
Abstract
Lebanese prisoners during the Israeli occupation of Lebanon (1981-1999) were subject to regular torture. We examined the association between torture events and post-traumatic stress and cardiovascular diseases (CVDs) among former women political prisoners. We conducted a retrospective survey and performed health check-ups among 108 former women prisoners. Post-traumatic stress disorder (PTSD) was measured through the Clinician-Administered PTSD Scale (CAPS), and CVDs were assessed by physicians’ diagnoses. The study was conducted between September 2008 and March 2010. All 67 participants in the study reported having been subjected to a variety of torture events. The prevalence of PTSD was 28.4% and that of CVD was 16.42%, respectively. PTSD and CVD were more likely to occur among women who had had longer imprisonment periods, and PTSD specifically was associated with exposure to torture (beating: OR = 1.49; 95% CI [0.48, 4.27] and threatening by rape: OR = 1.43; 95% CI [0.82, 9.30]). CVD was associated with asphyxia with water (OR = 3.86; 95% CI [0.03, 2.28]). Devoutness decreased the risk of PTSD (OR = 0.24; 95% CI [0.08, 1.41]). Torture had adverse long-term effects on prisoners’ physiological and psychological health; devoutness played a significant protective role. This study highlights the importance of documenting torture events and identifying the indicators of associated morbidity among surviving political prisoners for the provision of additional resources to care.
Introduction
During the Israeli occupation in South Lebanon (1981-1999), many Lebanese civilians were detained in the Khiam Detention Center, the largest Israeli prison in Lebanon at that time. Reports of the Commissioner of human rights documented different severe forms of torture and ill-treatment among hundreds of men and women kept in this prison over the span of several decades. Previous studies have also reported 14 deaths as a consequence of physical torture in the same prison (Saab, Chaaya, Doumit, & Farhood, 2003).
Many of the prisoners were released in the late 1980’s and early-mid 1990s and the remainder was released as the withdrawal of the Israeli army from Lebanon progressed in May of 2000. Previous research indicated that Lebanese prisoners held by Israeli forces experienced multiple torture and traumatic events and had a high prevalence of psychological distress that persisted after their release (L. F. Farhood, Chaaya, & Saab, 2010; Saab et al., 2003).
The effects of trauma on the health of prisoners and hostages have been widely discussed in previous literature in various contexts. A recent meta-analysis indicated that former prisoners exposed to war torture face severe psychological consequences including PTSD. The same review highlighted the importance of exploring the applicability of the concept of war torture and PTSD to non-Western populations and areas (Steel et al., 2009). In addition, it is worth mentioning that most studies in this field were based on samples composed solely or predominantly of male populations (Saab et al., 2003). These studies explained PTSD in relation to the exposure to trauma (el Sarraj, Punamaki, Salmi, & Summerfield, 1996; Punamaki, Qouta, & El Sarraj, 2010) and to the severities of the experienced trauma (Basoglu, Paker, Ozmen, Tasdemir, & Sahin, 1994; el Sarraj et al., 1996; Maercker, Beauducel, & Schutzwohl, 2000; Punamaki et al., 2010). Further similar studies explored the general mental health and the quality of life among refugees exposed to torture and traumatic events (Carlsson, Mortensen, & Kastrup, 2006).
At the same time, another systematic review about development and maintenance of PTSD after exposure to war torture trauma recognized the importance of focusing attention on women prisoners, as female gender and older age were risk factors in the development of symptoms of post-traumatic events (Johnson & Thompson, 2008). Furthermore, differences in the types of torture and their psychological consequences between men and women victims of war torture were highlighted in other studies in ex-Yugoslavia. Women were at greater risk for specific types of torture, for example, sexual torture, and had higher scores of depression, anxiety, and other psychological disorders, in particular PTSD, than men (Spiric et al., 2010). In addition, women who were subject to war torture in Nepal were more likely to report PSTD, persistent somatoform pain disorder, and dissociative (amnesia and conversion) disorders than men (Van Ommeren et al., 2001).
However, while the psychological (Olsen, Montgomery, Bøjholm, & Foldspang, 2007; Punamaki et al., 2010; Ramsay, Gorst-Unsworth, & Turner, 1993) and psychiatric morbidity (Maercker, Gabler, & Schutzwohl, 2012; Paker, Paker, & Yuksil, 1992; Ramsay et al., 1993) among political prisoners exposed to torture were explored, little is known about the association between the nature of traumatic events during imprisonment and the health among women prisoners subjected to torture. The general objective of this study is to explore the association between the exposure to torture events and the long-term development of PTSD and cardiovascular disease (CVD) among former women political prisoners.
Method
Participants and Procedure
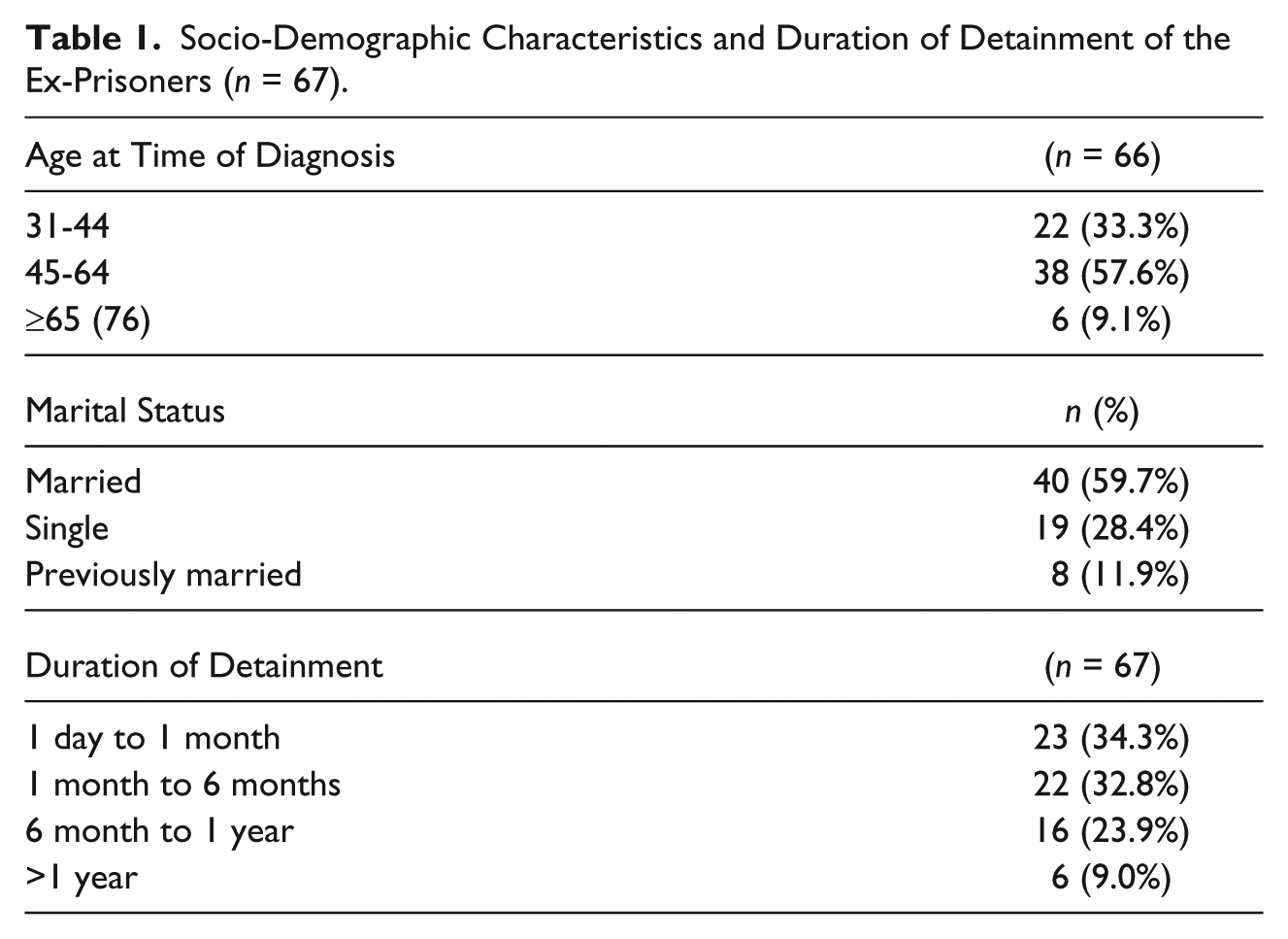
The study sample consisted of 67 Lebanese women prisoners previously imprisoned in the Khiam Detention Center during the Israeli occupation of Lebanon and released throughout the period from 1982 to 1997. Participants who agreed to take part in the study represented 62% of the total of 108 women who received clinical and psychological follow-up care from Khiam Rehabilitating Center (KRC), a Lebanese non-governmental organization that offered rehabilitation services to former Lebanese prisoners since 2006. The study sample has similar distribution to the total population (estimated to be around 500 women detained during the Israeli occupation in Lebanon) in terms of age and duration of imprisonment, as documented in the internal reports of the Khiam Rehabilitation Center: Average mean age on imprisonment and duration of imprisonment was 27.36 years and 212 days, respectively, in the study sample and 29.78 years and 188 days in the study population (Table 1).
Socio-Demographic Characteristics and Duration of Detainment of the Ex-Prisoners (n = 67).
In this retrospective study, former women prisoners were interviewed during the period between September 2008 and March 2010 after obtaining their informed oral consent. The individual interviews took place after the rehabilitation sessions at the KRC office and were performed by two trained psychologists. Only five individuals received home rehabilitation, and thus were interviewed at home. The study protocol received approval from the Ethics and Research Committee at the Researchers’ University.
Measures
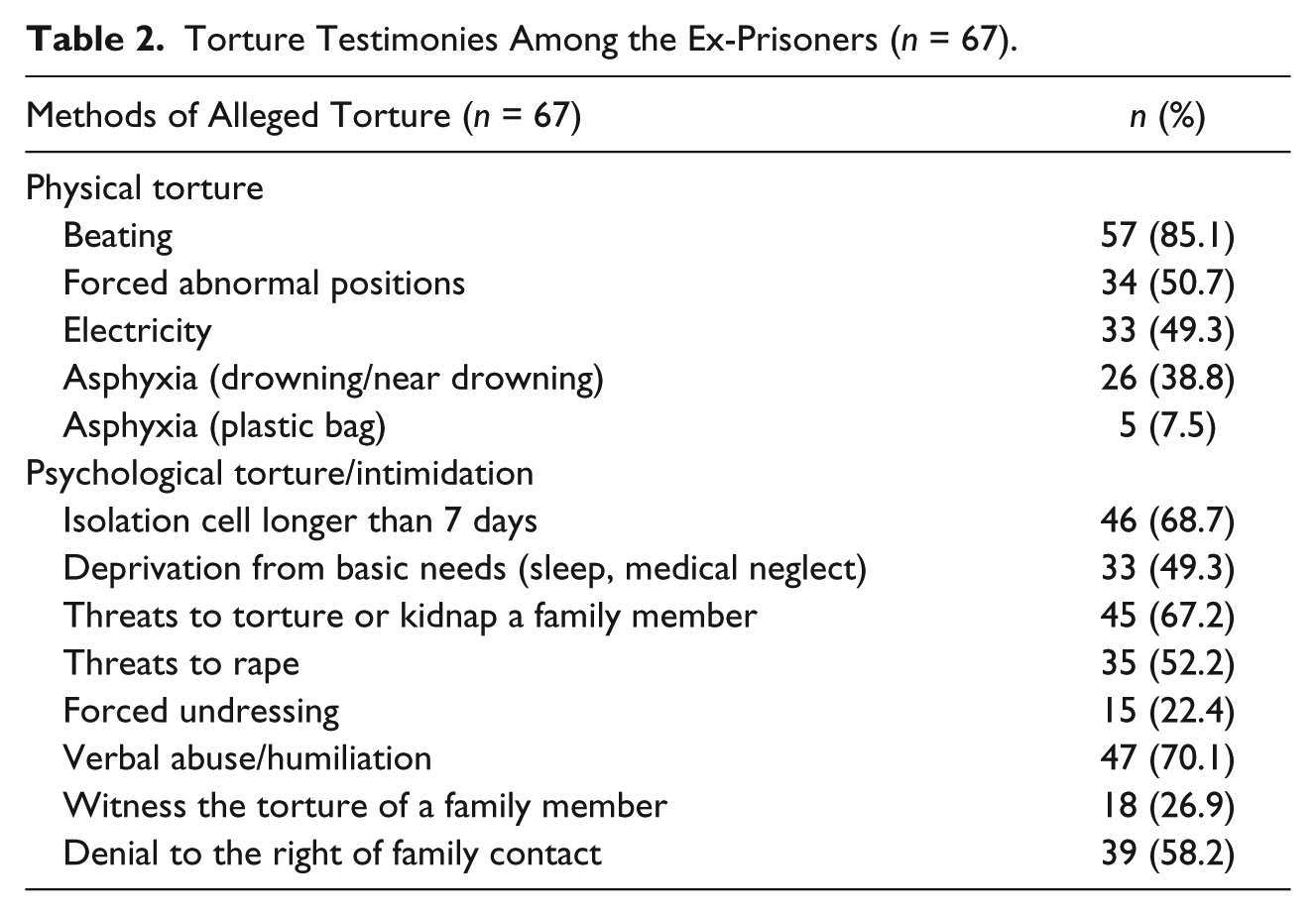
Information about previous exposure to traumatic torture events was based on self-reported testimonies of the participants during the interviews. The interviews were performed in private by one of the authors who is a trained psychologist working with the KRC (Z.A.). The interviews were individual and open and avoided leading questions. The term “physical or psychological abuse” was used instead of the word “torture” in the interviews and in the consent form. A simplified version of the protocol of the International Rehabilitation Council for Torture Victims (IRCT) was used to monitor data. Answers were categorized into two groups (physical torture or psychological torture; Table 2). The individual testimonies about torture events that were obtained from the different participants were then cross-matched by the same interviewer (Z.A.) to assess the consistency of answers.
Torture Testimonies Among the Ex-Prisoners (n = 67).
Post-traumatic stress disorder
PTSD was assessed through the Clinician-Administered PTSD Scale (CAPS) validated into Arabic and previously used on Arabic-speaking populations . This scale measures the frequency but not the intensity of the PTSD symptoms and follows the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. This 17-item core symptom scale assesses three criteria: re-experiencing symptoms, avoidance symptoms, and arousal symptoms. The frequency of each symptom’s occurrence in the past week is rated on a 6-point scale, ranging from 0 (not at all) to 5 (more than 1 day). Examples of questions include, “How often have you experienced flashbacks of past unpleasant events?” PTSD was reported if at least one symptom of re-experiencing the traumatic event, three or more symptoms of avoidance, and two or more symptoms of over-arousal were found. Test–retest reliabilities for the three-symptom cluster have been found to range from 0.77 to 0.96 and from 0.90 to 0.98 for the 17-item core symptom scale (Blake et al., 1995). The internal consistencies in the present study (as measured by the Cronbach’s alpha coefficient) were between 0.74 and 0.89 for the three-symptom cluster and were 0.84 for the 17-item scale.
Social support
Social support was assessed with eight closed-ended questions about the women’s perception of people’s views toward them after their release (e.g., if they felt needed, respected and appreciated by others; if they have someone to rely on for emotional support; if they have financial support). Scores of the social support scale were obtained by adding the scores of the individual items that ranged from 0 (not at all) till 3 (always). The social support scale was adopted from an existing social support scale used in the same country on a similar population (Farhood, Dimassi, & Lehtinen, 2006). The Cronbach’s alpha for this study was 0.78.
Clinical physical examinations
In addition, participants underwent clinical physical examinations to identify the presence of CVD. Electrocardiography and ankle–arm blood pressure measures were taken to document myocardial infarction and peripheral artery disease, respectively. The examinations were performed at the KRC clinic by an experienced cardiologist and included the assessment of precordial or retrosternal pain, palpitation, cyanosis, dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, nocturia, edema, heart murmur, hypertension, coronary artery disease, discoloration of hands or feet, varicose veins, intermittent claudication and thrombophlebitis.
Information about participants’ age, age on arrest, marital status, year and place of birth, and duration of imprisonment was also collected. Marital status was re-coded into three classes—single, married, and ever-married, as the sample contained few divorced or widowed women. Age was re-coded into three categories (31-44, 45-64, and ≥ 65 years) to compare cardiovascular morbidity as per the Center of Disease and Control classification of the age-specific groups (Centers for Disease Control and Prevention [CDC], 2011). Duration of imprisonment was categorized into four groups: 1 day to 1 month, 1 to 6 months, 6 to 12 months, and more than 1 year, taking into account the percentile values.
Devoutness
Finally, devoutness was assessed by asking the participants the following question: “Do you have faith or consider yourself religious?”
Analysis
The associations between the exposure to torture events and PTSD and CVD were assessed through constructing two multiple logistic regression models using the SPSS statistical program. The dependent variables (PTSD and CVD) were dichotomized as 1 for presence and 0 for absence. The explanatory variables included in the regression were the ones that showed statistical significance in the univariate analyses (p value set at .01). The adjusted odds ratios with 95% confidence intervals were calculated.
Results/Findings
Participants’ socio-demographic characteristics and duration of imprisonment are presented in Table 1. The age at the time of the interview ranged from 31 to 76 years (M = 48.97, SD = 9.89). The age on imprisonment ranged from 16 to 56 years (M = 27.36, SD = 9.86). All participants were detained during the period between 1981 and 1999. The majority of the imprisonments (46%) occurred during years 1985 to 1990, while 28% took place between 1991 and 1995, 17% between 1996 and 1999, and 9% during the first few years following the 1981-Israeli invasion to Lebanon (1981-1984). The duration of imprisonment ranged between 3 days and 7 years (M = 212 days and SD = 225.9 days). The mean time since imprisonment was 22.6 years, and the standard deviation was 4.09.
Table 2 displays the frequencies and percentages of women who reported exposure to a variety of traumatic events, including physical and psychological torture, often associated with deprivation and sexual harassments.
All participants reported exposure to one or more forms of physical torture. The majority (85.1%) described events of severe random beatings with bare hands, legs, and instruments, such as whips and wooden sticks. Participants also reported that beatings were mainly on the back of the feet, the back, the abdomen, and the head, and in some cases, on the face (causing nose and teeth breaks). Others reported events of torture by means of electric currents induced through electric wires connected to the hands, legs, and sensitive body organs. Torture by asphyxia (obstruction of the airways inducing suffocation with water or with plastic bags) was also commonly reported. Others reported having been forced to stay in uncomfortable positions for long periods of time (standing on one foot, tied to chairs, tied to gates in the cold, and under the rain). Participants also described different forms of deprivation torture such as the denial of the basic needs (limited access to food, water, and shower). One liter of water was given per six prisoners per day, for example. Cell hygiene conditions were described as draconian; for example, as substitutes to toilets, cells had buckets that were not changed for weeks. Participants also reported deprivation from family contact and medical attention. Most of the participants reported torture by the forced inhalation of gasses.
In addition, participants gave accounts of various forms of psychological torture. The most frequently reported events were solitary confinement for 3 days to 1 week, deprivation from sleep, threats of kidnap, torture or murder of family members, forced undressing, and threats of rape. Participants also recalled psychological pressure under long hours of aggressive interrogations without rest.
Participants also described various forms of verbal abuse including threats, humiliation and intimidation that was used for the purpose of frightening the women detainees and humiliating their integrity and religious beliefs. The majority (45 women) reported hearing sounds of other women being tortured in adjacent rooms, 18 of who reported witnessing torture of other prisoners. In addition, about half of the interviewed women reported being threatened with rape. The most frequently reported form of sexual ill-treatment included forced removal of the veil (a fact that humiliates their values and religious beliefs) and forced removal of clothes and undergarments.
The prevalence of PTSD among the participants was 28.4%; all reported PTSD cases were imprisoned for more than 1 month. Table 3 shows the association between PTSD and the individual characteristics, as well as the torture events that had statistically significant links to the symptom criteria of PTSD in the univariate analysis. PTSD was more likely to occur among women who were exposed to beating (OR = 1. 49; 95% CI [0.88, 3.27]), threatened with rape (OR = 1.43; 95% CI [0.82, 5.30]), and imprisoned for longer periods of time (6 months to 1 year and above 1 year; OR = 2.35; 95% CI [1.63, 8.55] and OR = 3.23; 95% CI [0.43, 4.74], respectively). In addition, women who had high scores of devoutness were less likely to develop PTSD (OR = 0.24, 0.08, 1.21). The effect size estimate R2 was 0.36, which describes the proportion of variability accounted for by each independent variable in the regression model.
Logistic Regression With PTSD as Dependent Variable as Explained by Torture Events and Control Variables Among Former Women Prisoners (n = 67).

Note. PTSD = Post-traumatic stress disorder.
The medical examinations ended up with the diagnosis of 11 cases (16.42%) of CVDs, which included hypertension, arrhythmias, ischemic heart disease, and heart failure. Table 4 shows the association between the exposure to torture events and CVD, after controlling for age. The multiple logistic regression model showed that women who spent longer periods of time in detention (6 months to 1 year and >1 year) were more likely to develop CVD (OR = 8.56; CI [0.42, 13.09] and OR = 21.22, CI [0.96, 65.77], respectively) than those detained for less than 1 month (reference group). In addition, torture by asphyxia with water was significantly associated with CVD (OR = 3.86; 95% CI [0.63, 2.28]). Age remained greatly associated with CVD: Women between 45 and 64 years (OR = 5.36; 95% CI [0.06, 27.18]) and above 65 years (OR = 12.85; 95% CI [0.43, 12.32]) were more likely to develop CVD than those less than 40 years old (reference group). In addition, although devoutness and social support decreased the risk of CVD, the association was not statistically substantial (p = .55 and p = .22, respectively). The effect size estimate R2 was .28.
Logistic Regression With CVD as Dependent Variable as Explained by Torture Events and Control Variables Among Former Women Prisoners With CVD (n = 67).

Note. CVD = cardiovascular disease.
Discussion
The current study revealed that the prevalence of PTSD and CVD among former women prisoners exposed to traumatic torture events during imprisonment was high one to two decades after their release. The prevalence of PTSD among the tortured former prisoners in the study sample was high (28.4%), but comparable with that among political tortured prisoners in Lebanon (30.6%; Farhood et al., 2010), among political tortured prisoners in Occupied Palestinian Territory (Punamaki et al., 2010), and among political prisoners in Germany (33%; Maercker et al., 2000). However, the prevalence of CVDs adjusted for age was relatively high in the study sample as compared with a normal population of women belonging to the same age group not previously exposed to torture (16.42% vs. 6%, respectively; CDC, 2011; Mittelmark et al., 1993). In addition, in agreement with other studies, the prevalence of CVD was the highest in the older age group (33.33% in the age group > 65 years).
Another important finding was that the risk to develop PTSD increased with the duration of imprisonment and with exposure to beating and threatening with rape and decreased with devoutness. The present findings seem to be consistent with other research that found that sexual harassment and threatening by rape increased the risk for PTSD (Hooberman, Lhewa, & Keller, 2007). Results of this study disagree with other studies that found that religiousness is a risk for post-traumatic symptoms (Halvorsen & Kagee, 2010). On the other hand, the results of this study replicated previous knowledge about the protective role of social support against PTSD (Steel et al., 2009) and the positive role of spirituality on health and rehabilitation outcomes (Agger, Igreja, Kiehle, & Polatin, 2012) among survivors from traumatic torture events. In addition, results of the current study pointed out that the risk to develop CVD increased with the duration of imprisonment, age, and exposure to asphyxia with water. These results are consistent with those of other studies and suggest that asphyxiation, which is commonly associated with generating fear and stress, is associated with adverse health effects including cardiac problems and vagal inhibition (Ely & Hirsch, 2000; van Beeck, Branche, Szpilman, Modell, & Bierens, 2005).
The present study has certain limitations that have to be taken into consideration on the interpretation of the results. First, it should be mentioned that the sample size was rather small to permit definitive conclusions: The study covered 67 out of the 500 women released from Israeli prisons (as estimated per KRC). Although non-participants had similar characteristics with the study population in terms of duration and conditions of detention (the majority were detained in the same Khiam prison), caution should be taken on the generalization of the results to the larger population, especially taking into consideration the obtained effect size in the regression models. It is also important to bear in mind the possible bias related to the selection of the participants. In fact, participants were those who had the will and the means to participate in the rehabilitation programs of KRC. One could argue that a considerable number of people have not participated in rehabilitation programs perhaps to avoid remembering traumatic events experienced during imprisonment (Agger, 1989), which implies a source of underreporting in the results. Another fact that could jeopardize the internal reliability of the results is the underreporting that is commonly observed in studies concerning self-reported measurements among populations exposed to torture (Heisler, Moreno, DeMonner, Keller, & Iacopino, 2003), especially in conservative societies. However, one could argue about the validity of the self-reported measures of previous torture events. Actually, it is known that forensic investigation is the standard objective method for the documentation of torture and its consequences, as per adopted international guidelines, in particular the Istanbul International Protocol on the “Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment” (Moreno & Iacopino, 2008; Perera & Verghese, 2011). Furthermore, the UN Human Rights Council has encouraged the adoption of the principles of this protocol and use forensic examination as a useful tool to combat torture. However, it could be argued that although forensic examination is a gold standard measure of the exposure to torture among male torture survivors, it might not have the same applicability and validity for female torture victims or prisoners. One acknowledged difference in this regard is that male survivors’ cultural contexts make them less likely than women to disclose details of sexual ill-treatment when interviewed by one or the other gender (Sorsoli, Kia-Keating, & Grossman, 2008). Nevertheless, it should be noted that although forensic examination did not take place after imprisonment, the consistent way the respondents described their exposures to previous torture events (types and frequency of beatings, description of the deprivation torture, such as the type of food, the scarcity of water, the way of receiving electrical shocks) added more credibility to their self-reported answers. In addition, while the majority of the participants were detained and released in the 80s and the 90s, diagnostic data were collected in 2008, the fact that implies a retrospective information bias that can impact the recall of former exposure to risk variables. Nevertheless, it is worth noting that long-term effects of trauma on PTSD are well documented in previous research (Basoglu et al., 1994; Maercker et al., 2012; Ramsay et al., 1993). In fact, there is conflicting evidence about the association between PTSD and the acuteness of trauma (time since release), as some studies describe an increased risk (Kanninen, Punamaki, & Qouta, 2002) and others show a decreased risk of PTSD with acuteness of trauma (Maercker et al., 2012). Furthermore, it should be noted that relevant data related to lifestyle (cigarette smoking, drug or tranquilizer consumption, exercise, sleeping and working hours) and major life events (changes in social status in the past year, death of a loved-one and daily problems related to loss of work and financial situations) was not measured, despite their possible effects on the morbidity. It would be quite interesting to use the Life Events scale in future research (L. Farhood, Dimassi, & Lehtinen, 2006) as a method of evaluating these events and adjusting the analysis to their possible confounding effects. Moreover, although devoutness decreased the risk of PTSD in the present study, these results should be interpreted with caution as devoutness was measured with only one item rather than a validated measure.
One of the issues that emerge from the study’s findings is the importance of maintaining clinical services for the support of torture victims and the prevention of PTSD and CVD that could persist for decades after exposure to torture. The study findings illustrate the importance of the involvement of physicians in the care for survivors of torture and the provision of expert testimony on behalf of torture victims. Future studies on the current topic are recommended to rely on modern technologies in measuring previous exposure to torture events. Imagery techniques such as plain films, scintigraphy, computed tomography, and MRI guarantee an unbiased documentation of the anatomical and pathological changes occurring after exposure to torture (Vogel, Schmitz-Engels, & Grillo, 2007). As a matter of fact, such objective methods for the documentation of torture events abide by the Istanbul protocol on the documentation of torture (Perera & Verghese, 2011). Last, the documentation of torture is an important approach for the recognition of the victims, the restoration of their rights, and the prevention of torture in the long term (Holst, 2012; van Beeck et al., 2005).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.