
Abstract
Although infants born to adolescent mothers are at increased risk of adverse birth outcomes, little is known about contributors to birth outcomes in this group. Given past research linking partner abuse to adverse birth outcomes among adult mothers, we explored associations between pre-pregnancy verbal and physical dating violence and the birth weight and gestational age of infants born to adolescent mothers. Data from the National Longitudinal Study of Adolescent Health Waves I (1995/1996), II (1996), and IV (2007/2008) were analyzed. Girls whose first singleton live births occurred after Wave II interview and before age 20 (N = 558) self-reported infants’ birth weight and gestational age at Wave IV. Dating violence victimization (verbal and physical) in the 18 months prior to Wave II interview was self-reported. Controls included Wave I age, parent education, age at pregnancy, time between reporting abuse and birth, and childhood physical and sexual abuse. Weighted multivariable regression models were performed separately by race (Black/non-Black).On average, births occurred 2 years after Wave II interview. Almost one in four mothers reported verbal dating violence victimization (23.6%), and 10.1% reported physical victimization. Birth weight and prevalence of verbal dating violence victimization were significantly lower in Black compared with non-Black teen mothers. In multivariable analyses, negative associations between physical dating abuse and birth outcomes became stronger as time increased for Black mothers. For example, pre-pregnancy physical dating abuse was associated with 0.79 kilograms lower birth weight (p< .001) and 4.72 fewer weeks gestational age (p< .01) for Black mothers who gave birth 2 years post-reporting abuse. Physical dating abuse was unassociated with birth outcomes among non-Black mothers, and verbal abuse was unassociated with birth outcomes for all mothers. Reducing physical dating violence in adolescent relationships prior to pregnancy may improve Black adolescent mothers’ birth outcomes. Intervening on long-term violence may be particularly important.
Background
Compared with infants born to adult mothers, infants born to adolescent mothers are at increased risk of preterm birth and low birth weight (Koniak-Griffin & Turner-Pluta, 2001). Unfortunately, little is known about predictors of birth outcomes within adolescents, beyond some basic predictors such as age, body mass index (BMI), nulliparity, and smoking (Robson, Cameron, & Roberts, 2006; Stevens-Simon & McAnarney, 1993). Studies examining causes of elevated rates of infant mortality among adolescents have found that biological immaturity of the mother as well as social factors contribute to this disadvantage (Chen, Wen, Fleming, Yang, & Walker, 2008; Ekwo & Moawad, 2000; Markovitz, Cook, Flick, & Leet, 2005). Most studies of risk factors for infant preterm birth or low birth weight focus on adult mothers, or fail to distinguish between adult and adolescent mothers in their sample. In a recent study, maternal biobehavioral risk factors for preterm birth and low birth weight varied according to maternal age at birth and maternal race (Harville, Madkour, & Xie, 2012). To inform future intervention efforts, more research is required to determine social and psychological risk factors for adverse birth outcomes within this high-risk group.
Abuse by an intimate partner may be an important contributing factor to adverse birth outcomes in adolescent mothers. Although 1 in 10 adolescents in the United States experienced physical dating violence victimization in 2011 (Eaton et al., 2012), odds of physical dating abuse are estimated to be 3 to 6 times higher among adolescents having experienced pregnancy (Silverman, Raj, Mucci, & Hathaway, 2001). Psychological/emotional victimization among adolescents is even more common than physical abuse, with an estimated 30% prevalence nationally (Halpern, Oslak, Young, Martin, & Kupper, 2001).
Abuse prior to and during pregnancy may affect birth outcomes through a number of mechanisms. Direct trauma to the abdomen during pregnancy could cause fetal injury or death, as well as premature labor (Newberger et al., 1992). Victimization may also affect women’s birth outcomes through reducing access to prenatal care (Dietz et al., 1997) and/or increasing stress levels (Giscombé & Lobel, 2005). Stress can influence the likelihood a woman will engage in health-compromising behavior that adversely affects birth outcomes, such as smoking, alcohol use, or drug use (Campbell et al., 1999). Stress physiology can also impact risk for preterm delivery, through elevated levels of corticotropin-releasing hormone, cardiovascular reactivity, and reductions in immune response (Giscombé & Lobel, 2005). In addition, it has been found that women who experience dating violence are more likely to suffer from disordered eating patterns (Ackard & Neumark-Sztainer, 2002), which may affect birth outcomes through inadequate prenatal weight gain (Campbell et al., 1999). Notably, the stress and disordered eating patterns resultant from teen dating violence may continue even after dating violence has ceased. Studies document that mental health consequences of physical and emotional intimate partner violence persist for a period even after the violence ends (Blasco-Ros, Sanchez-Lorente, & Martinez, 2010; Scott-Gliba, Minne, & Mezey, 1995).
A number of studies have examined links between partner violence around the time of pregnancy and birth outcomes. Among adult mothers, physical intimate partner abuse either during or in the year prior to pregnancy has been associated with increased risk for preterm birth and low birth weight (El Kady, Gilbert, Xing, & Smith, 2005; Silverman, Decker, Reed, & Raj, 2006). Verbal abuse during pregnancy has also been related to an increased risk of low birth weight among adult mothers (Yost, Bloom, McIntire, & Leveno, 2005). In two studies of adolescent mothers, physical abuse prior to or during pregnancy was linked to preterm birth in both, but such abuse was linked to low birth weight in only one (Covington, Justason, & Wright, 2001; Curry, Perrin, & Wall, 1998).
Unfortunately, prior studies of the effects of abuse around the time of pregnancy on adolescent mothers’ birth outcomes have a number of limitations. First, they do not include an examination of verbal abuse, which could be linked to adverse birth outcomes through stress, disordered eating, or other pathways. Second, differences in effects by race were not examined, despite literature suggesting that determinants of adolescent birth outcomes may vary between Black and other mothers (Harville et al., 2012). Third, they fail to distinguish between abuse from an intimate partner versus other family members, so the unique contribution of each is unknown. Finally, they are limited in their geographic scope, so their generalizability to the wider country is unclear.
The objective of this study was to examine the relationship between pre-pregnancy verbal and physical dating abuse and adolescent mothers’ birth outcomes using data from a national sample. We also examined a number of potential mediating mechanisms, such as smoking during pregnancy, timing of prenatal care initiation, and pre-pregnancy underweight status as a proxy for disordered eating. The present study will add to prior research by examining the contribution of verbal and physical abuse, potential racial differences, and the separate impact of violence committed by partners and caretakers in the family-of-origin.
Method
Data
Data from Waves I, II, and IV of the National Longitudinal Study of Adolescent Health (Add Health) contractual dataset were utilized (Harris, 2009). Add Health is a prospective cohort study of a nationally representative sample of young persons enrolled in Grades 7 to 12 in the 1994-1995 school year (Wave I; Harris, 2011). Follow-up interviews were conducted in 1996 (Wave II), 2001 (Wave III), and 2007-2008 (Wave IV). Add Health utilized a multistage probability clustered sampling design to obtain its original Wave I sample. The first stage of sampling was a stratified, random sample of all public and private high schools in the United States. A feeder school was also recruited from each participating community. In-school surveys were attempted with all students attending participating schools; a total of 90,118 were completed. In the second Wave I sampling stage, a sample of adolescents was drawn for in-depth in-home interviews, consisting of a random core sample plus selected special oversamples; a total of 20,745 interviews were conducted at this stage. At Wave II, most students (except Wave I seniors) were eligible for re-interview; at Waves III and IV, all respondents to the Wave I in-home interview were eligible for re-interview. A total of 15,701 interviews were conducted at Wave IV (80.3% response rate). Sampling weights adjusted for unequal probabilities of selection into the original sample and for loss to follow-up. The original Add Health study was approved by the Institutional Review Board (IRB) at the University of North Carolina at Chapel Hill; the present secondary analysis was deemed exempt from review by the Tulane University Biomedical IRB.
We applied a number of inclusion criteria for our analyses. First, we limited to females who participated in Wave IV, as that was the only Wave by which all respondents had completed their teenage years and thus had complete data on teen births. Second, we limited our analysis to female participants with valid sampling weights to make generalizations to the wider U.S. population, and to adjust for attrition across waves. Third, we limited to females whose first births occurred during adolescence and after Wave II to ensure the temporal ordering of predictors and outcomes. Fourth, we limited analyses to first singleton live births (n = 655). Finally, we limited to females with complete information on all covariates. This left us with an analysis sample of 558 teen births. There were no statistically significant differences between included and excluded cases on any of the measured variables except for race (30.11% and 34.12% were Black in included and excluded cases, respectively; p = .04).
Measures
Outcomes
At Wave IV, girls were asked about previous pregnancies and their outcomes. If they had gotten pregnant, they were asked “How did this pregnancy end?” with options of abortion, ectopic/tubal, miscarriage, stillbirth, and livebirth. If they indicated they had given birth, they were asked “How much did the baby weigh at birth?” “Was [baby’s name] born before or after [his/her] due date?” and then “How many weeks or days early/late was [baby’s name] born?” This was subtracted from 40 weeks to calculate gestational age.
Partner violence predictors
At Wave II girls were asked about their romantic and non-romantic relationship history in the last 18 months. Up to three romantic partners and up to three non-romantic partners were reported by adolescent girls. For each partner, they were asked “Did [INITIALS] call you names, insult you, or treat you disrespectfully in front of others?” [Insulting]; “Did [INITIALS] swear at you?”[Swearing]; “Did [INITIALS] threaten you with violence?”[Threatening]; “Did [INITIALS] push or shove you?”[Pushing]; and “Did [INITIALS] throw something at you that could hurt you?” [Throwing]. Responses were dichotomized into 0 = no, 1 = yes. If respondents answered “yes” to “Insulting,” “Swearing” or “Threatening” for ANY reported relationship, they were coded as “Ever had verbal abuse.” If they answered “yes” to “Pushing” or “Throwing” for ANY reported relationship, they were coded as “Ever had physical abuse.” Girls who reported no relationships were coded as not having experienced abuse.
Mediators
Based on prior literature, we examined a number of potential mediators between dating violence and birth outcomes. First, timing of prenatal care initiation was based on two questions asked about each pregnancy reported at Wave IV: “During this pregnancy with [partner] did you ever visit a doctor, nurse-midwife or other health care provider for prenatal care, that is, for one or more pregnancy check-ups?” and “How many weeks pregnant were you at the time of your first prenatal care visit?” Responses to these two questions were combined and recoded to reflect prenatal care initiation in the first trimester versus no use or late initiation of prenatal care. Second cigarette smoking during pregnancy was assessed at Wave IV for each pregnancy reported. Respondents were asked to report on an ordinal scale how many cigarettes they smoked during their pregnancy (none/a few cigarettes but not every week/a few cigarettes a week but not every day/10 or fewer a day/11-20 a day/21-30 a day/31 or more a day). We combined responses into a dichotomous variable (yes/no) due to sparseness across smoker frequencies in the sample. Third, BMI category (underweight, normal, overweight, obese) was determined through adolescents’ self-reported height and weight at Wave I. This measure was included as a proxy for disordered eating.
Controls
We drew on our previous analysis of predictors of birth outcomes in this cohort to determine confounders (Harville et al., 2012). This analysis indicated effects of race, age at pregnancy, age at Wave I, and parental education. Self-reported race was categorized as Black/non-Black. Parental education was measured as the higher of either co-residential mother or father: less than high school diploma, high school diploma/general equivalency degree (GED) or higher. All such variables were measured at Wave I. Ethnicity (Hispanic vs. non-Hispanic) did not predict the outcomes in the prior and current sample and thus was excluded.
Two other theoretically relevant controls were also included. The time interval between Wave II interviews and the birth, in addition to interactions between this time interval and reports of verbal and physical partner abuse, were included. We included these variables to test whether partner violence experiences reported at Wave II more strongly influenced pregnancies that occurred soon after the reported abuse. Adolescent girls’ experience of sexual abuse and physical abuse in their family-of-origin were also included, to test the distinct contributions of partner violence and family-of-origin violence. At the Wave IV interview, participants were asked to recall any maltreatment experience before age 18. We created two variables from the following questions: “Before your 18th birthday, how often did a parent or adult caregiver hit you with a fist, kick you, or throw you down on the floor, into a wall, or down stairs?” [Family physical abuse] and “How often did a parent or other adult caregiver touch you in a sexual way, force you to touch him or her in a sexual way, or force you to have sexual relations?” [Family sex abuse]. Responses were dichotomized into 0 = never, 1 = one or more times.
Analyses
All analyses were conducted in SAS (SAS Institute, Cary, North Carolina) using survey procedures, which apply population weights and adjust standard errors for non-independence between observations due to school-based sampling. All analyses were conducted stratified on race (Black vs. non-Black) based on prior research suggesting different predictors of birth outcomes according to race (Harville et al., 2012). We began with descriptive statistics (means and percentages) for all analysis variables, statistically comparing their distributions in Black versus non-Black teen mothers. We also conducted bivariate analyses (linear ordinary least squares [OLS] regression and ANOVA) to test the crude relationships between analysis variables and birth outcomes (gestational age and birth weight). We next implemented multivariable OLS models to examine the adjusted relationship between partner violence and birth outcomes. Because of the potential for dating abuse experiences to be more salient for births that occurred closer to Wave II interview, we tested interaction terms between pre-pregnancy dating violence victimization and length of time between Wave II and birth; only significant interactions were maintained. Finally, for cases when dating violence was significantly related to birth outcomes, we tested possible mediators. We followed the approach of Baron and Kenny (1986), and thus limited examination of mediators to those variables that were significantly associated with the predictor and outcome in bivariate analyses. To assess mediation, we added the potential mediator(s) to full models and examined changes in dating violence effect estimates.
Results
Characteristics of teen mothers overall and by race are presented in Table 1. The average birth weight was 3.24 kilograms (kg) and the mean gestational age was 39.25 weeks. Young mothers’ average age at baseline was about 15 years, and on average they gave birth 2.5 years afterward. Almost 1 in 5 teen mothers had a highest parental education less than high school diploma. One in 5 adolescent mothers (19.68%) experienced physical abuse by a parent or other caretaker before age 18, and almost 1 in 10 (9.64%) had experienced sexual abuse. Twenty-four percent of adolescent mothers reported verbal abuse in dating or intimate relationships pre-pregnancy, and 10.09% reported physical abuse in such relationships. About 16% of teen mothers were overweight or obese, 25.50% smoked during pregnancy, and 17% had late initiation or no prenatal care. Black adolescents had significantly lower birth weight, childhood physical abuse, partner verbal abuse, and smoking during pregnancy but higher BMI compared with other adolescent mothers.
Characteristics of Teen Mothers Participating in Add Health (N = 558).
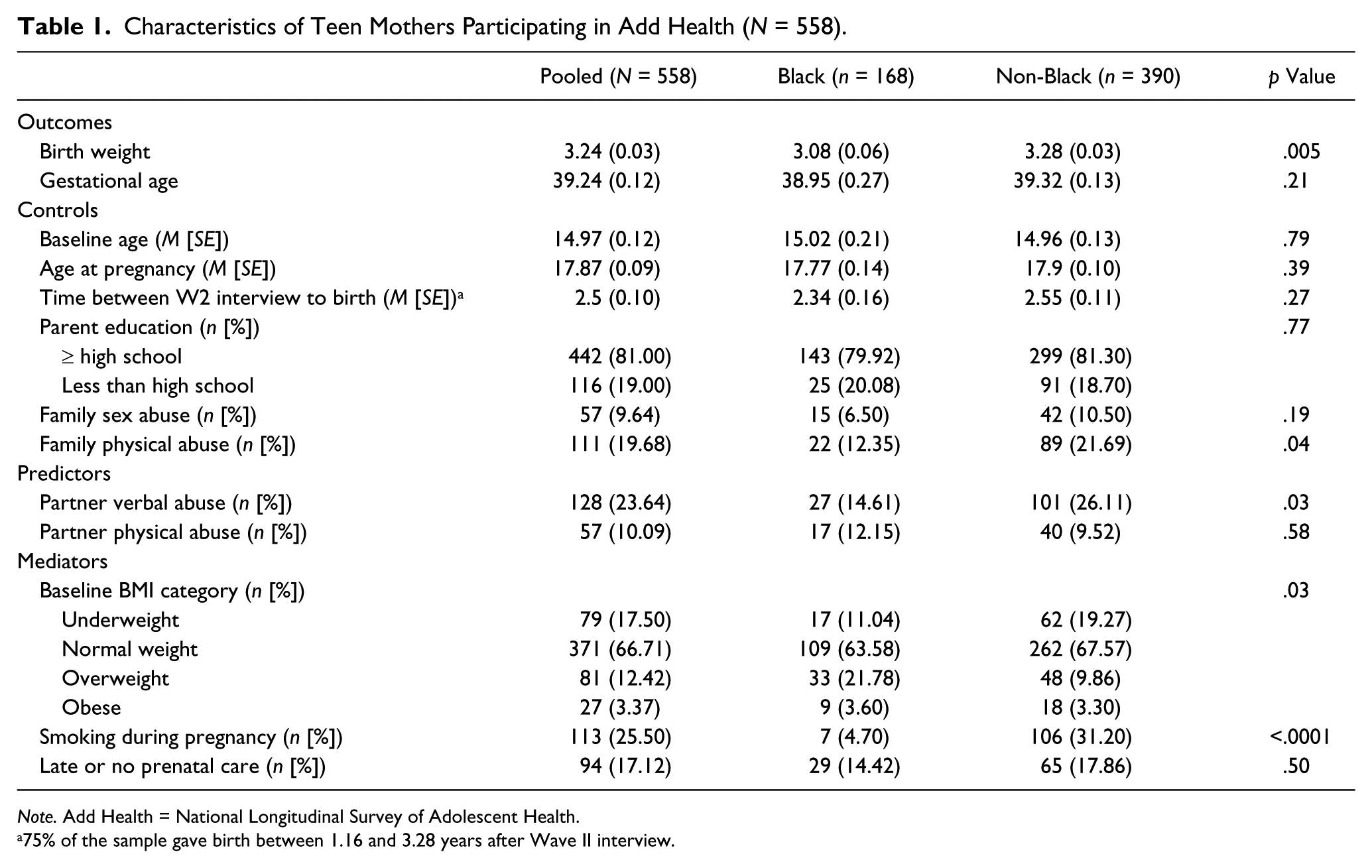
Note. Add Health = National Longitudinal Survey of Adolescent Health.
75% of the sample gave birth between 1.16 and 3.28 years after Wave II interview.
Only a few study variables were associated with birth weight in crude analyses (Table 2). Among Black teen mothers, lower parental education and family sex abuse were associated with significantly higher birth weights. Among non-Black mothers, none of the studied variables were significantly related to birth weight. Crude associations between study variables and gestational age were similarly sparse. For Black mothers, smoking during pregnancy and late or no prenatal care were associated with greater gestational age. For non-Black mothers, no factors were significantly related to gestational age.
Bivariate Analysis Between Maternal Characteristics, Dating Violence, and Birth Outcomes in Add Health (N = 558).

Note. Unless otherwise noted, figures represent means and standard errors of outcome variables. Add Health = National Longitudinal Survey of Adolescent Health; CI = confidence interval.
Further multivariable analyses were performed so that we could test differences in associations between dating violence and birth outcomes according to length of time between reporting the violence and the pregnancy. Models for birth weight are presented in Table 3. For Black mothers, verbal abuse in pre-pregnancy dating relationship was not significantly associated with birth weight. Pre-pregnancy physical dating violence was significantly positively associated with Black mothers’ infants’ birth weights when they gave birth shortly after Wave II interview; however, with time, associations between such abuse and birth weight became negative. For example, for Black mothers who gave birth 2 years after Wave II interview, pre-pregnancy physical abuse was associated with 0.79 kg lower birth weight (p< .001; Figure 1). For non-Black mothers, neither of the dating abuse variables were associated with birth weight. No mediation analyses were performed because none of the hypothesized mediators were significantly associated with birth weight in bivariate analyses.
Multivariable Analysis Between Maternal Characteristics, Dating Violence and Birth Weight in Add Health (N = 558).

Note. Figures presented are estimated β coefficients from OLS regression with standard errors. Add Health = National Longitudinal Survey of Adolescent Health; OLS = ordinary least squares.
p< .05. **p < .01.
Predicted birth weight among black girls comparing those with and without pre-pregnancy physical dating abuse.
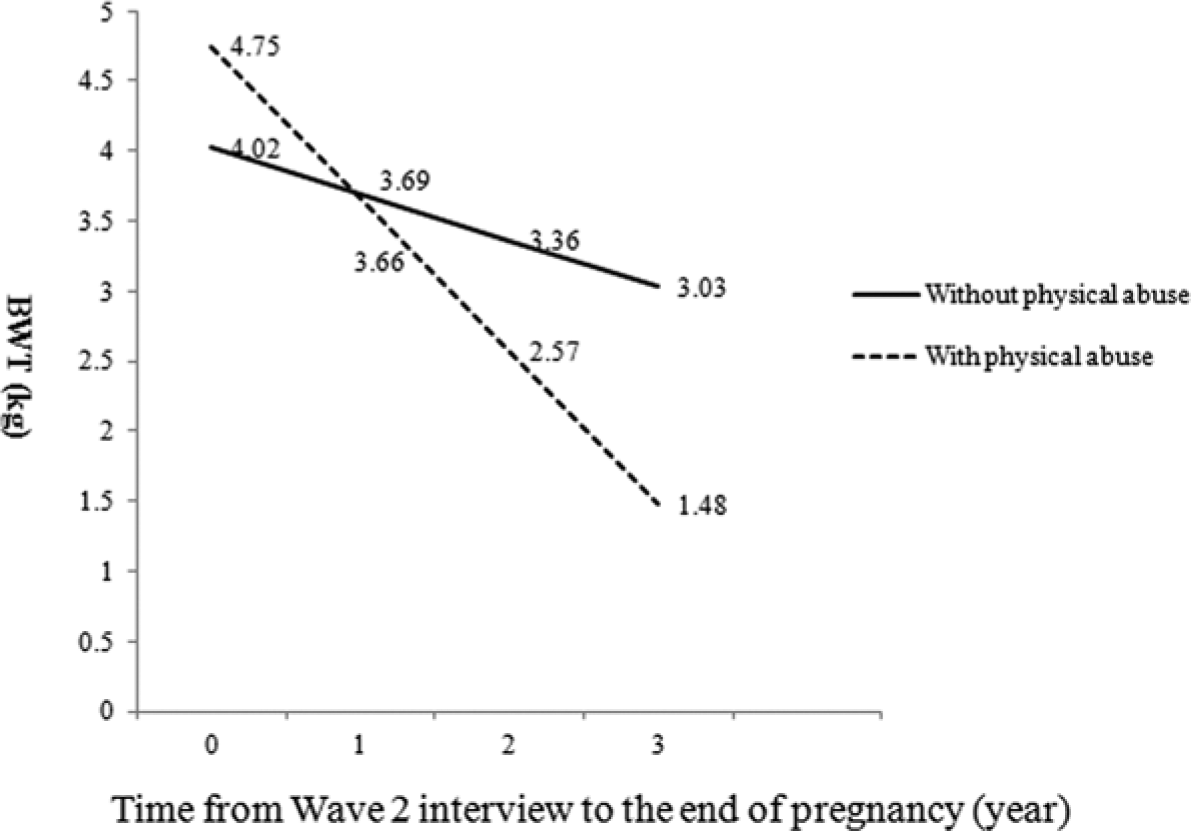
Associations between pre-pregnancy dating abuse and gestational age adjusted for maternal characteristics and abuse in the family-of-origin are presented in Table 4. Pre-pregnancy verbal abuse was not associated with Black teen mothers’ infants’ gestational age. Although pre-pregnancy physical abuse was not associated with gestational age for births that happened soon after Wave II, as time increased between Wave II and birth, negative associations became apparent and grew stronger (Model 1). For example, among Black teen mothers who gave birth 2 years after Wave II interview, pre-pregnancy physical dating violence was associated with 4.72 fewer weeks gestational age (p< .01; Figure 2). For mediation analyses, we only tested one variable (smoking during pregnancy) because the other variable found significantly associated with gestational age in bivariate analyses (later/no prenatal care) was not significantly associated with physical dating abuse. After adding this variable to the model for Black mothers (Model 2), effect estimates for physical abuse and its interaction with time did not change appreciably. Results do not support mediation. For non-Black mothers, neither verbal nor physical dating abuse pre-pregnancy were associated with infants’ gestational age.
Multivariable Analysis Between Maternal Characteristics, Dating Violence and Gestational Age in Add Health (N = 558).
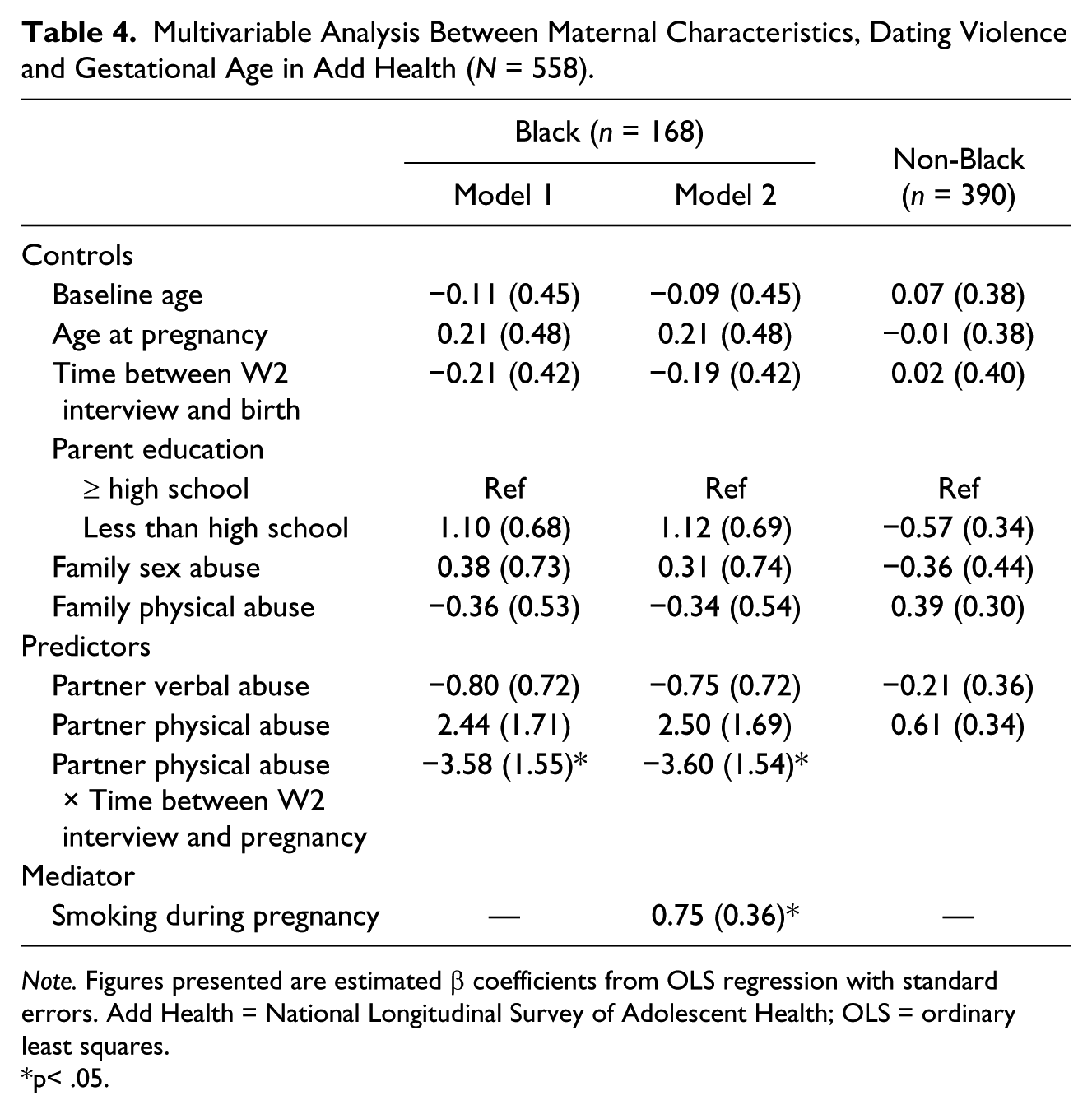
Note. Figures presented are estimated β coefficients from OLS regression with standard errors. Add Health = National Longitudinal Survey of Adolescent Health; OLS = ordinary least squares.
p< .05.
We also conducted a number of post hoc sensitivity analyses to test the robustness of our findings (results available from authors on request). We first limited our sample to young women who gave birth within 4 years of the Wave II interview (n = 476); we found similar results in terms of the magnitude and statistical significance of estimates reported here. When limiting to young women who gave birth within 3 years of the Wave II interview (n = 396), we found similar results for birth weight among Black teens, but the rest of the findings were non-significant. We also tried recoding exposure to dating violence using only experiences in the current or most recent relationship as of Wave II. Results from this analysis were consistent with the findings presented here.
Discussion
Despite research suggesting infants born to adolescent mothers are at increased risk of adverse birth outcomes relative to those born to adult mothers (Koniak-Griffin & Turner-Pluta, 2001), little is known about the risk factors for adverse birth outcomes in this group. Past research has linked experiences of physical abuse prior to or during pregnancy to negative birth outcomes among adolescent mothers (Covington et al., 2001; Curry et al., 1998). However, the impact of verbal abuse, and differences in effects according to maternal race or the relationship of the pregnant adolescent to the abuser (e.g., partner vs. family-of-origin) has not yet been explored. The present research addresses these shortcomings using data from a national sample.
For Black mothers, physical dating violence victimization was associated with worse birth outcomes as time between report of the abuse and pregnancy increased. This finding was surprising, given we expected that physical abuse would be more strongly related to birth outcomes the closer in time such reports were to the mother giving birth. To our knowledge, we are the only researchers who have examined lagged associations between adolescent dating violence/intimate partner violence on birth outcomes, and therefore reasons for this lagged association are unknown. We conjecture that this finding is possibly due to the severity of teen dating violence increasing over time. Continuation rates of adolescent dating violence are high—with approximately 40% of youth who experience dating violence during adolescence continuing to be victimized during early adulthood (Halpern, Spriggs, Martin, & Kupper, 2009). Studies have found that among adult women risk for psychological and physical intimate partner violence (IPV) increases with pregnancy (Burch & Gallup, 2004; Martin et al., 2004). In adult women, a longer duration of IPV is associated with increased severity of depression and post-traumatic stress disorder (PTSD; Golding, 1999), as well as increased odds of somatization (Samelius, Wijma, Wingren, & Wijma, 2007), all of which could influence birth outcomes through behavioral and/or stress pathways. Unfortunately, we cannot ascertain whether dating violence reported at Wave II continued or escalated during the pregnancy, therefore explanations for associations between pre-pregnancy abuse and birth outcomes are speculative. Future studies with more details on IPV over time for pregnant adolescents are needed to examine these mechanisms.
Our findings regarding the relationship between physical dating abuse and birth outcomes were not consistent across race. Racial differences in risk factors for adverse birth outcomes among teen mothers are consistent with some previous work with this same cohort (Harville et al., 2012). Such differences possibly arise from racial disparities in continuation rates of adolescent dating violence, which have been suggested in past studies (Halpern et al., 2009). Among adults, other negative pregnancy outcomes (i.e., maternal mortality) are elevated among women experiencing abuse, but even more so for Black compared with White women (Boy & Salihu, 2004). Again, further studies with more detailed histories of IPV and possible mediating factors are needed to tease apart these mechanisms.
In contrast to one study among adult mothers (Yost et al., 2005), verbal abuse was unassociated with birth outcomes among Black and non-Black teen mothers. Differences between studies could arise from differences in the time frame queried for verbal violence (i.e., during pregnancy for the adult study, prior to pregnancy in the present study), or real differences in risk factors for negative birth outcomes between adult and teen mothers (Harville et al., 2012). It is possible that verbal abuse alone is insufficient to disrupt what is, actually, a very robust system. Verbal abuse (and physical abuse) may also be underreported, which can lead to a bias toward the null. Finally, it is conceivable that positive aspects of relationships outweigh the negative effects of the verbal abuse, especially if such abuse is infrequent or non-recurring. As suggested above, further research that more closely follows adolescents during their pregnancy and that asks more in-depth questions about romantic relationships may shed further light on how such relationships influence pregnancy outcomes.
None of the mediators we examined were supported. It is possible that physical dating abuse operates through other pathways that we were unable to test (i.e., stress). It is also possible that the measurement of the mediators did not adequately capture the mechanism we intended. For example, with prenatal care, it is likely that it is not only early initiation but also consistent use as well as quality that influence birth outcomes. In addition, pre-pregnancy BMI is an imperfect proxy for inadequate weight gain during pregnancy or disordered eating during pregnancy. Further research examining these mediating pathways is needed.
A number of secondary findings of the present study were counter to expectations, namely that low parent education, childhood sexual abuse, and smoking during pregnancy were positively related to birth weight among Black adolescent mothers. This runs counter to extensive literature documenting negative effects of these factors on birth outcomes and health more generally (Browne & Finkelhor, 1986; Floyd, Rimer, Giovino, Mullen, & Sullivan, 1993). We believe sample selection biases may account for these counterintuitive findings, because our sample was limited to mothers who experienced a birth as an adolescent. In past analyses with this same cohort, comparing women who gave birth before versus after age 20, we found adolescent mothers were less likely to live with biologic parents during adolescence and to be married at the time of the birth, but they were more likely to have low parent education, an unemployed parent, to smoke during pregnancy, and to have late or no prenatal care (Harville et al., 2012). There also were very few Black teenage mothers who reported smoking during pregnancy in the present sample (n = 7). Given these issues, such results should be viewed with caution.
Although the present study has the strengths of using a national, population-based dataset, and prospective assessment of dating violence prior to pregnancy, findings should be interpreted with knowledge of the study’s limitations. First, we were only able to assess associations between pre-pregnancy dating violence and birth outcomes. It is possible that dating abuse changed in the time period between interview and pregnancy, due either to initiation of a different relationship or to violence changes within the Wave II reported relationship. Future studies that are able to more comprehensively assess longitudinal patterns of dating violence prior to and during teen pregnancy are warranted. Second, our measures of dating abuse are incomplete. It is possible that if other more severe acts had been queried, relationships between dating abuse and pregnancy outcomes would be stronger. Third, we are unable to elucidate the meaning or context of the acts reported by the adolescents, which could influence their effects on birth outcomes. For example, we are unable to distinguish between acts that the adolescent perceives as playful versus threatening. Past studies suggest substantial variability in the way acts are interpreted by adolescents (Foshee, Bauman, Linder, Rice, & Wilcher, 2007). Fourth, we reduced our sample size by requiring complete covariate data. However, analyses comparing included versus excluded adolescents indicated no significant difference in birth weight (p = .26), gestational age (p = .42), baseline age (p = .81), age at pregnancy (p = .78), BMI category (p = .75), partner verbal abuse (p = .30), partner physical abuse (p = .15), family sex abuse (p = .75), and family physical abuse (p = .28). The only difference is race distribution (p = .04). Finally, we relied on maternal self-reports of birth weight and gestational age, which may be subject to recall biases. However, past studies comparing birth records to maternal self-report have found maternal reports of birth outcomes are largely a valid method of obtaining data (Tomeo et al., 1999).
Conclusion
Physical dating violence victimization that occurred prior to pregnancy was related to reduced birth weight and gestational age for Black adolescent mothers as time increased. Such results suggest the potential utility of a life course or preconceptional health perspective for adolescent mothers, whereby enhancing pre-pregnancy physical and social health can positively influence birth outcomes. Findings suggest that teen dating violence prevention programs implemented prior to pregnancy potentially could have positive effects on the birth weight and gestational age of infants born to these young women. Intervening on long-term violence may be particularly important. Results also suggest the possible importance of screening for teen dating violence in more general pediatric practice, coupled with referral to supportive counseling services, that may help teens escape violent relationships.
Footnotes
Acknowledgements
This research uses data from Add Health, a program project directed by Dr. Kathleen Mullan Harris and designed by Dr. J. Richard Udry, Dr. Peter S. Bearman, and Dr. Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Dr. Ronald R. Rindfuss and Dr. Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (![]() ). No direct support was received from grant P01-HD31921 for this analysis.
). No direct support was received from grant P01-HD31921 for this analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NICHD Grant 1R03HD067240-01.