
Abstract
Women who experience intimate partner violence (IPV) during pregnancy also tend to experience depressive symptoms. Unfortunately, little is known about how victimized women’s levels of depressive symptoms change longitudinally before pregnancy, during pregnancy, and after infant delivery. In addition, few studies have used a comparison group of women to determine if levels of depressive symptoms among victimized women differ from depressive symptom levels in women who have not experienced IPV. To help address these knowledge gaps, we examined longitudinal trends in levels of depressive symptoms among a sample of 76 women who did (n = 33) and did not (n = 43) experience physical IPV during pregnancy. Using multilevel analysis, we estimated the relationship of physical IPV victimization and women’s depressive symptom levels across six time periods: (a) the year before pregnancy, (b) first and second trimesters, (c) third trimester, (d) the first month postpartum, (e) Months 2 to 6 postpartum, and (f) Months 7 to 12 postpartum. Women who experienced physical IPV victimization during pregnancy had significantly higher levels of depressive symptoms during each time period (p < .05). No significant difference between the two groups was found in the rate of change in levels of depressive symptoms over time. These findings point to the importance of screening for IPV within health care settings and suggest that women physically abused during pregnancy need safety interventions that are coordinated with interventions targeting symptoms of depression.
Keywords
Intimate Partner Violence (IPV) and Depressive Symptoms Before, During and After Pregnancy
Pregnancy is often considered to be a dynamic, positive time in many women’s lives. For some women, pregnancy can also be a time for increased vulnerability for complications and other problems. Two such problems that can occur during women’s pregnancies include depressive symptoms and IPV. Research has extensively investigated the relationship between pregnancy and depressive symptoms. Likewise, considerable research has investigated pregnancy and IPV. However, less research has investigated the relationships among all three factors, particularly in a longitudinal way. To help address the limited research on the relationships among pregnancy, depressive symptoms, and IPV, we investigated changes in levels of depressive symptoms across women’s pregnancies and their postpartum periods by comparing women who had experienced physical IPV victimization during their pregnancies to women who had not experienced physical IPV victimization during their pregnancies. Before presenting our study hypotheses, we discuss the existing research on pregnancy, depressive symptoms, and IPV.
IPV
Approximately 1.5 million women in the United States are physically assaulted by their partners (Rennison & Welchans, 2000; Tjaden & Thoennes, 2000), and IPV often occurs during women’s reproductive years (Gelles, 1988; Tjaden & Thoennes, 2000). Women in abusive relationships are at risk for IPV during the pregnancy and the postpartum period (i.e., within 1 year after delivery; Jasinski, 2004). Some research has shown that IPV may be a more common health risk during women’s pregnancies than is preeclampsia or gestational diabetes (Gazmararian et al., 2000). A recent study by Daoud et al. (2012) found that, among a national sample of Canadian women for whom partner violence was the most prevalent type of abuse, the majority of women experienced abuse before pregnancy (8.2%) compared to during pregnancy (3.3%) and after birth (2.2%).
Nonetheless, estimates of IPV prevalence vary considerably across studies of pregnant women (Bacchus, Mezey, & Bewley, 2006; Gazmararian et al., 2000; Jasinski, 2004; Rosen, Seng, Tolman, & Mallinger, 2007; Martin et al., 2006; Murphy, Shei, Myhr, & DuMont, 2001; Sharps, Laughon, & Giangrande, 2007). Findings from prior studies may have varied because of different samples used (e.g., national probability sample versus hospital-based or clinic-based samples), different timings of IPV assessment, and different definitions of IPV (e.g., physical versus psychological abuse; Jasinski, 2004). Sharps et al.’s (2007) review of recent research estimated that 3.7% to 14.7% of women experienced IPV during pregnancy.
IPV during pregnancy is associated with health problems for both women and infants (Jasinski, 2004; O’Reilly, 2007; Sharps et al., 2007). The health problems associated with IPV during pregnancy include increased risk of preterm delivery, premature rupture of membranes, low-birth-weight infants, fetal trauma, and neonatal death (Jasinski, 2004; Rosen et al., 2007; Shah & Shah, 2010). Women who are abused during pregnancy are also more likely to struggle with a variety of mental health problems, including symptoms of antenatal and postpartum depression, stress, anxiety, and low self-esteem (Bacchus et al., 2006; Campbell, Poland, Waller, & Ager, 1992; Flynn & Chermack, 2008; Jasinski, 2004; Martin et al., 2006). These mental health problems often co-occur. However, most researchers who have investigated the relationship between IPV during pregnancy and maternal mental health have documented a significant positive relationship between IPV during pregnancy and depressive symptoms (e.g., Amaro, Fried, Cabral, & Zuckerman, 1990; Certain, Mueller, Jagodzinski, & Fleming, 2008; Martin et al., 2006; Rodriguez et al., 2008). For example, a study of obstetric patients found that women who reported abuse during pregnancy were 4.21 times more likely to screen positive for postpartum depression, compared to women who did not report abuse during pregnancy (Certain et al., 2008). In addition to poor mental health, research shows that abuse during pregnancy is an indicator of a potentially lethal intimate partner relationship (McFarlane, Campbell, Sharps, & Watson, 2002). McFarlane et al. (2002) found a significant relationship between abuse during pregnancy and attempted or completed femicide.
Depression
As mentioned above, a common, serious mental health problem that pregnant and postpartum women are likely to experience is depression (Evans, Heron, Francomb, Oke, & Golding, 2001; Gaynes et al., 2005). Prevalence estimates from meta-analyses conducted by Gavin et al. (2005) revealed depression during pregnancy and/or the postpartum period affects 6.5% to 12.9% of women. Women with depressive symptoms during pregnancy are more likely to experience similar symptoms during the postpartum period (Beck, 2001; Boyd, Le, & Somberg, 2005). Postpartum depression is a significant issue for women, with persistent postpartum depression affecting 13% of mothers (Boyd et al., 2005; Leahy-Warren & McCarthy, 2007). Like IPV victimization, symptoms of depression during pregnancy and the postpartum period have been linked to devastating and enduring negative maternal, child, and family outcomes, including a strong association with infant mortality (Da Costa, Larouche, Dritsa, & Brender, 2000; Field, Diego, & Hernandez-Rief, 2006; Goldenberg, Culhane, Iams, & Romero, 2008; Grote et al. 2010; Hammen & Brennan, 2003; Johnson & Flake, 2007; Lewis, 2007; Marmorstein, Malone, & Iacono, 2004; Weissman et al., 2006).
Depression and IPV
A meta-analysis conducted by Golding (1999) found that abused women were 3.8 times more likely to experience depression when compared to women in general. In light of such findings, it is not surprising that research studies have found that women experiencing IPV during pregnancy reported significantly higher levels of depressive symptoms when compared with women who did not experience IPV during pregnancy (Amaro et al., 1990; Certain et al., 2008; Martin et al., 2006; Rodriguez et al., 2008). The combination of IPV victimization and depressive symptoms is troubling because both stressors put women at risk for health problems and pregnancy complications. One study found that women with poor fetal outcomes were more likely to have been depressed and to have experienced IPV (Rosen et al., 2007). Specifically, mothers who gave birth to low-birth-weight infants were more likely to have experienced IPV and to be depressed when compared to mothers who gave birth to infants of normal birth weight. Such findings underscore the risks associated with the co-occurrence of depression and IPV during women’s pregnancies.
Current Study
Little is known about the relationship between women’s physical IPV victimization during pregnancy and levels of depressive symptoms before pregnancy, during pregnancy, and after infant delivery. Research studies that have simultaneously examined IPV and depressive symptoms during women’s pregnancies were primarily cross-sectional. Although such correlational research is valuable, research is now needed to investigate how depressive symptom levels might change over time as women transition from their first and second trimesters into their third trimester as well as from delivery into the postpartum period. In addition, prior studies have not typically used research designs with comparison to women who did not experience IPV during their pregnancies. The inclusion of comparison groups in such research is important because it enables researchers to determine how women who experience IPV during their pregnancies differ (or do not differ) from women who have not experienced IPV during this vulnerable time in their lives.
This study addresses the aforementioned gaps in knowledge by examining the following research questions. First, are women who were physically abused during pregnancy more likely to exhibit higher levels of depressive symptoms before pregnancy, during pregnancy, and after infant delivery than women who were not physically abused during pregnancy? Second, we were interested in knowing whether patterns of depressive symptoms differ over time between women who were physically abused during pregnancy and women who were not physically abused during pregnancy. More specifically, do women who were physically abused during pregnancy have different rates of change in their levels of depressive symptoms before pregnancy, during pregnancy, and after infant delivery relative to women who were not physically abused during pregnancy?
In relation to our first research question, we hypothesized that, relative to women not physically abused during pregnancy, women physically abused during pregnancy would be more likely to exhibit higher levels of depressive symptoms before pregnancy, during pregnancy, and after infant delivery. This hypothesis was informed by prior cross-sectional research showing a positive relationship between IPV during pregnancy and depressive symptoms (Certain et al., 2008; Rodriguez et al., 2008). To the best of our knowledge, this is the first study to investigate the relationship between physical IPV victimization during pregnancy and depressive symptoms before pregnancy, during pregnancy, and after infant delivery using both a longitudinal design and a group of comparison women. Therefore, we considered this to be an exploratory study. We did not a priori specify a directional hypothesis regarding differences in the rates of change in depressive symptoms between women victimized by IPV during pregnancy and women not victimized by IPV during pregnancy.
Methods
Study Design
Research participants were drawn from the Transition in Pregnancy Study (TIPS). The overall purpose of the TIPS was to investigate how IPV during pregnancy and the postpartum period affects the lives of pregnant and postpartum women and their infants. Participants were recruited from two prenatal care clinics that served a predominantly low-income population of women in the Southeastern United States. Health care providers (i.e., nurses and social workers) screened all incoming prenatal care patients for IPV and then invited women who reported being physically abused during pregnancy (i.e., victimized women) and women who did not report physical abuse during pregnancy (i.e., comparison women) to participate in the study. The research team asked the health care clinicians to invite one comparison woman to participate in the study for every identified victimized woman who they invited to participate. Participants had to be 18 years or older, speak English, and have no current or history of severe mental illness (as assessed by clinicians). In addition, eligible study participants had to have begun prenatal care prior to their sixth month of pregnancy. Women received nominal monetary incentives for their participation in the study; the incentive amounts escalated the longer women participated in the study. Written consent was obtained from all participants. All study protocols were approved by the human subjects protections review board from the university at which this research was conducted.
Data were collected during private meetings in the prenatal care clinics by trained female study team members, and participants were invited to complete surveys comprising standardized instruments. Participants were asked to complete the surveys at four times throughout the study: (a) For the first interview, data collection occurred when the women were 6 to 7 months pregnant; (b) for the second interview, data collection occurred 1 month after delivery; (c) for the third interview, data collection occurred 6 months after delivery; and (d) for the fourth interview, data collection occurred 1 year after delivery. The interviews were scheduled in this manner because they permitted participants to be interviewed during times that were most feasible for data collection and helped to reduce the burden of study participation for the women enrolled in the study (i.e., during their prenatal and postnatal medical check-up schedules). Furthermore, to help insure the safety of the study participants, data collection meetings were held during times that women were attending health care appointments. Thus, a woman could simply tell an abusive partner that she was going to a health care check-up if she did not wish to disclose that she was participating in this research study.
At the four data collection points, women were invited to provide detailed information about their experiences with physical IPV victimization and depressive symptoms for six time periods: (a) the 12 months before pregnancy, (b) the first 6 months of pregnancy, (c) the last 3 months of pregnancy, (d) the first month after delivery, (e) Month 2 to Month 6 after delivery, and (f) Month 7 to Month 12 after delivery. When the women were 6 to 7 months pregnant, they were asked to recall their experiences of symptoms of depression during the year before they became pregnant and to report depressive symptoms experienced during the first 6 months of pregnancy. One month after delivery, participants were asked to recall symptoms of depression experienced during the last 3 months of pregnancy and to report depressive symptoms experienced during the first month after delivery. Six months after delivery, participants were asked to report symptoms of depression experienced during Month 2 through Month 6 after delivery. During the final interview, 1 year after delivery, participants were asked to report the symptoms of depression experienced during Month 7 through Month 12 after delivery. To stimulate women’s memories of these issues, a calendar was used during each interview to help the women recall and sequence their experiences throughout the pregnancy and postpartum months. Table 1 presents information about the timing of each of these interviews as well as the time periods about which participants were asked questions during the surveys.
Timing of Personal Survey Interviews for the Transitions in Pregnancy Study.

Study Sample
The overall TIPS sample included 104 women; however, only women who reported their IPV experiences during pregnancy were included in the current study. Thus, a subsample of 76 women comprised the sample used in the current study. It is noteworthy to mention that we conducted bivariate analyses to compare the sociodemographic characteristics of the subsample of women included in this study to the subsample of women not included in this study. Findings revealed that the two samples did not significantly differ on education level, employment status, marital status, having other children, and age at delivery; however, the samples differed on race. Specifically, the women who were not included in the current study (n = 28) were less likely to report being African American (0.00%) than the women who were included in the current study (48.78%).
Measures
Depressive symptoms
Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). The CES-D is a 20-item retrospective self-report instrument developed to measure how frequently symptoms of depression occurred during the past week. However, similar to past studies (e.g., De Berardis et al., 2002; Kurtz, Kurtz, Given, & Given, 1997; Radloff, 1977), and for the purpose of this study, we adapted the CES-D’s time frame so that it coincides with the six time periods referenced in the current study. Specifically, the CES-D was used to ask participants about symptoms of depression that occurred during six time periods: (a) the 12 months before pregnancy (i.e., “Please tell me how often you have felt this way during the year before pregnancy”), (b) the first 6 months of pregnancy (i.e., “Please tell me how often you have felt this way during the first 6 months of pregnancy.”), (c) the last 3 months of pregnancy (i.e., “ Please tell me how often you have felt this way during the last 3 months of pregnancy.”), (d) the first month after delivery (i.e., “Please tell me how often you have felt this way during the first month after delivery.”), (e) Month 2 to Month 6 after delivery (i.e., “ Please tell me how often you have felt this way during the 2 to 6 months after delivery.”), and (f) Month 7 to Month 12 after delivery (i.e., “Please tell me how often you have felt this way during 7 to 12 months after delivery.”). The instrument includes statements such as “I felt depressed,” “I felt sad,” and “I felt everything I did was an effort.” Responses were scored on a 4-point scale ranging from rarely or none of the time (less than 1 day, scored as 0) to most or all of the time (5 to 7 days, scored as 3). Items were summed to generate a total score with a possible range from 0 to 60, with scores of 16 to 26 indicating “mild depressive symptoms” and scores of 27 or more indicating “major depressive symptoms” (Ensel, 1986; Zich et al., 1990).
Physical IPV
The women’s experiences with physical IPV victimization during pregnancy were assessed using the Conflict Tactics Scale 2 (CTS-2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The CTS-2 is an instrument that assesses the frequency and severity of five different types of violence: (a) negotiation, (b) psychological aggression, (c) physical assault, (d) sexual violence, and (e) injury. The current study only uses reports from the physical assault measures of the CTS-2.
The Physical Assault CTS-2 subscale contains 12 items, each item assessing a behavioral act of IPV victimization that may have occurred in the women’s relationships during a particular time. For the purpose of this study, the time frame inquired about IPV during pregnancy. The physical assault measures assessed behaviors such as “my partner pushed or shoved me” and “my partner beat me up.” Responses were scored on a 7-point scale ranging from never (scored as 0) to more than 20 times (scored as 6), which indicated how frequently this behavior occurred within the specified time frame (i.e., during pregnancy). Women were considered victimized if they reported any incident of physical IPV victimization at any time during their pregnancies. Thus, we developed a dichotomous (0 to 1) variable using the physical assault data to identify members of the victimized and comparison groups.
Analysis
Depressive symptoms were measured using multiple observations on each participant over time. Therefore, the data were multilevel, with Level 1 as the occasion level and Level 2 as the individual level. To account for participant-specific response correlations that occur with multilevel data, we conducted the analyses in this study using hierarchical linear modeling (HLM; Raudenbush & Bryk, 2002; Singer & Willett, 2003). One possible consequence of ignoring the presence of participant-specific correlated responses is that standard errors estimated by models assuming mutual independence (i.e., ordinary least squares) can be either too high or too low, leading to biased statistical conclusions (Singer & Willett, 2003). Furthermore, the lack of independence among observations violates assumptions embedded in most conventional linear models. This type of statistical analysis is recommended for an investigation of changes over time (Luke, 2004; Raudenbush & Bryk, 2002). Thus, we used HLM to model patterns of depressive symptoms before pregnancy, during pregnancy, and after infant delivery using participants’ CES-D scores to determine whether rates of change in depressive symptoms over time differed between women who were physically abused during pregnancy and women who were not physically abused during pregnancy. This modeling strategy allowed for an assessment of time-period-specific differences in average CES-D scores between victimized and comparison groups. Data in this study were analyzed using the HLM Version 6.0 (2004) and SPSS Version 16.0 (2007) statistical software packages.
Results
Participants
As previously mentioned, the present study used data from 76 participants who reported their IPV experiences during pregnancy. Thirty-three of these women reported physical IPV victimization during pregnancy. For study purposes, these women constituted the victimized group. Another 43 women reported no physical IPV victimization during pregnancy, and these women made up the comparison group. For the complete sample (n = 76), participants’ ages at delivery ranged from 18 to 45 years (M = 26.51, SD = 6.43).
Comparisons between victimized and comparison groups’ sociodemographic characteristics (see Table 2) revealed a significant difference only in employment status: 57.6% of the victimized group was employed as compared with 79.1% of the comparison group (p < .05). The two groups did not differ significantly in terms of their education, marital status, race, or having had other children. The two groups were similar in age at delivery, with the victimized group having a mean delivery age of 26.5 years and the comparison group having a mean delivery age of 26.6 years.
Participants Sociodemographic Characteristics.
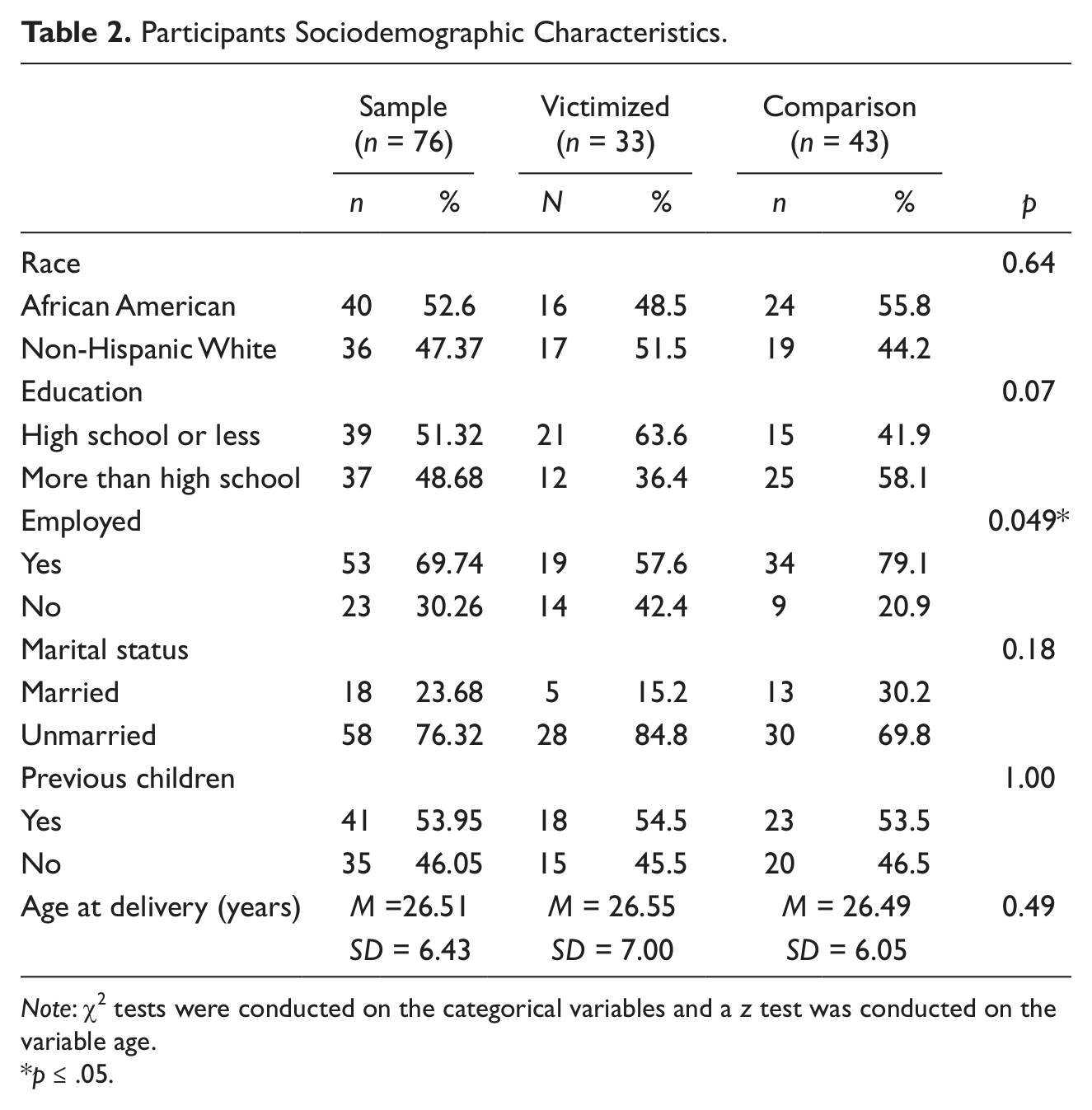
Note: χ2 tests were conducted on the categorical variables and a z test was conducted on the variable age.
p ≤ .05.
HLM Model
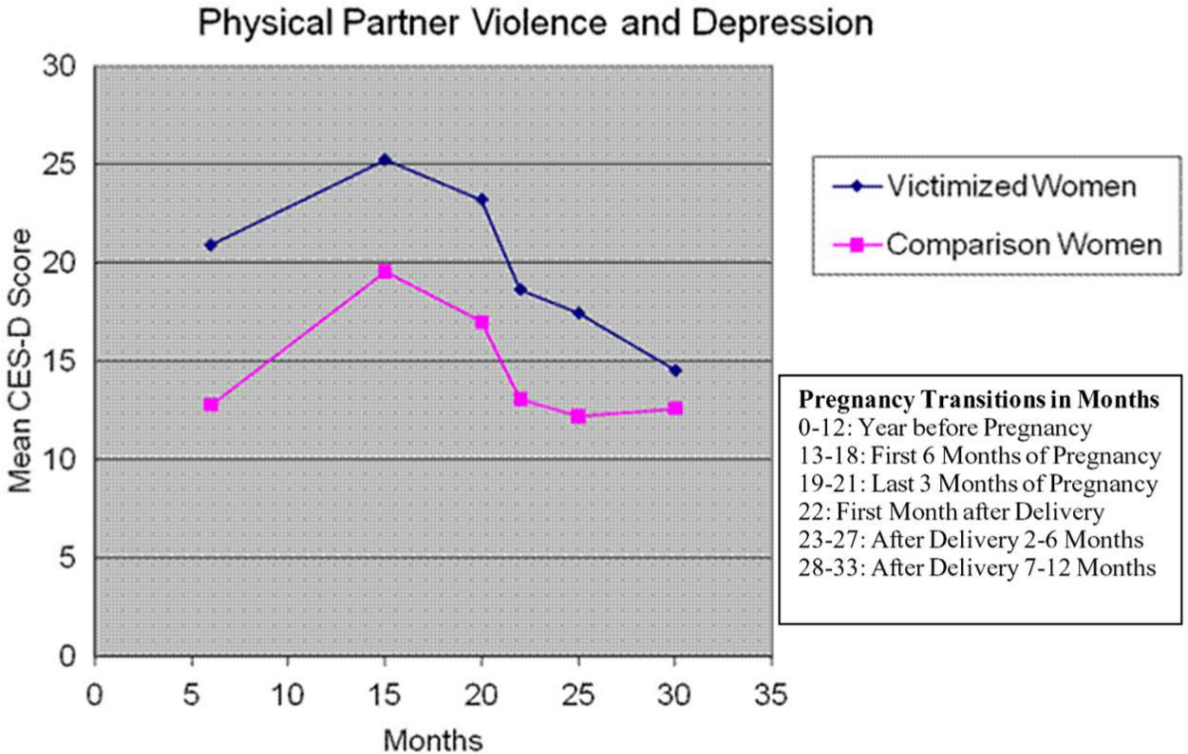
We used HLM to quantify differences between victimized women and comparison women’s changes in levels of depressive symptoms over time. We investigated (a) whether victimized women were more likely to exhibit higher levels of depressive symptoms than comparison women and (b) whether there were differences between victimized women and comparison women’s rates of change in depressive symptoms over time. Figure 1 suggests a curvilinear relationship between time and mean depressive symptom scores, both for the victimized women’s group and for the comparison women’s group. Hence, our HLM modeling process considered two predictors, a dichotomous (0 to 1) variable (delineating members of the victimized and comparison groups) and linear and quadratic (i.e., squared) time variables. There was no statistical evidence of interaction effects between the dichotomous variable and the linear and quadratic time variables. This finding indicated that the rate at which CES-D mean scores changed over time was statistically the same for each group. In other words, the victimized women and comparison women had similar patterns of changes in depressive symptoms before pregnancy, during pregnancy, and after infant delivery. Therefore, the best fitting HLM model indicates that there are two parallel quadratic curves, one curve for the victimized group and one curve for the comparison group. And at any point in time, the expected difference in mean depressive symptoms between a woman in the victimized group and a woman in the comparison group is constant. The 95% confidence interval for this constant difference is (1.326, 9.538), indicating that women who experienced physical IPV victimization during pregnancy had a significantly higher (but non-time-varying) level of depressive symptoms before pregnancy, during pregnancy, and after infant delivery than women who did not experience physical IPV victimization during pregnancy. Furthermore, based on the fitted model, depressive symptom levels (i.e., mean CES-D scores) are predicted to rise steadily from a baseline value to a maximum value estimated to occur at about 3 months into pregnancy for each group and then to decline steadily thereafter. This finding agrees closely with the group-specific mean CES-D scores before pregnancy, during pregnancy, and after infant delivery presented in Table 3.
Mean Depressive Symptoms Scores Experienced by the Victimized and Comparison Women Across Six Time Periods.
Victimized (n = 33) and Comparison Women (n = 43) Mean Center for Epidemiologic Studies Depression Scale Scores

Note: Higher Center for Epidemiologic Studies Depression Scale scores indicate higher levels of depressive symptoms.
Discussion
In this exploratory study, we investigated whether women who reported physical IPV victimization during pregnancy were significantly more likely to exhibit higher levels of depressive symptoms than women who did not report physical IPV victimization during pregnancy. We also examined whether women who were physically abused during pregnancy have different rates of change in their depressive symptoms before pregnancy, during pregnancy, and after infant delivery relative to women who were not physically abused during pregnancy. To the best of our knowledge, this is the first study to examine the relationship between physical IPV victimization and depressive symptoms before pregnancy, during pregnancy, and after infant delivery using a longitudinal design and a comparison group.
Consistent with prior research (Amaro et al., 1990; Certain et al., 2008; Rodriguez et al., 2008), we found that women who reported physical IPV victimization during pregnancy were more likely to exhibit depressive symptoms than women who did not report physical IPV victimization during pregnancy. We also found that women who reported physical IPV victimization during pregnancy had higher levels of depressive symptoms throughout the postpartum period relative to the comparison women.
Although the women who experienced physical IPV victimization during pregnancy were more likely to have higher levels of depressive symptoms than women who did not experience physical IPV victimization during pregnancy, our findings indicate that the rates at which depressive symptoms changed before pregnancy, during pregnancy, and after infant delivery did not differ significantly between the two groups of women. Levels of depressive symptoms were higher during pregnancy than during times before or after pregnancy for all women in this study. It is possible that women’s elevated depressive symptoms during pregnancy were related to pregnancy-specific issues (e.g., somatic symptoms, parenting concerns, physiological changes, and body-image) they experienced (Da Costa et al., 2000; Leahy-Warren & McCarthy, 2007). Therefore, all the women in this sample may have appeared to experience depressive symptoms during pregnancy that were, in fact, related to pregnancy-specific issues rather than to depression.
Despite our finding that the two groups of women did not differ significantly in how their rates of depressive symptoms changed over time, our finding that the victimized group had a significantly higher (non-time-varying) level of depressive symptoms than the comparison group over all six time periods is noteworthy. Our study’s findings add to the extant research on IPV, depressive symptoms, and pregnancy by providing important information regarding the times before pregnancy, during pregnancy, and after infant delivery when levels of depressive symptoms may be highest among women who experience physical IPV victimization during pregnancy. Notably, prior research shows that depression significantly hampers IPV survivors’ ability to seek safety (e.g., Rose et al., 2010) and increases the risk of poor fetal outcomes (e.g., Rosen et al., 2007). In light of this earlier research, our findings suggest that women victimized by physical IPV may be in particular need of interventions to help alleviate depressive symptoms during their pregnancies. Nonetheless, women victimized by IPV during pregnancy may benefit from interventions for depression even after delivery because the victimized women in this sample had elevated levels of depressive symptoms throughout the year after their deliveries relative to the comparison women.
Screening and Interventions for IPV Victimization During Pregnancy
Based on this study’s findings that show that women victimized by IPV during pregnancy are at greater risk for experiencing symptoms of depression, health care providers may want to screen all women receiving prenatal care for IPV. When providers identify IPV for particular patients, these women should be offered interventions aimed at preventing and/or alleviating depressive symptoms, as well as IPV. However, recommendations about routine IPV screening have been controversial. Although researchers have recommended that screening and rescreening for symptoms of depression during pregnancy and postpartum should be performed routinely (e.g., Austin & Lumley, 2003), the U.S. Preventive Task Force concluded that there is insufficient evidence to support the practice of routine screening in health care settings (MacMillan et al., 2009; Macy, Ermentrout, & Johns, 2011; Plichta, 2007). This recommendation has been reinforced by systematic review studies that have reported no improvements or modest improvements in IPV survivor outcomes once IPV is detected (MacMillan et al., 2009; Ramsay, Richardson, Carter, Davison, & Feder, 2002; Spangaro, Zwi, & Poulos, 2009). Despite such evidence, it is noteworthy that researchers have identified significant positive relationships between screening for IPV and IPV detection (Plichta, 2007; Spangaro et al., 2009). Researchers have also concluded that, although IPV screenings do not always lead to improved outcomes for IPV survivors, IPV screening in health care settings causes no harm to patients (MacMillan et al., 2009).
Taking into account such findings, some IPV researchers have continued advocating for universal IPV screening in health care settings in spite of recommendations against IPV screening, (e.g., Macy et al., 2011; Plichta, 2007; Spangaro et al., 2009). Researchers in support of universal IPV screening in health care settings argue that IPV screening is beneficial when followed by the appropriate IPV interventions. The findings from this current research, showing elevated depressive symptoms for women physically abused during pregnancy relative to comparison women who were not abused, add weight to such recommendations.
Nonetheless, our review of the literature produced little information regarding the efficacy of interventions for treating pregnant women who are both victimized by IPV and who are experiencing elevated depressive symptoms. We only found one published study investigating an intervention concerned with depressive symptoms among women victimized by IPV during pregnancy (Duggan et al., 2004). This study investigated a social support intervention and found this intervention had no effect on women’s levels of depressive symptoms or IPV prevalence over time (i.e., at childbirth and annually for 3 years). In light of this study’s findings, we recommend future research to examine the effects of social support interventions on depressive symptoms before pregnancy, during pregnancy, and after infant delivery in women experiencing IPV during pregnancy.
We recommend that interventions not only focus on lowering depressive symptoms but also directly address IPV victimization through efforts to promote women’s safety and violence cessation. We believe such a focus is important given our study’s findings that women’s depressive symptoms are significantly associated with their IPV experiences during pregnancy. Safety-focused interventions may play an important role in reducing IPV and thereby reduce depressive symptoms before pregnancy, during pregnancy, and after infant delivery. Accordingly, we encourage future research to develop and investigate combined mental health and safety interventions that directly target both IPV victimization and depressive symptoms among pregnant women who are victimized by IPV.
Limitations, Future Research, and Conclusions
This study has strengths, including the use of a comparison group and the measurement of women’s depressive symptoms over several times. The study also has limitations. First, our findings are not representative because the majority of participants were low-income women living in the Southeastern United States. In addition, the study sample was limited to participants with IPV information during their pregnancies and differed significantly by race compared to the women who were not included in the study. We encourage future research to investigate depressive symptoms and IPV with large, nationally representative samples of pregnant and postpartum women. Second, depressive symptoms were sometimes assessed retrospectively. This was specifically the case when examining depressive symptoms experienced during the year before pregnancy and during the last 3 months of pregnancy. We used a calendar during each interview to help the women recall how they felt during the times they were asked to retrospectively report symptoms of depression. However, it is possible that some accounts did not correspond to depressive symptoms experienced at times of interest. Third, we were unable to tease apart whether some symptoms were due to common pregnancy experiences or to depression because we used the CES-D to measure depressive symptoms. For example, the CES-D asks about depressive symptoms, such as changes in appetite, sleep patterns, and concentration, which are also common pregnancy symptoms. We recommend that future research use an instrument, such as the Edinburgh Postnatal Depression Scale, designed to measure depressive symptoms in pregnant and postpartum women. Furthermore, the analysis did not include information on the numerous types of potentially stressful events that occurred during each time period, including other forms of IPV (i.e., psychological and sexual violence) and different levels of IPV (i.e., mild and severe IPV). In a related vein, because of the small sample size and given the power needed to precisely assess the effects of changes in time-varying covariates, we were unable to examine the relationship between changes in IPV and changes in depressive symptoms. Specifically, our analysis does not take into consideration violence that occurred (or did not occur) at times other than during pregnancy and how IPV outside of pregnancy may or may not influence depressive symptoms before, during, and after infant delivery. Such events, particularly changes in women’s IPV victimization, likely relate to women’s depressive symptoms. Therefore, we recommend that future research assess the relationship between changes in IPV before pregnancy, during pregnancy, and after infant delivery along with changes in women’s depressive symptoms. We also recommend that future research explore the relationship between IPV and depressive symptoms while controlling for different types of stressors besides IPV that affect pregnant women.
Despite these limitations, this novel study provides evidence about the relationship between IPV and levels of symptoms of depression before, during, and after pregnancy. Furthermore, this exploratory investigation helps to identify times at which depressive symptoms are most elevated among pregnant women physically abused during pregnancy. Such results highlight the need for interventions for victimized pregnant and postpartum women that simultaneously address the effects of depression and IPV. We recommend the development and testing of such coordinated safety and mental health interventions as an important next step for researchers concerned with the intersection of pregnancy, depression, and IPV. It is important that we recognize the comorbidity of IPV and depression before pregnancy, during pregnancy, and after infant delivery and continue to advance and develop this research area.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.