
Abstract
Abuse in childhood has been established as a predictor of adult abuse, with the strongest associations found between childhood sexual abuse (CSA) and adult sexual victimization. Revictimization has been demonstrated among women, and there is a growing literature on revictimization experiences among men who have sex with men (MSM). No studies have assessed revictimization among MSM living with HIV, despite strong evidence for disproportionately high rates of life span abuse among this group, along with the added vulnerability of living with HIV and sexual minority stress. In this study, we contribute to the literature by exploring associations between multiple types of childhood and adult abuse experiences (physical, sexual, and psychological; perpetrated by partners and non-partner), rather than examining sexual victimization alone. A sample of 166 HIV-positive MSM attending primary HIV health care clinics in Seattle, Washington, completed a one-time questionnaire. Results of regression analyses revealed associations between experiencing CSA and adult sexual abuse, and experiencing childhood physical abuse and adult physical and sexual abuse. Childhood psychological abuse was associated with adult physical and psychological abuse and partner psychological abuse. At higher frequencies, childhood psychological abuse was associated with all forms of adult abuse. These findings suggest that various forms of childhood abuse experiences confer broad vulnerability to adult abuse experiences and point to potentially different pathways to revictimization based on childhood abuse type.
A growing body of research on the health of men who have sex with men (MSM) has revealed high rates of childhood physical, sexual, and psychological abuse, as well as additional forms of violence, such as hate crimes and sexual identity based victimization (Dragowski, Halkitis, Grossman, & D’Augelli, 2011; Herek, 2009). In one large national study, Balsam, Rothblum, and Beauchaine (2005) found that lesbian, gay, and bisexual (LGB) individuals reported more frequent childhood abuse of all types compared with their heterosexual siblings of the same sex; the greatest differences in victimization by sexual orientation were observed for men. In a retrospective study, Wilson and Widom (2010) found that men who reported same-sex partners as adults were more likely to have experienced childhood sexual abuse (CSA) compared with heterosexually coupled men. Based on this association, researchers posit that gender atypical behavior among some young MSM may contribute to this increased vulnerability for experiencing abuse in childhood (as atypical gender expression may lead to social isolation or rejection). Furthermore, this perceived social vulnerability may account for disparities in victimization rates between sexual minority and heterosexual men, as men exhibiting gender atypical behavior may be targeted as victims (Grossman, D’Augelli, Howell, & Hubbard, 2006).
High rates of childhood abuse among MSM, especially CSA, are well-documented in the literature (e.g., Austin et al., 2008; Friedman et al., 2011), and CSA has emerged as a non-specific predictor of a host of negative psychosocial outcomes for this group. For example, MSM with CSA histories are more likely to report polysubstance use (Stall et al., 2001), depression (Stall et al., 2003), suicidal ideation (Arreola, Neilands, Pollack, Paul, & Catania, 2008), and sexual risk behaviors (Mimiaga et al., 2009), compared to MSM without CSA histories. Fewer studies have addressed the long-term consequences of childhood physical or psychological abuse among MSM, including their relation to risk of subsequent victimization. In one study, childhood psychological abuse emerged as the strongest predictor of adult psychopathology (Balsam, Lehavot, Beadnell, & Circo, 2010). In another study, early physical or sexual victimization mediated the associations between LGB identity and suicidality, depression, and alcohol abuse (McLaughlin, Hatzenbuehler, Xuan, & Conron, 2012). Other research has detailed links between childhood physical abuse histories and depression and posttraumatic stress disorder (PTSD) among gay men (Gold, Feinstein, Skidmore, & Marx, 2011). Taken together, these findings suggest that MSM are at increased risk of mental health problems, substance use, and multiple forms of abuse as adults—due to disproportionately high rates of childhood victimization.
It is well-established in the general trauma literature that women who have experienced childhood abuse are at increased risk of subsequent victimization in adulthood (for a review, see Classen, Palesh, & Aggarwal, 2005). Consistent with the broader child maltreatment literature, the investigation of revictimization among MSM has predominately focused on CSA and tends not to examine other forms of childhood abuse and neglect. For example, Kalichman and colleagues (2001) found that one third of their sample of gay and bisexual men reported sexual revictimization (CSA and adult sexual assault). Heidt, Marx, and Gold (2005) found that 24% of gay men and 39% of bisexual men and women reported similarly defined sexual revictimization. Despite high sexual revictimization rates among MSM, there has been little research on the role of other types of childhood abuse and adult revictimization. For example, although rates of partner abuse (PA) among MSM are high (e.g., Greenwood et al., 2002), there has been little research on the differential effects of revictimization by abuse type, or on how childhood abuse experiences are associated with later PA.
There is strong evidence to suggest that MSM living with HIV may be at even higher risk of revictimization compared with HIV-negative MSM, given that revictimization is associated with sexual risk behavior and HIV acquisition (Stall et al., 2003). Numerous studies have shown that a large proportion of HIV-positive MSM report a CSA history (e.g., Bartholow, Doll, Joy, & Douglas, 1994). One study found that 24% of HIV-positive MSM reported CSA histories compared with 14% of HIV-negative MSM (Paul, Catania, Pollack, & Stall, 2001). HIV-positive MSM are also more likely to report high-severity CSA histories than HIV-negative MSM (Brennan, Hellerstedt, Ross, & Welles, 2007). In terms of adult victimization, HIV-positive (vs. HIV-negative) MSM are 1.5 (Greenwood et al., 2002) to 2 times (Stall et al., 2003) more likely to experience PA of all types. Thus, the available data indicate that HIV-positive MSM appear to be at extremely high risk of both childhood abuse and adult revictimization; however, what remains unknown is associations between these and other types of victimization.
Furthermore, a growing body of literature has identified CSA and PA (along with substance use and depression) as having a synergistic effect (i.e., syndemic effect; Singer & Clair, 2003) on sexual risk behavior among MSM, such that each of these experiences has an additive effect on risk of acquiring HIV (e.g., Stall et al., 2003). Thus, individuals possessing a history of CSA and experiencing current PA are more likely to be HIV-positive, relative to having experienced CSA or PA alone. Although these factors are associated with increased likelihood of having HIV (Stall et al., 2003), little is known about how they relate to functioning post-HIV diagnosis. In the present study, we aim to be the first to capture and describe the prevalence of these revictimization experiences in HIV-positive MSM. In doing so, we hope to draw attention to the need for tailored interventions for HIV-positive MSM that address post-abuse sequelae. We hope that our findings will lay a foundation for future research on mechanisms of revictimization in this population. We believe that this line of inquiry is especially important given that both CSA and PA have been associated with poorer HIV health, including medication adherence and health status indicators (e.g., Ironson et al., 2005; Markowitz et al., 2011; O’Cleirigh, Skeer, Mayer, & Safren, 2009).
Given the paucity of research on revictimization among HIV-positive MSM, we aim to provide novel data in this area by establishing the relations between early and later abuse experiences. First, we will investigate associations between various types of childhood and adult abuse experiences (partner and non-partner) to identify risk factors for revictimization. Our study advances the literature by systematically investigating multiple domains of abuse (physical, sexual, and psychological), both during childhood and adulthood, in this uniquely vulnerable population. We expect that the associations between childhood abuse experiences and adult abuse experiences will be similar to those of the broader victimization literature (e.g., Widom, Czaja, & Dutton, 2008), in that experiences of childhood physical and sexual abuse will be associated with adult interpersonal victimization. However, we expect that due to unique vulnerabilities of this sample (i.e., combined stress of managing HIV and sexual minority stress), overall rates of abuse will be higher compared with previously investigated samples of women and HIV-negative MSM.
Method
Participants and Procedures
A purposive (or targeted) sampling strategy (Watters & Biernacki, 1989) was used to recruit HIV-positive MSM (N = 171, see Table 1) from two urban, university-affiliated, public HIV/AIDS clinics. Eligible participants were active patients at one of the clinics, at least 18 years old, biologically male at birth, English-speaking, and self-identified as a sexual minority or MSM. After consenting to participate, men completed survey questionnaires via computer-assisted self-interview (CASI). The CASI method aims to maximize time efficiency, increase confidentiality, decrease socially desirable responding, and aid in subsequent data management and analysis (e.g., Metzger et al., 2000; Turner et al., 1998). Participants were paid $20 (U.S.) and given a list of HIV-related community resources. This study received continuous institutional review board (IRB) approval.
Percentage of Participants Reporting One or More Events of Childhood Abuse, Adult Abuse, and Partner Abuse.

The average age of the participants was 44.12 years (SD = 8.40, range = 25-66). Most participants identified as White (61%) and currently non-partnered (62%; see Table 1). Nearly half (47%) of the respondents reported a monthly income below the regional poverty level, and few reported being employed (15%). Almost a third (29%) of the men reported that they were living in someone else’s home or marginally housed. At least 60% were considered disabled by the state or federal government.
Measures
Demographics
We assessed participants’ age, race, and ethnicity; income, employment, and disability status; educational attainment; living situation; and relationship status (Table 1).
Childhood abuse
We used an abbreviated version of the Childhood Maltreatment Interview Schedule–Short Form (CMIS-SF; Briere, 1992) to assess childhood physical abuse (five items), CSA (sexual abuse by someone who was 5+ years older than the respondent and/or by someone of any age who used force or coercion; two items), and childhood psychological abuse (seven items). The CMIS-SR was chosen based on its use of commonly accepted definitions of childhood abuse constructs and wide use in the childhood abuse literature. To reduce participant burden, we used the abbreviated version. Cronbach’s alphas for the subscales in this sample were .82, r = .80, and .96, respectively.
Adult abuse
Participants were asked behaviorally specific questions about the frequency of experiences of physical, sexual, and psychological abuse since age 18. To assess physical abuse experienced as an adult, participants were asked to report how many times since their 18th birthday they were robbed or mugged; punched, kicked, hit, or beaten; and assaulted with a weapon using a measure adapted from prior research (Herek, Gillis, & Cogan, 1999; α = .76). One additional item from Herek and colleagues (1999) was used to assess serious psychological abuse: “Since your 18th birthday, have you ever been verbally threatened or attacked? /How many times were you verbally harassed or verbally attacked since your 18th birthday?” Respondents were also asked nine questions (α = .92) about adult sexual abuse victimization experiences since the age of 18 from the Sexual Experiences Survey (SES; Koss & Gidycz, 1985; Koss, Gidycz, & Wisniewski, 1987). The SES has been used extensively throughout the literature to assess for a range of sexual victimization experiences. As a way of facilitating recall of personal experiences without the use of stigmatized language such as “rape,” “abuse,” or “sexual assault,” the measure provides behaviorally specific examples of sexual aggression.
Partner abuse
We assessed partner physical, sexual, and psychological abuse in the past year with the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996), a behaviorally anchored measure with well-established psychometric properties. In these analyses, we used the physical abuse (11 items; α = .87), sexual coercion (7 items; α = .70), and psychological abuse (8 items; α = .83) subscales.
Analyses
Demographic, childhood abuse, and adult abuse factors were examined with frequencies and percentages. Bivariate analyses were conducted with either chi-square or Fisher’s exact tests. Each childhood abuse variable (i.e., physical, psychological, and sexual) was recoded into one of three groups using the following procedure. First, participants who reported zero instances of abuse were categorized as “no abuse.” Next, for participants who endorsed one or more instances of that specific type of abuse, a median split was used to categorize participants into either “low” or “high” abuse categories. As frequencies of reported abuse varied by type of abuse, the range within low and high abuse categories also varied for each abuse type. No gold standard exists for inferring severity of abuse from epidemiologic measures; frequency is the most commonly used, as we have here (e.g., Briere & Runtz, 1988; Casey & Nurius, 2005). It should be noted that the low abuse categories do not necessarily imply an inconsequential amount of abuse in this sample. For example, the low CSA group reported 1 to 20 instances of abuse and the high CSA group reported 21+ instances. Adult abuse factors remained continuous variables, with outlier responses truncated to 1,000 episodes. Responses to PA questions were summed within each subscale (higher scores indicating a greater frequency).
Associations between demographic and abuse outcomes were assessed using one-way ANOVA. A series of six negative binomial regression analyses were used to assess for associations between childhood abuse and adult abuse/PA, and adjusted for demographic factors (age, income, and race) shown to be marginally significant (p < .10) in the bivariate analyses. Negative binomial regression analyses were chosen for the multivariate analyses as adult abuse/PA outcomes were not normally distributed (i.e., when data have an unbounded positive range and the sample variance exceeds the sample mean). Because <10% of the data were missing, cases were excluded from models in the event of missing data.
Results
Overall Abuse by Type
The percentage of participants reporting childhood abuse, adult abuse, or PA is shown in Table 1. The lowest proportion of participants reported partner sexual abuse (18.7%), and the greatest proportion of participants reported childhood psychological abuse (93.5%).
Bivariate Associations Between Childhood Abuse and Adult Abuse/PA
Table 2 shows the proportion of participants who endorsed experiencing adult abuse or PA who also reported having experienced childhood abuse. Reporting any CSA experiences was associated with reporting adult physical, χ2(1, N = 171) = 16.29, p < .001; sexual, χ2(1, N = 171) = 12.06, p < .001; and psychological abuse, χ2(1, N = 164) = 15.29, p < .001.
Percentage of HIV-Positive MSM Reporting Childhood Abuse by Self-Reported Adult Abuse and Partner Abuse.

Note. MSM = men who have sex with men.
Column percentage.
Fisher exact test unless otherwise noted.
Chi-square test, in which χ2(1, N = 169) = 0.20.
p < .10. *p < .05. **p < .01. ***p < .001.
Bivariate analyses revealed that men who reported childhood physical abuse were more likely to report partner physical, χ2(1, N = 171) = 10.12, p < .01; sexual, χ2(1, N = 171) = 4.82, p < .05; and psychological abuse, χ2(1, N = 171) = 6.07, p < .05; compared with those without histories of childhood physical abuse (physical: 31% vs. 11%; sexual: 26% vs. 13%; psychological: 63% vs. 43%). Significant associations were not found between CSA or childhood psychological abuse and PA.
Multivariate Models of the Association Between Childhood Abuse and Adult Abuse
Childhood abuse experiences were entered into multiple negative binomial regression models to determine their associations with adult abuse (Table 3) and PA (Table 4). Each model was adjusted for demographic factors that were marginally significant (p < .10) in the bivariate analyses as follows: Adult physical abuse was adjusted for age; adult sexual abuse for age; partner physical abuse for income; partner physical abuse for race; partner psychological abuse for age and income (note: age, income, and race were not associated with adult psychological abuse).
Multiple Negative Binomial Regression of Childhood Abuse on Adult Physical, Sexual, and Psychological Abuse (Adjusted for Key Demographic Factors).
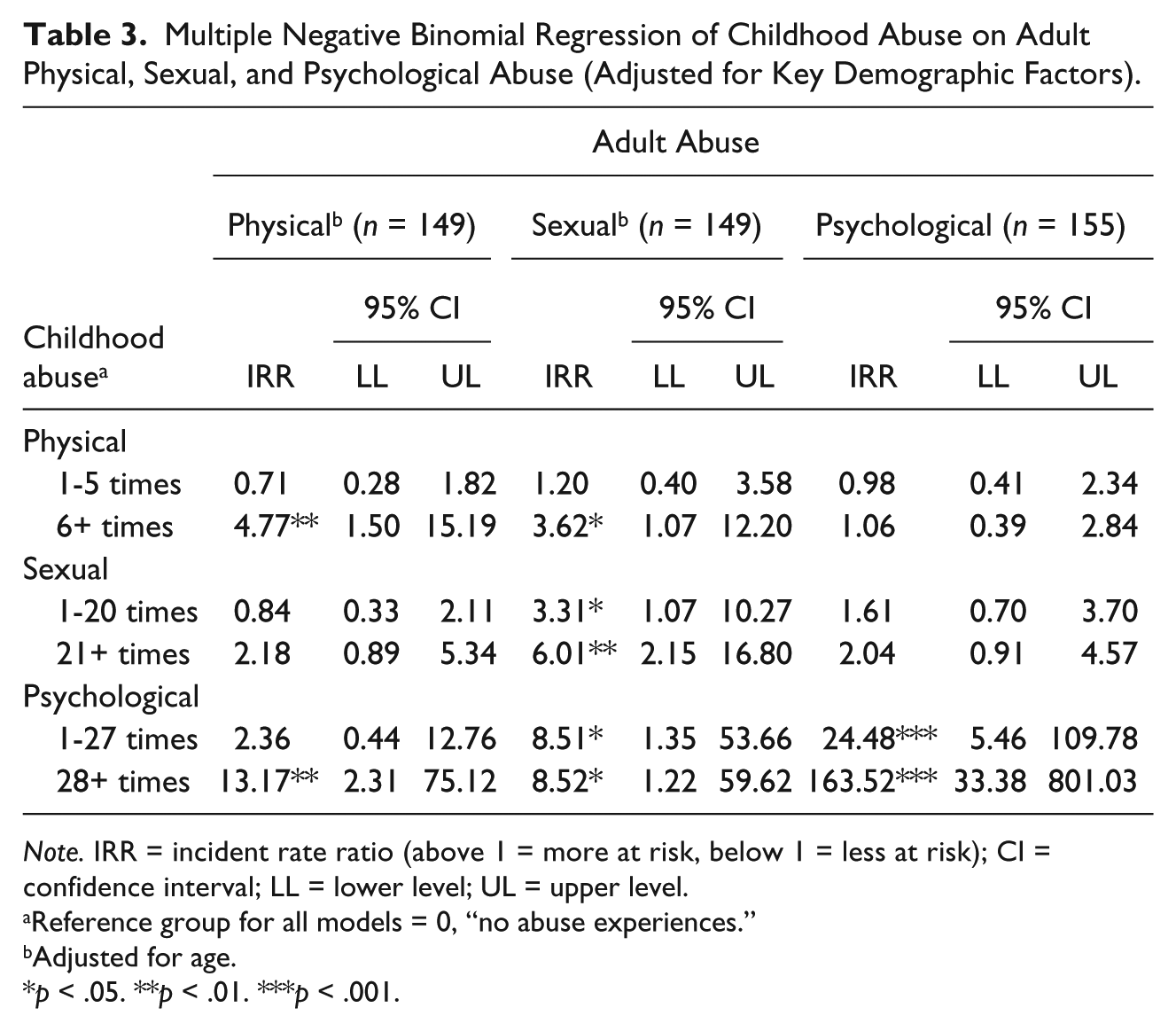
Note. IRR = incident rate ratio (above 1 = more at risk, below 1 = less at risk); CI = confidence interval; LL = lower level; UL = upper level.
Reference group for all models = 0, “no abuse experiences.”
Adjusted for age.
p < .05. **p < .01. ***p < .001.
Multiple Negative Binomial Regression of Childhood Abuse on Physical, Sexual, and Psychological Partner Abuse (Adjusted for Key Demographic Factors).

Note. IRR = incident rate ratio (above 1 = more at risk, below 1 = less at risk); CI = confidence interval; LL = lower level; UL = upper level.
Reference group for all models = 0, “no abuse experiences.”
Adjusted for income.
Adjusted for race.
Adjusted for age.
p < .05. **p < .01. ***p < .001.
Compared with men who reported no childhood physical abuse (0 = “no abuse”), those who reported six or more experiences of childhood physical abuse were at significantly greater risk of adult physical (incident rate ratio [IRR] = 4.77; 95% confidence interval [CI] = [1.50, 15.19]) and sexual (IRR = 3.62, 95% CI = [1.07, 12.20]) abuse. Participants who experienced CSA were at increased risk of adult sexual abuse, compared with those who did not report CSA (1-20 CSA: IRR = 3.31, 95% CI = [1.07, 10.27]; 21+ CSA: IRR = 6.01, 95% CI = [2.15, 16.80]). Men who reported childhood psychological abuse were at significantly increased risk of adult sexual abuse (1-27 Childhood Psychological: IRR = 8.51, 95% CI = [1.35, 53.66]; 28+ Childhood Psychological: IRR = 8.52, 95% CI = [1.22, 59.62]) and adult psychological abuse (1-27 Childhood Psychological: IRR = 24.48, 95% CI = [5.46, 109.78]; 28+ Childhood Psychological: IRR = 163.52, 95% CI = [33.38, 801.03]) compared with participants who did not report childhood psychological abuse. Men who reported 28 or more experiences of childhood psychological abuse were at increased risk of adult physical abuse (IRR = 13.17, 95% CI = [2.31, 75.12]).
With respect to PA as the outcome (see Table 4), childhood physical and sexual abuse was not associated with any of the PA outcomes. However, men who reported childhood psychological abuse at any level were at much increased risk of psychological abuse experiences as an adult (1-27 Childhood Psychological: IRR = 5.00, 95% CI = [1.05, 23.82]; 28+ Childhood Psychological: IRR = 7.93, 95% CI = [1.50, 42.03]).
Discussion
The present study is the only published report we could identify examining associations between multiple types of childhood abuse and adult revictimization (partner and non-partner) for HIV-positive MSM. In general, our findings are consistent with previously published work detailing high levels of abuse in both childhood and adulthood for MSM (e.g., Balsam et al., 2005; Greenwood et al., 2002); rates of abuse in our sample are comparable rates observed in nationally representative samples of women (Black et al., 2011). These findings are also in line with research suggesting that people living with HIV experience higher rates of abuse relative to HIV-negative MSM (Stall et al., 2003). Also, consistent with the extant literature on revictimization, our results suggest that a history of childhood abuse is associated with abuse experiences in adulthood. However, our more comprehensive investigation of abuse experiences suggests differential associations between various types of childhood abuse and abuse in adulthood and, thus, highlights the potential for different mechanisms.
Of the various forms of childhood abuse, CSA has been most studied by far in the revictimization literature for men of all sexual orientations (e.g., Kalichman et al., 2001). In our sample, CSA was associated with elevated risk for all types of adult (non-partner) revictimization, and CSA independently predicted adult sexual abuse with a dose–response association—such that the more frequent the CSA experiences the higher the likelihood of a participant also endorsing adult sexual abuse. These findings suggest that experiencing CSA confers a broad vulnerability to additional trauma exposure, as well as a specific vulnerability to sexually based abuse. Indeed, men who endorsed more frequent CSA were 4 times more likely to endorse adult sexual abuse. Given that, on average, these men were diagnosed with HIV as adults in their 20s and 30s, it is possible that their adult sexual victimization may have contributed to their HIV seroconversion.
Our results are consistent with studies suggesting that CSA exposure is important in understanding adult psychological and physical abuse, in addition to sexual revictimization (Kalichman et al., 2001). CSA’s influence on the risk of violence in adulthood may work through changes in psychological functioning. For example, CSA has been associated with depression and PTSD symptoms, sexual risk behaviors, and substance use (Reed, Anthony, & Breslau, 2007). Individuals who struggle with these and other mental health problems may exhibit impaired risk perception, fewer emotional regulation skills, or fewer protective behavioral strategies (e.g., Messman-Moore, Brown, & Koelsch, 2005; Messman-Moore, Walsh, & DiLillo, 2010). Recent research has also found that avoidant coping and trauma symptoms mediate the associations between CSA and revictimization (Fortier et al., 2009). In a prospective study of female college students (Messman-Moore, Ward, & Brown, 2009), substance use, which may function as an avoidant coping strategy, mediated the relation between CSA and adult sexual revictimization. It is likely that CSA increases the general risk of revictimization through increasing PTSD, depression, and substance use. However, these previous models have not investigated CSA and adult (partner and non-partner) physical or psychological abuse.
At the bivariate level, respondents who endorsed childhood physical abuse were more likely to endorse recent PA of all forms with trends for non-partner physical abuse; however, in the multivariate models, it flipped. The PA findings do not hold, and instead, more frequent childhood physical abuse was associated with adult physical and sexual abuse. Here, too, we see a broad vulnerability rather than a more circumscribed effect. In general, we expect that overt modeling plays a role here and, although we did not measure childhood exposure to PA, we know that it is often concomitant with physical abuse of children (e.g., Brill, Fiorentino, & Grant, 2001). One possible mechanism for revictimization is the development of a negative attributional style following childhood experiences of violence, whereby subsequent experiences of violence confirm expectations about the world and the behavior of others and are, therefore, unavoidable (Elwood, Hahn, Olatunji, & Williams, 2009). It is possible that children exposed to abuse have internalized norms about violence as a problem solving strategy, or that violence in adulthood seems familiar—normal, even—because of those early experiences. The normalization of violence is another potential mechanism for revictimization that may be operating here. Given the relatively low incomes of many of the participants, these men may have lived in neighborhoods with high rates of endemic violence, and these men’s physical and social context may be a driver of lifetime abuse exposure (Stein, Jaycox, Kataoka, Rhodes, & Vestal, 2003).
Surprisingly, nearly 94% of the sample screened positive for childhood psychological abuse using a commonly used measure of childhood abuse (Briere, 1992). This exceptionally high proportion may be the result of participants being targeted for abuse based on their perceived sexual orientation (Balsam et al., 2005), or some unmeasured reason. Participants who endorsed childhood psychological abuse were more likely to endorse psychological abuse from adult partners and non-partners and, in multivariate models, frequent childhood psychological abuse was associated with all forms of adult abuse. Notably, the IRRs display a dose–response relationship in terms of the frequency of reported childhood psychological abuse and likelihood of endorsing psychological abuse in adulthood. One concern we have is that (in the interest of reducing participant burden) our measure of adult psychological abuse consisted only of one item and, thus, may be too low a bar. However, the wording of that item, which asks whether a participant has been “verbally threatened or attacked,” does connote more serious abuse than an item which asks, for example, if a person had been “yelled/shouted at.” Psychological abuse is sometimes overlooked in research on victimization in favor of contact abuse (i.e., physical and sexual; Follingstad, 2009). Given the pattern of findings in this population, it seems as if increased attention to this construct is warranted, at least among HIV-positive MSM.
As with any individual study, there are limitations that hamper our ability to generalize our findings. First, these data are cross-sectional, so we cannot infer causal relations between the early and later abuse experiences. In addition, given the retrospective self-report data and cross-sectional design, it was not feasible to investigate possible mediators (PTSD, substance abuse, internalized heterosexism) that may have contributed to our findings. We would need to have measured these or other mental health variables in the time between the initial and subsequent victimizations. We also did not determine which victimization experiences were specifically targeted toward these men because of their sexual orientation. Finally, here, we report on the experiences of HIV-positive MSM who were relatively engaged with the health care system. It is possible that different patterns of findings might emerge for heterosexually identified individuals with HIV, or even for HIV-positive MSM who are not receiving medical care (Cunningham et al., 2006).
Conclusion
Results from the study presented here indicate that HIV-positive MSM who have experienced childhood abuse are at increased likelihood of revictimization in adulthood. Future work in this area should investigate the common pathways related to revictimization, as well as the unique mechanisms that may be operating for this extremely vulnerable population. Furthermore, investigation of the potential mental health and HIV-health correlates of revictimization among HIV-positive MSM is warranted. Developers of HIV-related interventions should assess abuse histories and address the sequelae of proximal and distal abuse as part of comprehensive intervention packages that aim to increase the physical and psychological health of these men, as well as to improve their quality of life.
Footnotes
Acknowledgements
The authors wish to express gratitude to the project’s staff at the University of Washington, as well as the staff and patients of the cooperating clinics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a National Institute of Mental Health award (F31 MH71179) and a small grant from the Robert C. Bolles Research Fund of the University of Washington, both awarded to the first author under the mentorship of Dr. Jane Simoni. T. A. Hart is funded by a Career Scientist Award from the Ontario HIV Treatment Network.