
Abstract
To provide differential effectiveness on length of stay at a shelter and receipt versus non-receipt of a protection order (PO), and outcomes of violence, functioning, and resiliency, in 300 abused women (150 first-time users of a shelter and 150 first-time applicants for a PO) who participate in a 7-year study with outcomes measured every 4 months. Four months after a shelter stay or application for a PO, abused women staying 21 days or less at a shelter reported similar outcomes compared with women staying longer than 21 days. Similarly, women receiving and not receiving a PO reported overall equivalent outcomes. Seeking shelter or justice services results in similar improved outcomes for abused women 4 months later, regardless of length of stay at the shelter or receipt or no receipt of the PO. Contact with shelter and justice services results in positive outcomes for abused women and indicates the urgent need to increase availability, accessibility, and acceptability of shelter and justice services.
Introduction
In the United States and worldwide, it is estimated that 30%, or more, of women have experienced intimate partner violence (Black et al., 2011; World Health Organization [WHO], 2013). Women who have experienced partner violence are at greater risk for mental health symptoms, including depression, post-traumatic stress disorder (PTSD), and anxiety than women who have not experienced partner violence (WHO, 2013). Women with intimate partner violence history are also more likely to experience chronic pain (Bonomi, Anderson, & Reid, 2009; Dillon, Hussain, Loxton, & Rahman, 2013; Ellsberg et al., 2008; Kelly, 2012; Vives-Cases, Ruiz-Cantero, Escribà-Agüir, & Miralles, 2010; Vung, Ostergren, & Krantz, 2009). Somatization, experiencing symptoms of illness out of proportion with or without apparent relationship to illness, is also associated with partner violence experiences. In a study of 109 couples, Liu et al. (2011) found that 19% of variance in somatization scores was due to partner violence. Mental health symptoms secondary to partner violence traumatic experiences may affect the exposed individual’s attachment style, ability to regulate emotions, and ways of thinking about being in the world (Lilly & Lim, 2013). The untoward mental health effects of partner violence may go beyond the women to influence the function of their children. Maternal depression is associated with long-lasting effects on children (Katz, Hammen, & Brennan, 2013).
Herrman et al. (2011) described resilience as the capacity to cope with adverse events, recovering with intact mental health. They list risk factors (stressors) that may decrease resilience and protective factors (resiliency factors) that may enhance resilience. When traumatic events occur, the interactions between the stressors and resilience factors may lead to mental illness or to thriving. Understanding resilience is an important part of planning effective responses to enhance function following trauma.
Among the major public or community-based options for women with children who are seeking protection from perpetrators of partner violence are safe shelters, also known as women’s shelters or domestic violence shelters, and protection orders (POs) through government justice services. The U.S. Health and Human Services website, in its discussion of safety planning, mentions obtaining a restraining order and protective shelter as part of safety planning. In addition to these community resources, they also suggest private resources, such as family and friends (WomensHealth.gov, 2011). For women who are seeking safety from an abusive relationship, there are few other resources available. While women may seek both safe shelter and justice services, there is little evidence to guide practitioners and policy makers in deciding which is likely to be the most effective first course of action for a given woman and her children.
The WHO guidelines for policy and clinical practice for partner violence call for evidence-based interventions that are culturally sensitive and effective for low, medium, and high resource countries (WHO, 2013). The Institute of Medicine (2011) calls for evidence for strategies to decrease violence against women and children. The recent U.S. Preventive Services Task Force revised its recommendations, now a B recommendation that supports all health care providers screen all women between the ages of 14 and 46 for intimate partner violence and provide or refer to services that offer support to abused women (Moyer, 2013). The WHO (2013) guidelines for clinicians provide a discussion of issues related to universal screening, and establish a conditional recommendation that universal screening not be implemented unless there are findings that may be caused by, or complicated by, partner violence. The rationale for advising against universal screening is that there is little evidence that such screening improves outcomes (WHO, 2013, Recommendation 2, pp. 17-19). Included in the recommendations is that health care providers have knowledge about the availability of resources. Presumably, such awareness includes an understanding of the likely outcomes for women who use given resources. The need for evidence about resources available to women needing protection is twofold: first, to establish the safety outcomes for women who use a given safety resource, and second, to establish women’s longer term outcomes, related to the safety resource they use. To our knowledge, there have been no studies that considered women who were using these safety resources for the first time.
To provide evidence on the effectiveness of length of shelter stay and the receipt or non-receipt of a PO and subsequent violence, functioning, and resiliency outcomes for abused women who use shelters or justice services for the first time, a 7-year prospective study is underway. Women who are first-time users of shelter and justice services are followed to maximize the potential to interrupt the cycle of violence and prevent repeated use of services. Although no published literature was found on the effectiveness of shelter services or POs for first-time users, some outcome information is available post shelter stay and following application for a PO.
Outcomes Following a Shelter Stay
Women who seek protection from abuse in a shelter are more likely to have (a) lower incomes, (b) more children, (c) experienced more abuse, and (d) made more attempts to obtain help than abused women who do not seek shelters (Ham-Rowbottom, Gordon, Jarvis, & Novaco, 2005). Outcomes following a shelter stay include re-abuse and mental health functioning. R. Campbell, Sullivan, and Davidson (1995) found that 43% of 141 women exiting a shelter reported re-abuse 6 months later. In contrast, Ham-Rowbottom et al. (2005) found that of 81 women who were met at least 6 months post shelter, 60% were in a romantic relationship and only 2 of those women experienced abuse. It is noteworthy that the women in the Ham-Rowbottom study received housing support, either in the form of 2 months in an apartment in a middle-class neighborhood or 1 year in a traditional housing program with a related 5-year program of support. Despite the housing support, of the potential participants (N = 156 with 2-month housing; N = 92 with 1-year housing), only 24% (N = 37) of those with 2-months of housing and 48% (N = 44) of those with 1 year of housing completed the study, suggesting the study results may be skewed to those with better outcomes. Bybee and Sullivan (2005) reported that 3 years post shelter, 81% of 124 sheltered women did not return to the abuser; however, 19% of women reported being assaulted and 22% reported being harassed by the abuser. Half of the women in their sample had received post-shelter services. A year earlier, those who received the post-shelter services were less likely than the other women to have experienced post-shelter assault. However, at 3 years, the post-shelter assault rates were similar for the two subsets of the sample. Of the women who were assaulted by the abuser, 35% reported not being in a relationship with the abuser in the previous 6 months.
Researchers have identified lack of economic resources as factors associated with an increased risk for abuse following shelter (Bybee & Sullivan, 2005; Byrne et al., 1999; R. Campbell et al., 1995). Similarly, women with lower economic resources are at higher risk for mental health problems, including depression and PTSD, following a shelter stay (Ham-Rowbottom et al., 2005). The association of a lack of resources with abuse and with mental health symptoms is consistent with the Herrman et al. (2011) description of social-economic factors that support resilience and protect against mental illness.
A decline in mental health symptoms following a shelter stay has been widely reported. In one study, 83% of women reported symptoms of depression while in the shelter, but only 50% of the women had depression at 10 weeks post shelter. The rate was stable at 6 months post shelter stay (R. Campbell et al., 1995). Similar improvements were found in PTSD symptoms. Johnson and Zlotnick (2012) studied 104 shelter women and found that rates of PTSD in the sample dropped from 86.1% in the shelter to 58.2% at 6 months. Despite the decrease in mental health symptoms by participants in the Ham-Rowbottom et al. (2005) study, whom the researchers describe as the “cream of the crop” (p. 118) of intimate partner abuse survivors, 43% of the women had depression cutoff scores above the level for clinical depression, and their intrusion and avoidance scores were comparable with levels for those being treated for clinical levels of PTSD. Similarly, Alsaker, Moen, and Kristoffersen (2008) reported statistically significant improvements in quality of life measures 1 year after leaving the shelter (N = 22), specifically domains of vitality, mental health, social functioning, and physical role. However, the quality of life measures for the women remained far below the general population scores for Norway, where the study was performed, even after the improvement at 1 year.
Abuse following a shelter stay is consistently linked with poorer mental health functioning post shelter. Post-sheltered women who report re-abuse also report more depression (Bybee & Sullivan, 2005; R. Campbell et al., 1995). It may be that being abused post shelter and poorer mental health are both related to factors associated with resilience. For example, Ham-Rowbottom et al. (2005) reported that depression and PTSD, in the absence of further violence post shelter, were associated with childhood abuse and financial problems post shelter. Child abuse may be related to several of the stressors that Herrman et al. (2011) suggested increase the risk for low resilience (e.g., low infant nurturance, poor relationships, negative life events) and, when compounded by a lack of resiliency factors such as social-economic factors, may result in an increased risk for abuse and mental health symptoms.
Outcomes Following Application for a PO
POs are designed to protect individuals at risk for violence by another individual from future harm through legal means that restrict the perpetrators’ access to the at-risk individual. The way in which POs are sought, received, and implemented varies widely, based on the jurisdiction. One possibility is that an individual will seek a hearing in a civil court to obtain a PO. The variation in implementation adds to difficulties in evaluating their effectiveness (Benitez, McNiel, & Binder, 2010). Based on a review of 15 empirical studies of outcomes following POs, Benitez et al. (2010) concluded that there is evidence that receiving a PO reduces the victim’s risk for further violence. McFarlane et al. (2004) found significantly lower levels of violence over 18 months after women (n = 150) who were qualified for a PO had applied for a PO. This held whether they had actually received the PO. Holt, Kernic, Wolf, and Rivera (2003, n = 2,691) found that women who received permanent POs experienced an 80% reduction in physical violence over the following year, based on police-reports. The Odds Ratios (ORs) of women with POs being contacted (OR = 0.4), threatened (OR = 0.4), psychologically abused (OR = 0.5), or physically abused (OR = 0.3) by the perpetrator were lower than comparable women who had not obtained POs. Kothari and colleagues (2012) conducted a retrospective review of police, emergency room, family court, and prosecutor administrative records. Compared with a matched group without POs, those with POs had double the police incidence rates prior to the PO, but the same rate after the PO. The researchers concluded that receiving a PO has protective effects. The studies presented here are important because they go beyond simply reporting the rate of violation of the PO to evaluating the violence experiences outcomes. The latter two studies, with the comparison groups who did not have POs, present good evidence that the decrease in violence is not simply an artifact of time.
Carlson, Harris, and Holden (1999, n = 210 couples) examined court and police records for 2 years prior to and 2 years following the PO and found that the longer the PO was in effect, the less likely it was that the women would experience physical violence. Their results also indicated that, despite the generally positive findings that violence decreases as a result of POs, there is reason to apply caution when recommending POs. Women with low-socioeconomic status and women who were African American were more likely to report abuse following the PO. In a further discussion and evaluation, based on that data set, Mears, Carlson, Holden, and Harris (2001) reported similar findings. Spitzberg (2002) also found evidence of abuse following a PO being obtained, reporting that violence increased in 21% of cases.
Study Purpose
The purpose of this study was to provide evidence for differential effectiveness of length of shelter stay and receipt compared with no receipt of a PO, and abused women outcomes 4 months following initial use of services. As the median length of a shelter stay is 21 days (National Network to End Domestic Violence, 2007), this research examines differential effectiveness of length of stay according to less than or more than the mean of 21 days.
For the purposes of this article, we are examining the interaction effect of time (Baseline [entry to service; 4-month follow-up) by dose (Days at Shelter [<21 days; >21 days]; PO [received; not received]). See McFarlane, Nava, Gilroy, Paulson, and Maddoux (2012) for a full review of the aim, scope, and methodology of the 7-year prospective study, which will evaluate the impact of shelter and justice services accessed for the first time by abused women with children over a 7-year period.
Research Questions
Method
Design
A quasi-experimental observational prospective design is followed with repeated measures every 4 months for 7 years.
Setting
The study is occurring in a large urban metropolis in the United States with a population exceeding 4 million. Five shelters designated for abused women with a collective bed capacity of 400 for women and their children serve the population along with a central District Attorney’s (DA) Office for processing of POs. The shelters offer standard services of safe shelter, counseling, and advocacy. Services of the DA’s Office are legal processing for a PO.
Population and Sample Size Determination
Our eligible population is English- and Spanish-speaking abused women seeking a shelter for abused women or justice services, specifically a PO, for the first time who had never used shelter services or applied for a PO in the past and who also had at least one child between the ages of 18 months and 15 years who live with the mother at least 50% of the time. (Only one child was selected at random due to time burden for the participant and study costs.) Sample size was determined with G-power. Considering two independent samples (i.e., sheltered women and PO applicants) with a conservative effect size of .40, a power of .90, and alpha of .05, 135 women were needed in each group. Allowing for attrition, we set the sample at 150 women and 150 children in each group for a total of 300 women and 300 children. If the woman had more than one child between the ages of 18 months and 15 years, each child was given a number according to birth order and a die was rolled to select one child at random to be followed in the study.
Procedures
Following internal review board approval, recruitment began at five local shelters for abused women and the DA’s Office. Trained, bi-lingual researchers in English and Spanish approached all women entering the shelter or applying for a PO and established eligibility criteria. If the women were eligible, the women were taken to a private room and invited to participate in the study. After signing informed consent and completion of the 60-min interview, all 300 women were offered US$30 cash. Two native Spanish and English speakers completed standard forward and backward translation of all questionnaires from English to Spanish and back to English. The interview could be completed in 60 min in both languages. The researchers recorded the woman’s responses. Recruitment, eligibility screening, and entry into the study continued daily for 13 months at the five shelters and Monday through Friday at the DA’s Office. Over the 13 months, 330 women met eligibility criteria. A total of 19 eligible women refused to participate, usually due to a lack of time, and 11 women were missed (i.e., left the shelter or DA’s Office before the study could be explained). A total of 300 women (e.g., 150 at the shelters and 150 at the DA’s office) met eligibility criteria and agreed to participate in this study.
Participants
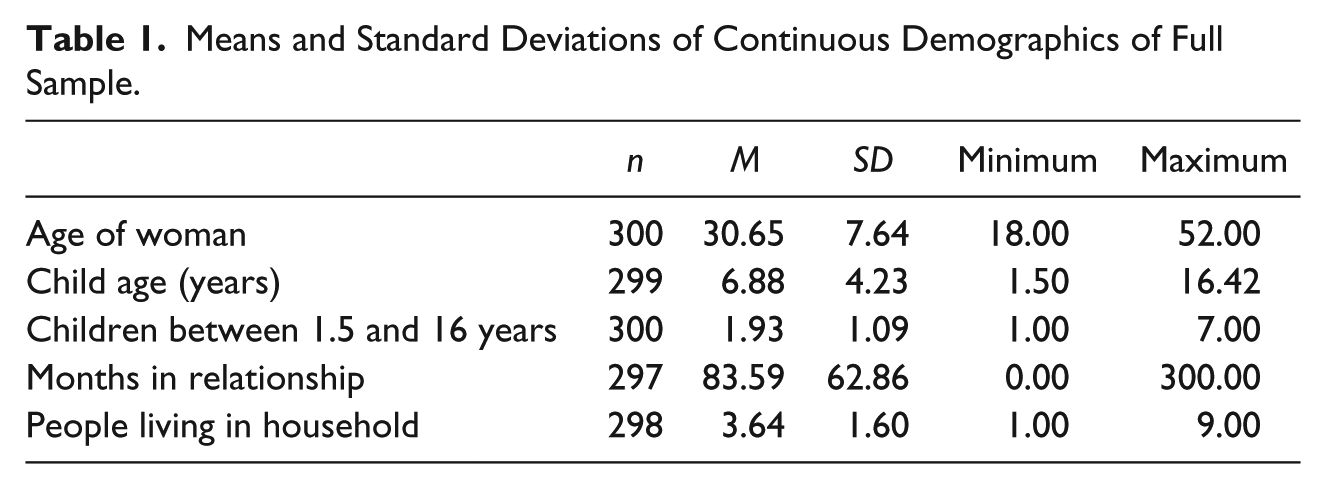
Means and standard deviations for continuous demographic variables for the full sample are outlined in Table 1. Women who participated in this study had ages ranging from 18 to 52 years old (M = 30.65; SD = 7.64), with the age of the randomly chosen child ranging from 1.5 to 16.42 years old (M = 6.88, SD = 4.23). Participants reported an average of 3.64 (SD = 1.60) people living in their household, and that there was an average of 1.93 (SD = 1.09) children living in the home. The length of the relationship with the abuser ranged greatly from 0 months to 300 months (25 years) (M = 83.59, SD = 62.86).
Means and Standard Deviations of Continuous Demographics of Full Sample.
Frequencies and percentages of categorical demographics for the full sample are shown in Table 2. The greatest percentage of the sample self-identified Spanish or Hispanic as their ethnic background (n = 137; 45.7%), followed by Black (n = 78, 26.0%) and White (n = 32; 10.7%); the remaining women self-classified as multi-racial or Asian. A large majority of the sample reported that they are not currently in a romantic relationship (n = 251; 83.7%). In addition, a majority of the sample reported that they are not currently in a relationship with the abuser (n = 190, 63.3%). Most participants reported that they had completed secondary education or equivalent.
Frequencies and Percentages of Categorical Demographics of Full Sample.

Measures
To establish temporal sequencing, the measures were asked at entry into the study, prefaced with “During the last 4 months” and repeated every 4 months for 7 years, prefaced by “Since we talked on (date of last visit”). A 4-month interval was selected for maximum stability of the child functioning instruments and to minimize recall bias. All measures were completed within 48 hr of entry into the shelter or application for a PO.
Abused Women’s Functioning
BSI-18
The BSI-18 (Derogatis & Lazarus, 2001) is an abbreviated version of the 53-item BSI (Derogatis, 1993) which, in turn, is a shortened form of the 90-item Symptom Checklist–90–Revised (SCL-90-R; Derogatis, 1994). The BSI-18 is an 18-item self-report scale of statements that test-takers respond to based on their level of distress over the preceding 7 days (5-point Likert-type scale from 0, not at all, to 4, extremely). The 18 statements are divided equally among three dimensions: somization, anxiety, and depression. Items were taken verbatim from the 53-item BSI. The Global Severity Index (GSI) of distress constitutes the sum of the three dimensions. Dimension scores for somization, anxiety, and depression range from 0 to 24. The total GSI score ranges from 0 to 72 with higher scores indicating higher levels of psychological distress (Derogatis & Lazarus, 2001). Reported internal consistency estimates are acceptable (.74 for Somization, .79 for Anxiety, .84 for Depression, and .89 for the total GSI). Concurrent validity with the SCL-90-R is high, ranging from .91 to .96 on both dimensions and total scores. Factor analysis on a clinical sample of 1,134 persons yielded a four-factor solution with two of the factors containing exact items belonging to the Somatization and Depression scales. The other two factors are composed of items belonging to the Anxiety scale and considered acceptable (Derogatis & Lazarus, 2001). Example items for depression, anxiety, and somatization, respectively, include “feeling no interest in things,” “feeling tense or keyed up,” and “numbness or tingling in parts of your body.” Respondents are asked to endorse how much they were bothered during the past 7 days by each of the 18 items. For this study, coefficient alpha was .91 for the GSI, .86 for Anxiety, .79 for Somatization, and .85 for Depression.
PTSD
This seven-item symptom scale screens for PTSD (Breslau, Peterson, Kessler, & Schultz, 1999) and is a subset of items from the National Institute of Mental Health Diagnostic Interview Schedule for PTSD. The seven items were empirically derived in the context of an epidemiological study of PTSD in an urban area of the United States. The seven items selected were those that most efficiently predicted PTSD diagnostic status (Breslau et al., 1999). The screen consists of five avoidance items and two hyperarousal items. Items include “Do you avoid being reminded of the abuse by staying away from certain places, people, or activities?” and “After the abuse, are you having more trouble than usual falling asleep or staying asleep? Respondents rate each item as either “yes” or “no” and adding the number of “yes” responses scores the instrument. When the seven-item scale was evaluated for predictive validity in a National Epidemiological Survey, a score of 4 or more on the seven-item scale identified cases of PTSD with sensitivity of 78%, specificity of 97%, positive predictive value of 75%, and negative predictive value of 98%. The percentage of correctly classified respondents was 96% (Bohnert & Breslau, 2011). For this study, coefficient alpha was .70.
Brief Pain Inventory (BPI)
This self-report 17-item patient self-rating scale is designed to measure the intensity, location, quality, treatment, and impact on daily life of chronic pain (Daut, Cleeland, & Flanery, 1983). Concurrent validity was established between use of pain medications and overall pain ratings and respectful reliability was demonstrated over short intervals resulting in test–retest item correlations of .78 for usual pain and .93 for present pain (Keller et al., 2004; Tan, Jensen, Thornby, & Shanti, 2004). The Taxonomy Committee of the International Association for the Study of Pain defined chronic pain as pain of > 3 months duration (Merskey & Bogduk, 1994). Therefore, a participant was considered to have recent chronic pain if she answered in the affirmative to pain that did not go away and lasted 3 months or more during the last 4 months. If the participant answers yes, she was asked to rate the intensity of her worst pain as well as current pain using 0 (no pain) to 10 (pain as bad as you can imagine) numeric rating scales (NRS). The degree to which pain interferes with seven domains of functioning (i.e., general activity, mood, walking ability, normal work, relations with others, sleep, and enjoyment of life) was assessed using 0 (does not interfere) to 10 (completely interferes). Scores are generated for severity of pain that can range from 0 to 30 and interference of pain with activities of daily living, which can range from 0 to 30. For this study, coefficient alpha was .84 for Pain Severity and .87 for Pain Interference.
Maternal Resiliency
Safety Behavior Checklist
The checklist is a seven-item safety survey to assess present use of safety behaviors and chart future adoption (McFarlane & Parker, 1994). The safety behavior checklist was initially published in 1994 by the March of Dimes as part of a comprehensive protocol on the care of abused women (McFarlane & Parker, 1994) and subsequently updated (McFarlane, Parker, & Cross, 2001, 2007). Content validity was established by a group of nurse researchers in the field of violence against women and since has been used to evaluate safety behaviors adoptions (McFarlane et al., 2002; McFarlane, Parker, Soeken, Silva, & Reel, 1998). An example of a question is, “Have you hidden an extra set of house and car keys?” Scoring of the checklist proceeds as follows. Not all seven items on the checklist are applicable to every participant (e.g., a woman with a child less than 5 years of age would be “not applicable” for teaching the child to dial 911); therefore, the scoring of the checklist is “adjusted” for purposes of interpretation and comparison. The adjusted total score falls within a 0-to-7 range of behaviors performed. The following equation expresses the relationship of the number of applicable behaviors performed to the “adjusted” total number of behaviors: a / b = x / 7, where a is the number of behaviors performed, b is the total number of applicable behaviors, and x is the adjusted total. An “adjusted” total number of behaviors performed is calculated each time the safety behavior checklist is completed. For this sample, coefficient alpha was .58.
General Self-Efficacy Scale (GSE)
This 10-item instrument was created to assess a general sense of perceived self-efficacy with the aim to predict coping and adaptation after stressful life events (Schwarzer & Jerusalem, 1995). Responses to each item are made on a 4-point scale: 1 = not at all true, 2 = hardly true, 3 = moderately true, 4 = exactly true. An example of an item is “I am confident that I could deal efficiently with unexpected events.” Responses are summed. The possible range of scores is 10 to 40. Criterion-related validity is documented in numerous correlation studies where positive coefficients were found with favorable emotions and negative coefficients were found with depression, anxiety, and somatization. In samples from 23 countries, Cronbach’s alphas ranged from .76 to .90, with the majority in the high .80s (Schwarzer & Jerusalem, 1995). For this study coefficient alpha was .86.
Norbeck Social Support
This six-item instrument measures multiple components of social support, including functional properties of social support (e.g., emotional and tangible support) and network properties (e.g., stability of relationships, frequency of contact), as well as the amount of support from specific sources (e.g., relatives, friends; Norbeck, Lindsey, & Carrieri, 1981, 1983). Respondents are asked to list first names or initials for each significant person in their lives who provides personal support to them. Respondents indicate the kind of relationship for each person on this network list by use a 5-point rating scale to describe the amount of support available from each person with 0 = no support, 1 = a little support, 2 = moderate support, 3 = quite a bit of support, and 4 = a lot of support. Example of a question is “If you needed to borrow $10, a ride to the doctor, or other immediate help, how much could (name of person) help?” Construct and concurrent validity are established on samples of employed adults ranging in age from 22 to 67 and internal consistency established with Pearson correlations (Norbeck et al., 1981, 1983). The instrument was revised to the present form in 1995 (Norbeck, 1995). For the purposes of this study, respondents are asked for the initials of their three primary sources of support. An extra question follows the Norbeck standard questions that ask if the abused woman has shared the violence with this individual. Responses are summed and ranged in this study from 6 to 84. The coefficient alpha was .83
Koci Marginality Index (KMI)
This 5-item, abbreviated version of the KMI-95 items and KMI-70 items is a 5-point Likert-type scale to assess women’s marginality, the perception of living on the periphery of the social center (Koci, 2004). Women are asked to endorse five questions with responses of 1 = strongly disagree, 2 = disagree, 3 = neither disagree nor agree, 4 = agree, and 5 = strongly agree. Responses are summed and scores range from 5 to 25. An example of a question is, “Meeting new people is hard for me.” The higher the score, the more marginalized the woman. In previous research, the internal consistency (Cronbach’s α coefficient) of the (KMI-70) was .96 (n = 244; Koci, 2004). For this study, coefficient alpha was .84.
Maternal Abuse
Danger Assessment Scale (DAS)
This 19-item questionnaire with a yes/no response format is designed to assist women in determining their potential risk for becoming a femicide victim (J. C. Campbell, 1986). All items refer to risk factors that have been associated with murder in situations involving abuse. Examples of questions include “Has the physical violence increased in severity or frequency?” and “Has the abuser forced the woman to have sex?” Convergent construct validity of the instrument has been supported by correlations in the moderately strong range, with instruments measuring severity and/or frequency of abuse (J. C. Campbell, 1995). Validity in terms of differentiating groups is supported by the different means in seven groups of abused women studied that accurately reflect the differing degrees of severity of abuse one would expect in different populations. For example, the lowest scores were in the non-abused sample, with the highest scores in the hospital emergency room group. Samples of abused women from the community had scores in the intermediary range (J. C. Campbell, 1995). Initial reliability of the instrument was .71 (J. C. Campbell, 1986) and ranged from .60 to .86 in five subsequent studies (J. C. Campbell, 1995). Weighted scoring results in four ranges of danger: less than 8 = Variable Danger; 8 to 13 = Increased Danger; 14 to 17 = Severe Danger; and 18 or more = Extreme Danger. For this study, coefficient alpha was .66.
Severity of Violence Against Women Scale (SAVAWS)
This is a 47-item instrument designed to measure threats of abuse (19 items) and physical abuse (28 items; Marshall, 1992). Physical abuse items include 6 items on sexual abuse. Examples of behaviors that represent threats are “How often has (name of abuser) threatened to hurt you?” and “How often has (name of abuser) thrown an object at you?” Examples of questions that represent physical assault are “How often has (name of abuser) kicked you?” and “How often has (name of abuser) punched you?” An example of sexual assault is “How often did the (name of abuser) make you have anal sex against your will?” Included are nine factors or subscales that have been demonstrated valid through factor analytic techniques: Symbolic Violence, and Mild, Moderate, and Serious Threats (Threats of Violence dimension) and Mild, Minor, Moderate, Serious, and Sexual Violence (Actual Violence dimension). For each item, the woman responds using a 4-point scale to indicate how often the behavior occurred (1 = never, 2 = once, 3 = 2-3 times, 4 = 4 or more times). The possible range of scores is 19 to 76 for the threats of abuse and 28 to 112 for physical assault. Initial internal consistency reliability estimates ranged from .92 to .96 for a sample of 707 college female students and from .89 to .96 for a scale of 208 community women (Marshall, 1992). Subsequent reliability for abused women have ranged from .89 to .91 for threats of abuse and .91 to .94 for assault, respectively (Coker, Smith, McKeown, & King, 2000; Gist et al., 2001). For this study, coefficient alpha was .95 for the total scale, .90 for Threats of Abuse subscale, .93 for Physical Abuse subscale, and .84 for Sexual Abuse subscale. At baseline, threat scores ranged from 19 to 76 (M = 41.78, SD = 13.32), sexual abuse ranged from 6 to 22 (M = 8.32, SD = 3.64), and physical abuse scores ranged from 21 to 78 (M = 36.52, SD = 13.88).
Data Analysis
Data were confidentially encoded and entered into a secure database in the research office. Prior to conducting the primary analyses, preliminary analyses were conducted to test the simple relationships among key demographics (e.g., age, ethnicity, length of time in relationship with the abuser, level of education) as well as other potential covariates (e.g., physical abuse severity, sexual abuse severity, danger assessment, being hit by family as a child, working status at intake) on the outcome variables of interest (anxiety, depression, somatization, PTSD, pain interference, pain severity, safety behaviors, general self-efficacy, social support, marginalization, danger assessment weighted, threats, physical abuse severity, sexual abuse severity). These preliminary analyses revealed that the following variables were associated with the outcome measures and were, therefore, included as covariates in the primary analysis: physical abuse severity, sexual abuse severity, danger assessment weighted, age, being hit by family members as a child, working status at intake, ethnicity (Black compared with other ethnicities; Hispanic compared with other ethnicities), education (attending school as a child; completing Grades 9-11; completing 1-3 years of college; completing 4 or more years of college), and length of time in the relationship with the abuser.
To test the primary research questions, a series of MANCOVA tests were conducted to test for an interaction between time (baseline and 4 months) and group (shelter stay less than 21 days vs. shelter stay greater than 21 days; PO received vs. PO not received) on maternal functioning (i.e., anxiety, depression, somatization, PTSD symptoms, pain interference, pain severity), maternal resiliency (i.e., safety behaviors, general self-efficacy, social support, marginalization), and maternal abuse (i.e., danger assessment weighted scores, threats of abuse, physical abuse, sexual abuse). The significance level for all tests was set at .05. The measure of effect size reported along with MANCOVAs is η2, which can be interpreted as follows: ~ .01 = small, ~ .06 = medium, ~ .14 large (Cohen, 1988).
Power Analysis and Sample Size
To determine the minimum number of participants needed to find significance if in fact significance exists, a priori power analyses were conducted using G*Power 3.1 for the highest level of statistical test utilized in this study, which was MANCOVA tests. For two groups and two measurement time points, an alpha level of .05, and an estimated effect size of .25, it was determined that a minimum sample size of 128 was needed to achieve statistical power of .80. Out of the 300 women recruited in the sample, 150 women sought services through safe shelters and 150 women sought protective services through the DA’s office, thus meeting the minimum sample requirement for the primary analyses.
Results
Length of Shelter Stay
To test the dose response of median shelter stay on mother’s functioning (e.g., anxiety, depression, somatization, PTSD symptoms, pain severity, and pain interference), a series of MANCOVAs were conducted controlling for physical abuse, sexual abuse, age, working status at intake, ethnicity, level of education, childhood abuse, and maternal danger. When controlling for the aforementioned covariates, there was not a significant effect of days at shelter across any of the maternal functioning items (see Table 3). What this indicates is that women’s functioning increased at 4 months regardless of the amount of time spent at the shelter, which further suggests that any amount of support through safe shelters has a positive impact of maternal function.
Means and Standard Deviations of Maternal Functioning Outcomes by Days at Shelter and Time.

Note. Multivariate effect = F(6, 119) = .41, p = .871, η2 = .020, Observed Power = .166. BSI = Brief Symptom Inventory; PTSD = Post-Traumatic Stress Disorder.
Similarly, results from a MANCOVA testing for differences in maternal resilience (safety behaviors, general self-efficacy, social support, marginalization) when controlling for the covariates already mentioned yielded no significant effects of time at shelter on all measures of maternal resiliency, providing additional support for the argument that any time spent at a safe shelter has positive impacts of female survivors of intimate partner violence (see Table 4). Thus, at 4 months following a shelter stay, women had higher levels of resiliency regardless of the amount of time spent at the safe shelter.
Means and Standard Deviations of Maternal Resiliency Outcomes by Days at Shelter and Time.
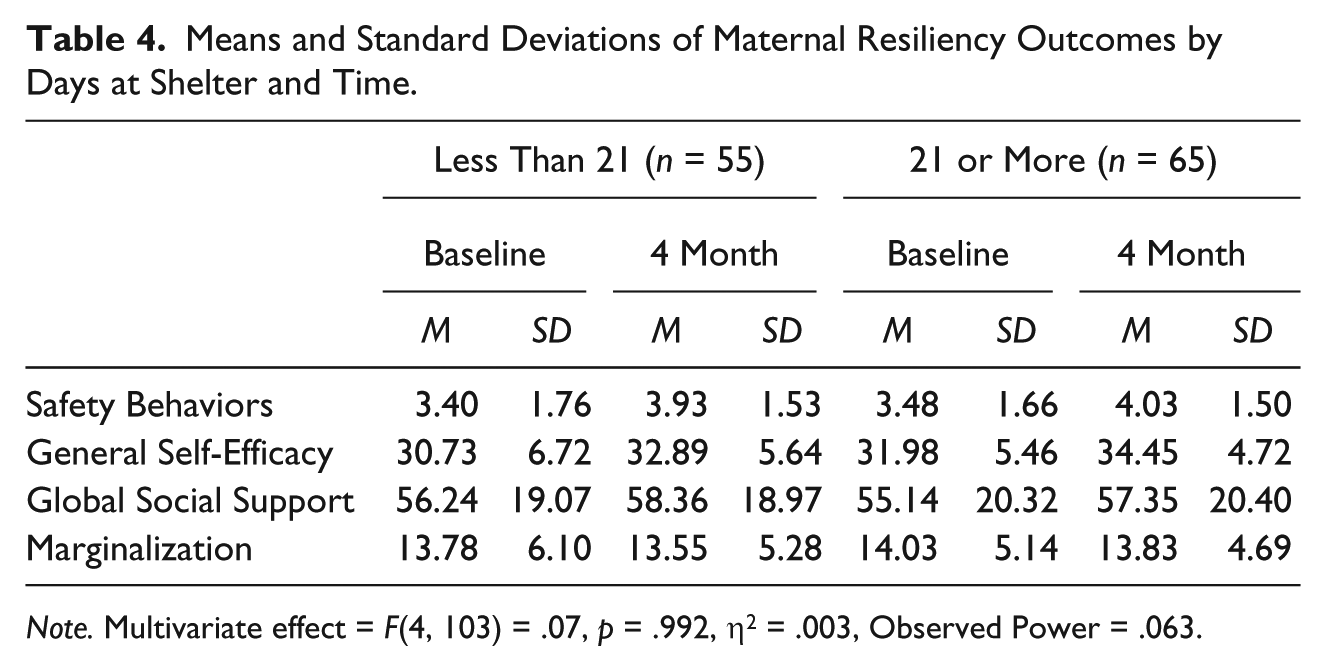
Note. Multivariate effect = F(4, 103) = .07, p = .992, η2 = .003, Observed Power = .063.
Last, a MANCOVA was conducted to test for differences in maternal abuse (danger, threats, physical abuse, sexual abuse) at 4 months depending on the amount of time at the shelter. Analysis regarding length of time at the shelter yielded no significant effect of time at shelter on maternal abuse factors (see Table 5). Both groups of sheltered women, women staying less than 21 days and 21 or more days, had decreases in abuse from baseline to 4-month follow-up, indicating that regardless of the amount of time spent in shelter, women’s reported level of abuse decreased at 4-month follow-up.
Means and Standard Deviations of Maternal Abuse Outcomes by Days at Shelter and Time.

Note. Multivariate Effect = F(4, 124) = .52, p = .719, η2 = .017, Observed Power = .173.
Protective Order
To test the function of receiving a PO or not on maternal functioning, maternal resiliency, and maternal reported abuse, a series of MANCOVAs were conducted controlling for physical abuse, sexual abuse, age, working status at intake, ethnicity, level of education, childhood abuse, and maternal danger. Similar to shelter stay, maternal functioning outcomes did not significantly differ based on whether or not a PO was received (see Table 6). Furthermore, across all measures of maternal functioning (anxiety, depression, somatization, PTSD symptoms, pain severity, pain interference), there were decreased levels of maternal distress, indicating that changes in maternal functioning can be best accounted for by the change over time, and not a function of whether or not the PO was received. Similarly, there was not a significant interaction between whether or not a woman received a PO on time or any of the included covariates (see Table 7). Last, there was not a significant effect of receiving a PO on maternal reported abuse (see Table 8). The analysis indicates that changes in danger and severity of abuse appears to be a function of time rather than whether or not a woman received a PO.
Means and Standard Deviations of Maternal Functioning Outcomes by Whether or Not PO Received and Time.
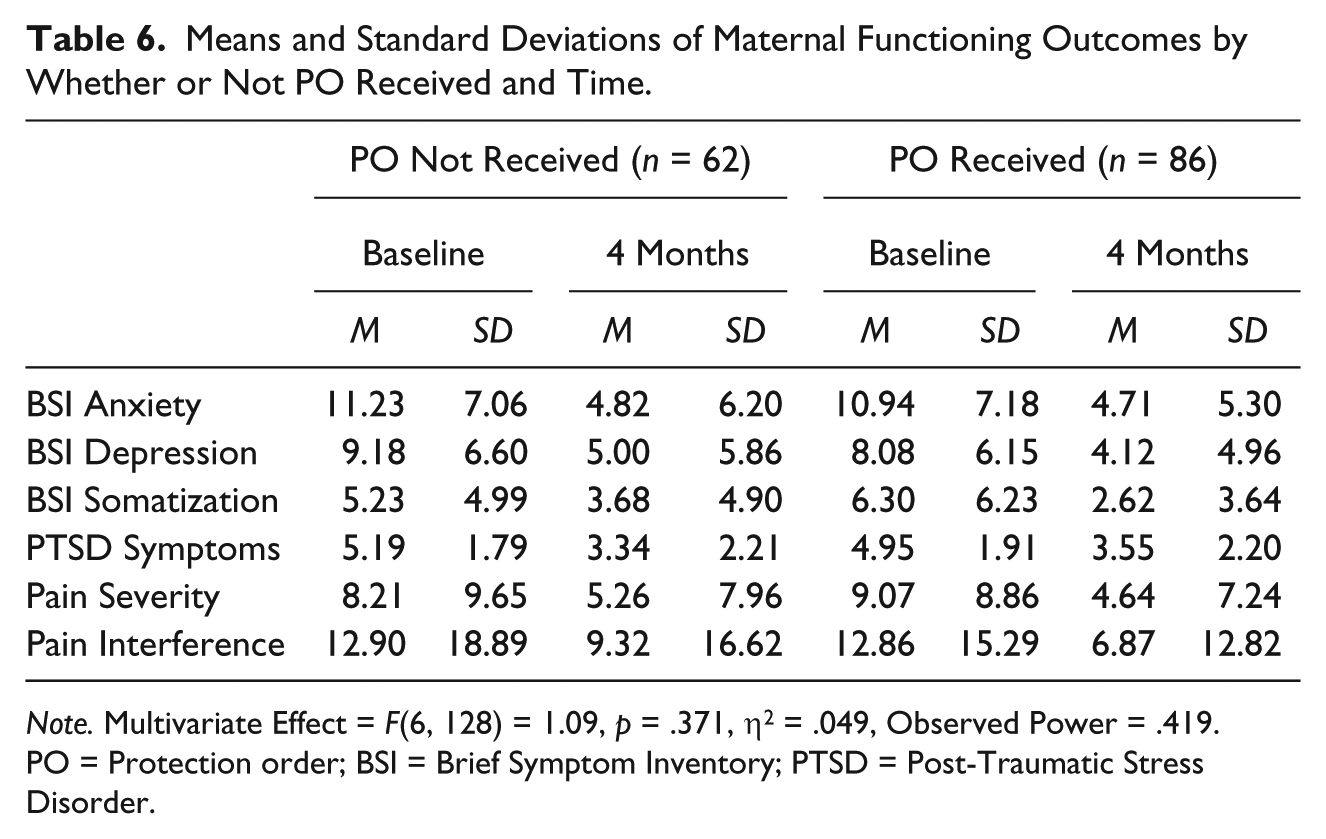
Note. Multivariate Effect = F(6, 128) = 1.09, p = .371, η2 = .049, Observed Power = .419. PO = Protection order; BSI = Brief Symptom Inventory; PTSD = Post-Traumatic Stress Disorder.
Means and Standard Deviations of Maternal Resiliency Outcomes by Whether or Not PO Received and Time.

Note. Multivariate effect = F(4, 124) = 1.35, p = .257, η2 = .042, Observed Power = .410. PO = Protection order.
Means and Standard Deviation of Maternal Abuse by Whether or Not PO Received and Time.
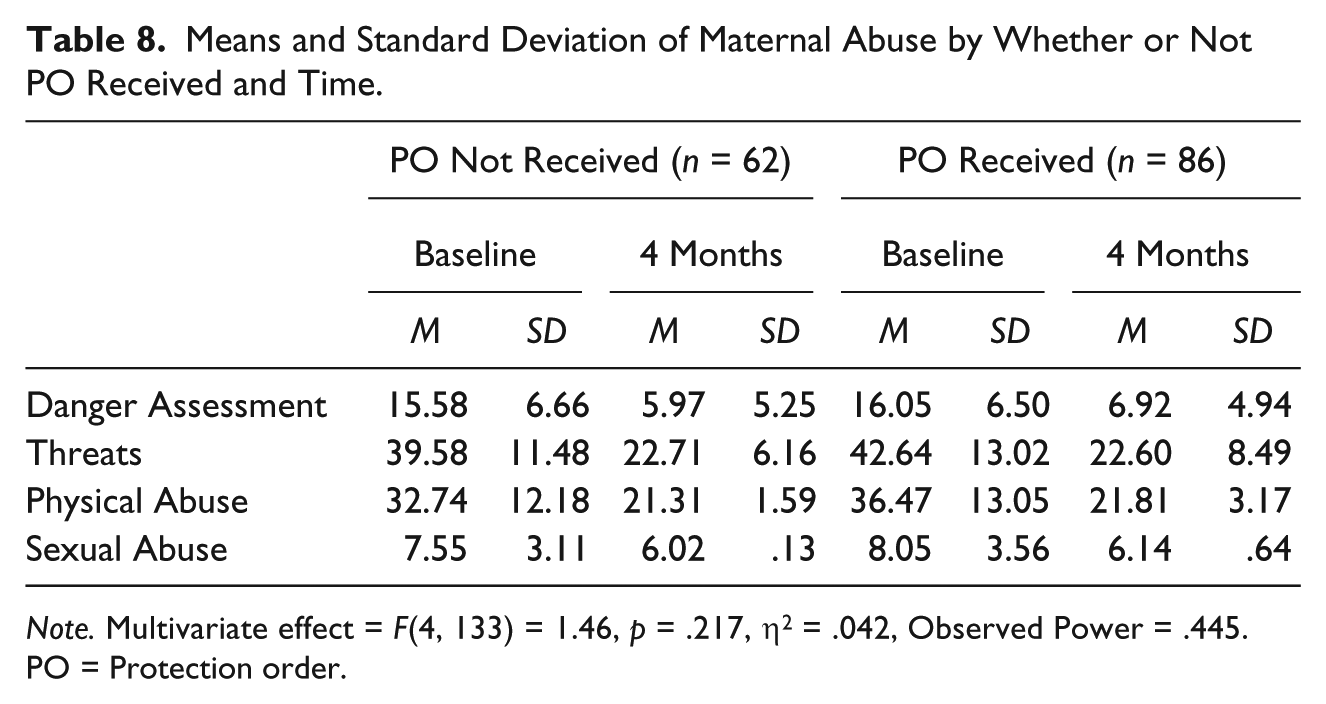
Note. Multivariate effect = F(4, 133) = 1.46, p = .217, η2 = .042, Observed Power = .445. PO = Protection order.
Observed Power Limitations
While efforts were made to determine an adequate sample size to achieve power of .80, when running primary analyses, observed power was lower than expected likely due to weaker effect sizes than initially estimated. These effect sizes and observed power were much lower in the shelter group than the DA group, and as such, these findings should be interpreted with some caution.
Discussion
Length of Shelter Stay
No differences were found between the two shelter groups, providing evidence that at 4 months after entering shelter, women who stayed less than 21 days did not differ on function, resiliency, or abuse from those who stayed 21 days or more. It may be that differences would emerge if factors such as history of childhood abuse and financial status had been controlled for. It is our plan to consider these factors later in the parent study. We suspect that women who seek shelter protection have limited personal, social, and economic resources. It is probable that they need far more help establishing resiliency factors to promote differences in outcomes overtime than were available to the study participants.
PO Received
For most outcomes, among those who sought POs, there were no significant differences between those who received them and those who did not. One exception was that somatization decreased significantly more for those who received POs than for those who did not. Although speculative, it may be that physical symptoms are a proxy for a “cry for help” and that those who perceive that their cry is heard, in the form of receiving a PO, lessen their ongoing “cry.” The other exception was that those who received a PO reported an increase in safety behaviors while those who did not reported unchanged safety behaviors. Again speculative is the possibility that those who received a PO may feel that they have the needed support to act to achieve safety while those who did not lack a sense of having such support. Contrary to the Holt et al. (2003) findings, there was no difference between the two PO groups. It may be that the difference in findings is related to the fact that the Holt findings compared receiving permanent versus non-permanent POs, rather than simply receiving a PO or not. It may be relevant that this study is taking place in the same community where McFarlane et al. (2004) found that violence decreased for women who sought POs regardless of whether they received a PO. If that is the case, then we would not expect a difference between the PO and no PO received groups. Most puzzling is that increased safety behaviors for the PO group did not lead to a difference in safety outcomes. It may be that time is needed to see the effects of changes in safety behaviors and that as the study progresses a difference will emerge.
Among 300 abused women who reached out to safe shelter or justice services for the first time, 4 months following receipt of services, with two exceptions, no measurable outcome differences existed between lengths of shelter stay or receipt versus no receipt of a PO. Both shelter and PO groups reported similar levels of violence, danger, mental health functioning, and resiliency factors. Two exceptions are noted. Abused women who received the PO reported a greater decrease in somatization and adoption of more safety behaviors compared with women who did not receive the PO. Women who did not receive the PO did not change their safety behavior adoption.
Striking is the drastic improvement in functioning and resiliency and decrease in abuse for all women, irrespective of service used or intensity of use. A longer shelter stay was not associated with a greater reduction in abuse or improvement in functioning and resiliency compared with a shorter stay. With the exception of safety behaviors and somatization, receipt of a PO was not correlated with any better outcomes compared with applying for and not receiving the PO. Noteworthy is the increase in safety behaviors for women receiving the PO and decrease in somatization, perhaps related to the acquisition of the order and associated limitation of access of abuser to the woman.
How do we account for the reduction in abuse and improvement in function and resiliency, irrespective of service received or dose of the service? When an abused woman decides to access a shelter or apply for a PO, or responds affirmatively to screening questions about abuse, information about the abused is shared, and contact is made. Just as privatization of abuse contributes to its continuation, acknowledgment of the abuse, affirmation that she is not alone, and knowledge that help is available can empower the woman to take actions to interrupt the violence, prevent reoccurrence, and result in better functioning.
A qualitative study (Fischer & Rose, 1995) examined why abused women seek orders of protection. The women discussed the PO as a “loudspeaker” to notify the abuser that the law knew about the abusive behavior. The legal system was viewed as a force larger than the woman that possesses power over the abuser that the woman had lost as a result of the abuse. Application for the PO became an announcement that the abused woman refused to “take it” anymore. Acknowledgment of the abuse, whether to justice or shelter personnel or health care and social service providers, can function to name the abuse and open the window of services and a larger network of providers to assist the woman in decision making and safety seeking.
Limitations
Our methodology has limitations that may under-represent victimization and functioning outcomes of abused women who access justice services for a PO or seek safe shelter for the first time. First, the sample was a convenience sample and although we were present at the shelters and DA’s office daily, the possibility exists that women were missed. Furthermore, we only sampled from shelters designated for abused women; therefore, abused women who access a shelter for homeless persons would have been missed. In like fashion, abused women who seek orders of protection from a private lawyer or legal service other than the county DA’s office would have been missed. Another limitation of the sample could be that women who sought services either through the justice system or through safe shelters have differing characteristics, which has driven the avenue in which they reach out for support. One way in which we attempted to minimize these differences is by running analysis on each group separately, so that inferences made about each group are not overgeneralized to all abused women seeking support for the first time. Our participants were limited to English and Spanish speakers. Second, participants may have underreported or minimized victimization or functioning status. Third, the questions may miss some episodes of victimization and incorrectly classify others. The study was limited in the types of violence against women that were measured; for example, financial and spiritual abuse was not measured. The researchers acknowledge recall bias was operant in all responses. Finally, the majority of the women were not in a relationship with the abuser at the time of entering the shelter or application for a PO. How this separation may impact the findings is unknown. Despite these limitations, the researchers feel this study provides the most detailed and comprehensive data available on abused mothers who use the justice and safe shelter services for the first outcome and subsequent safety, re-abuse, and functioning status.
Conclusion
Among 300 abused women who reached out to safe shelter or justice services for the first time, 4 months following receipt of services, with two exceptions, no measurable outcome differences existed between lengths of shelter stay or receipt versus no receipt of a PO. Both shelter and PO groups reported similar levels of violence, danger, mental health functioning, and resiliency factors. Two exceptions are noted. Abused women who received the PO reported a greater decrease in somatization and adoption of more safety behaviors compared with women who did not receive the PO. Women who did not receive the PO did not change their safety behavior adoption.
Footnotes
Acknowledgements
We appreciate the unflagging assistance and support of the administrators and staff of the five shelters in Harris County and the chief and staff of The Harris County District Attorney’s Office, Family Criminal Law Division. The 300 women and children who allowed us to record their pain and recovery took emotional risks each time we met. As one woman said, “I want to talk but it hurts to remember.” We thank each woman who chose to remember and dedicate the findings of this research to her courage and determination.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge funding by The Houston Endowment.