
Abstract
There has been an abundance of research in recent years on mindfulness, including mindfulness within individuals seeking substance use treatment. However, to date, there has been no research on whether trait mindfulness is associated with increased aggression among individuals seeking substance use treatment. Past research has demonstrated that individuals in substance use treatment evidence higher levels of aggression than non-substance abusers, and preliminary research has shown that trait mindfulness is inversely associated with aggression in non-substance-use treatment-seeking populations. The current study examined whether trait mindfulness was associated with aggression among men seeking residential substance use treatment (N = 116). Results demonstrated that lower trait mindfulness was associated with increased aggression (physical, verbal, and aggressive attitude). Moreover, this relation held for both verbal aggression and aggressive attitude after controlling for alcohol use, drug use, and age, all known predictors of aggression. Findings provide the first evidence that mindfulness is negatively associated with aggression among men in substance use treatment, which could have important implications for intervention. That is, mindfulness-based interventions may prove helpful for the treatment of both substance use and aggression.
Substance use disorders are associated with a wealth of negative health and societal outcomes, including aggressive behavior. Research has demonstrated that men who seek substance abuse treatment evidence higher levels of aggressive behavior (i.e., physical, verbal, sexual) than the general population (Stuart, O’Farrell, & Temple, 2009), including aggression against intimate partners (e.g., Mattson, O’Farrell, Lofgreen, Cunningham, & Murphy, 2012) and general aggression (i.e., aggression against friends, strangers; Stuart, Moore, Ramsey, & Kahler, 2004). Moreover, alcohol and drug use are robust correlates of aggression (Hoaken & Stewart, 2003), with aggression more likely to occur on substance use days relative to non-substance use days (Moore, Elkins, McNulty, Kivisto, & Handsel, 2011; Mulvey et al., 2006; Stuart et al., 2013). Thus, it is not surprising that research has demonstrated that aggression decreases following substance use treatment (O’Farrell, Murphy, Stephan, Fals-Stewart, & Murphy, 2004; Stuart et al., 2009). However, there remains a significant prevalence of aggression following substance use treatment, with aggression being more prevalent among individuals who relapse to substance use relative to those who remain remitted (e.g., Schumm, O’Farrell, Murphy, & Fals-Stewart, 2009). Therefore, there is a need for continued research into aggression among individuals who seek substance use treatment, specifically research on risk and protective factors for aggression that may be amenable to change, as aggression often persists even with reductions in substance use. Thus, in the current study, we examined trait mindfulness as a predictor of aggressive behavior among men seeking residential substance use treatment, as previous research has demonstrated mindfulness to be a protective factor for substance use and relapse to substance use (e.g., Bowen et al., 2009), and preliminary research has shown lower levels of aggression among non-substance abusers who are higher in trait mindfulness (e.g., Heppner et al., 2008).
Mindfulness
One of the most common definitions of mindfulness is “paying attention in a particular way: on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 1994, p. 4). That is, mindfulness is a “way of being” (Kabat-Zinn, 2003), not a state-like quality or a set of techniques to be learned. The qualities of mindfulness allow individuals to be more open to experience feelings, thoughts, and behaviors with an open awareness, non-judgmentally, and non-defensively (Heppner et al., 2008). Because mindfulness is present-moment based, it can help individuals to decrease rumination and worry, as all experiences are allowed to naturally come and go without any effort to remove unpleasant emotions/thoughts or engage in reactive behavior (Segal, Williams, & Teasdale, 2002). As mindfulness is a way of being, it is assumed that the qualities of mindfulness (e.g., non-judgment, acceptance, curiosity of experience) can be enhanced with appropriate training (e.g., mindfulness meditation) and practice, which has been supported by a number of studies (Baer, 2003). That is, unlike a skill to be learned (e.g., deep breathing) that can be used during times of stress, usually to reduce stress or change an experience, mindfulness training leads to natural changes in the way events and experiences are held in awareness, namely, with acceptance and non-judgment, and thus transforms the way individuals may perceive stress, for example, as a fleeting experience that does not need to be changed.
In the current study, we examined mindfulness as a trait. Trait mindfulness is considered a naturally occurring, dispositional characteristic, and can be assessed by asking individuals to report on their tendencies to have sustained awareness and attention to what occurs in the present moment of their everyday life (Bowen & Enkema, 2014; Brown & Ryan, 2003). In essence, high trait mindfulness would be consistent with the “way of being” that is sought through mindfulness meditation practice. It should be noted that, empirically, measuring trait mindfulness has proven difficult, which is likely due to various definitions in the literature, a disagreement about whether mindfulness is a unidimensional or multidimensional construct (e.g., Brown & Ryan, 2003), and whether self-report measures accurately capture the construct of trait mindfulness. However, research has consistently shown that trait mindfulness increases with mindfulness meditation training (e.g., Bowen et al., 2009) and is associated with positive mental health (e.g., Brown & Ryan, 2003) and researchers have continued to advocate for the investigation of trait mindfulness as a way to advance the field of mindfulness (e.g., Bowen & Enkema, 2014).
The existing literature has demonstrated the positive effects of higher levels of trait mindfulness, as well as the beneficial effects of mindfulness-based interventions. For instance, higher levels of trait mindfulness have been associated with fewer mental health symptoms (e.g., depression; Brown & Ryan, 2003), improved quality of life (Van Dam, Sheppard, Forsyth, & Earleywine, 2011), lower impulsivity (Peters, Erisman, Upton, Baer, & Roemer, 2011), and better emotion regulations skills (Goodall, Trejnowska, & Darling, 2012). In addition, mindfulness-based interventions, which generally include weekly classes in mindfulness meditation for a specified period of time (e.g., 8 weeks), have demonstrated robust positive effects across mental health disorders and physical health complaints (for reviews, see Eberth & Sedlmeier, 2012; Keng, Smoski, & Robins, 2011).
More recently, research has begun to examine mindfulness among individuals seeking substance use treatment. It is believed that mindfulness meditation training may affect neurobiological mechanisms associated with negative affect and craving, thus reducing the risk of relapse (Witkiewitz, Lustyk, & Bowen, 2012). Research has demonstrated that trait mindfulness is lower among substance abuse treatment seekers relative to the general population (Dakwar, Mariani, & Levin, 2011; Shorey, Brasfield, Anderson, & Stuart, 2014). Bowen and Enkema (2014) demonstrated that trait mindfulness was inversely associated with substance use dependence severity among men and women seeking outpatient substance use treatment. In addition, Mindfulness-Based Relapse Prevention (MBRP; Bowen et al., 2009), an 8-week outpatient group therapy for substance use, has been shown to reduce cravings and relapse to substance use to a greater degree than a 12-step, process-oriented outpatient program 4-months post-treatment. Thus, initial evidence suggests that mindfulness training may be a helpful component of substance use treatment by decreasing risk of relapse.
Mindfulness and Aggression
To date, only a handful of studies have examined the relation between trait mindfulness and aggression, all of which, to our knowledge, have utilized non-clinical undergraduate student samples. 1 Heppner and colleagues (2008) demonstrated that a higher level of trait mindfulness was negatively associated with verbal aggression perpetration among male and female college students, although no such association was found for physical aggression. Borders, Earleywine, and Jajodia (2010) found that trait mindfulness was negatively associated with both verbal and physical aggression perpetration among college students. In addition, Gallagher, Hudepohl, and Parrott (2010) demonstrated that increased trait mindfulness was negatively associated with sexual aggression perpetration against a dating partner in a sample of male college students. It should be noted that all of the above studies assessed mindfulness as a unidimensional construct, utilizing the same self-report measure of trait mindfulness that was used in the current study (the Mindful Attention Awareness Scale [MAAS]; Brown & Ryan, 2003).
In a more recent study, Shorey, Seavey, Quinn, and Cornelius (2014) demonstrated trait mindfulness to be associated with psychological and physical aggression against intimate partners among female undergraduate students. Specifically, findings demonstrated that the mindfulness facets of non-reactivity (the ability to view and process emotional stimuli without automatically reacting) and act with awareness (the ability to make deliberate and conscious decisions, as opposed to automaticity of behavior) were negatively associated with psychological and physical aggression, and that these relationships were mediated by anger management skills.
Although the existing research literature on aggression and mindfulness is scant, researchers have speculated that mindfulness-based interventions may be an effective alternative or complementary treatment for aggressive behavior (Fix & Fix, 2013; Shorey et al., 2012). Specifically, mindfulness-based interventions are believed to reduce impulsive behavior, to increase adaptive emotion regulation, and, thus, to reduce negative affect (Baer, 2003), all known correlates of aggression. Still, there is a continued need for basic research into the relation between trait mindfulness and aggression, particularly among clinical populations, to determine whether there is a sufficient link between trait mindfulness and aggression to warrant the investigation of mindfulness-based interventions as a treatment for aggressive behavior. Because aggression is highly prevalent among substance abuse treatment seekers (e.g., Stuart et al., 2009), trait mindfulness is lower among substance abuse treatment seekers relative to other populations (e.g., Shorey et al., 2014), and mindfulness-based interventions have proven effective for reducing relapse to substance use among individuals seeking substance abuse treatment (e.g., Bowen et al., 2009), individuals seeking substance use treatment represent an important population in which to examine the relation between trait mindfulness and aggression.
The Current Study
The purpose of this study was to examine the relation between trait mindfulness and aggression among adult men seeking residential substance use treatment. Specifically, we examined whether trait mindfulness was associated with different types of aggression (verbal, physical, and attitudinal) and also whether trait mindfulness remained associated with aggression after controlling for alcohol use, drug use, and age, all known correlates of aggression among men seeking substance use treatment (e.g., Stuart et al., 2008). On the basis of previous research and theoretical understandings of mindfulness, we hypothesized that (a) lower trait mindfulness would be associated with increased aggression and (b) trait mindfulness would remain associated with aggression even after controlling for alcohol use, drug use, and age.
Method
Procedures and Participants
The treatment records from adult male residential substance use treatment seeking patients in a private residential substance abuse treatment facility located in the Southeastern United States were reviewed for the present study. Patients are informed that their treatment records may be de-identified and utilized for research as part of their treatment informed consent. The treatment facility provides a 28 to 30 day program, largely guided by the traditional 12-step model. All patients must have a primary substance use disorder and be approximately 25 years of age or older to be admitted to the facility. On admission, and after medical detoxification (if necessary), patients complete an extensive intake assessment, including interviews and self-report measures (discussed below). All substance use disorder diagnoses, which are based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000), are diagnosed through the consultation of treatment team members, which includes a licensed psychologist, a psychiatrist, a general physician, and substance abuse counselors. Study procedures were approved by the Institutional Review Board of the first author.
Patient records were examined from January 2013 to May 2013 in the current study, which represents all adult male patients admitted to the inpatient treatment facility during this time. This resulted in a sample of 116 male patients. The primary substance use diagnoses for this sample were alcohol dependence (54.3%), opioid dependence (17.2%), and polysubstance dependence (5.2%). The remaining patients had a mix of primary substance use diagnoses (e.g., cocaine dependence, amphetamine dependence). Racially, the majority of patients were non-Hispanic Caucasian (90.5%). The remaining self-reported racial groups were African American (4.3%), Hispanic (2.6%), and “other” (e.g., Indian descent; 2.6%). The mean age of patients was 41.55 (SD = 11.02). Prior to entering treatment, 21.6% of patients were employed full-time and 27.6% took medical leave from their employment to obtain treatment. The mean number of years of education completed by patients was 13.70 (SD = 2.03).
Measures
Trait mindfulness
The 14-item version of the MAAS was used (Brown, West, Loverich, & Biegel, 2011). The 14-item version does not contain the item “I drive places on ‘automatic pilot’ and then wonder why I went there,” which is included in the 15-item version of the MAAS (i.e., Brown & Ryan, 2003). The treatment facility where charts were reviewed for the current study did not include this item because patients cannot drive during their residential stay in treatment and the treatment facility wanted the option to eventually examine pre–post treatment changes in trait mindfulness. The MAAS is designed to capture a receptive state of mind, in which awareness of what is taking place in the present moment is simply observed, without appraising or evaluating experience. The 14-item version of the MAAS has demonstrated good reliability (Cronbach’s α = .88) and validity (Brown et al., 2011). A mean score was obtained by summing all items on a 6-point Likert-type scale (1 = almost always; 6 = almost never) and dividing by the total number of items. Higher scores on the MAAS indicate higher levels of trait mindfulness.
Aggression
The Aggression subscales from the Personality Assessment Inventory (PAI; Morey, 1991) were used to measure aggression. The PAI consists of four Aggression subscales: Physical (prone to physical displays of anger, such as physical fights and damage to property), Verbal (tendency to be verbally aggressive [e.g., insulting, verbally threatening] with little or no provocation), Attitude (easily angered, low anger control, and perceived by others to be hostile), and an Overall Aggression Composite Score (the combination of the Physical, Verbal, and Attitude subscales). Morey (1991) reports that average scores on the PAI aggression scales are T-scores of 59 or below, with scores from 60 to 69 indicative of impatience, irritability, and quick-tempered; 65 to 69 are individuals who are easily provoked; and 70 or higher are chronically angry and hostile, with great potential for aggression. The PAI Aggression subscales have demonstrated good internal consistency, convergent validity with other commonly used measures of aggression and hostility, and discriminant validity (Crawford, Calhoun, Braxton, & Beckham, 2007; Morey, 1991).
Alcohol use
Alcohol use in the year prior to treatment was assessed with the Alcohol Use Disorders Identification Test (AUDIT; Saunders, Asaland, Babor, de la Fuente, & Grant, 1993). The AUDIT, which contains 10 items, examines the intensity and frequency of alcohol use, symptoms that might indicate dependence or tolerance to alcohol, and negative consequences associated with alcohol use. The AUDIT has shown good reliability and validity across multiple populations (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001).
Drug use
The Drug Use Disorders Identification Test (DUDIT; Stuart, Moore, Kahler, & Ramsey, 2003; Stuart et al., 2004) is a 14-item self-report measure that is modeled after the AUDIT. That is, the DUDIT assesses the frequency of drug use and symptoms that may indicate tolerance or dependence. The DUDIT examines seven different types of drugs (cannabis, cocaine, hallucinogens, stimulants, sedatives/hypnotics/anxiolytics, opiates, and other substances [e.g., steroids, inhalants]). The DUDIT has demonstrated good reliability (α = .90) and validity across multiple samples (Stuart et al., 2004; Stuart et al., 2008).
Data Analytic Strategy
All statistical analyses were conducted using SPSS version 20.0. Variables were first examined for skewness and kurtosis, with results demonstrating that all variables fell within normal limits (e.g., skewness less than 2.0). Bivariate correlations were conducted to examine basic relationships among study variables. Next, to examine whether trait mindfulness remained associated with aggression after controlling for alcohol use, drug use, and age, we utilized stepwise regression analyses. In the first step, alcohol use, drug use, and age were entered as predictors of aggression. In the second step, trait mindfulness was added as a predictor. This allowed us to determine the extent to which trait mindfulness added unique variance to the prediction of aggression by examining the change in R2 from the first to the second model (Cohen, Cohen, West, & Aiken, 2003). Analyses were conducted separately for each of the four Aggression subscales.
Results
Table 1 displays means, standard deviations, and correlations among study variables. Mean scores for the MAAS and PAI Aggression subscales were consistent with those of previous research from clinical samples (e.g., Dakwar et al., 2011; Kirby et al., 2012). As displayed, trait mindfulness was negatively and significantly correlated with drug and alcohol use, as well as all four Aggression subscales. In addition, trait mindfulness was positively correlated with age. Drug use was positively associated with all four Aggression subscales, and alcohol use was positively associated with aggressive attitude and the Composite Aggression subscale. Age was negatively associated with all Aggression subscales, with the exception of aggressive attitude.
Means, Standard Deviations, and Correlations Among Study Variables.

p < .05. **p < .01. ***p < .001.
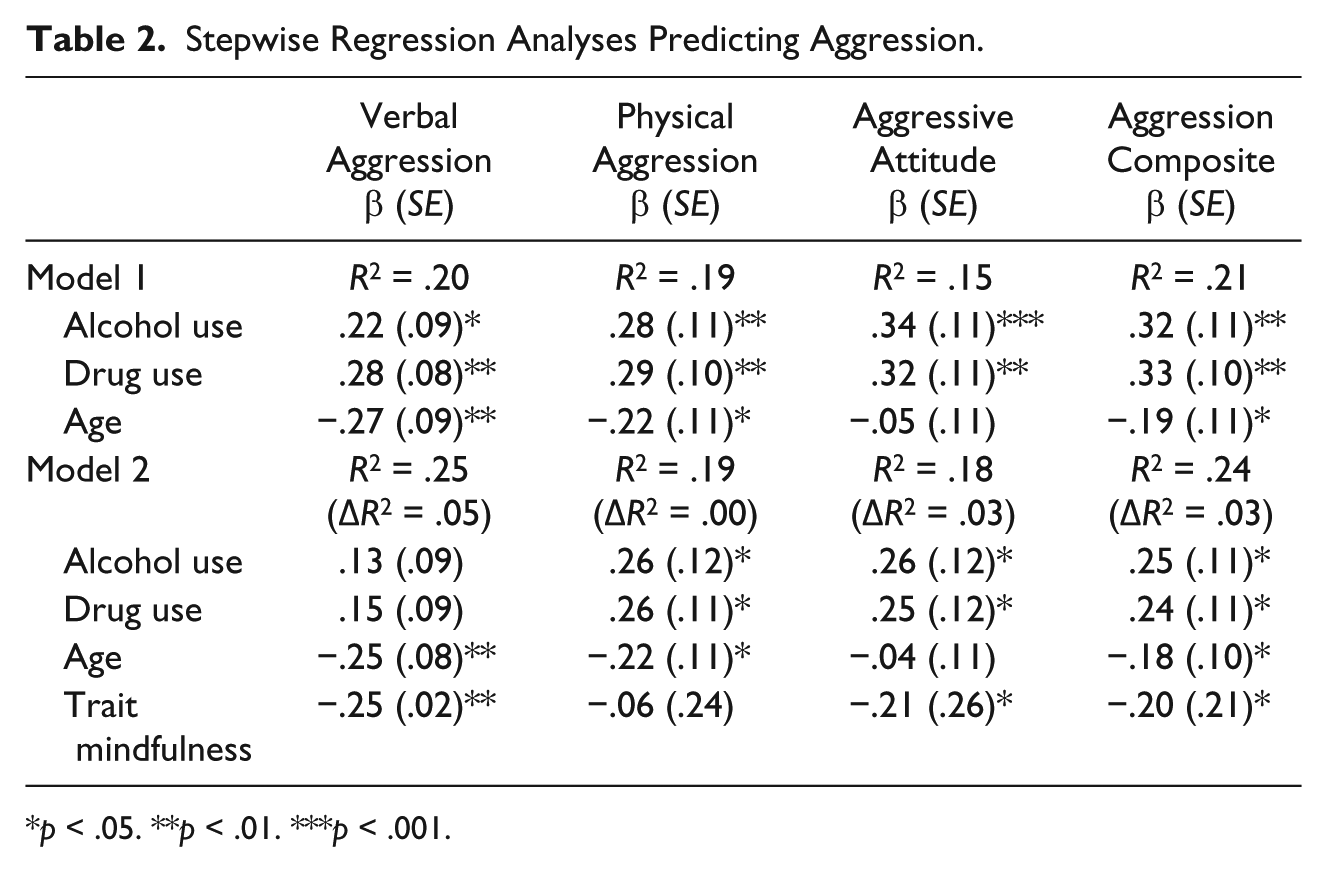
Table 2 displays the results of the stepwise regression analyses. As displayed, for verbal aggression, trait mindfulness remained negatively and significantly associated, as did participant age. For aggressive attitude, results demonstrated that trait mindfulness remained negatively associated, and alcohol and drug use remained positively associated. For the overall Composite Aggression subscale, both trait mindfulness and participant age were negatively associated, whereas alcohol and drug use were positively associated. Trait mindfulness was no longer significantly associated with physical aggression. Participant age, alcohol, and drug use were all significant predictors of physical aggression.
Stepwise Regression Analyses Predicting Aggression.
p < .05. **p < .01. ***p < .001.
Discussion
Mindfulness has been increasingly investigated among individuals seeking substance use treatment and only recently has been studied as a correlate of aggressive behavior. Due to the high prevalence of aggressive behavior among individuals seeking substance use treatment, the current study examined whether trait mindfulness was associated with aggression among men seeking residential substance use treatment. Consistent with hypotheses, trait mindfulness was negatively correlated with verbal and physical aggression, aggressive attitude, and a composite aggression score of all three types of aggression. Moreover, even after controlling for alcohol use, drug use, and age, all known predictors of aggression, trait mindfulness remained significantly associated with verbal aggression, aggressive attitude, and the composite aggression score. To our knowledge, this is the first study to examine and demonstrate a relation between trait mindfulness and aggression among individuals seeking substance use treatment, a population at heightened risk of aggressive behavior.
Findings from the current study were consistent with previous research that has demonstrated significant relationships between trait mindfulness and verbal/psychological aggression (e.g., Borders et al., 2010; Heppner et al., 2008; Shorey, Seavey et al., 2014). However, to our knowledge, this is the first study to demonstrate more aggressive attitudes to be negatively associated with trait mindfulness. Because higher levels of trait mindfulness is associated with non-judgment and compassion, it makes sense that individuals lower in trait mindfulness may be more prone to hold aggressive attitudes and cognitions. Indeed, Heppner and colleagues (2008) demonstrated that trait mindfulness was negatively associated with hostility, which can be interpreted as similar to aggressive attitudes. Additional research is needed that replicates these findings among individuals seeking substance use treatment and other clinical populations.
It is interesting to note that trait mindfulness did not remain significantly associated with physical aggression in the regression analyses. This finding is consistent with that of a study on college students that also did not find a significant relationship between trait mindfulness and physical aggression (i.e., Heppner et al., 2008). There are a number of potential explanations for this finding. First, it is possible that trait mindfulness is only related to physical aggression through some third variable. That is, the relation between trait mindfulness and physical aggression is likely mediated by variables more proximally associated with aggression. For instance, state angry affect or acute alcohol intoxication may mediate this relationship for individuals low in trait mindfulness. This would be consistent with previous research with college students demonstrating that the relationship between mindfulness and physical aggression was fully mediated by anger management (i.e., Shorey, Seavey et al., 2014). As discussed below, there are a number of possible mediators that should be examined in future research that incorporates longitudinal designs.
Although statistically significant in three of the four models, it should be noted that trait mindfulness accounted for only a small amount of variance in the overall prediction of aggression in the stepwise regression analyses. It would be easy to interpret these findings as lacking in clinical value due to this small amount of variance, but as discussed below, we believe that it is likely that the relation between trait mindfulness and aggression is mediated by a multitude of factors that would be more closely linked to episodes of aggression. Thus, it is not overly surprising, in our opinion, that trait mindfulness did not account for a larger proportion of the variance in the prediction of aggression. Still, caution should be taken in the interpretation of findings until additional research replicates and extends our findings in substance abuse treatment seekers.
The results of this study and other research (e.g., Borders et al., 2010; Heppner et al., 2008; Shorey, Seavey et al., 2014), as well as theoretical writings on mindfulness and aggression (e.g., Fix & Fix, 2013), raise the possibility that mindfulness-based interventions may help reduce aggressive behavior. This is an empirical question that remains unanswered. Nonetheless, given that existing violence prevention and intervention programs are largely abysmal in reducing aggressive behavior (e.g., Shorey et al., 2012; Stuart, Temple, & Moore, 2007), there is a need for innovative programs that address aggression, and mindfulness-based approaches may be one such intervention. As applied to individuals seeking substance use treatment, mindfulness-based interventions have already proven effective in reducing risk of relapse (Bowen et al., 2009), and it is possible that modifications of these programs to include a focus on aggression may concurrently reduce aggressive behavior, above and beyond aggression that declines as a result of reductions in substance use. Future research is needed that explores this possibility.
Directions for Future Research
Findings from the present study provide initial evidence of a relation between trait mindfulness and aggression among men seeking substance use treatment, although there is a wealth of research still to be conducted in this burgeoning area. One direction for future research is to determine whether trait mindfulness is associated with violence against intimate partners among men in substance use treatment. Violence against intimate partners is highly prevalent among men in substance use treatment (Stuart et al., 2009) and previous research with female college students has demonstrated negative associations between trait mindfulness and violence against dating partners (e.g., Shorey et al., 2014). Knowing whether this relationship exists across populations, including men seeking substance use treatment, will help inform our understanding of the relation between trait mindfulness and intimate partner violence.
Another area for future research is to examine potential mediators of the relationship between trait mindfulness and aggression among men seeking substance use treatment. For instance, previous research has demonstrated that rumination (Borders et al., 2010) and anger management (Shorey et al., 2014) have mediated the relation between trait mindfulness and aggression among college students, although there is a wealth of hypothesized mechanisms for the beneficial effects of mindfulness that could be examined. For instance, previous research has shown that greater emotion regulation is associated with higher trait mindfulness (Goodall et al., 2012), that emotion regulation improves after mindfulness-based interventions (Goldin & Gross, 2010), and that emotion regulation is associated with aggression (Shorey, Brasfield, Febres, & Stuart, 2011; Tager, Good, & Brammer, 2010). Thus, it is possible that emotion regulation may be one of many pathways through which mindfulness is related to aggression. Other possible mediators could include mental health symptoms (e.g., depression, posttraumatic stress), distress tolerance, trait anger, or empathy, to name a few. Additional research is needed that examines these potential mediators. In addition, future research should also examine the relationship between trait mindfulness and aggression while simultaneously examining other personality variables known to be associated with substance use and aggression (e.g., antisocial personality traits, neuroticism).
Although preliminary, given the extensive literature supporting mindfulness-based programs for the improvement of a wide range of mental health disorders and problems, including substance use (e.g., Bowen et al., 2009; Bowen & Enkema, 2014), it may be fruitful for future research to investigate mindfulness-based interventions for violence among individuals seeking substance use treatment. Indeed, mindfulness-based interventions is an area that has been previously discussed as a new direction for violence intervention research (e.g., Shorey et al., 2012), although no known research has examined the effectiveness of mindfulness-based interventions for violence among substance use patients. It is possible that mindfulness-based interventions could help reduce aggression, for example, by enhancing emotion regulation, reducing impulsivity, and increasing compassion for self and others. Moreover, research on Dialectical Behavior Therapy (DBT; Linehan, 1993), which includes instruction in mindfulness meditation, has shown promise with substance use (e.g., Dimeff, Rizvi, Brown, & Linehan, 2000) and adaptations of DBT for aggression (Wupperman et al., 2012), lending further support to the possibility that mindfulness-based interventions could be highly effective for reductions in violence.
Limitations
The present study has a number of limitations that should be addressed in future research. The sample was comprised of primarily non-Hispanic Caucasian men, which limits the generalizability of findings to more diverse treatment-seeking populations. Future research should examine these relations among women who seek substance use treatment, as they represent a population with high levels of aggressive behavior (e.g., Stuart et al., 2009). In addition, the treatment facility where charts were reviewed does not utilize structured diagnostic interviews for assessing substance use disorders and, therefore, future research should utilize such interviews. This would also allow for the examination of comorbid mental health disorders. The use of a single measure of mindfulness limits our ability to determine whether different facets of mindfulness are more strongly associated with aggression. For instance, prior research has demonstrated that different dimensions of mindfulness, such as non-reactivity, are associated with aggressive behavior against intimate partners among female college students (Shorey et al., 2014). Thus, future research should examine whether different facets of mindfulness are associated with aggression among men seeking residential substance use treatment. In addition, future research should use aggression measures that identify specific forms or targets of aggression (e.g., aggression against intimate partners) to further examine the relation between trait mindfulness and aggression among substance use treatment seekers, as the PAI assessed aggression generally and thus limits the conclusions that can be made. Finally, the cross-sectional nature of the present study precludes the determination of causality among study variables and limits the conclusions that can be drawn from the results. There is a need for longitudinal research on the relation between trait mindfulness and aggression, as to date the existing research has all been cross-sectional.
Conclusion
In summary, the current study demonstrated that trait mindfulness was negatively associated with aggression among men seeking residential substance use treatment. Moreover, trait mindfulness was associated with aggression even after controlling for alcohol use, drug use, and age, all known correlates of aggression. Although preliminary, these findings and those of other research on trait mindfulness and aggression raise the possibility that mindfulness-based interventions may help with the reduction of aggression, although this remains an empirical question. Thus, future research should continue to examine the relation between trait mindfulness and aggression among individuals in substance use treatment, including potential mediators of this relationship, as well as possible effects of mindfulness-based interventions.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by grants F31AA020131 and K24AA019707 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) awarded to the first and last authors, respectively.