
Abstract
The current conflicts in Afghanistan and Iraq present unique risk factors for military personnel that increase the likelihood of psychological distress and concomitant consequences related to trauma. Several studies have found that the stress brought about by financial difficulties, unemployment, and the need to renegotiate roles and responsibilities with spouses following discharge increases the likelihood of relationship strain and even intimate partner violence in the veteran population. This study was undertaken to determine the challenges related to maintaining healthy relationships for college student veterans who have served in the armed forces since September 11, 2001. Psychological distress, substance use, and hypermasculine attitudes were explored as risk factors for intimate violence. Social support was found to be a protective buffer against psychological aggression. However, approximately a third of college student veterans reported low social support along with symptoms of distress, placing them at elevated risk of partner abuse. The current article explores models for predicting risk of perpetrating aggression in college student veterans and concludes that culturally tailored programs and services are needed.
Since October 2001, nearly 2 million U.S. troops have deployed as part of Operation Enduring Freedom (OEF, Afghanistan) and Operation Iraqi Freedom (OIF, Iraq; American Council on Education [ACE], 2012; Steele, Salcedo, & Coley, 2010; Tanielian, 2009), and more than 420,000 military personnel have deployed multiple times (Korb, Rundlet, & Bergman, 2007; Tanielian & Jaycox, 2008). More than half (52%) of these veterans are between the ages of 20 and 29, the phase of life now understood as “emerging adulthood,” a critical period focused on identity development in both intimate relationships and career (Arnett, 2004). As American troops withdraw from the conflicts in the Middle East, thousands of veterans are returning to civilian society and are initiating or reassuming responsibilities related to pursuing education, occupations, and family and relationship roles. Currently, there are over 1000,000 veterans receiving education benefits under United States Code Title 38, which known as the G.I. Bill (U.S. Department of VA, National Center for Veterans Analysis and Statistics, 2011; National Center for PTSD & VITAL, 2014) with about 66% enrolled at 2-year colleges (Radford, 2011). In contrast to the traditional undergraduate population, almost three quarters of college student veterans are male (Radford, 2009). A report by the ACE Foundation (Radford, 2009) reveals that 62% have a dependent spouse or child.
Compared with their non-military peers, military members and veterans experience a higher incidence of psychological and relational difficulties (Hoge et al., 2004; Swords to Plowshares, 2011). According to the Armed Forces Health Surveillance Center (AFHSC) Report (2013), mental health problems are actually the leading cause of hospitalization for active duty service members. In fact, mental disorders are the only category of illness or injury for which hospitalization rates significantly increased during the first 11 years of the Iraq and Afghanistan conflicts (AFHSC, 2013). Not surprisingly, the current literature demonstrates that post-deployment mental health symptoms affect returning warriors in a variety of ways including work effectiveness, family stability, and social interactions (Harmon, Hoyt, Jones, Etherage, & Okiishi, 2012). Veterans of the current conflicts in the Middle East (OIF/OEF) present unique concerns and symptoms related to the nature of modern warfare. Exposure to improvised explosive devices (IEDs), multiple deployments, and chronic hypervigilance related to the lack of clear battle lines, coupled with higher survival rates overall, has resulted in unprecedented numbers of veterans returning home with trauma-related symptoms, brain injuries, and other disabilities (Hoge et al., 2004). Combat experience has been identified as the primary stressor associated with mental health problems such as posttraumatic stress disorder (PTSD; Harmon et al., 2012) and soldiers serving more than one tour of duty have been found to be 50% more likely to suffer from PTSD than soldiers serving one tour (Hoge et al, 2004).
Several studies across different samples of veterans (Bradley, 2007; Cascardi & Vivian, 1995; Riggs, Caulfield, & Street, 2000; Straus, 1990) have found that PTSD, depression, substance abuse, and hypermasculine attitudes cultivated in military environments can be understood as factors that increase the likelihood of intimate partner violence (IPV; Savitsky, Illingworth, & DuLaney, 2009). However, the existing literature suggests that veterans’ adjustment to civilian life is significantly influenced by their perceived social support, with higher support relating to less psychological distress, a reduced likelihood of posttraumatic stress symptoms, lower rates of anger and hostile behavior, and greater satisfaction with interpersonal relationships (Barrera, Graham, Dunn, & Teng, 2013; Benotsch, Brailey, Vasterling, & Sutker, 2000; Brewin, Andrews, & Valentine, 2000; Cohen, Gottlieb, & Underwood, 2000; Cohen & Wills, 1985; Csibi & Csibi, 2011; Holahan & Moos, 1991; Pietrzak, Johnson, Goldstein, Malley, & Southwick, 2009). Thus, the purpose of this study was to understand the factors that predict aggression in intimate partner relationships for college student OIF/OEF veterans.
Literature Review
Alarming rates of IPV in marital relationships where one partner is a combat veteran have been well documented across different samples (Bradley, 2007; Morland, Leskin, Block, Campbell, & Friedman, 2008; Solomon, Dekel, & Zerach, 2008; Teten, Sherman, & Han, 2009). A 2005 review (Marshall, Panuzio, & Taft, 2005) of the existing literature on the prevalence of IPV in the military revealed that rates of partner violence ranged from 13.5% to 58%, across military and active veteran samples with lower rates revealed in non-clinical populations. Moreover, self-reported rates of IPV among military couples are higher than rates among civilian couples (Jones, 2012; Stamm, 2009). Heyman and Neidig (1999) found that wives of Army servicemen stationed in at 38 different U.S. installations experienced significantly higher rates of moderate partner violence (13.1% vs. 10.0%) and severe partner violence (4.4% vs. 2.0%) as compared with their civilian counterparts. Moderate violence included having something thrown at them, being pushed, grabbed, shoved, slapped, kicked, bit, or hit with a fist, and severe violence entailed being beaten up, choked, assaulted, or threatened with a weapon. Although Army servicemen themselves reported committing moderate partner violence at rates comparable with those of men in the civilian sample (10.8% vs. 9.9%, respectively), these servicemen reported committing significantly higher rates of severe husband-to-wife violence than did the civilian men (2.5% vs. 0.7%). In another sample of approximately 15% of White male personnel of 38 randomly selected army bases located across the 48 contiguous Unites States, 30% reported perpetrating IPV during the past year (Pan, Neidig, & O’Leary, 1994).
Psychiatric symptoms appear to play a primary role in IPV perpetration. Recent studies of different veteran samples have revealed that veterans with PTSD (Byrne & Riggs, 1996; Marshall et al., 2005; Savarese, Suvak, King, & King, 2001) or depression (Sherman, Sautter, Jackson, Lyons, & Han, 2006) are more likely to perpetrate violence toward their partners as compared with veterans without these disorders. It is estimated that up to 35% (700,000) post-9/11 Global War on Terror veterans experience some form of posttraumatic stress (Institute for Operations Research and the Management Sciences, 2009). In a recent study by Taft et al. (2009) of post-9/11 recent tour veterans, 33% of veterans experiencing posttraumatic stress were identified as domestic violence abusers. More specifically, in a recent study of 129 male combat veterans screened at the National Center for PTSD/VA Boston Healthcare System between 2003 and 2008, Taft and colleagues (2012) found that PTSD was particularly associated with higher rates of IPV particularly in men who had not experienced head contact events (e.g., concussion). Other studies of combat veterans reveal a significant relationship between the severity of PTSD symptoms and the severity of domestic violence perpetrated (Finley, Baker, Pugh, & Peterson, 2010; Gerlock, 2004; Sayers, Farrow, Ross, & Oslin, 2009).
In a study of couples seeking relationship therapy at a Midwestern Veterans Affairs Clinic between 1997 and 2003, Sherman et al. (2006) found that more than 80% of depressed veterans committed at least one act of violence (e.g., slapping partner) in the last year, and more than 40% committed at least one severe act of violence (e.g., choking partner). Studies of both Vietnam era veterans, and of a cross sample of veterans seeking help at a VA clinic, reveal that combat veterans with depression, as well as those with PTSD, display higher levels of anger than do combat veterans without either disorder, supporting the hypothesis that anger, rather than combat experience itself, may best predict the likelihood of perpetrating IPV (Novaco & Chemtob, 2002; Sherman et al., 2006). Among OIF/OEF veterans with current or recently separated partners, 53.7% reported incidents of shouting, pushing, or shoving, and 27.6% reported that their partner was “afraid of them” (Sayers et al., 2009). The same study revealed that depressed veterans identified acts of anger or violence as the reason for seeking counseling.
Ample evidence exists that abusing alcohol and other drugs increases the propensity to perpetrate IPV (Hurlbert, Whittaker, & Munoz, 1991; Kantor & Straus, 1987; O’Keefe, 1997; Straus, 2000). According to the Substance Abuse and Mental Health Services Administration (SAMHSA, Office of Applied Studies, 2007), 7.1% of veterans met the criteria for past year substance use disorder (SUD), and a breakdown by age reveals that 25% of veterans aged 18 to 25 meet those criteria. Veterans with PTSD and depression are highly likely to self-medicate through the use of alcohol and other drugs, with about 75% to 79% meeting the criteria for co-morbid substance abuse disorders (Kulka et al., 1990; L. A. Taylor, Kreutzer, Demm, & Meade, 2003). Marshall et al. (2005) reported that IPV rates among veterans suffering from substance abuse disorders and PTSD range from 1 to 3 times higher than IPV rates in the general population, and the severity of substance abuse is correlated with the frequency and severity of partner abuse.
The structure and culture of military life itself pose considerable challenges for veterans returning home after deployments, because many of the skills and behaviors that are considered adaptive and necessary for survival during war conflict with behaviors that are considered appropriate in the civilian world (Demers, 2008; Hoge, 2010). Military recruits learn to separate themselves from individual emotions, depersonalize acts of violence, and dehumanize the other, to successfully fight wars. Moreover, recruits use battlemind, the “inner strength to face fear and adversity in combat with courage” (Adler, Bleise, McGurk, Hoge, & Castro, 2009, p. 930), in part, through the utilization of aggression. These attitudes are closely related to hypermasculinity, an extreme and rigid adherence to beliefs and characteristics associated with the masculine gender role (Jones, 2012; Katz, 2006; Kivel, 1992; Morris, 1996), and are associated with adherence to domestic violence myths, a set of attitudes and beliefs that serve to justify and excuse committing IPV (Katz, 2006; Kivel, 1992; Peters, 2008; Tolman, 1989, 1999). Morris (1996), for example, proposed that in some military units, men bond with each other around stereotypically masculine characteristics such as dominance, aggression, risk taking, and develop and maintain shared attitudes that support anger toward women and the abuse of female partners. Supporting this suggestion, Rosen, Kaminski, Parmley, Knudson, and Fancher (2003) found that in a sample of married male soldiers who were stationed in Alaska in 1998, increased cohesion and group disrespect, characterized by rude aggressive behavior, conversations that degrade women, consumption of pornography, sexualized discussion, and the encouragement of alcohol use, was associated with increased mean frequency of IPV at both the group and the individual levels. Using cultural spillover theory as a framework, Bradley (2007) analyzed data from the National Survey of Families and Households Wave 1 (1987-1988) to determine whether military training and culture were related to higher rates of IPV among veterans who had separated from military and their spouses. Cultural spillover theory (Baron & Straus, 1987, 1989) suggests that the more a given subculture supports the use of violence to attain socially approved ends, the greater the likelihood that this legitimization of violence will spill over, or be generalized, into other spheres of life. Contrary to expectations, Bradley found that, in his sample, veterans were no more likely than non-veterans to engage in IPV. Furthermore, it is possible that the length of separation time from the military acted as a mediating factor, and that the population under investigation had become sufficiently reintegrated and re-acculturated into civilian norms so as to be protected from IPV risk.
Furthermore, the recent literature suggests that many veterans experience a crisis of identity and report a deep sense of disconnection from family members and other civilians when they return from war and separate from the military (Armstrong, Best, & Domenici, 2005; Demers, 2009; Hoge, 2010). In a meta-analysis of risk factors for PTSD in trauma-exposed adults, Brewin and his colleagues (2000) found that, across the existing literature, factors such as lack of social support and life stress were more strongly linked to trauma effects as compared with individual-level vulnerability. Indeed, social support appears to be inversely related to ongoing effects of PTSD, including relationship problems, as suggested by a 2004 study of Vietnam veterans (Schnurr, Lunney & Sengupta, 2004). A lack of positive social support has also been identified as a primary correlate of IPV, with evidence suggesting that men who feel disenfranchised may use violence against female partners as a way to establish a sense of dominance or social control (Renzetti, 2011).
In sum, the current returning veteran population experiences unique challenges related to reassuming relationship roles and managing hostility. A preponderance of the literature reveals that perpetrators of intimate violence are characterized by reliance on psychological aggression in conflict management, low verbal negotiation skills, adherence to domestic violence myths, and marked anger reactions (Barnett, Miller-Perrin, & Perrin, 2010). Distinct risk factors for perpetrating partner violence in veterans include depression, anxiety, substance abuse, and hypermasculinity. Given the paucity of the literature about IPV risk and co-morbid problems among student veterans on college campuses, this study was undertaken to understand specific factors that predict aggression in the intimate partner relationships of post-9/11 student veterans. It was hypothesized that based on existing research, psychological distress and substance abuse would play a primary role in predicating the characteristics associated with intimate violence perpetration in veterans (Elbogen, Beckham, Butterfield, Swartz, & Swanson, 2008). Based on extant studies, veterans’ identification with hypermasculine attitudes (Jakupcak, Blais, Grossbard, Garcia, & Okiishi, 2013; Katz, 2006) was believed to predict IPV risk beyond the primary effects of psychological symptoms. Conversely, as supported by relevant research, we predicted that social support would reduce the likelihood of aggression, hostile attitudes, and anger in relationships, even in the face of psychological strains and hypermasculinity characteristic of military veterans (Hoge, 2010; Hoge et al., 2004).
Method
Participants
In all, 230 people agreed to participate in an online survey assessing issues for college student veterans. However, only 166 people met the criteria for the study (U.S. post-9/11 veterans currently attending a California college and in a relationship with a significant other). Of those, 79% (n = 131) were male and 21% (n = 35) were female veterans. Due to the small sample, data from female respondents were not included in this analysis. The participants ranged in age from 19 to 50 with the average age 29.3 years (SD = 5.96 years). A total of 39% were part of the Army branch of service, 23% Marines, 20% Navy, 14% Air Force, and the remaining 4% Coast Guard. The majority of participants (60%) indicated their current status as “separated” from military service. In total, 3% reported that they were currently on active duty status, 21% reported that they were on reserve status, and 3% were currently serving in the National Guard. An additional 13% reported that they were retired. A total of 6% reported that they had never been deployed overseas, 23% reported they had been deployed overseas once, and 71% reported that they had been deployed overseas multiple times. Although not all post-9/11/2001 military service indicates deployment to a combat zone, a full 77% of participants in the current sample had experienced at least one deployment to Iraq or Afghanistan.
Procedure
Veterans who had served in the military since September 11, 2001, were recruited from California State Universities and Community Colleges, via flyers, email listservs, and Craigslist advertisements. Participants were directed to an anonymous, electronic survey that included informed consent and was designed using standardized measures (See Appendix A) to assess psychological distress (Brief Symptom Inventory [BSI]; Derogatis & Melisaratos, 1983), alcohol use (Alcohol Use Disorders Identification Test [AUDIT]; Babor, Higgins-Biddle, Sunders, & Monteiro, 2001), drug use (Drug Abuse Screening Test [DAST]; Skinner, 1982), hypermasculine attitudes (Hypermasculinity Index [HI]; Peters, Nason, & Turner, 2007), social support (Social Support; Boscarino, 1995), relationship satisfaction (Relationship Assessment Scale [RAS]; Hendrick, 1988), conflict tactics (Conflict Tactics Scale [CTS]; Straus, Hamby, Boney-Mccoy, & Sugarman, 1996), domestic violence myth beliefs (Domestic Violence Myth Acceptance [DVMAS]; Peters, 2008), and anger (Dimensions of Anger Reactions Revised [DAR 5]; Hawthorne, Mouthaan, Forbes, & Novaco, 2006). A resource list of veteran-specific counseling services was provided, and participants were directed to a second website to enter an email address to participate in a drawing for one of six Apple Ipods. Institutional review board (IRB) approval was granted by San José State University. Completion of the survey indicated consent.
Results
The current study provides a descriptive snapshot of IPV in male college student veterans. Although the majority of our sample of college student veterans (80%) indicated satisfaction with their relationship, approximately one third (36%) reported problems in their relationship and 25% endorsed beliefs related to IPV. Veteran students’ beliefs were supported by their self-reported behaviors: 68% insulted or swore at their partner, 67% had shouted at their partner, 12% had threatened to hit or throw something at their partner, 12% had grabbed their partner, 10% had destroyed something of partner’s, and 28% had coerced their partner to have sex with them.
To understand risk factors for IPV, we explored the ways in which psychological distress, substance use, hypermasculine attitudes, and social support were related to psychological aggression, using verbal negotiation tactics instead of violence, domestic violence myth endorsement, and anger. Individuals reporting high levels of psychological distress, substance use, and hypermasculine attitudes were predicted to have greater anger reactions, lower use of negotiation strategies, higher adherence to domestic violence supportive beliefs, and high levels of psychological aggression.
Existing research provided the basis to examine psychological distress and substance abuse as primary predictors of risk for IPV. Based on extant studies, veterans’ identification with hypermasculine attitudes was believed to predict IPV risk beyond the effects of psychological symptoms. In contrast, building on the existing literature, social support was understood as decreasing the likelihood that a veteran would commit IPV, even in the face of mental health concerns, substance abuse, and stereotypically masculine attitudes. Correlational and regression analyses were conducted to examine the relationships between these variables.
Descriptive Statistics
Contrary to expectations, means of self-reported concerns were low in the current sample. On average, based on a 5-point Likert-type scale (0 = not at all, 1 = a little bit, 2 = moderately, 3 = a lot, 4 = very much), participating veterans did not report experiencing high levels of psychological distress (M = 1.06, SD = 0.89, as compared with a mean of 0.93 found across subscales in University students, and a mean of 1.36, SD = 0.86, among psychiatric inpatients; Derogatis & Melisaratos, 1983; Hayes, 1997) or anger (M = 1.4, SD = 1.1) Similarly, though 7.1% of veterans overall experience a substance abuse disorder (SAMHSA, Office of Applied Studies, 2007), the mean endorsement of drug abuse (M = 0.08, SD = 0.16), and alcohol abuse (M = 0.77, SD = 0.62) was low in our sample with most student veterans not meeting criteria for substance abuse. Domestic violence myth adherence (M = 2.59, SD = 0.60) was also low in our overall sample, with findings directly comparable with other studies of college populations (Carr & Vandeusen, 2002; Jakupcak et al., 2013; Peters, 2008). Furthermore, 29% endorsed at least some agreement with highly hypermasculine attitudes. Outside of their partnered relationships, more than one third of veterans reported feeling lonely (38%), and having low social support (34%), and more than one fourth (26%) indicated that they had no close friends.
Based on the BSI (Derogatis & Melisaratos, 1983), the majority of veterans in the current study did not meet clinical criteria for psychological disorders such as depression, generalized, anxiety, and panic disorder. However, despite the fact that most participants endorsed no to moderate overall levels of distress, substance abuse, and domestic violence myth adherence, item analysis revealed a variety of specific concerns. For example, a noteworthy number of veterans reported experiencing “some” to “a huge amount” of symptoms of depression: 65%, worrying too much about things; 51%, low energy or feeling slowed down; 43%, blaming self for things; 39%, feeling blue; 39%, loss of interest in things and symptoms of anxiety—34%, scary thoughts and images; 31%, nervousness or shakiness; and 29%, feeling trapped or caught. These findings are striking in comparison with research that suggests that 13.8% of non-veteran male college students have been found to experience depression (Eisenberg, Gollust, Golberstein, & Hefner, 2007), and only 2.4% of male college students have been found to experience generalized anxiety disorder or panic disorder.
In addition, more than half (55%) of the veterans in the current sample reported feeling “moderate” to “huge amounts of anger,” a symptom believed to be a common strain for OIF/OEF veterans (Demers, 2008; Harmon et al., 2012). Also, of concern is that rates of substance use for our sample were even higher than rates expected for samples of veterans with 36% meeting criteria for alcohol use disorder (scoring an 8 or higher on the 10 items of the AUDIT), 11% reporting abuse of prescription drugs, and 27% reporting use of drugs for nonmedical reasons. Of course, substance dependence is age related as well. For example, although the National Survey on Drug Use and Health (SAMHSA, 2007) found that only 7.1% of veterans in the United States met criteria for substance dependence in the past year, 25% of veterans in the 18- to 25-year-old range met criteria for substance use dependence. In studies of overall college samples, 18% of students were found to meet criteria for alcohol dependence and 28% for drug dependence (J. Taylor, James, Bobadilla, & Reeves, 2008).
As predicted, perpetrating violence against a partner was correlated with psychological distress, alcohol abuse, anger, hypermasculinity, and domestic violence myth endorsement. Social support was revealed as a potentially protective factor related to decreased psychological violence.
Regression Analysis
Four hierarchical regression analyses (see Appendix C) were conducted to predict risk factors for relationship aggression in college student veterans. Psychological aggression, low negotiation, domestic violence myth adherence, and anger reactions were examined as risk factors for IPV for the sample of male veterans. In keeping with the existing literature, for all four analyses, psychological distress, alcohol, and drug abuse variables were entered together in the first step as primary factors contributing to likelihood of relationship abuse. Hypermasculinity attitudes were entered as the second step as a factor that would increase the likelihood of relationship aggression in a sample facing strains that compromise relationship coping. Social support was entered in the third and final step, based on findings that high support mitigates the likelihood of intimate abuse.
Psychological aggression
In the hierarchical regression analysis predicting psychological aggression, all three steps were statistically significant at alpha set at .05. The first step containing the symptoms explained 35% of the variability in psychological aggression (R2 = .35, p < .01). However, the only significant predictor from the set of symptoms included in Step 1 was psychological distress (β = .58, p < .01). The finding suggests that the higher the degree of psychological distress, the higher the likelihood of reporting psychological aggressiveness toward his partner.
Hypermasculinity attitudes were entered in the second step and explained an additional 6% of the variance in psychological aggression (β = .29, ΔR2 = .06, p < .01). Higher hypermasculinity attitudes were associated with higher levels of psychological aggression.
Social support, Step 3, explained an additional 6% of the variability above and beyond all the other variables in the model (β = −.28, ΔR2 = .06, p < .01). The beta weight was negative indicating that higher levels of social support were related to lower levels of psychological aggression.
Negotiation tactics
In the hierarchical regression analysis predicting negotiation tactics, the first step was statistically significant at alpha set at .05. The first step containing the symptoms explained 8% of the variability in negotiation tactics (R2 = .08, p < .05). Both psychological distress and alcohol use were significant predictors (β = −.27, β = .22, p < .05, psychological distress and alcohol use, respectively). As expected, the higher the degree of psychological distress, the lower the likelihood of reporting negotiation tactics. However, surprisingly we found that alcohol use was positively related to negotiation tactics.
Hypermasculinity attitudes were entered in the second step and did not explain a significant amount of additional variance (ΔR2 = .03, p > .05), nor did social support (ΔR2 = .03, p > .05). When hypermasculinity and social support were added, psychological distress was no longer statistically significant.
Domestic violence myths
In the hierarchical regression analysis predicting domestic violence myths, two of the three steps were statistically significant at alpha set at .05. The first step containing the symptoms explained 9% of the variability in negotiation tactics (R2 = .09, p < .05). The three variables as a set explained a significant amount of variance in domestic violence myths; however, no individual predictor was statistically significant.
Hypermasculinity attitudes were entered in the second step and explained the most amount of variance (β = .57, ΔR2 = .24, p < .01) suggesting that the male veterans who endorsed hypermasculinity views also endorsed domestic violence myths. Interestingly, when hypermasculinity was entered into the model, drug use became a significant predictor as well. Social support was not a significant predictor (β = −.10, ΔR2 = .01, p > .05).
Anger reactions
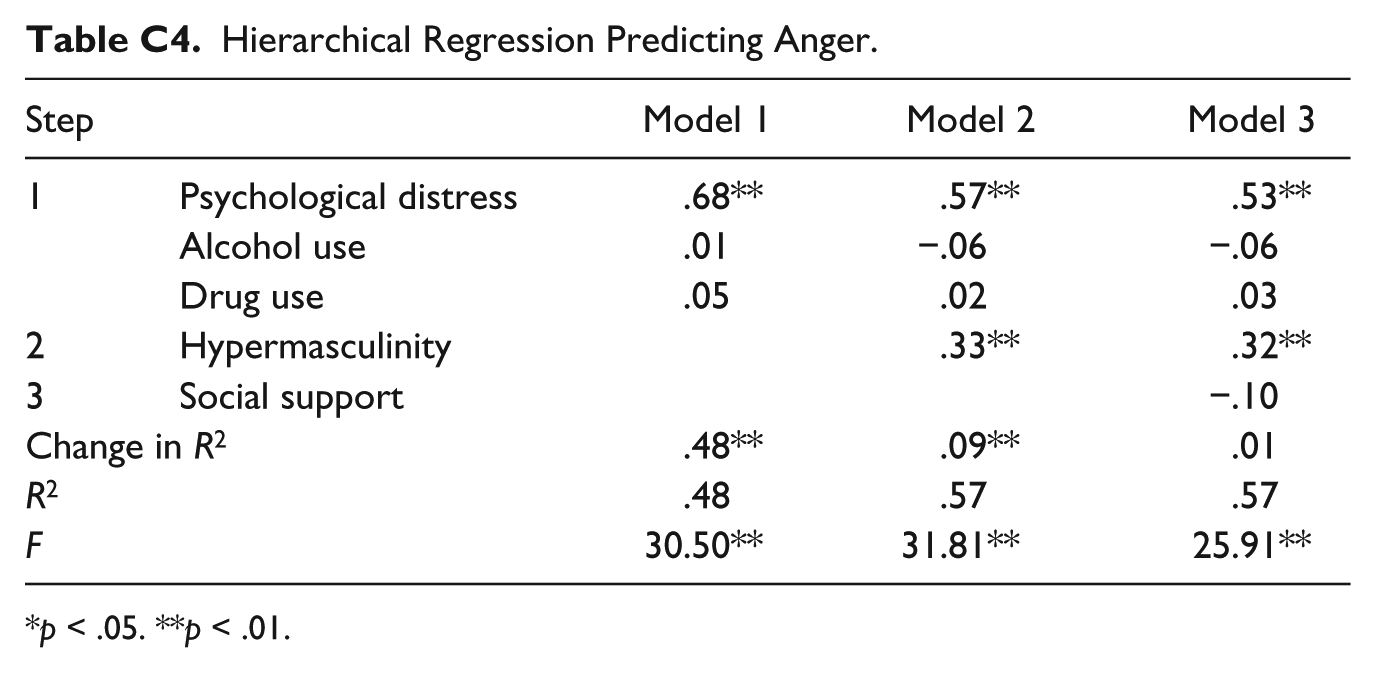
In the hierarchical regression analysis predicting anger reactions, two of the three steps were statistically significant at alpha set at .05. The first step containing the symptoms explained 48% of the variability in anger reactions (R2 = .48, p < .01). However, the only significant predictor from the set of symptoms included in Step 1 was psychological distress (β = .68, p < .01). The finding suggests that the higher the degree of psychological distress, the higher the likelihood of reporting high levels of anger. Hypermasculinity attitudes were entered in the second step and explained an additional 9% of the variability in anger reactions (β = .33, ΔR2 = .09, p < .01) suggesting a positive relationship between hypermasculinity attitudes and anger reactions. Social support was not a significant predictor (β = −.10, ΔR2 = .01, p > .05).
Discussion
It appears that anger, relationship dynamics, and IPV are much more complex for veterans than previously reported. Although mean levels of psychological distress, and substance abuse were not significant among the current group, our sample consists of a higher functioning population of veterans than the non-student veteran population usually studied in that they were all enrolled in college, involved in relationships with a significant other, and both willing and able to complete a lengthy survey. Nevertheless, item analysis revealed that approximately 20% to 30% of this group are highly distressed, abusing alcohol and/or drugs, and at risk of partner abuse. In fact, self-reported rates of moderate IPV among this sample were comparable with rates reported by veterans in other studies, such as 12% versus 11% to 13% found by Heyman and Neidig (1999) in their examination of servicemen randomly sampled from 38 army installations between 1990 and 1994.
Correlational analyses revealed significant relationships between certain variables (See Appendix B), suggesting that rates of IPV may be explained by the negative relationship identified between social support and psychological distress as well as the inverse relationship between distress and using verbal negotiation strategies to handle conflict. Again, although the direction of relationship between the experience of distress, and low social support cannot be determined without longitudinal data, both existing research and current findings reveal that aggression is likely to occur when participants experience high levels of psychological distress, anger, and low levels of social support (Lento-Zwolinski, 2007). Unfortunately, in addition to being highly distressed, one third of respondents in this study reported low levels of social support and feeling lonely, and one fourth reported having no close friends. The results of our correlations support a body of literature that suggests that though social support may reduce anger reactions and aggression (Babcock, Roseman, Green, & Ross, 2008; Barrera et al., 2013; Cohen et al., 2000; Csibi & Csibi., 2011; Pietrzak et al., 2009), a lack of social support places veterans at significant risk of using aggressive strategies instead of verbal negotiation to manage conflict (Barrera et al., 2013; Boscarino, 1995; Cohen et al., 2000; Csibi & Csibi, 2011; Pietrzak et al., 2009). Of course, correlations cannot fully explain rates of IPV; they serve only to quantify the relationships among the variables.
In addition to the direct relationships demonstrated between social support, psychological distress, and psychological aggression, in keeping with previous studies, current results demonstrate a strong positive relationship between psychological distress and anger. Furthermore, our findings reveal that distressed and angry veterans are more likely to endorse hypermasculine attitudes and behaviors, such as condoning both physical fighting and risk tasking. As demonstrated by a growing body of literature, hypermasculinity places men at greater risk of using aggressive strategies to manage interpersonal conflict as opposed to using verbal negotiation tactics. Although findings regarding the effects of military training and culture on veterans’ rates of IPV are inconclusive, it is possible that cultural spillover theory can account for hypermasculinity in the current sample. The unique stressors faced by OIF/OEF veterans (prolonged and repeated deployments with little downtime, lack of clear battle lines) may place this group of veterans at special risk of developing hypermasculine attitudes that translate into relationship aggression on the home front. Our findings are in line with current research on more than 2,000 OIF army combat soldiers that suggests that mental health providers should consider focusing on risky behaviors instead of overall posttraumatic stress response (Harmon et al., 2012).
In summary, there is a reciprocal relationship between social support, psychological distress, anger, and the use of verbal negotiation tactics, which has significant implications for veterans and their loved ones. In keeping with a strong body of literature, based on the correlations found, the more social support a veteran experienced, the less distress he experienced and the more likely it was that he used verbal negotiation tactics in his intimate relationship, and a lower likelihood of using aggression.
Regression analyses may shed light on predicting signs of likelihood of aggression in warriors: High levels of psychological distress and hypermasculine attitudes are significant predictors of anger and psychological aggression. Social support seems to negatively predict psychological aggression, reducing the likelihood of this form of abuse even in the presence of other risk factors. This model suggests that IPV cannot be predicted by anger alone (as hypothesized by Sherman et al., 2006) but may be the result of a much more complex constellation of factors.
It may be that military training and culture play a role in hypermasculine attitudes and anger (as a coping mechanism during combat enabling veterans to suppress feelings of fear or sadness that may put the veteran and his or her comrades at risk), and anger may be related to military separation and transition to civilian culture. The relationship between social support, psychological aggression, and hypermasculinity is also complex, with social support appearing to reduce the likelihood of psychological aggression. It is unknown if anger and/or hypermasculine attitudes prevent the development of strong social support, and each of these areas warrants additional exploration.
Limitations
The findings of this study provide new perspectives on the ways in which mental health problems, hypermasculinity, and low social support increase the likelihood of anger and psychological aggression in a relationship, thus pointing to new directions for further research. However, the small sample size of the current sample posed a significant limitation, as it limited the statistical power of analyses conducted, and restricted both the variability and the range of responses to the items assessed. Other limitations include the sampling framework (online survey) and the design (cross-sectional, which limits our understanding of directionality). In addition, we do not know veterans’ psychological state, substance use, and adherence to hypermasculine attitudes and behaviors prior to service and/or being deployed. To address these limitations, a longitudinal study should be undertaken, along with qualitative examinations (interviews and focus groups) to better understand risk factors for IPV in this population.
Recommendations
Although military services are available to address issues such as IPV, most of the programs are located on military installations and available only to active duty service members and their families (Savitsky et al., 2009). Veterans who have separated from the military can access VA services; however, many veterans may be resistant to seeking diagnosis or treatment due concerns regarding stigma (Hoge et al., 2004). In fact, only 30% of veterans with PTSD or depression were found to seek help from the VA services (Tanielian & Jaycox, 2008). Similarly, the Mental Health Advisory Team (MHAT; 2008) for OIF found that only 40% of veterans who screened positive for serious emotional problems actually sought help from mental health professionals. VA services are also unavailable to veterans who were less than honorably discharged, limiting their access to mental health care. The alarming increase in suicides among veterans, which showed a rise of 26% from 2005 to 2007 (American Psychological Association, n.d.), indicates that comprehensive care for returning warriors is sorely needed (Hoge et al., 2004). At the same time, it is important to note that 80% of veterans, who served in Iraq or Afghanistan, were not found to suffer from either PTSD or depression (RAND, 2008) and a full 93% did not meet criteria for a substance abuse disorder.
In addition, many service providers—both on and off college campuses—are unprepared to deal with the challenges of this returning population, prompting the need for more specific interventions to address skills for successful reintegration, coping, and relationships. The nature of current conflict creates unique challenges for some veterans including PTSD with co-morbid depression and/or substance abuse, difficulties with reintegration into civilian life, and difficulties with intimacy related to feelings of conflicts between military and civilian identities, and cultural disenfranchisement. In light of the fact that veterans are returning to college campuses in record numbers, we must develop ways to meet their psychological and social needs that lie outside the framework of traditional clinical services. Based on our own work reported elsewhere (Klaw, Demers, Barnes & Hrnic, in press), we suggest providing peer support groups for student veterans, along with topical workshops related to both healthy relationships and the transition process. In addition, we suggest that all colleges and universities develop an academic class that orients veterans to college life, explains the transition process and its challenges, and equips student veterans with tools and resources for college and career success. Our findings suggest that to address partner violence, classes and programs offered to college student veterans must enhance social support, address entrenched ideas about masculinity, and provide tools and resources for student veterans to cope with feelings of anxiety, depression, and isolation. In sum, a culturally tailored approach that emphasizes prevention, community outreach, and the institutionalization of community support services is essential for reaching all individuals who have served our country.
Footnotes
Appendix A
Appendix B
Descriptive Statistics and Bivariate Correlations.

| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Psychological distress | 1.06 | .89 | ||||||||
| 2. Alcohol use | .77 | .62 | .35** | |||||||
| 3. Drug use | .08 | .16 | .13 | .23* | ||||||
| 4. Hypermasculinity | 2.62 | .67 | .44** | .34** | .18 | |||||
| 5. Social support | 1.08 | .44 | −.44** | −.13 | .02 | −.26* | ||||
| 6. Psychological aggression | .66 | .63 | .59** | .23* | .09 | .48** | −.51** | |||
| 7. Negotiation tactics | 2.08 | .87 | −.21* | .13 | .03 | −.20* | .28** | −.09 | ||
| 8. DV myths | 2.59 | .60 | .22* | .21* | −.13 | .54** | −.21* | .33** | −.05 | |
| 9. Anger reactions | 1.33 | 1.08 | .69** | .26** | .14 | .59** | −.42** | .62** | −.10 | .33** |
Note. DV = domestic violence.
p < .05. **p < .01.
Appendix C
Hierarchical Regression Predicting Anger.
| Step | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|
| 1 | Psychological distress | .68** | .57** | .53** |
| Alcohol use | .01 | −.06 | −.06 | |
| Drug use | .05 | .02 | .03 | |
| 2 | Hypermasculinity | .33** | .32** | |
| 3 | Social support | −.10 | ||
| Change in R2 | .48** | .09** | .01 | |
| R 2 | .48 | .57 | .57 | |
| F | 30.50** | 31.81** | 25.91** | |
p < .05. **p < .01.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Blue Shield of California Foundation.