
Abstract
The present study examined emotion dysregulation, coping drinking motives, and alcohol-related problems as predictors and consequences of alcohol-involved sexual assault (AISA). A convenience sample of 424 college women completed confidential surveys on paper and online. Data were collected at baseline (T1), weekly for 10 weeks (T2-10), and at 1 year (T11). The cross-sectional and longitudinal associations among variables were examined in a cross-lagged panel model. Within each time point, all variables were correlated. Drinking to cope and emotion dysregulation predicted AISA in the short term (within 10 weeks), alcohol problems increased risk for AISA in the long term (within 1 year), and AISA history predicted AISA revictimization regardless of time frame. Drinking to cope and alcohol-related problems predicted future victimization, but their impact seems to fluctuate over time. Coping drinking motives were both a predictor and consequence of AISA, suggesting a cyclical pattern. However, additional analyses indicated that coping drinking motives and alcohol problems might act as suppressors in the model. Overall, findings indicate that interventions focused on improving emotion regulation skills may decrease short-term risk for AISA.
Keywords
Sexual assault is a public health concern within the United States that has garnered increasing attention over the last several decades. Although the lifetime prevalence of sexual assault within the general population of women is already alarmingly high (11%-18%), the prevalence of sexual assault increases substantially during the college years, with one in four women reporting attempted or completed sexual assault (Gross, Winslett, Roberts, & Gohm, 2006; Post, Biroscak, & Barboza, 2011). Various forms of sexual assault exist. Emerging research suggests alcohol-involved sexual assault (AISA) is more prevalent than forcible sexual assault among female college students (Lawyer, Resnick, Bakanic, Burkett, & Kilpatrick, 2010), with risk for AISA increasing upon entry to college and risk for forcible assault decreasing (Krebs, Lindquist, Warner, Fisher, & Martin, 2009). One study of college women indicated that the likelihood of experiencing sexual assault may be as much as 19 times higher on days when women engage in heavy drinking (Parks, Hsieh, Bradizza, & Romosz, 2008).
Heavy drinking in college women has been linked with rape and sexual assault in general (Krebs et al., 2009; Mohler-Kuo, Dowdall, Koss, & Wechsler, 2004), with AISA specifically (Kaysen, Neighbors, Martell, Fossos, & Larimer, 2006; Marx, Nichols-Anderson, Messman-Moore, Porter, & Miranda, 2000; McCauley, Calhoun, & Gidycz, 2009), and appears to play a role in sexual revictimization (Messman-Moore, Ward, & Brown, 2009; Walsh et al., 2013). However, at least one study suggested that the victim’s alcohol use does not predict forcible assault (Testa, Livingston, VanZile-Tamsen, & Frone, 2003). Thus, more studies are needed to examine risk specifically for alcohol-related sexual assault. This is particularly important given that rates of heavy episodic drinking among young women, particularly college women, are on the rise (Grucza, Norberg, & Beirut, 2009). This shift in drinking patterns is even more disturbing given that college women seem to be more likely than college men to experience alcohol-related problems including tolerance, blacking out, passing out, and injury as a result of their drinking (Sugarman, DeMartini, & Carey, 2009). In fact, some of the negative consequences of heavy drinking, such as passing out, may contribute to women’s vulnerability to AISA. Alcohol use by the perpetrator, victim, or both parties is a factor in almost 75% of college sexual assaults (Mohler-Kuo et al., 2004); however, few studies have presented practical interventions to successfully prevent sexual assault of women. It is critical to acknowledge that the ultimate responsibility for sexual assault lies with perpetrators who choose to violate unconscious or incapacitated women. Although research, particularly with men, that examines beliefs, values, and other characteristics that enable, support, or condone sexual aggression is necessary to prevent and eliminate sexual violence, such research is incomplete. It remains important to simultaneously identify potential points of intervention that may enable women to more effectively cope with risky situations.
Numerous prospective studies have documented that heavy alcohol use, or alcohol-related problems, predict risk for AISA (Kaysen et al., 2006; Messman-Moore et al., 2009). Some prospective studies also suggest that heavy alcohol use or alcohol-related problems also increase following sexual assault (see Kaysen et al., 2006, but not Gidycz et al., 2007), which may indicate a cyclical pattern. Among college women, heavy alcohol use and sexual assault are definitely linked. Most studies support a model that alcohol use increases risk for sexual assault, but the mixed findings for problematic alcohol use increasing as a result of sexual assault warrant further investigation to clarify this relationship. The strongest evidence utilized a 3-year prospective design and suggests a cyclical pattern—finding that women’s alcohol use is elevated prior to experiencing alcohol-involved rape, and that alcohol use (and alcohol-related problems) increases following such assault (Kaysen et al., 2006). Unfortunately, because data were collected at 1-year increments, Kaysen and colleagues could not determine, in any given year, whether alcohol-involved rape predicted increased alcohol use/problems or vice versa.
If alcohol use or alcohol-related problems do increase following sexual assault, such patterns would be consistent with a self-medication or coping model, which would predict an increased propensity for women to use alcohol to cope with the negative effects of sexual abuse (Grayson & Nolen-Hoeksema, 2005). Although few studies have examined whether sexually assaulted women drink to cope, at least one suggests that sexual coercion among college students is correlated with higher levels of drinking to cope (Fossos, Kaysen, Neighbors, Lindgren, & Hove, 2011). Other studies focusing on coping and alcohol use suggest adolescent girls and young women report using alcohol to improve their mood or cope with problems (Borjesson & Dunn, 2001; Cooper, 1994; Norberg, Norton, Olivier, & Zvolensky, 2010). Young women are also more likely than young men to initiate heavy episodic drinking to escape or alleviate distress (Liu & Kaplan, 1996), and use alcohol in the context of emotional pain (Beck, Thombs, Mahoney, & Fingar, 1995). Given that young women have a greater tendency to drink in the context of negative affect (Norberg et al., 2010), it is important to examine how drinking to cope may function not only as a risk factor for sexual assault but as an outcome as well.
Correlational data suggest women use alcohol to cope with psychological distress related to sexual assault (Miranda, Meyerson, Long, Marx, & Simpson, 2002) and that drinking to cope is elevated among survivors of sexual assault (Fossos et al., 2011; Ullman, Filipas, Townsend, & Starzynski, 2005). Emotion dysregulation, which includes the inability to identify and utilize adaptive coping strategies, may contribute to drinking to cope. Emotion dysregulation is not limited to maladaptive coping strategies; it also involves impaired emotional awareness and clarity, rejection of emotional experiences, as well as the inability to inhibit maladaptive coping responses when distressed (Gratz & Roemer, 2004). Although emotion dysregulation is associated with different forms of psychopathology including substance use disorders (see Aldao, Nolen-Hoeksema, & Schweizer, 2010, for a review), it is not a clinical condition per se. In fact, it may best be understood on a continuum from emotion dysregulation to healthy emotion regulation, and has been studied in adolescents and college students as well as in clinical populations (Gratz & Roemer, 2004). Emotion dysregulation may be an underlying mechanism for utilizing substances to cope with distress, which in turn may be placing women in more risky situations and increasing their likelihood of revictimization (Filipas & Ullman, 2006; Grayson & Nolen-Hoeksema, 2005), although studies have not yet assessed this specifically. The few studies examining emotion dysregulation in the context of sexual assault report an association with repeated sexual victimization (Messman-Moore, Walsh, & Dilillo, 2010; Walsh, Dilillo, & Scalora, 2011), but do not specifically examine AISA or focus on women’s alcohol consumption. Although there is evidence that women’s alcohol use/problems increase vulnerability for AISA, there is less research examining whether emotion dysregulation and drinking to cope predict risk for AISA, or if sexual assault predicts emotion dysregulation or drinking to cope.
Study Aims and Hypotheses
Although the literature is mixed, it suggests overall that women’s alcohol consumption is a risk factor for AISA (Kaysen et al., 2006; Marx et al., 2000; McCauley et al., 2009). This consumption may also be an outcome of sexual assault (see Kaysen et al., 2006; but not Gidycz et al., 2007). Thus, it is critical to utilize prospective designs that examine proximal associations to determine whether risk factors precede, rather than follow AISA, as well as determine the possible bidirectional influence of these experiences. The present study utilized a multi-wave, prospective design to examine the relationships among emotion dysregulation, drinking to cope, alcohol-related problems, and AISA to determine how variables co-vary and predict AISA over time. Follow-up periods examined predictors and outcomes in both the short term (i.e., 10 weeks) and the long term (i.e., 1 year).
The primary focus of the current study was to examine both predictors and consequences of AISA. Specifically, we aimed to determine (a) whether emotion dysregulation and coping drinking motives increase risk for subsequent AISA while accounting for the presence of alcohol-related problems and (b) whether experiencing such an assault increases levels of emotion dysregulation, coping drinking motives, and alcohol-related problems. It was hypothesized that AISA would be predicted by emotion dysregulation, drinking to cope, and alcohol-related problems. Given the mixed literature to date (e.g., Gidycz et al., 2007; Kaysen et al., 2006), the role of AISA as a predictor of such problems was explored. Consistent with earlier studies on revictimization, it was also hypothesized that prior AISA would significantly predict subsequent AISA. Given the purpose of the study, we examined emotion dysregulation explicitly and drinking to cope versus drinking in general, in the context of alcohol-related problems, as predictors of AISA.
Method
Participants were 424 female undergraduates at a midsized, public, rural university in the Midwest; average age was 19.78 (SD = 1.30). The sample included women across all 4 years of education (19.4% first-year students, 22.3% sophomores, 22.1% juniors, and 27.4% seniors). Participants identified as Caucasian (88.4%), 26% were members of a sorority, 98.3% were unmarried, 72.4% were sexually active, and 48.6% reported being in an exclusive romantic relationship. The sample was predominantly upper-middle class, with 46.2% of participants reporting a family income greater than $100,000.
Measures
Alcohol-related problems
Alcohol-related problems were assessed at the study onset (Time 1), after the initial 10 weeks (Time 10), and 1 year later (Time 11) with the 23-item Rutgers Alcohol Problem Index (RAPI; White & Labouvie, 1989). Participants indicated how many times certain behaviors or problems occurred due to their alcohol consumption (e.g., “Not able to do your homework or study for a test”). Using a 5-point Likert-type scale from 0 = “never” to 4 = “more than 10 times,” the scale is scored by summing the 23 items. Instructions varied depending upon the time point assessed, with referent periods differing accordingly (Time 1 = past 3 years, Time 10 = past 9 weeks, Time 11 = past year). Higher levels mean more problematic drinking tendencies. In the current sample, the internal consistency for the RAPI was .90, .86, and .91 for Time 1, Time 10, and Time 11 respectively. See Table 1 for the means and standard deviations at each time point.
Descriptive Statistics and Correlation Matrix for Study Variables.

Note. During the 9-week follow-up period, Cronbach’s alpha average for the Coping Drinking Motives subscale was .86, and ranged from .84 (Week 8) to .88 (Week 7). DERS = Difficulties in Emotion Regulation Scale; RAPI = Rutgers Alcohol Problem Index; AISA = alcohol-involved sexual assault.
p< .05. **p < .01. ***p< .001.
Coping drinking motives
The coping subscale of the Drinking Motives Questionnaire–Revised (DMQ-R; Cooper, 1994) was used to assess drinking to cope (e.g., “To forget your worries”). Participants indicated how often they drank due to coping motives using a 5-point Likert-type scale (1 = “almost never/never” to 5 = “almost always/always”). Higher scores indicated that they used alcohol to cope more often. Participants completed the coping subscale weekly and again at the 1-year follow-up (Time 11). The coping subscale scores were averaged across Weeks 2 to 10. The internal consistency for the coping motives scale was .86 at each time point in the current sample.
Emotion dysregulation
The total score of the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was used to assess emotion dysregulation. The DERS is comprised of 36 items on six subscales, with higher scores indicating greater emotional dysregulation. All items are scored on a 5-point Likert-type scale from 1 = “almost never” to 5 = “almost always” indicating how often the participant experienced the statement. The total score measures emotion dysregulation that is reflected in a lack of emotional awareness, a lack of emotional clarity and personal understanding of emotions, the failure to accept feeling distressed, problems in the ability to control behaviors when experiencing negative affect, limited access to effective emotion regulation strategies, and difficulties accomplishing tasks when experiencing a negative emotion. Among untreated individuals, DERS scores are relatively stable over 14 weeks (Gratz & Tull, 2010). The DERS was administered in its entirety at Time 1 and Time 11. For brevity, the DERS was shortened for each weekly administration, utilizing the three items from each of the subscales, based on the highest factor loadings for each item published by Gratz and Roemer. This shortened the measure from 36 items to 18 items for weekly administrations. Internal alpha coefficients were excellent, and generally higher at the weekly administrations compared with the general (Time 1, Time 11) administrations. As with the coping drinking motives subscale, the shortened DERS total scores were averaged across weeks T2 to 10. See Table 1 for the means, standard deviations, and internal consistencies across time points.
AISA
The revised Sexual Experiences Survey (Koss et al., 2007) was administered at Time 1 (the first week of the study) to ascertain AISA victimization experiences from age 14 until entrance into the study. The revised Sexual Experiences Survey (SES) was re-administered weekly (Times 2-10) and at the 1-year point to identify prospective victims of AISA. For each week, several different questions assessed unwanted sexual experiences related to respondent alcohol and drug consumption for each of the three different types of unwanted sexual contact (kissing/fondling, oral-genital contact, and intercourse). Responses to these questions were collapsed together to assess AISA during each week. AISA was coded as a dichotomous variable (Yes = 1, No = 0) reflecting victimization prior to the study (Time 1) and at the 1-year follow-up (Time 11); given the low base rate of sexual assault, weekly affirmative responses across the 9-week period were aggregated into one variable reflecting victimization during the initial 9 weeks (Times 2-10).
Procedure
The committee for human subjects in research approved all procedures. Participants were recruited through fliers posted on campus and advertisements in the student newspaper. The study spanned 10 weeks with data collection at 1-week intervals. At the beginning of the study (Time 1), participants completed paper-and-pencil surveys. Women then completed online (Internet-based) surveys weekly (Times 2-9), and returned to complete paper-and-pencil surveys at Time 10. At Time 11 (1-year follow-up), all participants were invited via email to complete the survey online. Participant responses were linked via a unique identification number. All in-person data collection took place in group sessions staffed by female research assistants. Participants received an honorarium of $25 for the first session, and were eligible to earn up to $75 for Sessions 2 to 10 (pro-rated based on number of surveys completed, up to $50, with an additional $25 for completion of all 10 surveys), $25 for the last session, and a $25 bonus for completion of all sessions; thus, those participants who completed all sessions of the study received a total of $125. Following participation each week, women received information regarding counseling and support services, as well as researcher contact information.
Results
The main purpose of the study was to examine both predictors and consequences of AISA. To accomplish this, the cross-sectional and longitudinal associations among emotion dysregulation, coping drinking motives, alcohol-related problems, and AISA were examined in a panel model. Three time points were utilized to assess relationships over both short periods of time (10 weeks) and longer periods of time (1 year): Time 1 (entry to the study), Times 2-10 (averaged over the next 9 weeks of the study), and Time 11 (1 year following Time 10).
Descriptive Statistics
Regardless of drinking status, all women were included in all analyses. However, almost 90% reported drinking at some point prior to the study. On average, their first drink occurred at 16.03 years old (SD = 2.01). At Time 1, the sample’s recent drinking behavior was fairly heavy overall. The majority of women (68.2%) reported heavy episodic drinking (consuming 4 or more drinks on at least one occasion) in the last month: 14.6% engaged in heavy episodic drinking once, 19.1% 2 to 3 times, 20.8% 4 to 6 times, and 13.7% 7 or more times. During the last 30 days, the average peak consumption reported on one occasion was 5.67 standard drinks (SD = 4.30). At Time 10, 61.3% reported having consumed alcohol in the previous week, and 49.1% reported heavy episodic drinking on at least one occasion in the past week. The average peak consumption for the past week was 6.12 (SD = 4.52) standard drinks. At the 1-year follow-up (Time 11), 72.6% reported consuming alcohol in the previous year, and 58.5% reported heavy episodic drinking in the previous month. The average peak consumption for the past month at the 1-year follow-up was 5.66 (SD = 3.73) standard drinks.
At baseline, 32.1% (n = 139) women reported experiencing a history of AISA (i.e., at least one AISA since age 14 but prior to the study). During the 10-week study (Times 2-10), 5.7% (n = 24) reported at least one incident of AISA. At the 1-year follow-up, 4.5% (n = 19) reported at least one incident of AISA. Means, standard deviations, and correlations for study variables are in Table 1. Within each time point (i.e., T1, T2-10, T11), all variables were significantly correlated, and each variable was correlated with itself across time points, suggesting significant stability of each construct.
Structural Equation Models
Maximum likelihood estimation was used to examine relations between the constructs within a structural equation modeling framework utilizing Mplus version 6.11 (Muthén & Muthén, 1998-2011). The proposed models were based on theoretical predictions and were examined using the following criteria: (a) theoretical salience, (b) microfit indices (i.e., parameter estimates and residuals), and (c) global fit statistics (i.e., comparative fit index [CFI], Tucker–Lewis index [TLI], chi-square). To meet standards of theoretical salience, the model must be predicted from documented theory and previous research. For root mean square error approximation (RMSEA), a fit of less than 0.05 will be taken to indicate a well-fitting model (Browne & Cudeck, 1992). For global fit indices, a non-significant chi-square indicates that the data do not significantly differ from the hypotheses represented by the model; for CFI and TLI, fit indices of above .90 (preferably above .95) will be the criteria utilized to indicate a well-fitting model (Hu & Bentler, 1999).
Initial Model Results
The model fit the data well, χ2(19, n = 424) = 44.11, CFI = .98, TLI = .92, RMSEA = .06. Within each panel, AISA was associated with emotion dysregulation, coping drinking motives, and alcohol-related problems (ps < .01). High levels of emotion dysregulation and drinking to cope at T1 predicted a greater likelihood of AISA at T2 to 10, and high levels of emotion dysregulation and alcohol-related problems at T2 to 10 predicted AISA at T11 (see Figure 1). AISA did not predict emotion dysregulation or alcohol-related problems in the short term (T2-10) or over the long term (T11), although AISA during the initial 10 weeks (T2-10) did predict drinking to cope at the 1-year follow-up (T11; see Figure 2). All significant relationships were in the hypothesized direction, with one exception; high levels of emotion dysregulation at T2 to 10 were associated with lower risk for AISA at T11. This negative association stood in contrast to the positive bivariate correlation between the variables (see Table 1), which may be an indicator of suppression.
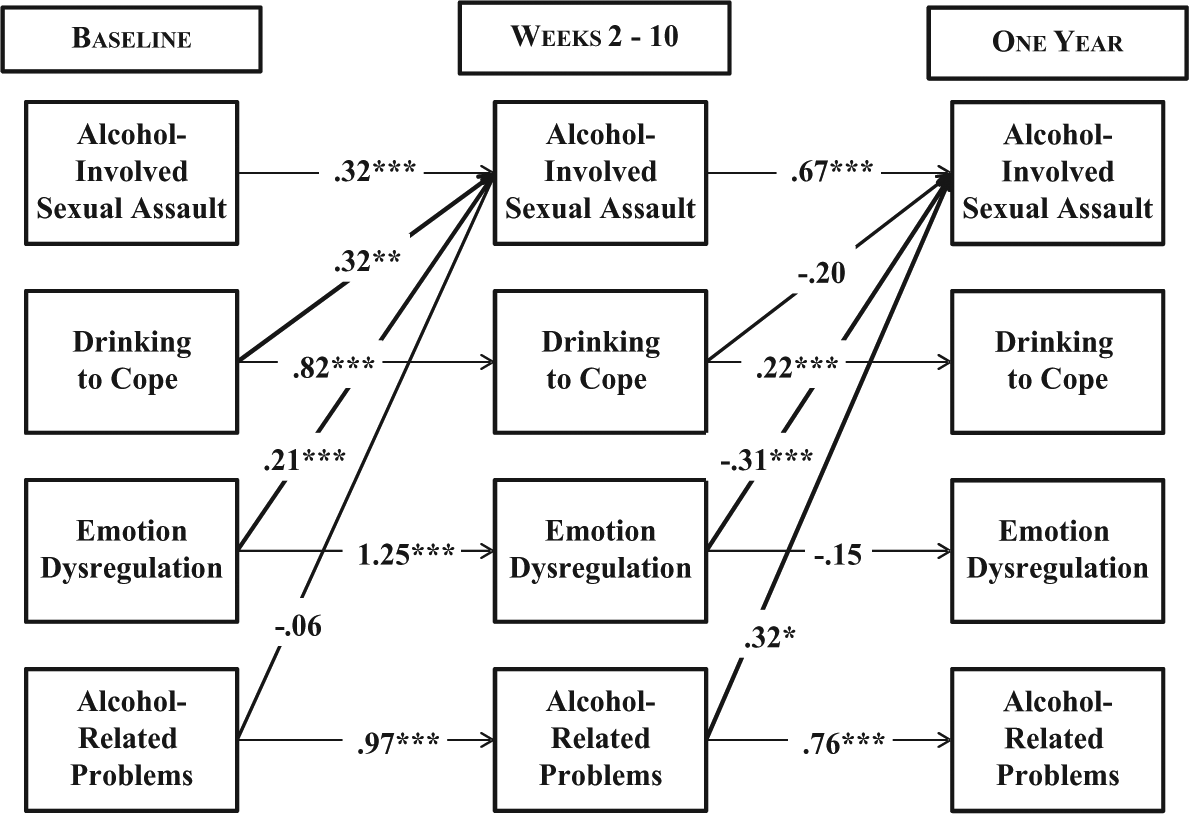
Predictors of alcohol-involved sexual assault across time.
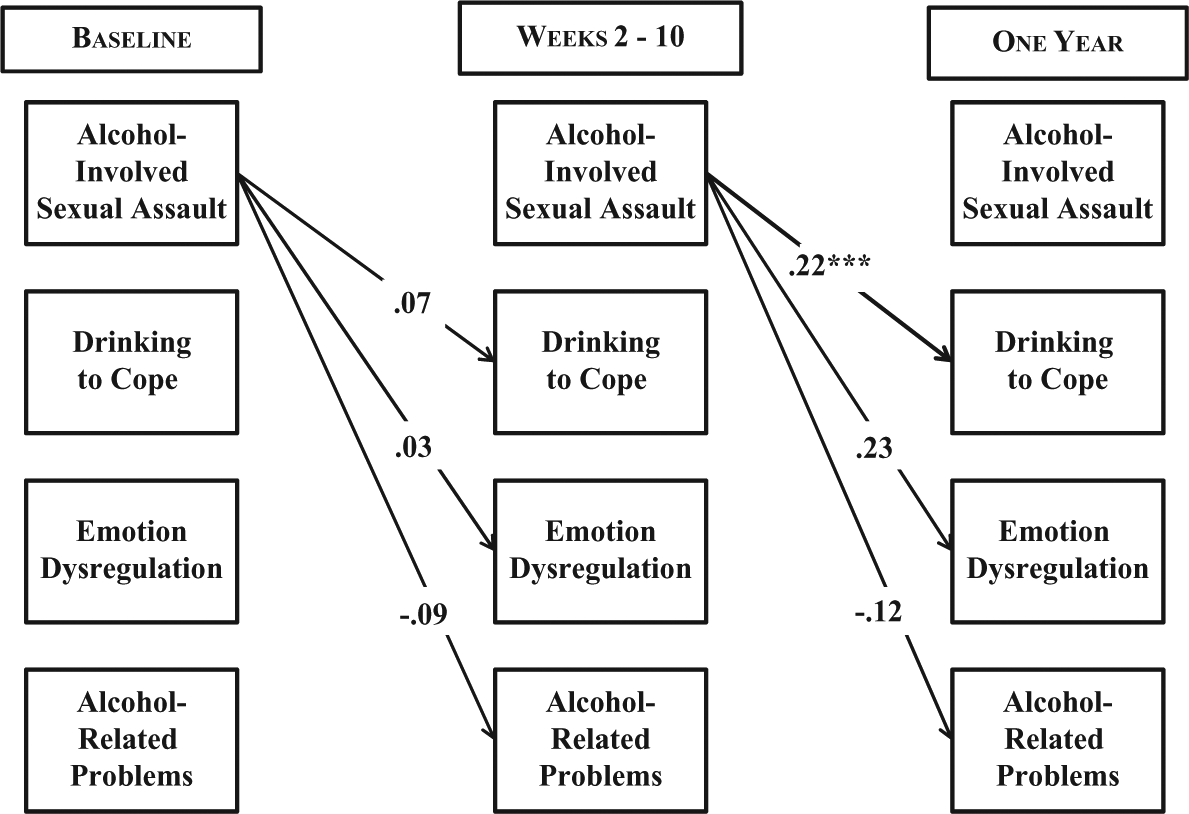
Consequences of alcohol-involved sexual assault across time.
Examination of Suppression Effects
Upon examination of the semi-partial correlations, correlations, and parameter loadings, the model seemed to be affected by a suppressor or several suppressors. Following the recommendations of Maassen and Bakker (2001) and Velicer (1978), the model was examined to determine which variable or linear composite of variables were suppressing the relationships. Given the inconsistent relationships in the semi-partial correlations, it was possible that the longitudinal design might be suppressing the relationships (i.e., the linear composite of each panel). A model examining the short-term variables (i.e., Time 1 and Time 2-10) had poor global fit, χ2(6, n = 424) = 64.63, CFI = .93, TLI = .68, RMSEA = .15. In addition, a model examining the long-term effects (i.e., Time 2-10 predicting T11) had poor global fit and a lot of non-significant paths, χ2(6, n = 424) = 34.43, CFI = .95, TLI = .75, RMSEA = .11.
A systematic series of models attempted to parse out the impact of the suppressor(s). The first model removed AISA at baseline due to the length of the retrospective nature of the variable (i.e., since age 14). The model fits well, χ2(15, n = 424) = 23.74, CFI = .99, TLI = .97, RMSEA = .04, but the suppressor effect was still present. Examining the possibility that AISA was the suppressor, a model with only DERS, drinking to cope, and RAPI only was examined. It had poor global fit, χ2(12, n = 424) = 120.88, CFI = .90, TLI = .73, RMSEA = .15. Next, to examine the most basic model with the central construct of interest, a model of AISA across time was examined. It fit well globally, χ2(1, n = 424) = 1.75, CFI = .98, TLI = .92, RMSEA = .04. However, this model does not provide information concerning the impact of the other variables. To build from this model and to further examine the suppression of effects of alcohol-related problems and drinking to cope, models were tested with AISA and one of the alcohol variables. The model of AISA and alcohol-related problems had mixed global fit and not many predictive paths. The model of AISA and drinking to cope had mixed global fit, but the T2 to 10 paths did not predict T11 paths. To further parse out the relationship, a model of drinking to cope and alcohol-related problems (with DERS and AISA removed) had good overall fit and adequate predictive paths. However, it failed to examine the impact of AISA.
A model of AISA, drinking to cope, and alcohol-related problems (removing DERS) fit well globally, χ2(7, n = 424) = 12.67, CFI = .99, TLI = .96, RMSEA = .04, but the impact of the suppressor was more pronounced. Given the bivariate correlations, parameter loadings, and semi-partial correlations, it seems that alcohol-related problems (as measured by the RAPI) and drinking to cope have a reciprocal suppressive relationship. Given this reciprocal relationship, a model with AISA and emotion dysregulation only (DERS) was tested. It fit the data well, χ2(4, n = 424) = 6.95, CFI = .99, TLI = .97, RMSEA = .04. See Figure 3 for the parameter estimates.
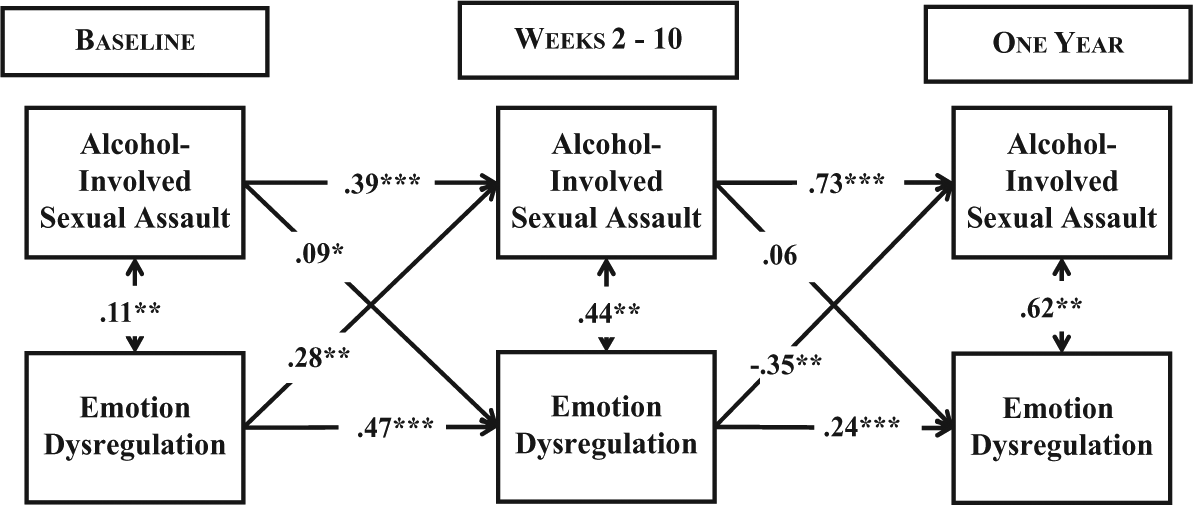
Relationship between emotion dysregulation and alcohol-involved sexual assault across time.
Discussion
The model under examination appeared to best explain risk factors for AISA rather than its consequences. Emotion dysregulation and drinking to cope predicted risk for AISA over the initial 10 weeks, whereas higher levels of alcohol-related problems at the end of the 10-week period were associated with greater risk for sexual assault at the 1-year follow-up. In contrast, in models containing all alcohol-related and emotion-related variables, AISA predicted few of the examined outcomes—the exception was the prediction of drinking to cope at the 1-year follow-up by sexual assault that occurred during the 10-week assessment period. However, another model which focused on emotion dysregulation indicated that AISA at baseline predicted emotion dysregulation during the 10-week period. Although AISA failed to predict increases in emotion dysregulation over the long-term or negative alcohol-related consequences, AISA is associated with other negative consequences that were not the focus of the current investigation, including psychological distress and posttraumatic stress disorder (PTSD; Brown, Testa, & Messman-Moore, 2009).
Findings suggested a potential reciprocal relationship between AISA and drinking to cope. The current study provides additional evidence to support a model that AISA predicts increases in drinking to cope, and that the relationship between drinking to cope and alcohol-related sexual assault may be cyclical. To date, we are aware of no other studies examining drinking to cope and AISA prospectively. However, these findings are consistent with another study of college women which found concurrent and prospective increases in alcohol use following alcohol-involved rape in 1-year intervals (Kaysen et al., 2006). Together, these two prospective studies suggest a cyclical pattern between AISA and alcohol consumption or drinking to cope (Kaysen et al., 2006, examined general alcohol consumption). Nonetheless, the current findings also contradict another investigation in which drinking behavior in college women did not change following sexual assault (at 2 or 6 months; Gidycz et al., 2007). Differences between the studies may be related to the type of drinking assessed (heavy drinking in general vs. drinking to cope), the length of follow-up periods, or the definitions of sexual assault. For example, the current study as well as that by Kaysen and colleagues examined AISA. However, Kaysen et al. (2006) examined alcohol-involved rape specifically, whereas the current investigation included other forms of sexual victimization besides rape. Gidycz and colleagues studied moderate and severe forms (which included rape) of sexual assault but did not focus on AISA. Thus, disparate findings might indicate that the significant relationship lies between alcohol consumption and specific types of sexual assault, that is, AISA (either rape or other types of AISA). The pattern observed among these prospective studies harkens to earlier research which suggested a specific functional relationship between women’s alcohol use and alcohol-involved assaults (Testa et al., 2003).
In contrast to drinking to cope, alcohol-related problems (as measured by the RAPI) were not an outcome of AISA in the current investigation after considering the impact of prior levels of alcohol-related problems. However, Kaysen et al. (2006) found a connection between alcohol-involved rape and an increase in later alcohol-related problems, utilizing the same measure. One potential explanation of these differential outcomes may be related to the severity of the AISA investigated. Disparate findings may suggest a stronger relationship between negative alcohol-related outcomes as a consequence of alcohol-involved rape versus AISA. It may also be that women who experience alcohol-involved rape (rather than sexual assault) are more likely to develop PTSD symptoms, which may then subsequently impact levels of alcohol use and related negative consequences. Kaysen et al. (2010) found that women who experienced an alcohol-related assault (either physical or sexual) initially reported less severe intrusive PTSD symptoms compared to those who had not been drinking prior to assault, but such symptoms took longer to remit in this group. Such lingering psychological distress may predict increased levels of alcohol-related problems over time.
This was the first study to examine emotion dysregulation and AISA. Although the hypothesized reciprocal pattern did not emerge, there was a bidirectional relationship between emotion dysregulation and AISA during the initial 10-week follow-up, suggesting emotion dysregulation may be both an immediate proximal predictor as well as an outcome of AISA. Emotion dysregulation was a robust short-term predictor, given its significance in predicting AISA alongside drinking to cope and alcohol-related problems. Not surprisingly, emotion dysregulation was also positively associated with drinking to cope and alcohol-related problems at each time point. It was beyond the scope of the current investigation to examine all possible relationships, so future studies should focus on whether emotion dysregulation mediates drinking to cope or whether these are two independent risk factors for alcohol-related sexual assault (current results suggest the latter, at least in the short term). Interestingly, over the long term, higher levels of emotion dysregulation were negatively correlated with risk for AISA (at 1 year). However, the direction change in this relationship appears to be due to negative suppression; upon examination of several models, it seems that the linear composite of drinking to cope and alcohol-related problems suppressed each other. In addition, emotion dysregulation and AISA seem to share common elements that act as a suppressing relationship between the T2 to 10 and T11 time points. Further research is warranted to further examine these relationships.
It is noteworthy that the strongest predictor of AISA was prior AISA, despite the theoretically relevant findings that emotion dysregulation may underlie a potentially cyclical relationship between drinking to cope and AISA. Thus, in conjunction with earlier studies (e.g., Messman-Moore et al., 2010; Walsh et al., 2013), the current study provides additional evidence of a strong revictimization effect, and highlights the importance of continuing to identify risk factors in order to develop targeted interventions for women with a history of AISA. Since one of the earliest studies (i.e., Koss & Dinero, 1989), researchers have not yet been able to identify factors that completely explain some women’s increased vulnerability for revictimization. However, recent studies seem to converge in concluding that particular risky behaviors are relevant. One such study examined both alcohol use and risky sexual behavior in the same model predicting sexual revictimization among first-year college women, with structural equation models suggesting an underlying mechanism may account for the high correlation among these behaviors (Testa, Hoffman, & Livingston, 2010). Emotion dysregulation is associated in some form with numerous psychological disorders including PTSD (Aldao et al., 2010), and other known risk factors for sexual revictimization among survivors of child sexual abuse such as substance use, risky sexual behavior, dissociation, and impaired risk perception (Messman-Moore et al., 2010). Based on current findings, it seems likely that this underlying mechanism is emotion dysregulation (Walsh, Galea, & Koenen, 2012), which may explain why suppression was a problem in many of the current models.
This is the first study to examine emotion dysregulation and drinking to cope as predictors and outcomes of AISA while also considering the impact of alcohol-related problems. Nonetheless, the significant contributions of the current findings should be noted in the context of some limitations. The timing of assessment may have been optimal for assessing emotion dysregulation and drinking to cope, but weekly follow-up periods were too brief to assess risk for sexual assault, and thus problematic. The resulting low prevalence of AISA experiences necessitated the collapse of variables that were assessed weekly between T2 and T10, and made it impossible to examine relations among variables at the weekly level. Thus, further spacing of assessment intervals will be important to consider in subsequent studies. Despite these problems, the design was still adequate to allow analyses to distinctly predict risk (and outcomes) of AISA, an improvement over the current literature. The small sample size, along with the low prevalence of AISA, prohibited examination of relationships among variables from week to week, as well as examination of more severe forms of sexual assault such as rape. Differential predictors of alcohol-involved and forcible sexual assault could not be examined because all women who reported forcible assault also reported alcohol-involved assault. It was not clear from assessment whether this overlap constituted two (or more) different episodes of assault or whether both forms of coercion were utilized during the same incident, a drawback of the current SES (Koss et al., 2007). The sample was fairly homogenous in terms of race, ethnicity, and socioeconomic status, and all participants were undergraduate college students. Thus, additional studies with more diverse samples are warranted to replicate the patterns reported. In particular, it will be important to examine similar models with samples of both college students and non-students, to determine whether emotion dysregulation and drinking to cope predict AISA among non-students. The pattern reported here may be unique to the sample, given that female college students have higher rates of alcohol use disorders compared with their same-aged non-student peers (Slutske, 2005). Regardless, it is critical to continue to study college women given the high rates of heavy alcohol consumption and incapacitated sexual assault in this population (Krebs et al., 2009; Lawyer et al., 2010; Slutske, 2005).
The implications for future studies are also important to note. Additional event-based research is needed with larger samples to determine the day-to-day changes in drinking to cope immediately following AISA, as the current findings suggest that drinking to cope may be a critical pathway linking alcohol-involved victimization experiences over time. However, it may also be useful to lengthen assessment periods to a few months (rather than weeks or years), to facilitate assessment of sexual assault as well as risky behavior, as the patterns emerging here were strikingly different for prediction of AISA in the short term and over the long term. Such findings suggest continued examination of the role of emotion dysregulation in general, as well as facets of emotion dysregulation that may be associated with drinking to cope. Emotion dysregulation is often associated with revictimization risk factors including substance use, dissociation, and PTSD, which should be studied together in future investigations. Unfortunately, the current study did not examine PTSD. However, even if it was assessed, its usefulness in analysis likely would have been limited given the very low prevalence of sexual assault-related PTSD in college women (4%; Read, Ouimette, White, Colder, & Farrow, 2011). Thus, future studies will need considerably larger samples to examine this question.
The emergent cycle of AISA, emotion dysregulation, and drinking to cope is consistent with earlier studies (Kaysen et al., 2006), suggesting an important function that alcohol consumption serves for survivors of AISA. Clearly it is critical for interventions to target women’s use of alcohol; however, it seems important to strive for a compassionate, non-judgmental focus on drinking to cope in addition to the more common focus on general levels of heavy drinking (Testa & Livingston, 2009). Interventions which aim to reduce risk for AISA may be informed by emerging research on the link between emotion dysregulation and risky sexual behavior associated with revictimization (Messman-Moore et al., 2010). Findings suggest that emotion dysregulation and drinking to cope may also be significant risk factors, and addressing both issues may be an important contribution to women’s programming.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of numerous research assistants, whose hard work and dedication made this work possible. We would also like to express our gratitude to the women who participated for their commitment to this prospective study and their willingness to share information about potentially distressing unwanted sexual experiences.
Authors’ Note
ABMRF/The Alcohol Foundation had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant to the first author from ABMRF/The Alcohol Foundation.