
Abstract
The existing literature on intimate partner violence (IPV) does not paint a consistent portrait of the impact of race/ethnicity. In addition, although research has clearly demonstrated that there is a relationship between substance use and IPV, the temporal ordering of these variables is not clearly established. This article seeks to examine the temporal ordering of IPV victimization and drug use using longitudinal data with a nationally representative racially and ethnically diverse sample. Data from Wave III (2001-2002) and Wave IV (2007-2008) of the National Longitudinal Study of Adolescent Health (Add Health) will serve as Time 1 and Time 2, respectively, to answer three research questions. First, does substance use during early young adulthood (Time 1) predict IPV victimization during young adulthood (Time 2) among women? Second, does IPV victimization during early young adulthood predict substance use during young adulthood for women? Finally, do these bidirectional relationships vary by race/ethnicity (i.e., White, African American, and Latina)? Four different forms of IPV (minor violence, major violence, rape/sexual coercion, and injury) are investigated along with binge drinking, marijuana use, and other drug use. Understanding not only the temporal relationship between substance use, trauma, and IPV but also the racial and ethnic differences in these relationships is critical to developing and refining culturally sensitive trauma-informed prevention and treatment services for women.
It is estimated that 4.7 million women in the United States are physically assaulted by an intimate partner each year, and more than one in three women (35.6%) have experienced rape, physical violence, and/or stalking by an intimate partner in their lifetime (Black et al., 2011), although the overall rate of intimate partner violence (IPV) is declining (Catalano, 2012). In addition, the risk of IPV varies across the life course. Young adult women, in particular, experience the highest rates of IPV (Black et al., 2011; Catalano, 2012). In 2010, 9.7 per 1,000 women aged 18–24 experienced IPV, whereas 12.1 per 1,000 women aged 25–34 experienced IPV (Catalano, 2012). Notably, the literature does not paint a consistent portrait of the association of race/ethnicity with reported IPV. Although a number of studies indicate that the rates of IPV are higher among racial and ethnic minorities, 1 the differences are rarely statistically significant (Caetano, Schafer, & Cunradi, 2001; Catalano, Smith, Snyder, & Rand, 2009; Cho, 2012). National data show that 31.7% of White women, 40.9% of Black women, and 35.2% of Hispanic women have experienced IPV (Black et al., 2011). In an effort to explain these differential rates, some scholars have pointed to the relationship between race/ethnicity and socioeconomic status, thereby arguing that the generally higher rates of IPV among minority communities are the result of the socioeconomic disadvantage experienced by these groups (Bent-Goodley, 2007; Cho, 2012; West, 2004). Others have discussed the differing perceptions of IPV (McNeely & Torres, 2009) as well as the differential rates of disclosure and access to resources and support (Belknap, Melton, Denney, Fleury-Steiner, & Sullivan, 2009) among minorities and nonminorities. In addition, a number of scholars point to racism and the other systemized forms of oppression (Miller, 2008; Potter, 2008; West, 2004).
Moreover, research has clearly demonstrated that there is a relationship between substance use and IPV. However, the temporal ordering of these variables is not clearly established. In the few studies that have sought to investigate the temporal ordering of these variables, the results are inconsistent, the samples are not nationally representative, and the investigators failed to fully explore racial and ethnic differences in the experience of substance use and IPV. This oversight is significant given that researchers and service providers are increasingly noting the importance of accounting for and understanding violence and trauma within treatment settings (Elliott, Bjelajac, Fallot, Markoff, & Glover Reed, 2005). Understanding not only the temporal relationship between substance use and IPV but also the racial and ethnic differences in these relationships is critical to developing and refining culturally sensitive trauma-informed prevention and treatment services for women.
Intimate Partner Violence and Substance Use
As a result of the astonishing prevalence of IPV among all groups of women, a number of scholars and researchers have turned their attention to the risk factors (Jewkes, 2002; Kantor & Jasinski, 1998; Stith, Smith, Penn, Ward, & Tritt, 2004; Stuart, Moore, Hellmuth, Ramsey, & Kahler, 2006) and consequences (Max, Rice, Finkelstein, Bardwell, & Leadbetter, 2004; Meisel, Chandler, & Rienzi, 2003; Plichta, 2004) of IPV. Substance use in particular is often cited in the literature. Studies show that between 20% and 50% of all incidents of IPV occur when one or both partners are under the influence of alcohol or drugs (Hart, 2007).
Although much research has shown that substance use increases the likelihood of IPV perpetration (Caetano et al., 2001; Fals-Stewart, Golden, & Schumacher, 2003; Foran & O’Leary, 2008; Lipsky, Caetana, Field, & Larkin, 2005; Moore, Easton, & McMahon, 2011; Reingle, Staras, Jennings, Branchini, & Maldonado-Molina, 2012; Stith et al., 2004), very little research has investigated whether substance use is a risk factor for IPV victimization. This limited body of research has shown that alcohol (Waller et al., 2012), marijuana (Centers for Disease Control [CDC], 2010b), and opioid (Moore et al., 2011) use are all risk factors for IPV victimization. Different mechanisms have been identified to help explain the influence of substance use on IPV victimization. For example, substance-dependent women are more likely to have substance-dependent spouses or partners (Amaro & Hardy-Fanta, 1995; Riehman, Iguchi, Zeller, & Morral, 2003; Tuten & Jones, 2003), which may contribute to the increased likelihood of IPV victimization given the strong association between substance use and IPV perpetration among men. In addition, for substance-abusing women with substance-abusing partners, seeking treatment may create a serious problem for the relationship (McCollum & Trepper, 1995) in the sense that substance-abusing partners often discourage their female partners from entering treatment and sometimes even threaten violence or threaten to leave the relationship (Amaro & Hardy-Fanta, 1995). Moreover, substance-abusing women are more likely to enter into dependent relationships dominated by their partners (Woodhouse, 1992), which may hinder their ability to perform basic life skills such as managing money and planning for the future (Brady & Ashley, 2005), leaving them entirely dependent on their partners and making it that much more difficult to leave abusive relationships. Notably, these explanations do not take the blame away from the perpetrator and are certainly not intended to insinuate that victims of IPV are at fault for their victimization (see Kaufman-Kantor & Straus, 1987). Nevertheless, the CDC does recognize substance use as a potential individual risk factor for IPV victimization (CDC 2010b).
Substance use is also often cited as a consequence of IPV victimization. For instance, longitudinal studies found that IPV is associated with higher rates of drug abuse (Roberts, Klein, & Fisher, 2003), heavy drinking (Martino, Collins, & Ellickson, 2005), and general substance use (Carbone-López, Kruttschnitt, & Macmillan, 2006; Zweig, Yahner, & Rossman, 2012). In addition, researchers found that poor and homeless single mothers with histories of IPV had nearly three times the odds of using illicit drugs (Salomon, Bassuk, & Huntington, 2002). The most common explanation provided for substance use as a consequence of victimization is that women use alcohol or other drugs in an effort to self-medicate (McFarlane, 1998) and cope with these traumatic events (Kayson et al., 2007; Miranda, Meyerson, Long, Marx, & Simpson, 2002). As such, the CDC also lists substance use as a consequence of IPV (CDC 2010a).
A handful of studies have attempted to determine whether substance use is best understood as a risk factor or a consequence of IPV victimization by investigating the temporal ordering of these variables. For example, according to a longitudinal study of 416 women on methadone, the relationship between frequent drug use and IPV is bidirectional and varies by type of drugs. Specifically, frequent drug use increases the likelihood of subsequent IPV among crack and marijuana users. However, the experience of IPV also increases the likelihood of subsequent frequent drug use among heroin users (El-Bassel, Gilbert, Wu, Go, & Hill, 2005). Similarly, a longitudinal community-based study in Buffalo, New York, surveying 724 heterosexual women found that within ongoing relationships, women’s use of hard drugs was associated with increased odds of experiencing IPV over the next 12 months. In addition, the experiences of IPV were modestly associated with subsequent heavy episodic drinking but not with subsequent drug use (Testa, Livingston, & Leonard, 2003).
Although the existing literature has clearly demonstrated that there is a relationship between substance use and IPV, researchers have primarily focused on perpetrators rather than victims. Even in studies focusing specifically on victims, the temporal ordering of these variables is not well understood. Therefore, to more accurately examine the temporal ordering of IPV victimization and substance use, longitudinal data with a nationally representative racially and ethnically diverse sample is needed. In this paper, we use data from Wave III (2001-2002), when the respondents are 18 to 26 years old, and Wave IV (2007-2008), when respondents are 24 to 32 years old, of the National Longitudinal Study of Adolescent Health (Add Health), which serve as Time 1 and Time 2, respectively, to answer three research questions.
Four different forms of IPV (minor violence, major violence, 2 rape/sexual coercion, and injury) are investigated, along with binge drinking, marijuana use, and other drug use. This study is significant in that we focus on the age periods of early young adulthood and young adulthood among women as these are the most vulnerable segments of the population (Black et al., 2011; Catalano, 2012).
Method
Data from the Add Health Wave III and Wave IV in-home interview were analyzed. Add Health examines health and health-related behaviors including personal traits, families, friendships, romantic relationships, peer groups, schools, neighborhoods, and communities among a nationally representative sample of adolescents in 7th through 12th grade. In 1994, 90,000 adolescents from 134 schools completed questionnaires. A subset of respondents later participated in four in-home interviews at Wave I (1994-1995), Wave II (1996), Wave III (2001-2002), and Wave IV (2007-2008). During Wave IV data collection, 92.5% of the sample was relocated and 80.3% of eligible sample members were interviewed yielding a sample size of 15,701. The sample size of women is 8,352. Survey data were collected in the respondents’ homes using a 90-min CAPI/CASI instrument. A total of 2,959 self-identified White, African American, and Latina women who completed the relationship section for a current male partner in Wave III and Wave IV were included.
Measures
Demographic control variables used in this study include age and marital status (not married 0, married 1). Socioeconomic status is represented by three variables: highest level of education (0 less than high school to 3 college graduate), employment (0 unemployed, 1 part-time, 2 full-time), and personal income measured with eight categories ranging from less than $10,000 to $75,000 or more. Dummy variables for race/ethnicity include White, African American, and Latina.
IPV is measured at Time 1 during early young adulthood and Time 2 during young adulthood by assessing four dimensions of IPV during the year prior to the interview: minor violence, major violence, rape/sexual coercion, and injury. A dummy variable was created for no = 0 or yes = 1. Minor violence is examined by asking, “How often does your current partner threaten you with violence, push or shove you, or throw something at you that could hurt?” Major violence is examined by asking, “How often does your current partner slap, hit, or kick you?” The question, “How often has your current partner insisted on or made you have sexual relations with him when you didn’t want to?” assesses rape/sexual coercion. Finally, the question, “How often have you had an injury, such as a sprain, bruise, or cut because of a fight with your current partner?” assesses injury.
Substance use is represented by three bivariate measures (0 = no, 1 = yes). Binge drinking is defined as drinking five or more drinks during a single occasion at least two to three times a month in the past year. Marijuana use and drug use (MDMA, inhalants, LSD, heroin, PCP, or other illegal drugs) include any use within the past 12 months.
Analysis
The Pearson chi-square and one-way analysis of variance (ANOVA) were conducted to assess the differences among race/ethnic groups on all measures included in the analysis. Multivariate logistic regression analyses were run for the total sample and within race/ethnic groups to examine each of the bivariate outcomes. Separate models regressed Time 2 substance use on Time 1 IPV controlling for Time 1 substance use and the demographic and socioeconomic variables. Similarly, separate models regressed Time 2 IPV on Time 1 substance use controlling for Time 1 IPV and the demographic and socioeconomic variables. All data are weighted to reflect the complex sampling design of the study.
Findings
Table 1 shows the frequencies of all study variables by race/ethnicity. At Time 1, these women are in early young adulthood with an average age of 22, and at Time 2, they are in young adulthood with an average age of 29 (not shown). Compared with other women, Latinas are slightly older, more likely to be married, and more likely to have lower levels of education. African American women are more likely to be unemployed and less likely to be employed full-time. The modal and mean response for income corresponds to the category $10,000 to $14,999 for each race/ethnic group.
Frequencies of Study Variables by Race.
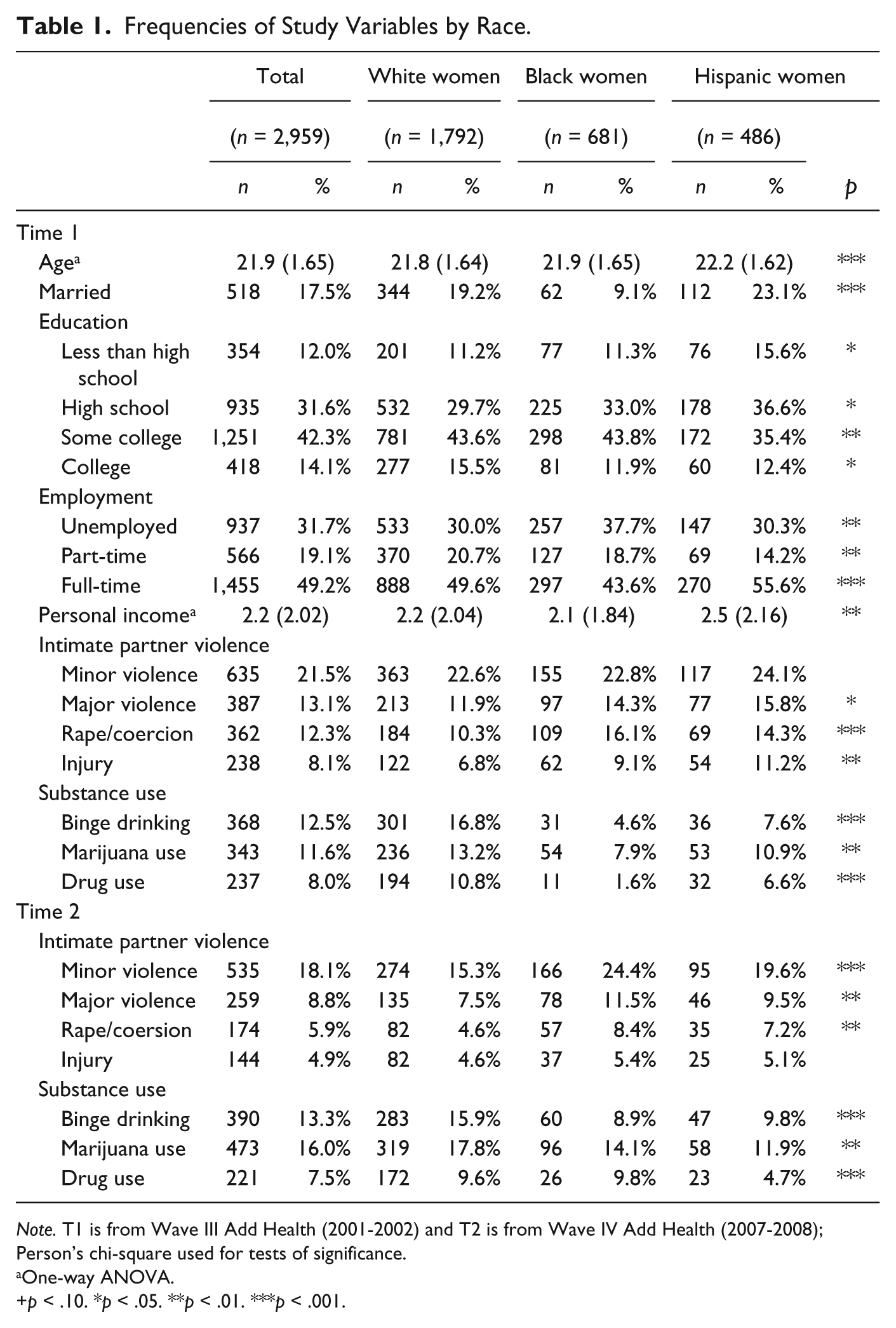
Note. T1 is from Wave III Add Health (2001-2002) and T2 is from Wave IV Add Health (2007-2008); Person’s chi-square used for tests of significance.
One-way ANOVA.
p < .10. *p < .05. **p < .01. ***p < .001.
Overall, 27.5% of women report experiencing some form of IPV during early young adulthood, and 20.8% of women report experiencing some form of IPV during young adulthood (not shown). During early young adulthood, Latinas have a higher prevalence of IPV, excluding rape/sexual coercion, compared with White and African American women. African American women have a higher prevalence of rape/sexual coercion, compared with White and Latina women. However, during young adulthood African American women have a higher prevalence of IPV in all categories compared with White and Latina women. There is a decrease in the prevalence of IPV from early young adulthood to young adulthood for each group of women. However, there is one exception: African American women reported a slight increase in minor violence (22.8% to 24.4%). In general, White women reported lower levels of IPV during both time periods compared with African American and Latina women with the most striking difference being the prevalence of minor violence during young adulthood. Fifteen percent of White women (15.3%) reported experiencing minor violence compared with 24.4% of African American and 19.6% of Latina women.
During early young adulthood and young adulthood, White women have a higher prevalence of substance use including binge drinking, marijuana use, and drug use, compared with African American and Latina women. Across the two time periods, rates of use remained about the same for White and Latina women. However, for African American women, prevalence of use doubled for binge drinking and marijuana use while drug use increased from 1.6% to 9.8% to be about the same as White women (9.6%).
With regard to the first research question, we find that all forms of IPV are associated with later marijuana use (Table 2). Specifically, experiencing minor violence during early young adulthood increases the odds of marijuana use during young adulthood by a factor of almost 2 (odds ratio[OR] = 1.9, 95%, confidence interval [CI] = [1.40, 2.58]). Similar results were found for major violence (OR = 2.0, CI = [1.40, 2.85]), while rape/coercion (OR = 1.4, CI = [0.97, 2.08]) and injury (OR = 1.5, CI = [0.93, 2.26]) were only marginally associated with later marijuana use. Intimate partner violence during early young adulthood was not associated with later binge drinking or drug use although minor violence was marginally associated with drug use (OR = 1.5, CI = [0.95, 2.21]).
Odds Ratios From Regressing T2 Substance Use on T1 Intimate Partner Violence by Race.
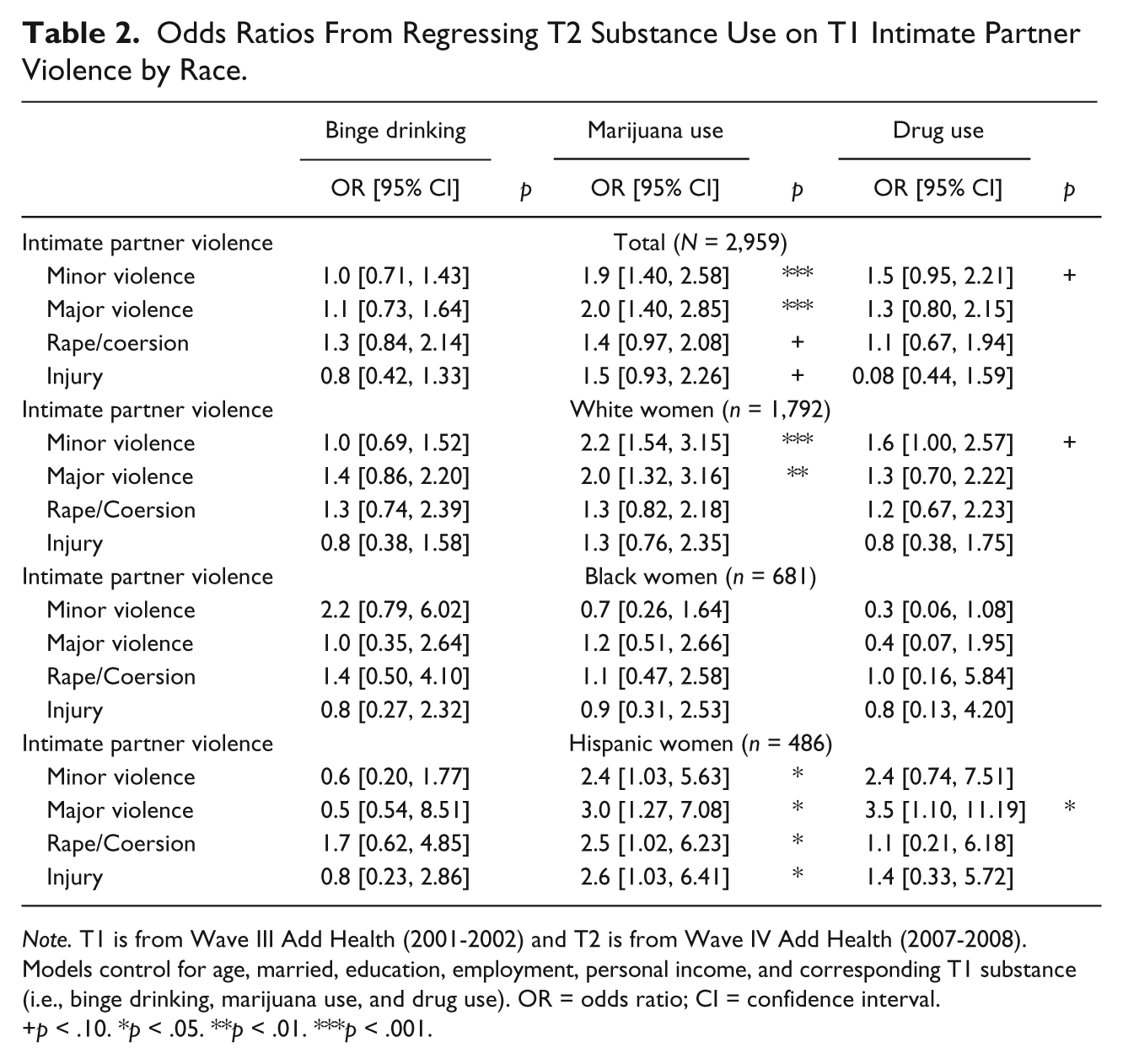
Note. T1 is from Wave III Add Health (2001-2002) and T2 is from Wave IV Add Health (2007-2008). Models control for age, married, education, employment, personal income, and corresponding T1 substance (i.e., binge drinking, marijuana use, and drug use). OR = odds ratio; CI = confidence interval.
p < .10. *p < .05. **p < .01. ***p < .001.
With regard to the second research question, we find that substance use is not associated with later IPV victimization when examining the whole sample of women (Table 3).
Odds Ratios From Regressing T2 Intimate Partner Violence on T1 Substance Use by Race.
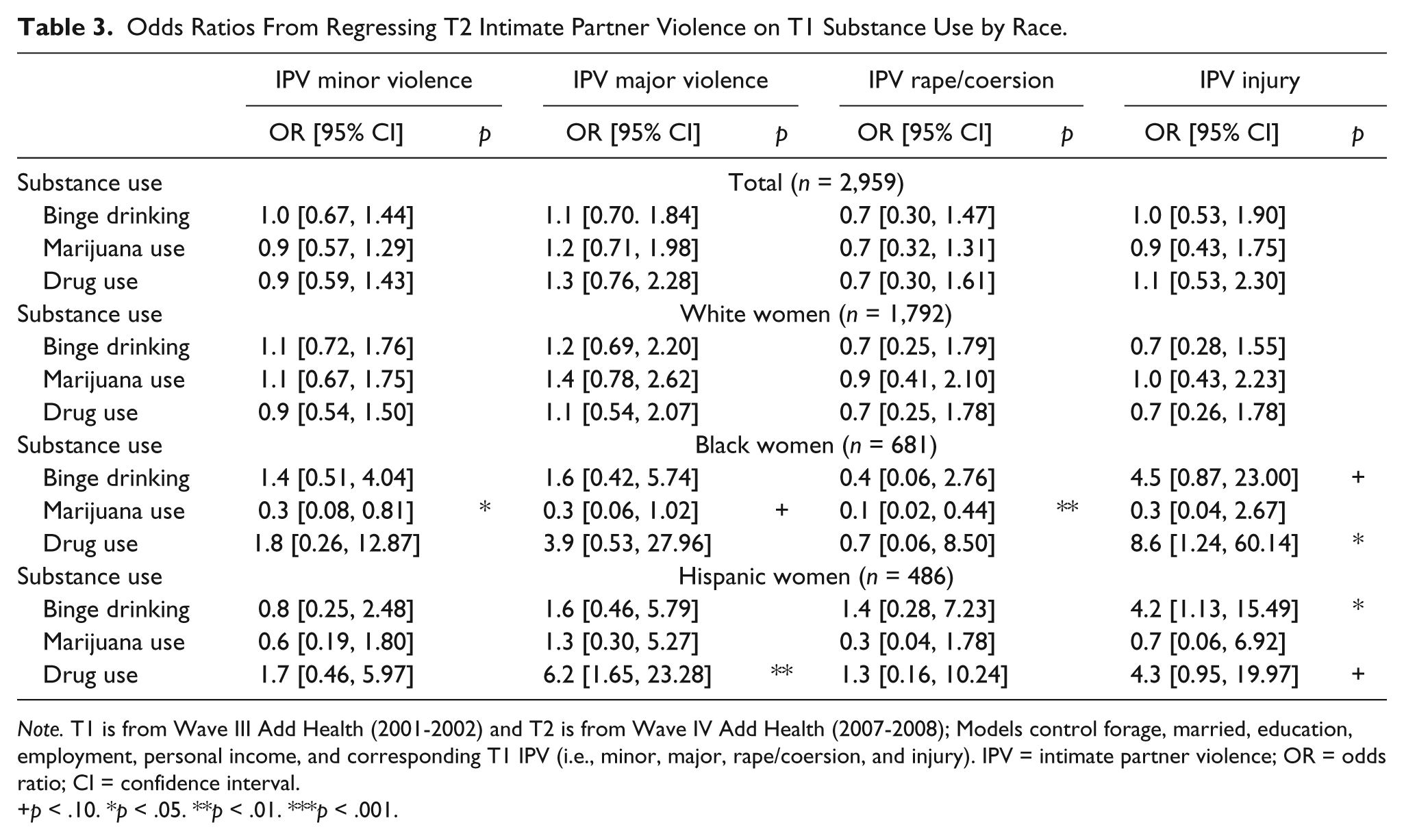
Note. T1 is from Wave III Add Health (2001-2002) and T2 is from Wave IV Add Health (2007-2008); Models control forage, married, education, employment, personal income, and corresponding T1 IPV (i.e., minor, major, rape/coersion, and injury). IPV = intimate partner violence; OR = odds ratio; CI = confidence interval.
p < .10. *p < .05. **p < .01. ***p < .001.
The third research question asks, “Do these bidirectional associations vary by race/ethnicity?” The separate models reveal distinct racial and ethnic differences. Table 2 shows that IPV during early young adulthood is not associated with later binge drinking for any of the different race/ethnic groups. Similarly, only major violence during early young adulthood is associated with an increase in the odds of using drugs during young adulthood for Latina women (OR = 3.5, CI = [1.10, 11.19]) although minor violence is marginally associated (p < .10) with increased odds of using drugs for White women (OR = 1.6, CI = [1.00, 2.57]). However, experiencing all forms of IPV increases the odds of using marijuana during young adulthood by a factor of 2.4 to 3.0 for Latinas. For White women, minor violence (OR = 2.2, CI = [1.54, 3.15]) and major violence (OR = 2.0, CI = [1.32, 3.16]) during early young adulthood increase the odds of using marijuana. None of the forms of IPV is associated with future substance use for African American women.
Table 3 shows that binge drinking during early young adulthood increases the odds of experiencing injury related to IPV during young adulthood for Latinas by a factor of four (OR = 4.2, CI = [1.13, 15.49]) and marginally (p < .10) for African American women (OR = 4.5, CI = [0.87, 23.00]). For drug-using Latinas, the odds of experiencing major violence increase by a factor of six (OR = 6.2, CI = [1.65, 23.28]) and the odds of experiencing IPV resulting in injury increase by a factor of four (OR = 4.3, CI = [0.95, 19.97]), although this is only marginally associated (p < .10). However, drug use is strongly associated with injury by IPV (OR = 8.6, CI = [1.24, 60.14]) for African American women. Finally, the African American women’s use of marijuana during early young adulthood is marginally (p < .10) associated with decreased odds of experiencing multiple forms of IPV including minor violence (OR = 0.3, CI = [0.08, 0.81]), rape/sexual coercion (OR = 0.1, CI = [0.02, 0.44]), and major violence (OR = 0.3, CI = [0.06, 1.02]). Substance use is not associated with any form of subsequent IPV for White women.
Discussion
Our findings contribute to the literature on the bidirectional relationship between substance use and IPV. Specifically, this study examined whether (a) experiencing IPV during early young adulthood was associated with later substance use during young adulthood, (b) whether substance use during early young adulthood was associated with later IPV during young adulthood, and (c) whether these relationships vary by race/ethnicity. We found that for women who experience different forms of IPV—minor (threaten, push, or throw something at you) and major (slap, hit, or kick you) violence, rape/coercion, and violence leading to injury—their odds of later marijuana use increase by a factor of 1.4 to 2.0. In addition, for women who experience minor forms of violence, their odds of later drug use increase by a factor of 1.5. Experiencing IPV was not associated with later binge drinking.
Moreover, distinct racial differences in the association between IPV during early young adulthood and substance use during young adulthood did emerge. For instance, none of the forms of IPV victimization is associated with later substance use for African American women even though their prevalence of substance use increased substantially between early young adulthood and young adulthood (binge drinking 4.6% vs. 8.9%; marijuana use 7.9% vs. 14.1%; drug use 1.6% vs. 9.8%) while White and Latina women decreased or only slightly increased their use. Yet, for White and Latina women, different forms of IPV victimization are associated with later marijuana and drug use. This suggests that different subgroups of women may have different coping strategies for their abuse. This finding is similar to one study that found that Asian American women were most at risk for problem drinking if they had experienced an alcohol-related sexual assault compared with White women (Nguyen, Kaysen, Dillworth, Brajcich, & Larimer, 2010). In addition, the dramatic increase in substance use for African American women may be a coping response to other stressors. These findings only consider physically violent forms of intimate partner abuse. Research that includes psychological/emotional abuse and other nonphysical forms of violence might produce different results.
Second, this study found that substance use during early young adulthood is not a risk factor for experiencing IPV during young adulthood for women. However, when examining distinct racial/ethnic groups of women, some interesting associations emerged. For instance, substance use during early young adulthood is not associated with any form of IPV victimization during young adulthood for White women even though White women have a higher prevalence of substance use during both the time periods compared with African American and Latina women. Alternatively, binge drinking and drug use increase the odds of experiencing different forms of IPV for Latina and African American women. In fact, drug use during early young adulthood increases the odds of IPV leading to injury during young adulthood for African American women by a factor of 8.6 and increases the odds of minor violence and IPV leading to injury for Latina women by factors of 6.2 and 4.3, respectively. Although substance abuse and dependence are not examined in the present study, some research suggests that while White women are more likely to engage in illicit drug use (McCabe et al., 2007; Substance Abuse and Mental Health Data Archive [SAMHDA], 2010), minorities such as African Americans and Latinas may be more likely to be dependent on or abuse illicit drugs (McCabe et al., 2007), although research in this area is not consistent (Compton, Thomas, Stinson, & Grant, 2007). As such, the differing problematic use of alcohol and other drugs may help to explain this finding. However, African American women who use marijuana have decreased the odds of experiencing all types of IPV even through binge drinking and drug use increase their odds of sustaining an injury related to IPV. It is possible that the negative association between marijuana use and IPV is due to the different pharmacological and behavioral effects of various substances. For example, previous research has found that the experiences and subcultural norms associated with marijuana use appear to be much less detrimental to relationship harmony among inner city couples (Golub, Dunlap, & Benoit, 2010).
There are several important limitations that need to be considered. First, a major limitation of this study is the time interval between baseline and follow-up (about 6 years), which may contribute to a potentially spurious relationship between substance use and IPV victimization especially when considering research that has identified substance use as a situational-level risk factor for IPV victimization (Valdez & Flores, 2005). Second, even though some women reported experiencing multiple forms of IPV in the past year, our study did not address this. We feel that this is outside the scope of the current study because the research questions focus on the relationships between different forms of IPV and different types of substance use. Third, the past year measures of substance use and IPV are self-reported, which can be unreliable. However, this is common to most observational research using survey data. Self-report bias may have been reduced in this case because more sensitive questionnaire sections were self-administered using CASI technology. A fourth limitation associated with using secondary data is that the four items assessing IPV do not include more serious violence such as chocking and striking with an object or more serious injuries such as broken bones, gunshot wounds, and loss of consciousness. It is possible that a stronger relationship between substance and IPV would be present for more serious forms of IPV. Finally, we do not account for the temporal sequence between substance use and IPV during Time 1; that is, we do not account for the time of onset for substance use and IPV. Our study focuses exclusively on 1-year periods during early young adulthood and young adulthood. Therefore, it is possible that women experienced substance use and/or IPV during the years not included in the study. This is an important limitation yet one that is difficult to address using secondary data. We attempted to address this concern by adding additional Time 1 controls. For example, when examining the association between experiencing rape/sexual coercion at Time 1 and binge drinking at Time 2, binge drinking at Time 1 was added as a statistical control.
In sum, this study confirms the IPV prevalence rates cited in other studies (Black et al., 2011; Catalano, 2012) and clearly demonstrates that there are varying rates of IPV among different racial and ethnic groups. This study also found substance use to be a risk factor and a consequence of IPV victimization. However, the association varies by type of substance use and IPV, as well as by race/ethnicity; that is, the relationship between alcohol and other drug use and IPV victimization is complex. Our findings can help develop and refine culturally sensitive trauma-informed prevention and treatment services for women that account for the unique experiences of different subgroups of women. For instance, it appears that White and Latina women engage in substance use as a response to earlier IPV. This pattern of use can be addressed in treatment by introducing women to healthier coping behaviors. For African American women, however, more research is needed to determine the way these women cope with the experience of IPV, as IPV does not increase the odds that they will turn to substances to cope. In addition, for women of color, it appears that substance use is a risk factor for later IPV. However, given the potential for spuriousness, more research is needed to document the mechanisms that link substance use across these specific periods of the life course. Nonetheless, these findings can benefit substance-use treatment programs by focusing on risk reduction for IPV among women of color in treatment.
Footnotes
Acknowledgements
The authors would like to thank Joanne Belknap and the anonymous reviewers for their helpful critiques and suggestions.
Authors’ Note
A previous version of this article was presented at the 2012 annual meeting of the Society for the Study of Social Problems (SSSP). This study used data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kathryn M. Nowotny received support from the NIH, NIDA training Grant R25 DA026401.