
Abstract
Despite efforts to use behavior modification interventions for male perpetrators, intimate partner violence (IPV) remains a significant problem in some male–female relationships. Childhood exposure to traumatic violent experiences, especially when untreated, can influence adult behaviors. Little is known about these possible factors in the lives of male perpetrators of IPV and if they influence their violent behavior against female intimate partners. This study’s aim was to explore the life perspective of men who have been violent with their female intimate partners using Gadamer’s hermeneutic phenomenology. Nine men with a history of female IPV were interviewed twice over a 5-month period. Interview content focused on their experiences in childhood and adult lives. Four themes emerged from the qualitative interviews: (a) childhood and family issues, (b) school and mental health issues, (c) substance abuse and (d) legal issues. Traumatic violent experiences in childhood, such as physical and sexual abuse, frequently led to school problems, misuse of substances, and arrests for a spectrum of crimes. These results highlight the importance of identifying traumatic violent exposures through a brief two-question screen of all children in primary care. Implications for individualized mental health treatment of male perpetrators and recommendations for further research are addressed.
Men who perpetrate intimate partner violence (IPV) have been treated as a uniform group. The current standard of care for IPV perpetrators is the Duluth Model (Gondolf, 2007), a gender-based cognitive-behavioral model intended to increase behavior responsibility and teach gender sensitivity. It is a standardized approach for men who have been arrested for IPV. This model was conceptualized by the feminist paradigm that defines IPV as a result of male dominance and paternalism, where male perpetrated violence can be stopped if men are taught a new respect for women through intervention of the criminal justice system and behavior modification. Family violence researchers such as Dutton, Corvo, and Hamel (2009) have attempted to demonstrate the failure of this model to provide a valid treatment option for IPV. They cite Conflict Tactic Scale data (Strauss & Gelles, 1999) that identify significant amounts of common couple violence and female violence toward children as evidence that women are also perpetrators of IPV. Intimate partner violence has been identified as a more complex family system that cannot be solved by a universal treatment program (Dutton et al., 2009). Male perpetrators have reported higher levels of anger and hostility than nonviolent men (Norlander & Eckhardt, 2005). However, little is known about lifetime exposures of male perpetrators that influence anger, hostility, and subsequent violence toward their female intimate partners. Not all male perpetrators of IPV are alike; some may have untreated mental health issues from traumatic exposures in their lives. Through understanding these potential exposures, clinicians will be able to recognize risk factors and plan interventions to break the cycle of IPV.
An estimated 3 to 10 million children witness IPV between their caregivers each year (Pulido, 2001; Strauss & Gelles, 1999). Studies indicate that children raised in homes where parents engage in IPV are at a higher risk of maltreatment either as intended targets of violence or as accidental victims (Berkowitz, 2005; Jouriles, McDonald, Slep, Heyman, & Garrido, 2008). It is estimated that approximately 60% of children in homes where IPV is present are victims of maltreatment (Berkowitz, 2005). In IPV families, mothers were as likely as fathers to use severe physical punishment against their children (Jouriles et al., 2008).
Research suggests that children exposed to IPV are more likely to become perpetrators or victims of IPV (Gil-Gonzalez, Vives-Cases, Ruiz, Carrasco-Portino, & Alvarez-Dardet, 2008; Healey, Smith, & Sullivan, 1998; Widom, 1989, 1992; Widom & Maxfield, 2001). Worley, Walsh, and Lewis (2004) examined the experiences of male perpetrators in their childhood and found men did not believe that exposure to IPV in their families affected their current issues with IPV. However, these men reported significant exposure to IPV between their parents and received severe punishments, such as being beaten by a belt, as children.
Widom’s Cycle of Violence (1992, 2001) followed children identified as being abused or neglected into adulthood and described how IPV has an intergenerational transmission. While most of the abused children in their study did not have problems with violence, the children who were abused or neglected were more likely to have contact with the juvenile justice system at a younger age and have more issues with violence later in life. Anda et al. (2006) used the Adverse Childhood Experiences Study data (ACE) to detect patterns in adulthood that are common in children who survive adversity. They found children exposed to trauma or stress, particularly as a witness or victim of IPV, frequently escape detection by the community and are less likely to receive treatment for their traumatic exposure symptoms. The ACE score increases with number of exposures to child abuse and/or neglect and corresponds to the individual’s perceived level of stress, ability to control anger, and likelihood of perpetrating IPV. Other areas evaluated include somatic disturbances, mental health issues, substance abuse, anger management issues, and sexual dysfunction. They describe a similar “graded relationship” between exposure and outcome. More severe childhood exposures were associated with increased health and mental health risks as an adult, including the potential of being a victim or perpetrator of IPV.
Studies have shown male perpetrators may have had childhood exposure to IPV or abuse. There are possibly many factors, such as biological, psychological, and/or social factors, contributing to violence in this group; however, little is known about these factors. Bowlby’s Attachment Theory (1969) and Bandura’s Social Learning Theory (1973) offer sociologic theories to explain perpetrator behavior. The evolving science of developmental psychopathology provides more evidence into the interaction between the child’s genetic blueprint, environment and family influences that may contribute to family violence (Fox, Levitt, & Nelson, 2010). It is critical for clinicians to understand these factors to have an effect on decreasing the incidence of IPV and subsequently intervening in the cycle of violence. The purpose of this phenomenology study was to understand the lives of men who have been violent toward their female intimate partners.
Method
Study Design
Hermeneutic phenomenology was used in this qualitative study to understand the lived experience of male perpetrators of IPV. The purpose of Gadamer’s (1989) hermeneutic phenomenology is to develop a new understanding of an area of health interest not previously examined in the field. This study design was deemed appropriate to identify factors that may influence the development of violence in male perpetrators of IPV since in-depth interviews allow participants to verbally tell their stories. Thus the words of the participants described their childhood and adult experiences presenting their perspective on their lives.
Ethical Considerations
The University of Maryland Baltimore’s Institutional Review Board (IRB) approved the study. The National Institute of Health issued a Certificate of Confidentiality used to protect participants from information obtained during the interviews being available for legal review. Participants were given a brief cognitive assessment tool recommended by university’s IRB before obtaining informed consent. This tool asks questions to ensure the participants understand risks and benefits of the study.
Sample
Participants were recruited from a department of corrections prerelease center in the mid-Atlantic region. This site was used for recruitment because potential participants had histories as perpetrators of female IPV and were involved in the legal system for IPV and/or other crimes. Men in the prerelease center were not currently abusing substances and were not receiving treatment for any IPV-related issues or mental health issues. An in-service about the study was presented to counselors at the prerelease center. These counselors identified eligible men and referred them to the first author (MW). Eligibility criteria include (a) a history of violence toward a female intimate partner with whom they had a history of cohabitation, (b) men between 22 and 65 years of age, and (c) the ability to speak and understand English. The concept of male perpetrator was delineated in this manner to ensure transferability of findings to male–female IPV. Female perpetrators and same sex perpetrators were excluded from the study because their experiences may be different than male–female IPV. The men were not compensated for their participation to ensure they were willing to discuss their stories with the first author (MW) and were not coerced.
Sample Characteristics
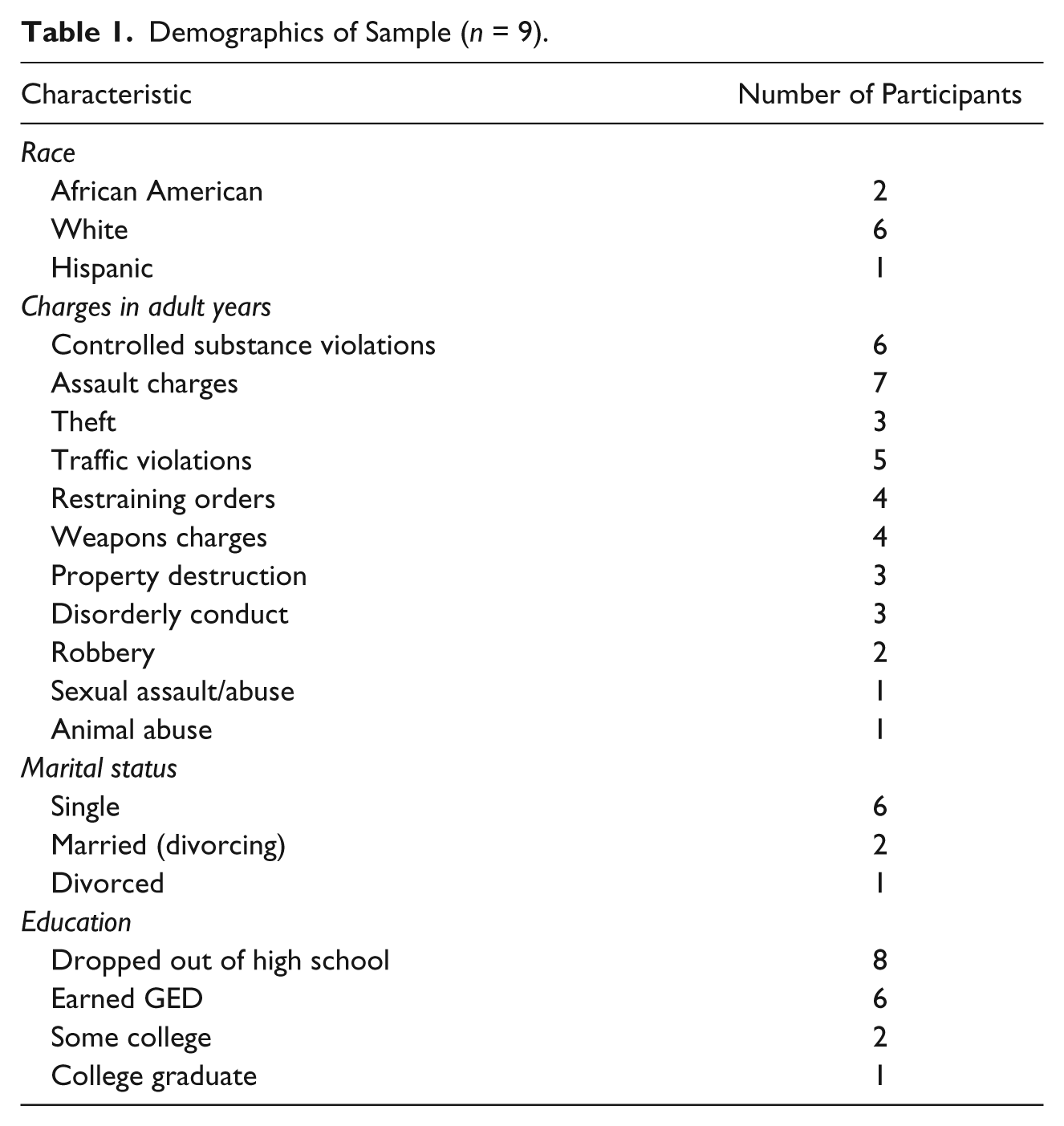
Nine men, ages 22 to 46 (mean = 31.8 years) participated in the study. According to Hermeneutic phenomenology research, as delineated in van Manen’s Rules (1990), sample size is determined by redundancy of information obtained through in-depth interviews. The redundancy of themes was reached after the 8th participant interview. However, an additional participant was interviewed to reaffirm redundancy of themes. Table 1 lists the race, education, marital status, and legal charges of the participants. Four of the men were currently serving time for IPV convictions. The men who were not incarcerated for IPV had a history of IPV and met the inclusion criteria. They had experienced the phenomena of IPV perpetration and were able to speak about their life experiences. Five children were present during their parent’s perpetration of IPV. Three men reported children in the room during IPV.
Demographics of Sample (n = 9).
Procedure
Two interviews were conducted with the participants. In a quiet, private room, the first author (MW) conducted initial interviews after informed consent was obtained at the prerelease center. These interviews were audiotaped and lasted 60 to 90 minutes, depending on each participant’s time needed to tell his story. The second interview, conducted within 1 to 2 weeks of the first interview, allowed the interviewer to ask questions generated from the first interview and give participants opportunity to add additional information. These second interviews lasted 15 to 45 minutes, depending on the participant. Both interviews consisted of open-ended questions. For example, to understand the men’s childhoods, they were asked questions such as “Tell me about your family,” and “Tell me about your experiences growing up.” Prompts were given allowing participants to tell their story as much as possible.
Data Analysis
Van Manen (2007) described the phenomenological practice as a “reflection on the lived experience of human experience” that is “free from theoretical, prejudicial and suppositional intoxications” (p. 11) as much as possible. He outlined six steps to follow in the practice of hermeneutic phenomenology, which were followed in the data analysis process. The researcher must first choose a phenomenon of which he/she is passionate. The phenomenon is examined and investigated as it occurs. The researcher filters out presuppositions and implicit assumptions of IPV behaviors and listens to the data to capture the meanings of the experiences of the participant. The next step involves deconstructing phenomenon to find themes that characterize it. The researcher then restructures the themes to create an explanation of the whole. Throughout this process, the researcher maintains grounding to the phenomenon. The final step is “balancing the research context by considering parts and whole” (van Manen, 1990, pp. 30-31).
The first author (MW) transcribed the interviews verbatim after the conclusion of each interview. Each participant was given a pseudonym to protect confidentiality. The texts were analyzed using the Atlas Ti program and van Manen’s Rules (2007). Atlas Ti is a qualitative software program that assists qualitative researchers to track codes and quotes when analyzing the interview texts. The Second author (DS) analyzed the interviews independently to ensure rigor. Two researchers independently coded transcripts and reached agreement on the themes. A methodological and analytical audit trail describing the coding process was maintained throughout data analysis.
Results
Thematic Overview
The thematic analysis revealed some possible factors that may contribute to male perpetrator IPV with women. Four overarching themes emerged: (a) childhood trauma/family issues, (b) school and mental health issues, (c) substance abuse, and (d) legal issues. The stories of the participants share a progression from childhood trauma to perpetration of IPV. School and mental health issues are linked because problems with mental health issues occurred during their childhood and impacted their school performance. All of the participants had substance abuse and legal issues throughout their lives.
Theme 1: Childhood trauma/family issues
This theme depicts the experiences of childhood traumas in these participants’ lives. Growing up in single parent households, witnessing violence between caregivers and being victimized by family members are examples of the participants’ experiences during childhood. Childhood trauma includes abandonment by parents, witnessing IPV, and victimization including being sexually abused as a child. All 9 participants had some type of childhood trauma. Subthemes were developed to highlight these experiences. These subthemes include abandonment, witnessing IPV in the family, and experiencing violence.
Abandonment
This subtheme included abandonment of fathers and/or mothers, whether it was the parent physically leaving the child or having the child leave the parents. Abandonment also included parents emotionally leaving the participants as children as in the example of a parent’s alcoholism. One participant, Cal, disclosed being abandoned by both parents:
I never met my father. She (mother) was barely ever around. I probably only saw her once or twice a week . . . she was there but I never really had a mother . . . Grew up on the streets, pretty much . . . . She was an alcoholic so she left when I was thirteen.
It also appeared there was variation in the responses to the abandonment by the participants now as adults. Responses ranged from not blaming the parent for the abandonment and maintaining adult relationships with him or her to having hatred for the parent. For example, Ben also experienced abandonment by his mother. The couple that raised him adopted him while his biological mother raised his siblings. He reported maintaining a relationship with his biologic mother and siblings.
My birth mother, she did the best she could. She had my brother and she had him when she was 15 . . . then she had me, then my sister. . . . But then, when my father got locked up, she couldn’t afford, she was already homeless. . . . so she had to put me up for adoption. . . . I’m not mad about it. I don’t have any resentment ’cause people ask me that a lot.
He described his adoptive father as his real father; however, his adoptive mother had difficulty controlling his behavior and committed him to an institution when he was 14. This situation was a second episode of abandonment for this participant.
Witnessing IPV in the family
Several of the participants experienced IPV as children in their family of origin. The violence between their caregivers ranged from physical to verbal abuse. A disconnect existed between the participants’ perception of their families and their descriptions of violence in the households. Participants described their family life in peaceful terms or as being “normal,” while stating parents engaged in frequent behaviors such as strangulation, pulling a knife, and verbally fighting, all in front of the children. For example, Ed described his mother as a “Quaker-hippy type.” However, he described a situation where his mother was violent:
My mother, one time, she tried to choke him (boyfriend) with a telephone cord. He was sitting on the steps . . . I don’t even know what they were arguing about. I think it had to do with . . . fidelity and lack of trust . . . He was sitting on the steps . . . and she tried to choke him . . .
In one altercation between his mother and her boyfriend, Ed actually intervened on his mother’s behalf as a child:
She pulled out a knife . . . tried to attack him but he restrained her to the ground. And I think it was more like instinct to defend my mother . . . I jumped on his back and tried to get him off her but I was very small . . . I couldn’t do anything . . . I tried to choke him . . . sticking my fingers into his Adam’s apple trying to get him off my mom. He didn’t hurt me. He didn’t touch me. He even told me and my brother he loved us before he left.
Three of the men described interactions between their parents as verbally abusive although they did not admit to the verbal abuse early in the interview. However, as their description continued, the nature of the interactions became apparent. One participant, Al, first described his family as “normal,” but later admitted to frequent parental conflict.
My parents did fight a lot when I was growing up . . . they were going through a messy divorce and I just remember them fighting a lot . . . one of my favorite movies to watch when I was like 10 years old was War of the Roses [a movie about violence in divorce] . . . I don’t know, I guess its ’cause my parents were going through a divorce like that.
There was a frequent perception by the participants that they are unclear if witnessing IPV had an effect on them. Henry described witnessing a similar interaction between his parents as Al. “. . . I remember looking up at him [father] and seeing them screaming at each other. I don’t know if that had an effect on me or not.”
Experiencing violence
Participants reported physical punishment, at times severe, during their childhood. In the interview, they were asked what would happen if they misbehaved as a child. If they answered they were spanked or physically struck, they were asked what was used to hit them, for clarification. Frequent responses are stated by Dave,
Whopped our ass. Belt, switch, extension cord, shoes, pluck. He’d tear my brother up . . . he would go to the body . . . Punching . . . But my brother was scared, so was I, that he would kill us.
The participants not only minimized the effects of witnessing IPV on their behaviors, they also tended to view the violence they experienced as children as acceptable. For example, Henry began by saying, . . . at one point my dad . . . he’s gotten physical with us but he’s never done anything serious . . . He’d use a belt . . . And I didn’t like it but I never thought he went too far when he went to spank us.
Participants would accept spanking with belts or hands as discipline as long as anger was not apparent in the parents. However, when an anger situation was present, participants identified that parents slap and hit without the intent of discipline. Henry later admitted in the interview, If he ever became involved in some anger situation, he’d [father] go over the line . . . we were like sitting around . . . eating pizza and something happened over a slice of pizza . . . I remember him . . . slapping one of my sisters in the face . . .
Henry continued to describe violence by his father and his mother toward him, where one episode led to his father being arrested for second degree assault.
Ben reported being spanked as a child, resisted this punishment as he aged, and had a fistfight with his father. He also minimized this episode by saying “he didn’t hit me hard”:
He would try to spank me . . . at like twelve or thirteen ’cause I got suspended from school and that was the day I tried to fight him . . . I think he hit me in my chest ’cause I hit him in his face . . . he didn’t hit me hard in the chest . . . He just hit me and knocked me on my bed.
Three of the men disclosed child sexual abuse. This question was not asked of the participants, rather it was mentioned by these participants. None of the men reported that they were ever treated for the trauma. One man told his parents but they did not believe him. One man was sexually abused at two different intervals, one man was abused over several years and one man reported a single event. These participants described feelings of shame, embarrassment, lack of control, and “I should have just handled it” about the sexual abuse. “There was another incident, a little bit later . . . That one I didn’t tell because I was more ashamed of that . . . I was thirteen . . . it’s embarrassing.” This participant never received treatment for the sexual abuse despite being hospitalized for severe substance abuse. The researcher was only the second person to hear his disclosure of sexual abuse.
Theme 2: School/mental health issues
School issues and mental health issues are linked because participants frequently stated their mental health issues coincided with the onset of school problems. These problems in school mostly led to dropping out of high school. However several did earned their General Equivalency Diplomas while others completed some college. The progression in many of the participants’ stories was traumatic events, such as abuse, abandonment, and neglect, followed by decline in school performance and later substance abuse. Experiences in school also involved exposures to violence. For example, Henry was placed in special education at a different school. This experience exposed him to additional violence and did not treat his underlying issues.
Most of the kids there are there for . . . violence in schools and . . . crime related. And someone like me, who has a learning disability . . . gets SHOVED [emphasized by participant] in there. So I’m not receiving help for my problems . . . I’m pretty much in an environment where most kids are in there for violence.
Participants reported many formal/informal mental health problems and evaluations for behavioral and academic problems. Four men reported formal diagnoses of Attention Deficit Hyperactive Disorder (ADHD), bipolar disorder, and learning disabilities. Some participants reported bouts of depression, suicide attempts, and combative behavior. One participant reported anxiety symptoms: “I wouldn’t say worried, more anxious. I guess I have anxiety.” One participant who reported sexual abuse described several depressive episodes in his lifetime, including an extended hospitalization as a teenager. He asked his parents to hospitalize him for his severe drug abuse.
I mean . . . I was, physically, I had fallen down and my heart had stopped beating so many times I thought I was going to die . . . I went to detox and they were able to get me there. That’s where I was actually diagnosed [with depression] . . . I was inpatient for two months . . . again for a month about six months later. Not for using but just having a hard time dealing with life.
Henry began having problems with depression in the fourth or fifth grade after his father told him people eventually die. He was medicated with sertraline and hospitalized several times. He reported having violent outbursts in school: “they restrained me right there on the floor [in special education] . . . I’m going to kill you, I’m going to get my Glock and shoot you . . .”
Previous traumatic issues, such as abandonment, affected Cal who initially enjoyed school and athletics, but quit after his alcoholic mother left him at age 13. “. . . I tried to stay in school . . . but it just wasn’t working. It was either go to school and be homeless or have a place to live . . .” He subsequently began selling drugs for money.
Theme 3: Substance abuse
All participants had problems with substance abuse; most began abusing substances in their early teen years. One of the men reported using marijuana at 8 years old, “sixteen, fifteen, gateway to drugs with weed and alcohol . . . seventeen, eighteen, ecstasy, ’shrooms . . . cocaine, snort . . . nineteen, twenty, crack . . . that’s it.” Another man described smoking cigarettes and occasional marijuana in his early teens and progressed.
I guess I took my first drink when I was seventeen, high school, you know. Alcohol has always been a major issue with me. I could sit there and drink ten beers and umpteen shots. I mean ten to twelve shots and just be gone. I wouldn’t drink just to drink. By the end of the night, I’d be passed out somewhere. I was a mess at one point but I was a better mess being an alcoholic than I was with the pills and heroin. That was a completely different ball game. You know and after the first high, it was all downhill from there. I started to, I was snorting stuff and now I was shooting up and now I don’t care. A month late, I don’t care what anybody thinks. I want, I started craving the needle.
The use of substances led to legal issues for the participants. For example, many participants sold drugs to support their habit and lifestyle.
I guess it’s fast . . . the money . . . You party all day . . . You can wake up at one, two, three o’clock . . . I would make six hundred to a thousand dollars a day . . . five thousand dollars a week.
One man described selling drugs to support his college education.
I was actually going toward my bachelor’s in business but drugs, it was drugs again. That lifestyle. I was actually selling drugs big for a time to pay for my school with it and it got to the point where the money was more important than my school.
Another man began selling drugs when he was thirteen years old and his mother left him to fend for himself.
I was doing it to eat, to live, you know. Other people had families to raise them and a house, you know. I had to do it with myself so I got in a lot of fights when I was young.
Three of the men described their drug use as self-medicating. When asked why they started using substances, they clearly identified what they believed triggered their use. They freely offered their insight into their behavior. One of the men who disclosed being sexually abused as a child said, “I self-medicated myself to the point where I won’t, I’ve never told anybody anything.” Another man used marijuana to ease his ADHD symptoms. “It was self-medication. That’s what I was doing. Self-medicating myself ’cause when I’m high, I don’t get as agitated. I’m more, I’m peaceful.”
Three participants relapsed after years of sobriety when they were prescribed pain medications for injuries. For example, Frank was given oxycontin for a back injury and began manipulating his medication. “Not going outside my prescription, per se, but breaking it for quick release, manipulating it and taking it quite a bit.” Incidentally, he was using oxycontin at the time of his domestic violence arrest. All three participants denied being asked by their provider if they had problems with substance abuse. A majority of the female IPV incidents described by the participants involved the use of substances.
Theme 4: Legal issues
During their narratives, several participants discussed crimes they had committed in their youth. Two participants discussed their juvenile charges.
Another guy and I got pegged with being the leaders [of a gang], which was true . . . some of the charges were malicious destruction of property, burglary . . . They threw everything they could at me at once.
Another man described his time in the juvenile system, where violence also was prevalent. “You was fighting ’cause you was bored . . . You fight somebody and then you make up with them the next day and then later on that day, you fight ’em.” As adults, a majority of the crimes perpetrated by the participants not only included IPV but other assault charges, violations of restraining orders, and property destruction. There was one participant who was charged with animal abuse and another participant with sexual assault/abuse.
Discussion
The pattern of progression from traumatic exposure to violence perpetration has not been described in the literature. Prior studies have examined the life of perpetrators in retrospect but did not examine this progression (Anda et al., 2006; Felitti et al., 1998; Whitfield, Anda, Dube, & Felitti, 2003). The progression that emerges from the results begins when the participants had traumatic experiences in childhood. Their school performance suffered and several had mental health diagnoses. All participants developed problems with substance abuse, violence, and the legal system. None of the participants reported receiving treatment specific for their traumas.
The participants were exposed to childhood adversities, such as trauma, school/mental health problems and substance abuse, and developed problems with IPV in adulthood similar to the results of Anda et al. (2006). The ACE (Anda et al., 2006; Felitti et al., 1998; Whitfield et al., 2003) studies showed how men who were exposed to violence in childhood are more likely to perpetrate violence against intimate partners and have a shortened life span. Roberts, McLaughlin, Conron, and Koenen (2011) also found an increased risk of IPV perpetration in adults with a history of childhood exposure to violence. Their study supported the Stress Sensitization Model, which has similarities to posttraumatic stress disorder (PTSD). This model hypothesizes that traumatic events in childhood sensitize the individual to later exposures. The model suggests an adult who is sensitized will be more reactive to an adverse situation than an adult who is not sensitized, in much the same way a traumatic situation can stimulate a person diagnosed with PTSD. This model may have implications for male perpetrators as well.
Sensitization to stress is also discussed in the neurobiological literature. Van der Kolk (2003) discussed the effects of childhood trauma on brain development. Children raised in an environment of chaos or violence have limited tolerance for stress later in life and traumatic exposures alter their neurodevelopment. Mitchell and Beech (2011) and Teicher (2007) describe changes in the amygdala, orbitofrontal cortex and anterior cingulate cortex in individuals who were traumatized at sensitive periods in their development. As a result, these individuals may have trouble interpreting social cues, forming attachments, and interacting in the environment. Stress from a traumatic event sequellae may lead to structural and functioning changes in the developing brain that may increase risk of violence. Teicher (2007) measured the prefrontal cortex, frontal lobes, corpus callosum, and hippocampus of abused and nonabused subjects. The age of time of abuse was ascertained. Children who were abused at 4 years of age had a significant reduction in volume of the hippocampus, a structure important in memory. They hypothesized this time as a developmentally sensitive time in the development of this structure. The developmentally sensitive time for the corpus callosum is 10 years of age and the prefrontal cortex was most sensitive at 14 years of age. This research suggests possible reasons for differences in trauma responses depending on age of exposure. Participants, reported researchers such as Capsi et al. (2002), have attempted to hide experiencing childhood traumas at different times in their neurodevelopment and they all progressed, ultimately, to IPV perpetration.
Normalization of violence was another common factor found in this study. The participants described moderate to severe punishment as routine and did not recognize it as abusive behavior that led to their perpetration of violence against their partners. This finding is contradictory to Flinck, Astedt-Kruki, and Paavilainen (2008) where male perpetrators recognized the violence perpetrated against them in childhood and its influence on their current relationships. The sample obtained for their study did not include incarcerated men or men from the United States. These perceptions of parenting and violence may not be similar to U.S. perceptions and culture.
Child sexual abuse had a significant impact on the lives of at least three of the participants in this study. All reported normal school functioning early in their educational careers and developed significant pathology around the time of adolescence. Teicher (2007) also described the delayed effects of stress where childhood sexual abuse leads to depression that emerges in early to midadolescence. All three men experienced severe substance abuse and one participant reported attempting suicide. One man disclosed his sexual abuse to a substance abuse counselor but did not receive treatment. Another participant has been through several rounds of substance abuse treatment but still cannot identify what triggered his drug use. He never discussed his abuse with anyone, including his sibling who was victimized with him. These findings were similar to Flinck et al (2008) who found men felt mental health professionals did not listen to them or treat them for sexual abuse.
Limitations
As in qualitative studies, sample size was small, but using multiple interviews adequate in length enhanced the development of these themes relevant to the participants’ lives. The researcher has the potential to have biases about the participants and thus the interactions can influence the participants according to Gadamer’s hermaneutics. However, necessary steps, such as recording the researcher’s presumptions about IPV before commencing data collection, were completed to increase the researcher’s awareness of these preconceived notions. In addition, The second author (DS) who did not participate in the interviews reviewed all transcripts and analyses reaching agreement and consistency with the First author (MW). As it was not part of the design, there were no objective socioeconomic, psychological, or physiologic data collected during this study.
Conclusion
Male perpetrators of IPV have been treated as a homogenous group receiving standardized interventions. This qualitative study is an effort to understand the lives of male perpetrators against female partners. All participants experienced abuse, neglect, or violence exposure in childhood and exhibited similar patterns of behavior (school/mental health issues, substance abuse, and legal issues) that evolved into perpetration of IPV. Brief screening for trauma, abuse, and IPV exposure needs to be universal for all children instead of being selectively applied. Brief screens have been developed for pregnant women and The American Academy of Pediatrics (Thackeray et al. 2010) only recently recommended screening children for violence. Brief screening tools can help; however, attention to behavior patterns may indicate children at high risk for traumatic exposures. For example, the child who has an abrupt decline in school performance, begins fighting in school, or becomes oppositional may warrant closer screening. Once identified, clinicians can refer children survivors of trauma for an evidence-based therapy, such as Trauma Focused Cognitive Behavioral Therapy (Cohen, Mannarino & Deblinger, 2006) to improve their functioning.
It is also important to recognize that trauma may be normalized by males as children or adults. Screening questions given verbally, instead of a questionnaire, may more accurately identify violent exposures. Questions like “When you were punished, what did your parents do,” or “Did you ever see your parents hit each other?” may be more sensitive screens for traumatic exposures.
One third of the sampled reported child sexual abuse. Health care providers are beginning to receive more training in the recognition and treatment of child sexual abuse. However, more research is needed to understand the prevalence of male sexual abuse and how to best screen these patients. The similarities in behavior patterns for these participants who disclosed childhood sexual abuse were striking and warrant further study.
By understanding the lives of male perpetrators through their experiences of childhood traumas, clinicians can identify and treat children and families at risk for violence. Specific interventions targeting trauma in male perpetrators may be very important in decreasing the incidence of IPV. Such interventions may include cognitive processing therapy (CPT; Resick & Schnicke, 1996). Further research is needed to better understand biological changes in the brain from traumatic experiences and how these changes may influence the behaviors of IPV perpetrators. By uncovering underlying biological, psychological, and social factors that may influence male perpetrators of IPV, clinicians can make a difference in preventing further violence among this group.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.