda, various studies have shown high rates of violence and traumas alongside high rates of mental health disorders (Bolton, Neugebauer, & Ndogoni, 2002; De Jong, Scholte, Koeter, & Hart, 2000; Neugebauer et al., 2009; Pham, Weinstein, & Longman, 2004; Schaal & Elbert, 2006). Here, the accumulated experiences of collective violence and IPV may have acted to raise the risk of CMD. In reverse order, Rwandans suffering from mental health problems, including PTSD, may be more inclined to perpetrate IPV because of their state of hyperarousal.
Culture-specific factors may affect the generalizability of our findings to other postconflict settings. The attitude of suspicion and distrust, which is common within the Rwandan community, may add to the complexity of the association between CMD and IPV in our study sample (Richters, Rutayisire, & Dekker, 2010). Distrust may affect intimate partner relationships and induce aggression. Another factor that has recently been acknowledged as one of the strongest predictors of IPV is an accepting attitude toward IPV. In a comparative analysis of data from 17 Sub-Saharan countries, Uthman et al. showed that IPV against women was widely accepted under certain circumstances (e.g., a woman goes out without telling her spouse, neglects her child, argues with her spouse) by men and women in all of the countries studied. Contrary to expectations, women were more likely to justify IPV than men. In Rwanda, almost 50% of women “accepted” wife-beating, compared to less than 40% of men (Uthman, Lawoko, & Moradi, 2009).
This study has several limitations. We could not differentiate types of partner violence. The short version of the Revised CTS does not yield information on emotional partner violence. We have clear information on physical violence only, as after adapting the instrument as described in the Methods section, sexual violence was left out completely. However, evidence from different studies shows that when women report physical violence, it can be expected that a large proportion of them have also experienced sexual violence. Lifetime prevalence data from a national general population survey, the National Violence Against Women Survey (NVAWS) conducted in the United States, show that if a woman is physically assaulted by a partner or spouse, she also faces an increased risk of being raped (Miller, 2006). Data from Rwanda (Rwanda Demographic and Health Survey, 2005) show that 29% of married women had been confronted with acts of physical violence on the part of their husband/partner. Twelve percent of married women had experienced acts of sexual violence.
A disadvantage of leaving out the questions on sexual violence and changing the Likert scale and the period from 12 to 3 months is that our findings are hard to compare with that of other studies.
The use of interviewers for the administration of the questionnaire enabled clarification of questions to respondents when needed. This, however, may have lead to social desirability bias. In our experience in Rwanda, questions on poor health and social problems proved difficult to answer, especially for men (Scholte, Verduin, Kamperman et al., 2011; Verduin et al., 2010). Using a structured questionnaire with closed questions and limited response options is not optimal to obtain reliable data on the prevalence of IPV, mental health problems, and more specifically, suicidal ideation. Instead, an interviewing style that allows for the establishment of trust and openness would be more suitable. This particularly applies if a study population generally tends to hide problems or vulnerabilities. Given the Rwandan context, the interviews held for our study may not have met this condition sufficiently. It is possible that we would have found a stronger association between IPV and mental health if this condition had been met, that is, if there would not have been a social desirability bias.
Conclusion
Although previous studies have supported the association between IPV and mental illness, the nature of this relationship has not yet been fully clarified. Mental health problems may act as a predictor for IPV and vice versa. In addition, this may apply to both victims and perpetrators of IPV. Here, longitudinal data are needed for further understanding, especially if outcomes may also be related to other forms of violence in respondents’ past. This study shows the relevance of a focus on IPV in future research and mental health interventions in postconflict settings. Both men and women, victims and perpetrators, their attitudes toward IPV and other possible culture-specific factors, as well as previous exposure to violence, should be considered.
Footnotes
Appendix 1
Acknowledgements
We thank Prof. J. M. Richters, of the division of Culture, Health and Illness of the LUMC in Leiden for her contributions in qualitative research, and C. Dekker, who trained and supervised all the sociotherapy group leaders. We thank Ngendahayo Emmanuel, Sarabwe Emmanuel, and Hategekimana Balthazar for helping us organize and conduct the research. We also thank our loyal interviewers: Rukundo Ange, Mugisha-Bitanuzire John-Peter, Umuhoza Adelin, Uwizeye Beata, Ingabire Bernadette, Uwizeyimana Albertine, Mukanyiligira Marie Grace, and Muhongwanseko Scholastique.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by a grant to Femke Verduin from the Health Research Development Counsel, Department Prevention Program (ZonMW), OOG-Geestkracht (ZonMW: 60-60105-98-117). We also thank Cordaid for funding the research in Rwanda and Prins Bernhard Cultuurfonds for their grant to F. Verduin.