
Abstract
The objective of this study was to determine the relationship between a history of dyslexia and childhood physical abuse in a large population-based epidemiological sample. It was hypothesized that the prevalence of dyslexia would be significantly higher in individuals who reported a childhood history of physical abuse in comparison to those who did not report such a history. A secondary analysis examined data from respondents 18 years and older from the Saskatchewan and Manitoba sample of the 2005 Canadian Community Health Survey (CCHS). There were 13,640 respondents ages 18 and older. Due to missing data, the final sample size was 13,054 respondents. One third (34.8%) of respondents who reported they had been physically abused during their childhood or adolescence also reported being diagnosed with dyslexia in comparison with 7.2% of those who did not report being physically abused (p < .001). Initial adjustments for sociodemographic variables produced an odds ratio (OR) for dyslexia that was more than 7 times higher (OR = 7.09; 95% confidence interval [CI] = [4.42, 11.35]) for those who had reported being physically abused in comparison with their peers who did not report such a history; with additional adjustments for other adverse childhood experiences, these odds decreased only slightly to 6.09 times higher (95% CI = [3.58, 10.35]). Further research is needed to understand the mechanism linking physical abuse and dyslexia.
Keywords
Introduction
Despite the purported association between dyslexia and psychosocial difficulties (Sundheim & Voeller, 2004), there have been few large-scale epidemiological studies linking dyslexia to a history of childhood physical abuse in the adult population. This is an intriguing question given the relatively high prevalence of reading problems or dyslexia during childhood (Leach, Scarborough, & Rescorla, 2003; Shaywitz, 2004), and the finding that children with various disabilities are 3 to 4 times more likely to be physically abused than nondisabled peers (Sullivan & Knutson, 2000). Conversely, individuals who have been maltreated, especially those with manifest posttraumatic stress disorder (PTSD), reportedly have lower academic skills (De Bellis, Hooper, Spratt, & Woolley, 2009; Kinard, 1999, 2001; Kurtz, Gaudin, Wodarski, & Howling, 1993; Leiter & Johnsen, 1994, 1997; Perez & Widom, 1994; Shonk & Cicchetti, 2001; Slade & Wissow, 2007) including dyslexia, even when controlling for such variables as age, sex, race, and social class (Perez & Widom, 1994). Furthermore, there appears to be significant neurological vulnerability for individuals who have been maltreated, abused, or traumatized as children, especially with respect to brain structure and associated functions (De Bellis & Thomas, 2003; Teicher et al., 2003). Specifically, maltreatment in children has been shown to produce abnormal neurodevelopment and associated dysfunction in key areas related to learning including the prefrontal cortex (Richert, Carrion, Karchemskiy, & Reiss, 2006), hippocampus (De Bellis, Hall, Boring, Frustaci, & Moritz, 2001), and corpus callosum (Villarreal et al., 2004), potentially leading to inattention, executive dysfunction, impaired memory, and slower information processing. These neurobiological factors may influence the development of reading and associated academic skills (e.g., spelling, written language).
This study was designed to examine the relationship between a reported diagnosis of dyslexia and childhood physical abuse in a large population-based epidemiological sample of adults. Based on the available literature examining the connection between maltreatment and academic performance (e.g., Leach et al., 2003; Shaywitz, 2004; Sullivan & Knutson, 2000), it is hypothesized that a significantly higher rate of dyslexia will be reported in individuals who have a reported history of physical abuse versus those who do not have such a history. If present, this relationship would provide additional support for the existence of a significant association between physical abuse and dyslexia and, more specifically, provide information on the magnitude of that association in a representative community-based sample.
Method
Data Source and Sample
A secondary analysis examined data from respondents 18 years and above from the Saskatchewan and Manitoba sample of the 2005 Canadian Community Health Survey (CCHS). The CCHS is a nationally representative cross-sectional survey on the health and health behaviors of Canadians (Statistics Canada, 2007) conducted by Statistics Canada, the Canadian equivalent of the U.S. Census Bureau. Information was gathered through interviews. The combined response rate for Manitoba and Saskatchewan was 84% (Statistics Canada, 2007). Of the 13,640 respondents in Saskatchewan and Manitoba who were aged 18 and above, 9 respondents were missing information on both the physical abuse question and the dyslexia question, 538 were missing information only on the physical abuse question, and 39 were missing information only on the dyslexia question. Thus, the final unweighted sample size for the cross-tabs was 13,054. There were 1,020 respondents reporting abuse and 77 respondents reporting dyslexia. In the logistic regression analyses, 304 additional respondents had missing information on one or more of the control variables and were thus excluded, resulting in a sample size for the logistic regressions of 12,750 respondents. Those who reported they had been diagnosed with dyslexia had a mean age of 35.0 (SD = 11.8), which was significantly younger than those who reported they had not been diagnosed (Mage = 46.1; SD = 17.9; t = 8.55; p < .001). Both groups had an approximately equal percentage of women (dyslexia group: 47.0% female; without dyslexia: 51.7% female; χ2 = 0.73, p = .39).
Measures
Dyslexia was assessed in a long list of chronic conditions. The preamble to the section on chronic conditions began,
Now I’d like to ask about certain chronic health conditions which you may have. We are interested in “long-term conditions” which are expected to last or have already lasted 6 months or more and that have been diagnosed by a health professional.
Dyslexia was listed as one of the possible responses.
Childhood physical abuse was assessed in a section of the CCHS that asked questions about adverse childhood experiences. The following instructions prefaced this section: “The next questions ask about some things that may have happened to you while you were a child or teenager, before you moved out of the house. Please tell me if any of these things have happened to you.” Individuals who responded “yes” to the question, “Were you ever physically abused by someone close to you?” were identified as having a history of childhood physical abuse.
Other childhood stressors were assessed in the childhood adversity section including: (a) parental divorce: “Did your parents get a divorce?”; (b) parental unemployment: “Did your father or mother not have a job for a long time when they wanted to be working?”; and (c) parental addictions: “Did either of your parents drink or use drugs so often that it caused problems for the family?”
Demographic control variables investigated included age in years, sex, and race (self-reported White vs. non-White).
Data Analysis
A chi-square test of dyslexia by childhood physical abuse was conducted, as were two logistical regression analyses using dyslexia as the dependent variable. In our first model, age, sex, and race were adjusted for. In the subsequent model, childhood stressors including childhood parental divorce, childhood parental addictions, and childhood parental unemployment were adjusted for in addition to age, sex, and race. Due to missing data for the control variables, the sample sizes varied from 13,054 in the chi-square analysis to 12,750 in the fully adjusted model. All percents and odds ratios (ORs) were generated using a weighting variable to adjust for the probability of selection and non-response.
Results
Respondents who reported they had been physically abused during their childhood or adolescence were more likely to report they had been diagnosed by a health care professional with dyslexia. Only 7.2% of those without reported abuse indicated dyslexia in sharp contrast to 34.8% of those who reported physical abuse during their childhood (χ2 = 93.7; p < .001).
As can be seen in Table 1, the initial adjustments for age, sex, and race produced an OR for dyslexia that was more than 7 times higher (OR = 7.09; 95% confidence interval [CI] = [4.42, 11.35]) for those who reported they had been physically abused in comparison with their non-abused peers. When additional adjustments were made for other adverse childhood experiences, including parental divorce, parental addictions, and long-term parental unemployment, the odds of dyslexia for those who had been physically abused decreased only slightly to sixfold that of non-abused respondents (OR = 6.09; 95% CI = [3.58, 10.35]). For each additional year of age, the odds of dyslexia decreased by 4% (OR = 0.96, 95% CI = [0.94, 0.97]). None of the other control variables (i.e., gender, race, parental divorce, parental addiction, parental long-term unemployment) was significantly associated with dyslexia.
Logistic Regression of Childhood Physical Abuse and Other Adverse Childhood Experiences and Demographic Factors Associated With Self-Report of a Health Professional’s Diagnosis of Dyslexia.
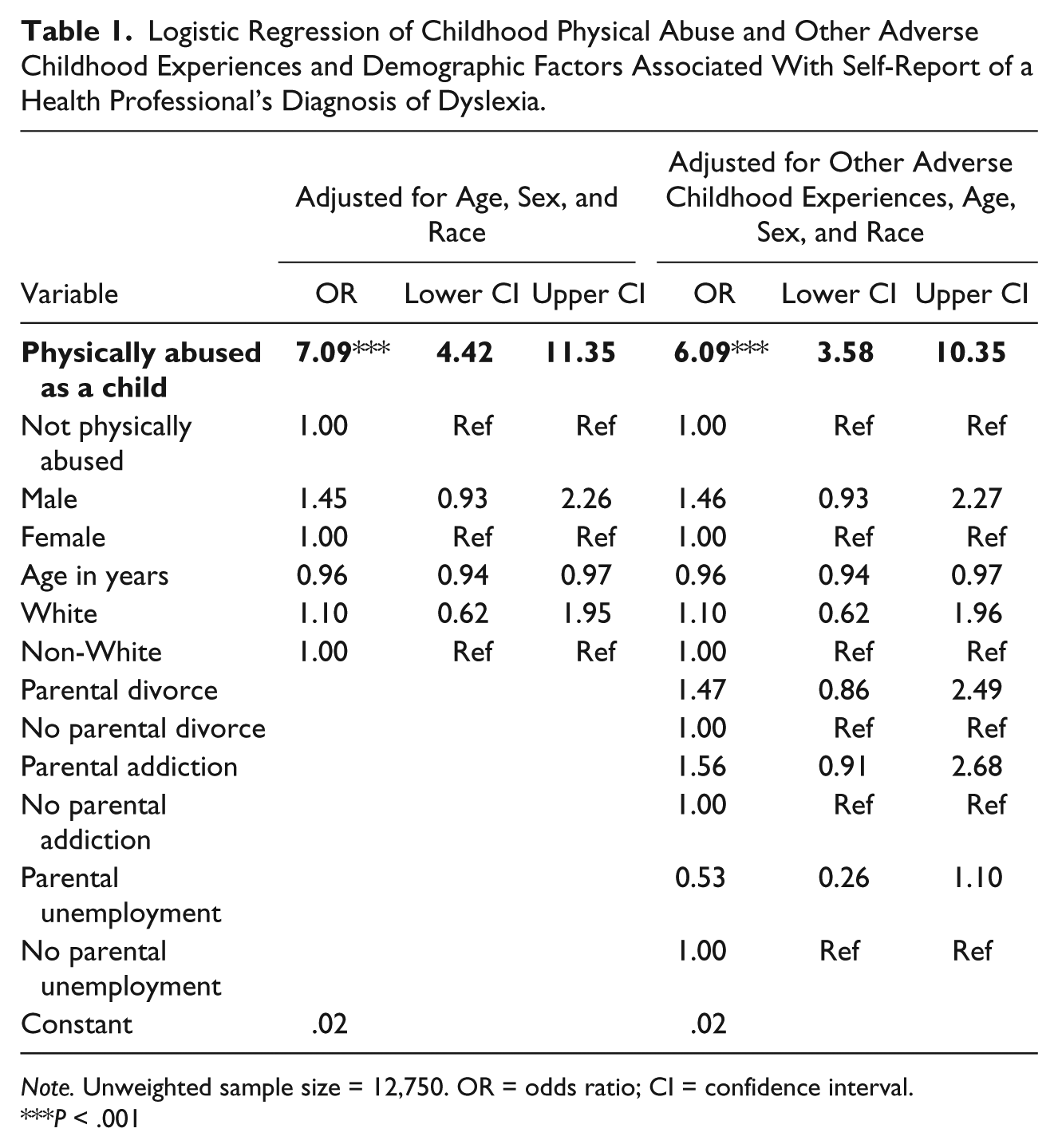
Note. Unweighted sample size = 12,750. OR = odds ratio; CI = confidence interval.
P < .001
Discussion
This study examined the relationship between reports of childhood physical abuse and the presence of dyslexia in a large epidemiological sample. Findings revealed sevenfold age–race–sex adjusted odds of dyslexia among adults reporting they had been physically abused during their childhood in comparison with their non-abused peers. These extremely high odds were not substantially attenuated by adjustment for several other adverse childhood experiences, age, race, or sex. These results raise significant questions with respect to the relationship between the brain changes that have been associated with physical abuse, and other types of events that contribute to brain impairment (e.g., substance abuse; Severtson, Hedden, Martins, & Latimer, 2012), and the appearance of learning problems, particularly dyslexia. For some children, the presence of dyslexia and related learning problems may place them at relatively higher risk for physical abuse, perhaps secondary to adult frustrations with chronic learning failure, child frustrations, and increased antagonistic behaviors with caregivers, associated attention-deficit hyperactivity disorder (ADHD) and related social-emotional difficulties, poor parent coping mechanisms, or increased neurological vulnerability (Gilger & Kaplan, 2008). Conversely, dyslexia is a neurodevelopmental disorder, with the core phonological processing deficits being present from early preschool (Mann & Foy, 2003). Given the known association between brain dysfunction and maltreatment (e.g., De Bellis & Thomas, 2003), it is speculated that the experience of physical abuse may also contribute to and/or exacerbate such learning problems, secondary to increased neurologic burden. At this juncture, the current findings do not point toward an etiological direction for this relationship but, from a public policy perspective, the findings do suggest that children and adults with a history of dyslexia should be screened for abuse, and those with a history of abuse should be screened for dyslexia or associated learning problems.
The large, population-based sample is a major strength of this study. The large sample size has allowed for detailed examination of the co-occurrence of two conditions (childhood physical abuse and dyslexia) and provided representative information of this association; however, there are several limitations of this study. First, for both dyslexia and physical abuse only self-report was available. The self-report of a medical diagnosis of dyslexia likely is an underrepresentation of the larger population of individuals with dyslexia, particularly as children are more likely to be diagnosed by an educational specialist rather than a health professional. The self-reported dyslexia rate of less than 1% was significantly below the 10% to 17% rates reported in either the child (Shaywitz, 2004) or adult (Katz, Goldstein, & Beers, 2001) literature, but probably represented individuals on the more severe end of the continuum. Although it is impossible to determine exactly how underreporting of dyslexia affected the association we found, it is likely it would bias the findings toward the null. Future research would benefit from verification of the dyslexia diagnosis through testing rather than through self-report of a medical diagnosis and an expansion to include other forms of reading disorder as well.
Second, childhood physical abuse was based on retrospective self-reports. Other research has indicated that retrospective reports of childhood abuse are vulnerable to underreporting (Berger, Knutson, Mehn, & Perkins, 1988; Fergusson, Horwood, & Woodward, 2000). Misclassifications in this direction would tend to bias results toward the null. An additional limitation is that the question on childhood abuse asked whether individuals, before the age of 18, had been “physically abused by someone close to” them. It is possible that some respondents categorized as “abused” may have been reporting dating violence they experienced at age 16 or 17. Consequently, the results need to be interpreted with caution and further replication is needed using other population-based studies which incorporate medical examination and access to child welfare records. Our confidence in our findings is stronger due to the similarity of our conclusions to those reported in a review of Omaha student files: That study concluded that there is a strong link between substantiated childhood maltreatment (which includes physical and sexual abuse and neglect) and learning and communication disabilities which had been verified by a multidisciplinary evaluation team (Sullivan & Knutson, 2000). Although a number of critical factors were controlled in our model, it was not possible to control for the presence of other problems, such as math disabilities, other psychiatric disorders, or pharmacological use, nor the chronicity, type, and severity of physical abuse including when the abuse occurred and who was the perpetrator, nor was information available on whether other types of childhood abuse occurred or whether the respondent had an impoverished childhood. These variables could have had an impact on our findings and will require further study.
In summary, findings from the current large-scale study document a six- to sevenfold higher odds of dyslexia among individuals who had been physically abused as a child or adolescent. Approximately one third of those who reported childhood physical abuse had dyslexia. Although the direction of this relationship will require ongoing examination using longitudinal data, the findings suggest that routine screening for physical abuse may be appropriate for children with dyslexia. This will be especially important for primary care providers and school-based practitioners, as they typically will be the first professionals to encounter dyslexia for any particular child. Future studies should focus on the developmental timing and chronicity of the physical abuse, and what specific underlying neurological mechanisms may be contributing to this relationship.
Footnotes
Acknowledgements
The authors would like to thank Rukshan Mehta, MSW; Katie Hunter, MSW; and Marla Battiston, MSW for assistance with manuscript preparation. We are grateful to Statistics Canada and the Social Sciences and Humanities Council of Canada for permission to access the 2005 Canadian Community Health Survey via the Research Data Center (RDC) at the University of Toronto and to the staff at the Toronto RDC for their help in accessing the data.
Authors’ Note
Both authors were involved in the conception and design of the study and drafting and critical revision of the manuscript. Esme Fuller-Thomson acquired the data and conducted the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author (Esme Fuller-Thomson) would like to gratefully acknowledge support received from the Sandra Rotman Endowed Chair in Social Work. The second author (Stephen R. Hooper) would like to gratefully acknowledge support received from the Maternal Child Health Bureau (T73MC00030).