
Abstract
This study examined the demographic features, trauma profiles, clinical severity indicators, problem behaviors, and service utilization characteristics of youth victims of commercial sexual exploitation (CSE) compared with a matched sample of sexually abused/assaulted youth who were not exploited in commercial sex. Secondary data analysis and propensity score matching were used to select a sample of 215 help-seeking youth who were exploited in prostitution (n = 43) or who were sexually abused/assaulted but not exploited in prostitution (n = 172) from the National Child Traumatic Stress Network Core Data Set (NCTSN CDS). Propensity Score Matching was used to select a comparison sample based on age, race, ethnicity, and primary residence. Statistically significant differences were noted between the groups on standardized (e.g., UCLA Posttraumatic Stress Disorder Reaction Index [PTSD-RI], Child Behavior Checklist [CBCL]) and other measures of emotional and behavioral problems (e.g., avoidance and hyperarousal symptoms, dissociation, truancy, running away, conduct disorder, sexualized behaviors, and substance abuse). This study provides useful insight into the symptom and service utilization profiles of youth exploited in commercial sex as compared with youth with other types of sexually exploitive experiences. Targeted screening and event-sensitive measures are recommended to more accurately identify youth exploited in commercial sex. More research is needed to determine if and what modifications to trauma therapies may be required to address the more severe symptomatology and behavior problems associated with youth exploited in commercial sex.
Commercial sexual exploitation of children (CSEC) is not a new social problem, but our understanding of it has changed in the past decade. CSEC is defined by the World Congress Against Commercial Sexual Exploitation of Children as “sexual abuse by an adult and remuneration in cash or kind to the child or a third person or persons” (Mutarbhorn, 1996, p. 3). Examples of CSEC include exploitation of minors in prostitution, sexual activity of minors that is controlled by a pimp, in strip clubs, massage parlors, Internet sex sites, or through pornography. CSEC is sometimes termed “sex trafficking of minors,” which is defined by the Trafficking Victims Protection Act (TVPA) of 2000 as
the recruitment, harboring, transportation, provision, or obtaining of a person for the purpose of a commercial sex act . . . in which a commercial sex act is induced by force, fraud, or coercion, or in which the person induced to perform such an act has not attained 18 years of age. (22 USC § 7102; 8 CFR § 214.11(a))
Unlike other forms of human trafficking, no proof of force, fraud, or coercion is needed when the person in commercial sex is under age 18 because children cannot consent to commercial sex (Boxill & Richardson, 2005).
Research has found that the majority of youth who are exploited in commercial sex had prior child welfare involvement (Gragg, Petta, Bernstein, Eisen, & Quinn, 2007), due in part to exposure to sexual abuse (Medrano, Hatch, Zule, & Desmond, 2003; Nixon, Tutty, Downe, Gorkoff, & Ursel, 2002; Potterat, Rothenberg, Muth, Darrow, & Phillips-Plummer, 1998; Raphael & Shapiro, 2002; Stoltz et al., 2007; Tyler, Hoyt, Whitbeck, & Cauce, 2001; Walker, 2002; Widom, 1995). Although the prevalence of child sexual abuse among women involved in commercial sex ranged from 26% to 73.3% in these studies, sexual abuse has consistently been identified as a robust risk factor for involvement in commercial sex.
Many youth who have been trafficked in commercial sex were runaways or truant before and/or after the trafficking began (Greene, Ennett, & Ringwalt, 1999; Nadon, Koverola, & Schludermann, 1998; Smith, Vardaman, & Snow, 2009). Youth who are exploited in commercial sex are likely to be involved with the adult or juvenile justice system, either directly because of their involvement in commercial sex or for status (e.g., truancy, runaway, beyond control), or public offenses that are related to their involvement in commercial sex (Gragg et al., 2007; Reid, 2010). However, it is important to recognize that many youth in traditional community settings (i.e., those who live at home and attend regular schools) are also commercially sexually exploited. These youth may be even more difficult to identify and provide effective interventions for, because they may not present with overt behavioral problems.
Exploitation in commercial sex inflicts psychological trauma on youth, negatively impacting development and future attachments (Gozdziak & Bump, 2008). Research has documented that CSEC is associated with complex trauma (Graham & Wish, 1994), posttraumatic stress disorder (PTSD; Farley, Baral, Kiremire, & Sezgin, 1998; Tsutsumi, Izutsu, Poudyal, Kato, & Marui, 2008), damaged sense of self, compromised interpersonal boundaries and distrust of others (Curtis, Terry, Dank, Dombrowski, & Khan, 2008; Smith et al., 2009), suicidality (Greene et al., 1999; Van Brunschot & Brannigan, 2002), anxiety and depression (Tsutsumi et al., 2008), and substance abuse (Nadon et al., 1998). Sex trafficking inflicts social deprivations, including stigmatization (Curtis et al., 2008), social isolation (Klain, 1999), and mistrust of others (Smith et al., 2009). This list of documented harms to youth victims of commercial sexual exploitation overlaps considerably with those associated with sexual abuse of youth. One of the questions that arises is “Does the commercial nature of CSE, including the frequency of sexual exploitation and greater number of perpetrators (i.e., traffickers, buyers), have a differential impact on youth compared with youth who experience noncommercial sexual exploitation?”
Purpose of the Study
Before sexually exploited youth can receive appropriate services, they must be identified as victims of CSE. Since behavioral health providers treat youth who present with trauma exposure and/or behavioral problems, these providers are in a critical position to identify youth who have been exploited in commercial sex activities. Given the paucity of literature with respect to CSEC and the provision of mental health services, we used data from the National Child Traumatic Stress Network Core Data Set (NCTSN CDS) as a starting point to better understand the histories, mental health symptoms/needs, and service utilization patterns for a clinical sample of youth exploited in commercial sex. Moreover, since prior sexual abuse/sexual assault is a known risk factor for CSE, this study compared the types of trauma exposure, trauma-related symptomatology, functional impairments, and problem behaviors of a clinical cohort of CSE victims (defined as youth who reported involvement in prostitution in the CDS) with a comparison clinical group of youth who had no reported involvement in prostitution but had a history of sexual abuse/assault to aid in screening and treatment protocols for youth who are exploited in commercial sex.
There are several study hypotheses. Compared with youth with sexual abuse/assault but no reported exploitation in commercial sex, youth who have reported exploitation in commercial sex (a) will be more likely to report involvement in the juvenile justice system, (b) will be more likely to have functional impairments (including academic problems, behavioral problems, truancy, history of running away from home, attachment problems, sexual behavior problems, alcohol and drug use, suicidality, self-injurious behavior, conduct disorder, and criminal activity), and (c) will be more likely to have clinically significant levels of PTSD, and have higher rates of externalizing behavioral problems.
Method
Participants and Setting
The overall CDS sample consisted of 14,088 clients from 56 NCTSN centers across the United States, representing all four census regions (West, Midwest, South, and Northeast). NCTSN assessment and treatment services were provided in a variety of child service settings, including community-based outpatient mental health clinics, child welfare agencies, juvenile justice facilities, and schools. Only 43 youth met the current study definition of confirmed exploitation in prostitution. To adequately assess the proposed hypotheses, several analytical steps were taken to create an appropriate comparison group to the youth who reported exploitation in prostitution.
First, the sample was reduced to those who reported exploitation in prostitution (n = 43) or youth aged 10 to 20 years who had a history of sexual abuse/maltreatment or sexual assault. Males and females, aged 18 to 20 years, were included in the sample to capture all the data of prostitution-involved clients served by participating child trauma treatment centers contributing to the CDS. Second, the data were further restricted to reduce heterogeneity due to inherent differences between NCTSN centers because of different service settings, treatment populations, and geographical locations. As a result, we limited our initial sample to 1,129 participants seen at the 16 sites with at least one client exploited in prostitution, because these centers differ from other centers in important ways that cannot be controlled for in the analysis (i.e., larger metropolitan areas, agency setting). The remaining sample was still large and unbalanced with inherent differences between the 43 youth victms of CSE and remaining sample on extraneous variables that could confound or bias the results. Conducting the analysis on such unbalanced groups could result in overly exaggerated statistical significance, making it difficult to judge the magnitude of group differences. Therefore, to make the final comparison group more comparable in size and composition and to minimize bias, propensity score matching was used to approximate random selection, with matching on key demographic variables: (a) age, (b) race—White, Black, Other, Unknown, (c) Latino ethnicity, and (d) primary residence (e.g., lives at home with family, foster care, residential treatment center, other).
The propensity score matching technique in the current study uses a logistic regression model to predict differences in sexual exploitation by accounting for the “matched” demographic characteristics that may be associated with sexual exploitation in the comparison group of CDS youth. In other words, this technique attempts to reduce the bias due to confounding variables (e.g., demographics) that could be associated with sexual exploitation by simply comparing outcomes across the two groups of youth. As a result, the comparison group more closely represents a matched cohort from a probability sample (Pearl, 2000; Rosenbaum & Rubin, 1983, 1985).
The CDS was a quality improvement initiative, and all participating NCTSN centers were subjected to individual center Institutional Review Board (IRB) reviews and approvals, in addition to the regulatory procedures and guidelines of the Duke University Health System IRB. After obtaining requisite approvals and exemptions, centers entered into a fully executed data use agreement with Duke University, as the data were stored in a repository at the Duke Clinical Research Institute (DCRI). All procedures for data collection met state and federal regulations for human subject protection.
Measures
The CDS is comprised of data derived from a battery of measures administered at intake, and every 3 months until the end of treatment. In the current study, only baseline intake data were analyzed. All forms and measures were available in English and Spanish.
Demographic characteristics
Demographic characteristics, including age, gender, race, ethnicity, and primary residence, were collected as part of the CDS battery. Terms and definitions for race and ethnicity complied with the Office of Management and Budget guidelines.
Indicators of severity
Clinicians used a 3-point scale, consisting of 0 (not a problem), 1 (somewhat a problem), and 2 (very much a problem), to rate the degree to which various types of impairment in youth behavior and functioning were present across a range of psychosocial domains, including academic problems, behavior problems in school or home, substance use, and other medical problems or disabilities. These Indicators of Severity were designed to capture impairments in day-to-day functioning that are common in trauma-exposed populations. Dichotomous variables (no/yes) were recoded from these 3-point scale values, such that cases with a response of 0 (not a problem) were recoded with a 0 (no) response, and cases with responses of 1 (somewhat a problem) or 2 (very much a problem) were recoded with a 1 (yes) response for the dichotomous variables.
CSE
The NCTSN CDS included only one question that ascertained potential CSE status: “exchanging sex for money, drugs, or other resources.” This question was included on the Indicators of Severity Form described in the previous paragraph. Cases with a response of 0 (not a problem) were coded as 0 (not exploited in prostitution), and cases with responses of 1 (somewhat a problem) or 2 (very much a problem) were coded as 1 (exploited in prostitution).
Clinical problems
Clinicians rated the degree to which children met criteria for 13 Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) disorders (e.g., depression, PTSD, generalized anxiety), other trauma-related symptoms (e.g., dissociation), and behavioral problems at intake. Ratings were made on a 3-point scale ranging from 0 (not present), 1 (possibly present/subclinical) to 2 (definitely present/met full criteria). Dichotomous variables (No/Yes) were recoded from these 3-point scale values, such that cases with a response of 0 (not present) were coded with a 0 (No) response, and cases with responses of 1 (possibly present/subclinical) or 2 (definitely present/met full criteria) were coded with a 1 (Yes) response for the dichotomous variables.
The Trauma History Profile
The clinician-administered Trauma History Profile (THP), administered at intake, was derived from the UCLA PTSD Reaction Index (UCLA PTSD-RI; Steinberg, Brymer, Decker, & Pynoos, 2004). The THP assesses exposure to 19 different types of trauma, loss, and separation on a 3-point scale. Definitions for some of the maltreatment trauma types were consistent with the definitions used in the National Child Abuse and Neglect Data System (NCANDS) glossary. Clinicians endorsed whether each event did not occur, occurred, or was suspected to have occurred, based on clinical interviews with the child, caregiver, and other collateral reporters (e.g., caseworkers). Each trauma type was accompanied by specific instructions, definitions, and examples to enhance reporting accuracy. Sexual maltreatment/abuse was defined as “actual or attempted sexual molestation, exploitation, or coercion by a caregiver,” and sexual assault was measured with the item, “actual or attempted sexual molestation, exploitation, or coercion not by a caregiver and not recorded as sexual abuse.” A computed variable was created from the sum of the total number of trauma types endorsed.
Service utilization
Service utilization, assessed at intake, referred to any services received 30 days prior to assessment and treatment services at an NCTSN center or clinic. Services examined ranged from residential treatment, case management, and in-home counseling to outpatient treatment and school-based services. For each of the 19 services described, respondents endorsed whether the child had received any of the services by checking No, Yes, or Unknown.
UCLA PTSD-RI
The UCLA PTSD-RI is a questionnaire to screen both for exposure to traumatic events and for PTSD symptoms in children and adolescents aged 7 or more years (Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998). It can be used as either a self-report or clinician-administered instrument, and assesses the frequency of occurrence of PTSD symptoms during the past month, rated from 0 (none of the time) to 4 (most of the time). The items map directly onto the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; APA, 1994) Criterion B (re-experiencing), Criterion C (avoidance/numbing), and Criterion D (arousal) for PTSD. A total of 20 of the items directly assess PTSD symptoms, while 2 additional items assess associated features: fear of recurrence and trauma-related guilt. Scoring algorithms permit tabulation of total PTSD-RI total score, and B, C, and D symptom subscale scores. Psychometric properties are fairly robust and have been previously described (Steinberg et al., 2004).
Child Behavior Checklist
The Child Behavior Checklist (CBCL) 6 to 18 was completed by a parent or caregiver who knew the child well. This widely used measure consists of 113 items scored on a 3-point scale ranging from 0 (not true) to 2 (often true) and yields scores on two broadband scales: Internalizing and Externalizing, as well as scores on DSM-IV-oriented scales, and empirically based syndrome scales that reflect emotional and behavioral problems and symptoms. The measure has been found to have sound psychometric properties with respect to reliability (with α coefficients of .98 and higher) and validity, across racially and ethnically diverse samples (Achenbach, 2009).
Procedure
The CDS standardized data collection takes place across a variety of settings within the NCTSN. Clinicians and clients completed the full CDS battery at intake. Clinician ratings drew on information reported in the intake interview that variably included child report, parent report, and school or archival reports, where available. Licensed clinical providers, with a master’s degree or higher, were trained in the administration, scoring, and interpretation of the CDS protocol. Real-time reports, quality control and data verification checks, and ongoing consultation and technical assistance were provided by the UCLA–Duke University National Center for Child Traumatic Stress, the coordinating center for the NCTSN. All monitoring procedures were implemented throughout data collection to ensure consistency and accuracy of reports.
Data Analysis
For continuous variables, means and standard deviations served as descriptive statistics; and for categorical data, frequencies and associated percentages were reported. Tests for significant differences between groups on types of trauma exposure, psychological distress, and service utilization were conducted using t tests for continuous variables and chi-square tests for categorical variables. Further comparisons of clinical significance for standardized measures, including odds ratios, were estimated using mixed models (fitted with SAS PROC GLIMMIX), with random effects adjusting for variability associated with differences between study sites. When applicable, missing data were addressed by listwise deletion of records without recusant data.
Results
Table 1 summarizes demographic information/matching variables for the two groups. No significant between-group effects exist for any of these variables, indicating that the propensity score matching yielded appropriate comparison groups. The final comparison cohorts were a sample of 43 youth with reported exploitation in commercial sex, ranging from age 10 to 20 years (median 14.5 years), and a sample of 173 youth who were not reported to be exploited in commercial sex, ranging from age 10 to 19 years (median 15 years). Both samples were predominantly female (< 80%), with approximately a third of the sample in residential treatment.
Demographic Characteristics for Matched Samples by Type of Sexual Exploitation (Sexual Abuse/Sexual Assault or CSE).
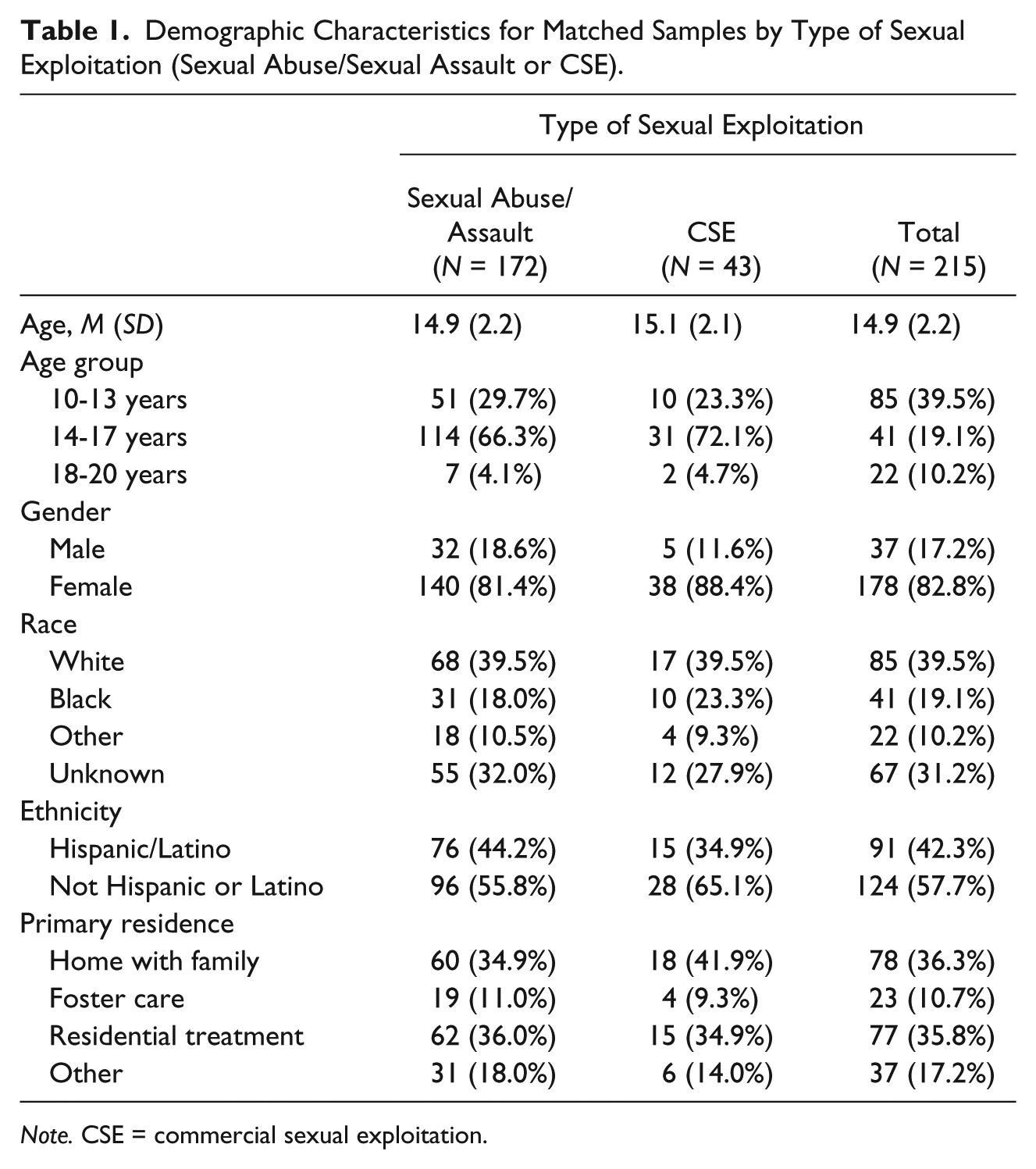
Note. CSE = commercial sexual exploitation.
The prevalence of exposure to the reported trauma types for each group is presented in Table 2. Because individuals were included in the comparison cohort based on their history of sexual maltreatment/abuse or sexual assault, it was expected that more individuals in this group would report each type of sexual trauma, and this was found for sexual maltreatment/abuse. Nonetheless, there was no significant difference by group in sexual assault prevalence. There were no other significant differences in trauma types by group. The two groups had experienced a similar average number of trauma types.
Trauma Type Prevalence for Matched Samples by Type of Sexual Exploitation (Sexual Abuse/Sexual Assault or CSE).

Note. Trauma types are not mutually exclusive. Boldface indicates that the bivariate relationship between the variable and the endorsement of prostitution indicator is statistically significant (*p = .05. **p = .01. ***p = .001). CSE = commercial sexual exploitation.
There were also few statistically significant differences in terms of service utilization in the last 30 days (not depicted in a table). The CSE group did have statistically significant higher rates of involvement with detention centers (20.9% vs. 5.9%, χ2 = 9.47, p < .01), hospital emergency rooms (21.4% vs. 9.8%, χ2 = 4.27, p = .04), and self-help groups (19.0% vs. 7.3%, χ2 = 5.32, p = .02) than the matched comparison group. Both groups (i.e., CSE group vs. matched comparison group) had high service utilization rates for residential treatment (34.9% vs. 35.5%), case management (48.8% vs. 51.8%), and child welfare (53.5% vs. 51.8%).
Percentages of reported functional impairments endorsed on the indicators of severity form are presented in Table 3. The CSE group had significantly higher rates on several indicators that can be classified as at-risk behaviors: skipping school (χ2 = 14.46, p < .01), sexualized behavior (χ2= 23.56, p < .01), alcohol use (χ2= 20.77, p < .01), substance abuse (χ2= 25.71, p < .01), criminal activity (χ2= 24.86, p < .01), and running away (χ2= 31.91, p < .01). These results were reflected further by the Clinical Problems for which the CSE group had significantly higher (not depicted in a table) prevalence of sexual behavior problems (61.0% vs. 29.2%, χ2= 14.39, p < .001), conduct disorder (24.4% vs. 6.8%, χ2= 10.81, p < .01), general behavioral problems (73.8% vs. 50.3%, χ2= 7.44, p < .01), and substance abuse (65.9% vs. 32.3%, χ2= 15.45 p < .01). The CSE group also had a higher proportion of youth with dissociation (41.5% vs. 22.4%, χ2= 6.16, p = .01).
Indicators of Severity for Matched Samples by Type of Sexual Exploitation (Sexual Abuse/Sexual Assault or CSE).

Note. Boldface indicates that the bivariate relationship between the variable and the endorsement of prostitution indicator is statistically significant (*p = .05. **p = .01. ***p = .001). CSE = commercial sexual exploitation.
Detailed results concerning the performance of each group with respect to the reported standardized measures of trauma-related symptoms are presented in Table 4. There were greater differences measured between the two groups with the UCLA PTSD-RI than the CBCL. As measured by the CBCL, the CSE group had statistically significant higher standardized scores with respect to Externalizing Behavior Problems (t148 = −2.82, p < .01). However, there were no statistically significant differences in percentage of youth in each sample with scores in the clinical range on the CBCL.
PTSD, Behavioral Problems, and Clinically Significant Symptoms for Matched Samples by Type of Sexual Exploitation (Sexual Abuse/Sexual Assault or CSE).

Note. Odds ratio estimates and statistical significance adjusted for treatment center effect via random effects modeling. The missing cases are due primarily to the age restrictions on each of the Measures 6 to 18, for example, on the CBCL; 7 to 18 on the UCLA PTSD-RI. Boldface indicates that the bivariate relationship between the variable and the endorsement of prostitution indicator is statistically significant (*p = .05. **p = .01. ***p = .001). CSE = commercial sexual exploitation; PTSD-RI = posttraumatic stress disorder reaction index; CBCL = Child Behavior Checklist.
The CSE group had significantly higher standardized scores on the UCLA PTSD-RI, for both the overall score (t196 = −3.04, p < .01) and the subscales measuring avoidance (t196 = −3.17, p < .01) and hyperarousal (t196 = −2.72, p < .01). In terms of clinical significance, the CSE group had significantly higher odds of a clinically significant score for the avoidance subscale (F = 5.67, p = .03). Although the differences between the two groups is not clinically meaningful with regard to the other subscales, it is worth noting that nearly the entire CSE group was in the clinically significant range with regard to both the re-experiencing and hyperarousal subscales.
Discussion
In this study, trauma exposure, largely in the caregiving social environment, was extensive in the group of youth exploited in commercial sex and the comparison group of youth who did not have reported exploitation in commercial sex but had a history of sexual abuse/maltreatment or sexual assault. Youth in the CSE group and in the matched sample of sexually abused or sexually assaulted youth reported a higher average number of types of trauma exposures (5.0 and 5.4, respectively) compared with the overall CDS sample (3.2; Briggs et al., 2013). Most of the frequently reported trauma exposures, with the exception of sexual assault, were within the caregiving social environment, such as sexual abuse and emotional abuse by a caregiver, domestic violence and traumatic separation, loss, and bereavement. Thus, the two groups were similar in experiencing complex patterns of trauma exposure, defined as “children’s experiences of multiple [traumatic] events that occur within the caregiving system—the social environment that is supposed to be the source of safety and stability in a child’s life” (Cook, Blaustein, Spinazzola, & van der Kolk, 2003, p. 5).
Even though only a small number of youth in the NCTSN CDS had reported involvement in prostitution (which was the only measure of exploitation in commercial sex available in the CDS), many of the study hypotheses were supported. Specifically, these youth reported significantly greater involvement in juvenile justice and child welfare, more functional impairments and risk behaviors, more clinical problems, and greater levels of trauma symptoms compared with the matched sample of sexually abused/assaulted youth. This study adds to previous literature in this area by further delineating the symptom and service use profiles of these youth, and suggests that involvement in commercial sex, over and above the effects of sexual abuse and assault, is associated with emotional, developmental, psychological, and behavioral dysregulation in those involved, and presents significant challenges and opportunities for service providers.
Symptom profiles in children are best understood within a developmental context (van der Kolk, 2005). Adolescents and preadolescents are normally struggling with issues of identity and self-esteem, concerns regarding physical appearance, and determinations about what constitutes “normal” behavior (Erikson, 1980). Youth who have experienced sexual abuse are more vulnerable to conflictual relationships with service providers, peers, and family, and misappraisals of danger and threat (Pynoos, Steinberg, & Piacentini, 1999). Youth exploited in commercial sex are often accused of “criminal” activity (e.g., charged with prostitution and placed in juvenile facilities) when these activities should be more accurately viewed as re-victimization experiences (Finkelhor & Ormrod, 2004; Halter, 2010). Exploited youth who were previously sexually abused by exploitive adults become confused about what constitutes kindness, intimacy, and safety, which may result in greater vulnerability to subsequent exploitation by adults (e.g., pimps) who initially seem kind, protective, and safe.
Results of this study are consistent with other research in showing an increased involvement of the CSE group in risk behaviors such as truancy, substance use, criminal activity, and running away, all of which may be a manifestation of reckless and self-destructive behavior included in the newly updated Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) diagnostic criteria for PTSD (APA, 2013, p. 272), reflecting developmental disturbance and the resulting cognitive and emotional distortions that induce these responses. Victimization, particularly victimization that goes unaddressed (including exploitation in commercial sex), can lead to a profound sense of distrust of adults and rules among youth, increasing their risk of delinquency and behavior problems (Buffington, Dierkhising, & Marsh, 2010). Traffickers/exploiters use this distrust of adults to their advantage, further isolating and alienating youth from family or others outside “of the life” who may offer youth a perspective that is markedly different from the perspective the traffickers feed their victims about their involvement in commercial sex (Hardy, Compton, & McPhatter 2013; Lloyd, 2011; Smith et al., 2009). It is also possible that youth who have more behavior problems are more likely to associate with more delinquent peers in deviant social networks, increasing their risk of encountering a trafficker/exploiter.
Dissociation is posited to be connected with the stress response system, such that dissociation functions to automate behavior when the individual is overwhelmed, compartmentalize painful memories, and detach from one’s self when experiencing trauma (Putnam, 1997). Roe-Sepowitz (2012) found that among women involved in prostitution, individuals who were commercially sexually exploited as juveniles had significantly higher scores on dissociation (including depersonalization, out of body experiences, derealization, and psychic numbing) compared with individuals who first became involved in prostitution as adults. When trauma exposure is chronic, an individual will rely more upon dissociation to manage the distress; however, reliance on dissociation as a coping strategy in the response to chronic stress contributes to behavior problems, affect dysregulation, and poor self-concept (Putnam, 1997). Even though the trauma details for the sexual abuse/maltreatment and sexual assault incidents reported by the youth in the sample allowed for comparison of the percentage of youth in each group that experienced repeated incidents of sexual abuse/maltreatment or sexual assault, it was not possible to examine actual frequencies of sexual traumatic events. It is possible that the youth who were exploited in commercial sex who were more likely to be diagnosed with a dissociation disorder experienced a higher number of sexually exploitive experiences, including the sex exchanges (e.g., having sex for food, shelter, or drugs) the youth may not have perceived of as fitting the definition of sexual assault, which in turn increased the likelihood of having a dissociation disorder. Even though some of the sexually abused/assaulted youth in the comparison group may have experienced a high frequency of sexually abusive incidents, it is possible that more of the youth exploited in commercial sex had more sexually exploitive encounters, which could contribute to their higher rates of dissociation disorders.
Children who are sexually abused are more likely than children who are not sexually abused to exhibit sexualized behavior (A. Friedrich, 1993; W. Friedrich, Fisher, & Dittner, 2001; Paolucci, Genuis, & Violato, 2001). In the current study, 29.2% of the youth who were sexually abused/assaulted and were not exploited in commercial sex had a probable or definite diagnosis of sexualized behavior, whereas 60.9% of youth exploited in commercial sex had a probable or definite diagnosis of sexualized behavior. Youth who are exploited in commercial sex are trained by pimps/traffickers to behave sexually. Youth who depend on survival sex (i.e., do not have a third party profiting from their sex exchanges) learn that sexual behavior is a means to securing money, drugs, shelter, or other material necessities, and they continually receive positive reinforcement for their sexualized behavior. In other words, each sex exchange reinforces the sexualized behavior of the child (Farmer & Pollock, 2003). Yet, developmentally inappropriate sexualized behavior among children exerts a significant emotional cost and may increase the risk for greater sexual victimization (Lalor & McElvaney, 2010). Moreover, some research has found that sexualized behavior is particularly resistant to change following treatment for child sexual abuse (Finkelhor & Berliner, 1995). Treatment for any child who exhibits sexualized behavior should include close “supervision, adequate sex education, modification of inappropriate sexual behavior, and therapeutic attention to the needs that underlie such behavior” (Farmer & Pollock, 2003, p. 101).
The finding that youth who were exploited in commercial sex had significantly higher overall scores on the UCLA PTSD-RI, and on the subscales measuring avoidance and hyperarousal compared with the matched group, suggests that exploitation in commercial sex may have unique effects on youth’s trauma symptoms, which may require modifications to treatment. The fact that the two groups had similar types of trauma exposure with the exception of sexual abuse/maltreatment by a caregiver, which was one of the criteria to define the comparison cohort, suggests that exploitation in commercial sex may elicit different trauma symptoms than other types of sexual exploitation.
Given the number of studies that have found delinquency and substance use are correlates of commercial sexual exploitation of children (Brawn & Roe-Sepowitz, 2008; Edwards, Iritani, & Hallfors, 2006; Pedersen & Hegna, 2003), the finding that more commercially sexually exploited youth in this sample had recently been involved with juvenile justice and self-help recovery group meetings is expected. The significant differences in recent service utilization highlight the need to screen for commercial sexual exploitation in juvenile justice, emergency medical care, and substance abuse treatment/recovery group settings. Traffickers often use a victim’s substance use or the victim’s caregiver’s substance use as a means of inducing victims to engage in commercial sex (Palmer, 2010). Furthermore, youth who are involved in commercial sex often use alcohol or drugs to cope with the emotional pain of working in commercial sex (Heilemann & Santhiveeran, 2011; Martin, Hearst, & Widome, 2010).
Limitations
The independent variable, reported exploitation in commercial sex, was measured with one item that measured how much of a problem “prostitution” was for the child, and is most likely underreported for several reasons. First, a wealth of literature has found that service providers often do not assess for involvement in commercial sex, and that even when they do, youth often do not disclose their involvement in commercial sex because of shame, fear of not being believed, and fear of consequences such as being removed from the home, criminal charges against the pimp (i.e., trafficker), and fear of retribution by, and in some cases attachment to, the trafficker (Clawson, Dutch, Salomon, & Grace, 2009; Smith et al., 2009). Moreover, individuals’ (i.e., youth and clinicians’) understanding of what constitutes prostitution may not include certain commercial sex activities that fit the legal definition of prostitution. For example, caregivers allowing adults to have sex with their children in exchange for money, drugs, or shelter fits the definition of commercial sex, but may not fit individuals’ understanding of the term; so even if this type of commercial sex had occurred, they would report “no” to the question about prostitution. Familial sex trafficking of minors is reported in nearly all communities where needs assessments of sex trafficking of minors have been conducted and may be more common than expected (Cole & Anderson, 2013; Smith et al., 2009). Even though prostitution is the most commonly reported commercial sex activity in which children are exploited, there are other types of commercial sex (e.g., child pornography and strip dancing) that are not captured in this measure. Thus, it is possible that some of the youth included in the comparison group were exploited in commercial sex, which would underestimate the differences between the two groups in the analysis and possibly increase the probability of Type II errors. Another related limitation of this study is the small number of youth with reported involvement in prostitution, which reduced the power of the statistical tests to detect differences between the groups.
Propensity score matching was used to address a couple of problems with the large, unbalanced sample of youth who were sexually abused/assaulted but were not exploited in commercial sex that were to be used as a comparison group: (a) minimize bias introduced by inherent group differences, and (b) reduce the sample size of the comparison group to decrease the probability of Type I error. However, use of propensity score matching also limits generalizability of the results to youth who were similar to the CSE group on several demographic variables.
There is no way to determine if the greater reported criminal activity among youth exploited in commercial sex is directly due to their commercial sex activity or if they are more likely to be involved in other types of criminal activity, such as their greater involvement in substance use and status offenses related to running away and truancy. This is a very important issue as discussed above, because youth exploited in commercial sex are frequently inappropriately labeled as criminal when in fact they are the victims of criminal activity. There is a critical need for increased awareness of this distinction among behavioral health providers, as well as in the juvenile justice and child welfare systems. Existing research on how systems intervene with youth exploited in commercial sex has shown that criminalization of youth has been the norm (Institute of Medicine and National Research Council, 2013; Smith et al., 2009), which may exacerbate trauma symptoms and reduce the likelihood that youth will receive appropriate services, such as educational and vocational training that will allow youth to earn their living outside of the commercial sex trade and cognitive behavioral therapy that will facilitate cognitive restructuring of their involvement in commercial sex as victimization (Clawson et al., 2009; Institute of Medicine and National Research Council, 2014). Finally, the lack of recognition of their involvement in CSE is a severe form of victimization, and the criminalization of victims of CSE reduces the likelihood that society will punish their exploiters.
Research Implications
More research is needed on the manifestation of trauma symptomatology of youth exploited in commercial sex, particularly in terms of differences that may be attributable to the nature of their exploitation in commercial sex, to determine if and what modifications to therapeutic interventions are needed. For example, does being exploited by the trafficker and multiple buyers increase trauma symptomatology, shame, or self-blame in youth compared with youth who are sexually exploited in other ways? The findings of the current study suggest that commercially sexually exploited youth’s greater avoidance and hyperarousal symptoms may be in part due to their exploitation in commercial sex, even when compared with a group of sexually abused/sexually assaulted youth. Shame and self-blame are common features of sexual abuse and assault. Nonetheless, do youth exploited in commercial sex, who oftentimes believe their involvement is their own choice, experience greater stigma when others learn of their involvement in commercial sex compared with youth who are sexually abused/assaulted by others in a setting that is not related to commercial sex?
Modifications of existing trauma therapies may be needed to address the youth’s exploitation in commercial sex. Further modification and enhancement of evidence-based trauma therapies (e.g., Trauma-Focused Cognitive Behavioral Therapy [TF-CBT], Trauma Affect Regulation: Guide for Education and Therapy [TARGET]) may be required to address high rates of sexual behavior problems if these problems are particularly resistant to treatment. A recent randomized controlled treatment trial for CSEC on war-exposed girls in the Democratic Republic of Congo demonstrated that TF-CBT was effective for improving PTSD and conduct symptoms, as well as depression, anxiety, and prosocial behaviors (O’Callaghan, McMullen, Shannon, Rafferty, & Black, 2013). The unpredictable and often ongoing trauma in the lives of youth who are exploited in commercial sex (e.g., returning to the pimp, being rejected by family and community due to having been commercially exploited) may also require evidence-based treatment applications.
Clinical and Policy Implications
Increasingly, there is a call for providers who work with at-risk youth, such as in the juvenile justice system, to screen for trauma histories (Buffington et al., 2010). Providers may believe that using a trauma inventory such as the Traumatic Events Screening Inventory (Ippen et al., 2002) and the Child Welfare Trauma Screening Tool (Igelman et al., 2007) would identify a child’s exploitation in commercial sex. However, youth may not disclose involvement in commercial sex that has not already been identified by the juvenile justice system because they may not perceive their involvement in commercial sex as fitting with the items that assess sexually exploitive experiences. Screening for commercial sex may be most effective when conducted by a clinician who has developed rapport with a child. Loyola’s Center for the Human Rights of Children and the International Organization for Adolescents (IOFA) have published a more comprehensive and rapid screening tool for child trafficking (Loyola’s Center for the Human Rights of Children and IOFA, 2011). Clinicians may require more training on how they can build rapport with clients and ask questions in a nonjudgmental, open-ended manner to increase victims’ likelihood of reporting their exploitation in commercial sex. As more youth are identified as victims of CSE in clinical and research samples, more robust studies may examine the effectiveness of various therapies with victims.
Youth who are trafficked in commercial sex are described by service providers as particularly challenging clients with whom to work (Hines & Hochman, 2012; Smith et al., 2009). Effective treatment of trauma occurs in the context of a trusting interpersonal relationship with a qualified professional (Herman, 1997). Unfortunately, the developmental injuries imposed by this type of experience in childhood or adolescence can create a barrier to effective therapeutic engagement. Sensitivity to the effect of complex trauma on youth, in particular the role of disorganized memories, inability to self-soothe, attachment problems, difficulties with appropriate interpersonal boundaries, and understanding how to implement evidence-based treatments for youth with complex trauma will greatly improve professionals’ ability to engage with and respond effectively to youth exploited in commercial sex (Cohen, Mannarino, Kliethermes, & Murray, 2012; Smith et al., 2009). Treatment goals must target these issues of trust, intimacy, and safety, and service environments must offer refuge from exploitive, unsafe conditions if recovery is to occur.
Conclusion
In summary, when entering mental health treatment, youth who were identified as being exploited in commercial sex had higher rates of involvement in juvenile justice, had more functional impairments and risk behaviors, more clinical problems, and greater levels of trauma symptoms compared with a matched cohort of youth who were sexually abused/assaulted but were not identified as being exploited in commercial sex. More research is needed to determine if and what modifications to therapeutic interventions for youth who are sexually abused/assaulted are required to effectively respond to youth who are exploited in commercial sex.
Footnotes
Authors’ Note
The views, policies, and opinions expressed are those of the authors and do not necessarily reflect those of Substance Abuse and Mental Health Services Administration (SAMHSA) or U.S. Department of Health and Human Services (HHS).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This manuscript was developed (in part) under Grants 2U79SM054284 and SM-12-007 from the Center for Mental Health Services (CMHS), Substance Abuse and Mental Health Services Administration (SAMHSA), and U.S. Department of Health and Human Services (HHS).