
Abstract
Disruptions within interpersonal relationships are often cited as a symptom of secondary traumatic stress (STS) and vicarious trauma among mental health therapists. However, the primary evidence to support these claims is based on theoretical explanations and limited descriptive data. The current study sought to test the theoretical model of STS and to extend prior research by directly measuring interpersonal and sexual disruptions and their association with STS symptomology. The study hypothesized that mental health therapists with higher levels of intrusion, avoidance, and arousal symptoms would also report disruptions in their interpersonal relationships. A total of 320 licensed mental health therapists completed the online study questionnaire. Results of the current study were mixed. Higher levels of STS symptoms showed a significant association with lower relationship satisfaction, lower social intimacy, less use of constructive communication patterns, and more use of avoidance communication and demand-withdrawal communication patterns. These relationships remained after controlling for gender, years of counseling experience, and exposure level to trauma clients. However, no association was found between STS, sexual activity interest, and sexual relationship satisfaction. Implications of these findings are reviewed.
Therapists who provide psychological treatment to victims of trauma frequently encounter vivid descriptions of traumatic events, unsettling accounts of human cruelty and abuse, and direct witnessing of strong emotional expressions from their clients (Figley, 1995b; Pearlman & Saakvitne, 1995a; Resick & Calhoun, 2001). Many consider this type of exposure to traumatic material indirectly from clients to be an occupational hazard of conducting clinical work with traumatized populations (Bride, 2004, 2007; Deighton, Gurris, & Traue, 2007; Figley, 1995b; Kassam-Adams, 1995). In a survey of 446 female psychotherapists, 72% reported exposure to graphic details of trauma either “sometimes” or “frequently” in their work with clients (Brady, Guy, Poelstra, & Brokaw, 1999). In a separate survey of 221 mental health professionals, 69.6% reported moderate to profound amounts of exposure to traumatic material (Kadambi & Truscott, 2004). As a result, therapists may be at risk of developing their own trauma-related symptoms, including profound changes in personal functioning and the emergence of clinical symptoms (Figley, 2002; McCann & Pearlman, 1990; Pearlman & Saakvitne, 1995a).
The impaired psychological and physical response to trauma exposure by therapists was first recognized by Figley (1983) and labeled secondary catastrophic stress. Today in the literature, the psychological community commonly refers to this phenomenon as either vicarious traumatization and/or secondary traumatic stress (STS; Bride, 2007; Dunkley & Whelan, 2006; Newell & MacNeil, 2010). Vicarious traumatization is the terminology used most often when referring to alterations that occur in the cognitive schemas of trauma therapists. Cognitive schemas constitute thoughts, beliefs, and interpretations about one’s self, others, and the world, and in regard to vicarious trauma, the cognitive schemas of safety, trust, esteem, control, and intimacy are viewed as most vulnerable. It is believed that exposure to trauma clients and their trauma experiences fundamentally alter how therapists construct these five core schemas (McCann & Pearlman, 1990, 1991). In contrast, STS is the terminology used most often when referencing the presence of intrusion, avoidance, and arousal symptoms. STS Disorder is conceptualized to mirror that of Post-Traumatic Stress Disorder (PTSD) apart from the source of the trauma being the client’s trauma, rather than the therapist’s own (Figley, 1983).
To date, research on vicarious trauma and STS has focused predominantly on the measurement of these two clusters of symptoms, with more compelling evidence emerging for the presence of elevated intrusion, avoidance, and arousal symptoms as part of STS among trauma therapists (Adams, Matto, & Harrington, 2001; Arvay & Uhlemann, 1996; Bober & Regehr, 2006; Bride, 2007; Chrestman, 1995; Cunningham, 2003; Ghahamanlou & Brodbeck, 2000; Kadambi & Truscott, 2004; McLean, Wade, & Encel, 2003; Pearlman & MacIan, 1995; Schauben & Frazier, 1995; VanDeusen & Way, 2006; Way, VanDeusen, Martin, Applegate, & Jandle, 2004).
Relevant literature however also identifies disruptions within interpersonal relationships as symptoms of STS and vicarious traumatization (Collins & Long, 2003; Dutton & Rubinstein, 1995; Yassen, 1995). These assertions in the literature regarding the occurrence of interpersonal disruptions primarily cite anecdotal accounts or reference back to theory as evidence (Canfield, 2005; Figley, 2002; Herman, 1992; Maltz, 1991; McCann & Pearlman, 1990; Pearlman, 1995; Pearlman & Saakvitne, 1995b; Rosenbloom, Pratt, & Pearlman, 1995). Empirically, there is little evidence to support these claims (Marmaras, Lee, Siegel, & Reich, 2003; Sabin-Farrell & Turpin, 2003).
Among the research that is available, only limited descriptive information has been reported. In their survey of 215 mental health professionals, Follette, Polusny, and Milbeck (1994) reported that 24.2% utilized “withdrawing from others” as a coping strategy when working with child sexual abuse survivors. Rich (1997) surveyed 135 therapists and health professionals who worked with trauma clients and who also self-identified as vicariously traumatized. Within this group, 35.7% reported feeling “removed from friends and family,” and 36.1% felt that their sex lives were less satisfying since starting their work as a trauma therapist.
More recently, a study of 515 mental health social workers found that over half of the sample (53.3%) felt that secondary trauma was having a “negative effect” on their personal and professional lives (Ting, Jacobson, Sanders, Bride, & Harrington, 2005). Finally, Bride (2007) found that in a sample of 294 social workers, 23.3% reported feeling “detached from others” in their lives as a symptom of STS. No prior studies have been located that specifically address the interpersonal disruptions experienced by mental health therapists as part of the symptomology of vicarious traumatization and STS.
Research to date has largely ignored interpersonal disruptions. Instead, researchers have focused primarily on the measurement of cognitive schema disruptions and intrusion, avoidance, and arousal symptomology. Given the theoretical premise that includes interpersonal disruptions as part of the vicarious trauma and STS response, this omission needs to be addressed. The present study addresses this omission by examining disruptions in interpersonal functioning among mental health therapists who also reported intrusion, avoidance, and arousal symptoms indicative of STS. Intrusion, avoidance, and arousal symptoms were selected due to the stronger evidence base related to these symptoms at this time. In addition, demographic variables of gender, years of counseling experience, and exposure to trauma clients were included due to their association with elevated levels of STS in prior research (Adams et al., 2001; Bober & Regehr, 2006; Chrestman, 1995; Deighton et al., 2007; Kassam-Adams, 1995; McLean et al., 2003; Schauben & Frazier, 1995; Sprang, Clark, & Whitt-Woosley, 2007; Way et al., 2004). It was hypothesized that mental health therapists with elevated levels of STS symptoms would also report more disruptions in their interpersonal relationships in the areas of relationship satisfaction, social intimacy, communication patterns, sexual activity interest, and sexual relationship satisfaction.
Method
Participants
The age range for study participants was 25 to 89 with a mean age of 51.20 (SD = 12.26). The mean number of years in practice for participants was 17.84 (SD = 11.20) with a range of 1 year to 55 years in practice. The participants’ current caseload averaged 56.13% trauma clients, and participants on average conducted 43.87 hours (SD = 36.60) of therapy with trauma clients within the prior month of completing the survey. A total of 67 participants identified as male, 249 identified as female, one participant identified as transgendered, and three participants failed to identify their gender. The self-identified ethnicities for participants in this study were 91.5% European American, 2.5% Latina/Latino, 2.8% African American, 0.3% Multi-racial, 0.6% Asian American, 0.3% American Indian, and 1.9% “Other.” The majority of participants (63.6%) identified their highest education level as a master’s degree (MA, MS, MEd, MSW) followed by 28.5% of participants with a PhD, 6.9% with a PsyD, and 0.9% with a Medical Degree.
Procedure
Following university Institutional Review Board (IRB) approval, the researcher identified study participants through the following organizations: the American Mental Health Counselors Association, the Nebraska Counseling Association, the Nebraska Psychological Association, members of APA Division 42 (Psychologists in Independent Practice), members of APA Division 56 (Trauma Psychology), members of the EMDR Association, and professionals via community mental health centers in Kansas and Nebraska. Individuals self-selected to participate in the current study and, per email instructions, accessed a web-based survey site that met industry standards for Internet security as well as IRB standards for the protection of human subjects. Participants completed a total of five measures, including one demographic questionnaire.
A total of 417 individuals participated in the study between January and June 2009. Of this group, 35 respondents were excluded because of the inability to determine study eligibility. An additional 56 respondents were excluded because they failed to hold a professional license, failed to meet minimum education criteria, or were not actively seeing clients. Finally, six respondents were not eligible for the study because they were not currently in a romantic relationship. The final sample for the study was 320 licensed mental health professionals. To achieve a power of .95 with a medium effect size (.15) and an alpha of .05, a sample size of 132 was needed to detect a significant model (Erdfelder, Faul, & Buchner, 1996).
Measures
Secondary Traumatic Stress Scale (STSS)
The STSS (Bride, Robinson, Yegidis, & Figley, 2003) is a 17-item, self-report instrument designed to measure intrusion, avoidance, and arousal symptoms in practitioners who have experienced traumatic stress through their clinical work with traumatized clients. A 5-point Likert-type scale is used for responses ranging from 1 (never) to 5 (very often). Sample items for the STSS include (1) “I had trouble sleeping,” (2) “I was less active than usual,” and (3) “I was easily annoyed.” Full scale and subscale scores are obtained by summing the respective items for each scale, with higher scores representing greater severity of PTSD symptoms due to STS.
Bride (2007) suggests using interpretative categories based on percentiles. Scores at the 50th percentile or below are interpreted as little to no STS, scores at the 51st to 75th percentile are mild STS, scores at the 76th to 90th percentile are moderate STS, scores at the 91st to 95th percentile are high STS, and scores above the 95th percentile are severe STS. Bride (2007) suggests that the score at the lower end of the moderate range (76th to 90th percentile) serve as the cut-off point for determining PTSD due to STS. In Bride (2007), a sensitivity of .93 and a specificity of .91 was obtained with this approach in accurately identifying those who met core criteria for PTSD. In the current study, the Cronbach’s alpha coefficient was .91 for the Full STSS, .73 for the Intrusion subscale, .82 for the Avoidance subscale, and .80 for the Arousal subscale.
Relationship Assessment Scale (RAS)
The RAS (Hendrick, 1988) is a seven-item self-report instrument designed to measure global satisfaction in romantic relationships (Vaughn & Matyastik Baier, 1999). Individual item responses range from 1 (poorly) to 5 (extremely well) on a 5-point Likert-type scale. All seven items are summed to obtain the total scale score, with a possible total score range of 7 (low satisfaction) to 35 (high satisfaction). Sample items include (1) “How well does your partner meet your needs?” and (2) “How much do you love your partner?” In the current study, the Cronbach’s alpha coefficient was .92.
Miller Social Intimacy Scale (MSIS)
The MSIS (Miller & Lefcourt, 1982) is a 17-item, self-report instrument designed to assess intimacy in adult relationships by measuring intimate behaviors (6 items) and intensity of emotions within the relationship (11 items). Respondents indicate on a 5-point, Likert-type scale from 1 (very rarely or not much) to 5 (almost always or a great deal), which best describes their current intimate relationship. Sample items include (1) “How often do you show him/her affection?” (2) “How often are you willing to understand his/her feelings?” and (3) “How important is it to you that he/she show you affection?” The overall score is the sum of items 1 through 17 with higher scores indicating a greater amount of social intimacy in the relationship. In the current study, the Cronbach’s alpha coefficient was .92.
Communication Patterns Questionnaire (CPQ)
The CPQ (Christensen & Sullaway, 1984) is a self-report questionnaire that aims to measure an individual’s perception of communication within an intimate relationship during three phases of conflict discussion (the presentation of a problem, the discussion of a problem, and post discussion of a problem). Respondents rate each item on a 9-point, Likert-type scale, indicating the likelihood of the particular pattern occurring when addressing a problem in the relationship (1 = very unlikely, 9 = very likely).
The current study used three subscales from the CPQ, including Mutual Constructive Communication (MCC), Mutual Avoidance and Withholding (MAW), and Total Demand-Withdrawal Communication (DWC). A total of 16 items were included, with higher subscale scores indicating the higher likelihood of the particular pattern occurring when engaged in a conflict discussion. Sample items include (1) “When some problem in the relationship arises, both members avoid discussing the problem”; (2) “During a discussion of a relationship problem both members express their feelings to each other”; and (3) “After a discussion of a relationship problem, both withdraw from each other after the discussion.” In the current study, the Cronbach’s alpha coefficients for the subscales were MCC, alpha = .78; DWC, alpha = .80; and MAW, alpha = .76.
Brief Sexual Function Questionnaire (BSFQ)
The BSFQ is a self-report inventory of sexual interest and satisfaction modified from the original Brief Sexual Function Questionnaire for Men (BSFQ-M; Reynolds et al., 1988). This study used two subscales of the BSFQ-M, the Sexual Interest Subscale (BSFQ-Interest), and the Sexual Relationship Satisfaction Subscale (BSFQ-Satisfaction) modified to use gender-neutral language. Respondents rate each item on a 7-point, Likert-type scale with higher scores indicating more interest in sexual activity or more sexual relationship satisfaction. Sample items include (1) “During the past month, how frequently have you felt sexual drive? and (2) “Overall, during the past month, how satisfied have you been with your sex life?” For the current study, the Cronbach’s alpha coefficient for the interest subscale was .86 and for the satisfaction subscale was .87.
Results
Missing Data and Tests for Violations of Assumptions
Three survey items reported missing values over 5%, and were evaluated for potential patterns (Tabachnick & Fidell, 2001). A pattern for age for two items among those cases with missing values was detected. Participants with missing values were significantly older than those without missing values; however, the magnitude of this difference was small for both items (η2 = .02). Missing values in the current study were addressed via mean value substitution (Tabachnick & Fidell, 2001). Bivariate scatterplots were reviewed to assess for violations of linearity and homoscedasticity, while skewness and kurtosis values were evaluated for normality. Three study variables displayed substantial negative skewness and were transformed using reflect and logarithm to improve the distribution.
Symptoms
Means, ranges, and standard deviations for each of the study variables are presented in Table 1. Total scores on the STSS (Bride et al., 2003) ranged from 17 to 67 with a total score mean of 32.05 (SD = 9.99).
Descriptive Statistics (N = 320).

Note. STS = secondary traumatic stress.
Correlations Among Demographic Variables and STS
Significant correlations between STS and the demographic variables of gender, years in practice, and percentage of trauma clients on the therapists’ caseloads were found. Gender showed a significant positive correlation to STS (r = .135, p < .05), while years in practice showed a significant negative correlation (r = −1.98, p < .01) to STS, and percentage of trauma clients showed a significant positive correlation (r = .173, p < .01) to STS. Being female, having fewer years of experience, and a greater number of trauma clients on the therapists’ caseloads was each associated with higher levels of STS with shared variance among these variables between 1.8% and 3.9%.
Correlations Among Symptoms
Hypothesis
The hypothesis for this study was that mental health therapists with more severe STS symptoms would also report more severe disruptions in their interpersonal relationships. This hypothesis was partially supported. Six out of the seven interpersonal functioning variables demonstrated a small correlation with STS (see Table 2). Higher levels of STS were related to lower levels of relationship satisfaction, social intimacy, constructive communication patterns, and interest in sexual activity. Higher levels of STS were also related to higher levels of avoidance communication and demand-withdrawal communication. Shared variance among STS and interpersonal functioning variables ranged from 1.2% to 9.4%. Only sexual relationship satisfaction showed no relationship to STS.
Pearson Zero-Order Correlations: STS and Interpersonal Functioning.
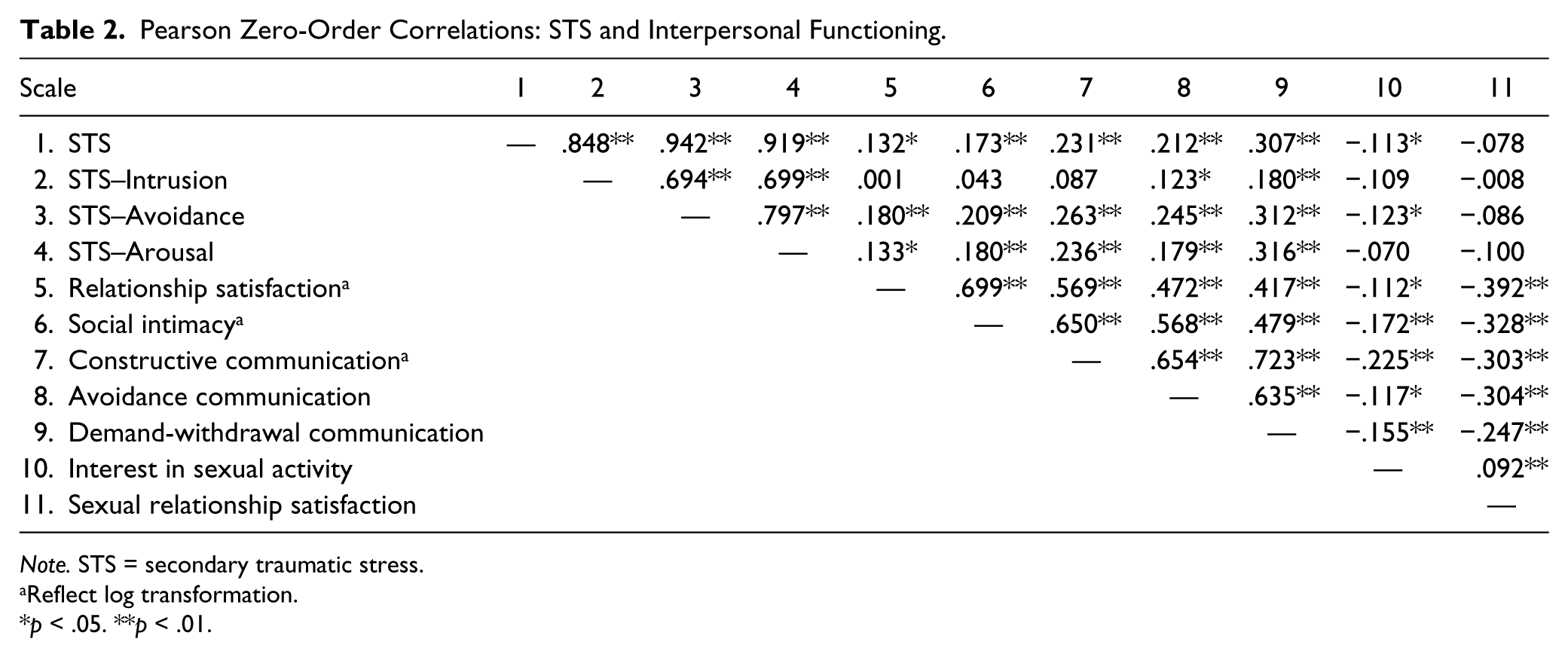
Note. STS = secondary traumatic stress.
Reflect log transformation.
p < .05. **p < .01.
Elevated levels of specific STS symptoms showed differential patterns related to interpersonal functioning. Specifically, only higher levels of intrusion symptoms showed a significant relationship with increased levels of avoidance communication and DWC patterns. A partial correlation was also conducted to explore the relationship between STS and interpersonal functioning, while controlling for the effects of gender, years in practice, and the percentage of trauma clients on the therapists’ caseloads. Partial correlations among these variables are presented in Table 3. In general, controlling for gender, years in practice, and the percentage of trauma clients on the therapists’ caseloads had very little effect on the strength of the relationships between STS and the interpersonal functioning variables. Shared variance among these variables ranged from 1.4% to 8.6%. Only interest in sexual relationship satisfaction was no longer significant, indicating that the initial relationship with STS was spurious.
Pearson Third-Order Correlations Controlling for Gender, Years in Practice, and Percentage of Trauma Clients in Caseload.

Note. STS = secondary traumatic stress.
Reflect log transformation.
p < .05 **p < .01.
Discussion
The current study hypothesized that mental health therapists with more severe STS symptoms would also report more severe disruptions in their interpersonal relationships. This study was designed to test the theoretical assumption that disruptions within interpersonal relationships are part of the expected trauma response for STS (Figley, 1995a, 1995b, 1995c, 2002). The results of the current study partially support the hypothesis. While relationship satisfaction, social intimacy, and communication pattern disruptions were each related to STS symptoms, sexual intimacy and sexual relationship satisfaction were not.
It is believed that STS symptoms that develop in therapists are often similar to those symptoms displayed by the victims they work with (Figley, 1995c). While interpersonal disruptions on the part of the clients were not measured in the current study, it is quite common for disruptions to interpersonal functioning to be part of a general trauma response for victims. Research on combat exposure has found that individuals with PTSD are at elevated risk for relationship dissatisfaction (Cook, Riggs, Thompson, Coyne, & Sheikh, 2004; Dekel & Solomon, 2006), intimacy problems (Cook et al., 2004; Riggs, Byrne, Weathers, & Litz, 1998; Roberts et al., 1982), and communication difficulties with significant others (Carroll, Rueger, Foy, & Donahoe, 1985; Cook et al., 2004). Victims of sexual and non-sexual trauma also report disruptions in relationship intimacy (Hall, 2007; Mills & Turnbull, 2004; Thelen, Sherman, & Borst, 1998). The presence of high levels of interpersonal disruptions among the therapists in the current study who also reported intrusion, avoidance, and arousal symptoms are consistent with the theoretical premise of STS.
Interpersonal disruptions specific to sexual interest and sexual relationship satisfaction, however, were not found to be associated with STS and thus do not support the study hypothesis. These results may suggest that disruptions to sexual activity interest and sexual relationship satisfaction are not part of STS symptomology. However, these results are preliminary and should be tempered with the acknowledgment that sexual functioning is broader than the two constructs of sexual interest and sexual relationship satisfaction measured in the current study (Meston & Derogatis, 2002). In addition, the scales used to assess for these constructs contained a small number of total items, which can increase measurement error and the likelihood of a Type II error.
Exposure level to trauma clients has also been studied as a relevant factor in the development of STS and is directly rooted in the theoretical assumptions of both STS and vicarious trauma. The exposure to a client’s traumatic material in session is viewed as the impetus for the therapist’s own trauma symptom development. Figley (1995c) describes an interplay between exposure to the client’s trauma and empathetic engagement with the client as the mechanisms through which a therapist comes to experience emotions and symptoms similar to his or her client. Alternatively, McCain and Pearlman (1990) outline a process based on exposure to the memories of a trauma client. The therapist subsequently internalizes these client memories resulting in alterations to the therapist’s own memory system and challenging core cognitive schemas. The threshold amount of exposure required for the development of STS symptoms is less clear. However, several studies cite more exposure to trauma clients as associated with higher levels of STS (Bober & Regehr, 2006; Brady et al., 1999; Chrestman, 1995; Creamer & Liddle, 2005; Deighton et al., 2007; Kassam-Adams, 1995; Schauben & Frazier, 1995). Findings in the current study support this trend, wherein therapists who reported a higher percentage of trauma clients on their caseloads within the past month also reported higher levels of STS symptoms.
Participants in the current study reported STS symptoms with a mean score of 32.05 (SD = 9.99). This average symptom level is not statistically different from that reported in other studies, including Bride (2007; M = 29.69, SD = 10.74), t(601) = .268, p > 1.96, and Choi (2011b; M = 32.07, SD = 10.39), t(473) = −.0019, p > 1.96. While participants in Bride (2007) and Choi (2011b) were predominantly social workers, 56.6% and 72.1% of participants were involved in direct mental health counseling. Comparatively, all participants in the present study were mental health therapists currently involved in clinical work with clients. Figley (1995b, 1995c) has identified a wide range of helping professionals as susceptible to the development of STS. Mental health therapists are considered especially vulnerable due to the empathic engagement they cultivate with their trauma clients.
Finally, previous research has reported mixed findings regarding the association of gender and years of counseling experience to STS symptoms. The general trend in the literature has been that female gender and fewer years of experience are each related to elevated levels of STS (Adams et al., 2001; Arvay & Uhlemann, 1996; Choi, 2011a; Kadambi & Truscott, 2004; McLean et al., 2003; Sprang et al., 2007; Way et al., 2004). The results of the current study support this trend.
Limitations
The results of the current study need to be interpreted within the context of several identified limitations. The operationalized definition of interpersonal and sexual disruptions by the respective measures used for each construct represents a potential limitation. Interpersonal functioning encompasses more than the isolated aspects addressed in this study (i.e., relationship satisfaction, social intimacy, and communication patterns). Likewise, sexual functioning encompasses more than the isolated aspects of sexual interest and sexual relationship satisfaction. There may be other areas of interpersonal functioning associated with STS, and this study did not assess those aspects.
Another limitation of the study is the omission of possible moderating variables such as self-care activities, general social support, and the personal trauma histories of the therapists. While changes in self-care and the loss of social support are both potential symptoms of STS, they may also serve as protective practices and could potentially moderate the overall impact of trauma client exposure (Choi, 2011a; Figley, 1995b; Sexton, 1999). A therapist’s own personal trauma history is another possible moderating variable; although, findings in the literature are currently mixed as to the overall impact a therapist’s own trauma history has on STS symptom development (Adams, Boscarino, & Figley, 2006; Adams & Riggs, 2008; Bober & Regehr, 2006; Creamer & Liddle, 2005; Deighton et al., 2007; Follette et al., 1994; Kadambi & Truscott, 2004; Kassam-Adams, 1995; Pearlman & MacIan, 1995).
The cross-sectional design of the study also presents as a limitation. The theoretical premise of STS is that interpersonal disruptions occur as symptoms along side intrusion, avoidance, and arousal symptoms. This study was unable to establish temporal sequencing to explore for the possibility of current interpersonal disruptions sensitizing a therapist to subsequent development of STS. Finally, the use of a non-random sample of mental health therapists limited the external validity of the current study. Participants in the current study were self-selected, which introduced the potential for selection bias among the study participants.
Implications
The results of the current study are relevant to both understanding and expanding current theories of STS and vicarious traumatization. Prior references to interpersonal disruptions as symptoms of STS and vicarious trauma were based on anecdotal claims and limited research. The current findings begin an empirical foundation for future research as it relates to STS and vicarious trauma theories and interpersonal disruptions as symptomology. The results are also important given that seeking interpersonal support is often cited as a key resource and coping strategy for managing the stress and pressures of a therapy practice (Baker, 2003; Coster & Schwebel, 1997; Rupert & Kent, 2007). When therapists struggle with STS and their interpersonal relationships suffer, they lose an important coping resource.
Finally, as researchers’ knowledge of the symptoms associated with STS and vicarious trauma grows, this information can inform and improve education and training practices for mental health therapists who work with trauma clients. Knowledge regarding occurrence and associated symptoms can impact how clinicians correctly identify and treat STS. The literature speculates that STS is one reason why therapists leave the mental health field prematurely (Bride, 2007). Given that fewer years of experience is related to higher symptom levels, reaching out to early career therapists with targeted training and education may be beneficial.
Suggestions for Future Research
DWC showed the strongest association with STS, accounting for 8.6% shared variance after controlling for gender, years in practice, and percentage of trauma clients in caseload. The DWC variable was the only variable in the study that addressed relationship conflict or conflict behaviors (i.e., criticizing, demanding, and nagging one’s partner). All other interpersonal variables were global assessments of satisfaction within a relationship or assessed the presence/absence of positive behaviors. Future studies need to assess specifically for relationship conflict or conflict behaviors and their association with STS.
Moreover, the current study measured intrusion, avoidance, and arousal-related symptoms as part of STS, not cognitive schema disruptions. It is possible that interpersonal and sexual disruptions show a stronger association with disruptions to cognitive schemas. McCann and Pearlman (1990, 1991) proposed that cognitive schema disruptions (in the areas of safety, trust, esteem, control, and intimacy) are hallmark symptoms of vicarious trauma.
Future research also needs to address the temporal sequencing of symptoms and the inclusion of more moderating variables. For example, social support may mitigate the development of STS or may be a factor that is altered as a result of STS. Lastly, because STS is hypothesized to develop as a cumulative result of repeated exposure to the traumatic material of clients and the empathetic engagement with clients and this material, better overall conceptualization and measurement of these constructs is needed to further refine the theories behind this phenomenon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.