
Abstract
A marital status of divorced or separated, as opposed to married, predicts increased risk of health problems, but not for all persons. Focusing on one established health risk that has been linked with divorce—poor subjective sleep quality—the present cross-sectional study examined whether a history of physical intimate partner victimization (IPV) helps identify divorced women at potentially greater risk of health problems. Community midlife women with divorce histories, all of whom were free of current IPV, reported on their past month sleep quality and lifetime IPV. The predicted odds of poor sleep quality were significantly greater for women with, versus without, IPV histories. This held after adjusting for socioemotional, medical, or sociodemographic risks. A dose–response relationship between IPV chronicity and poor quality sleep was observed. IPV history may help identify divorced women at increased risk of poor quality sleep and, more broadly, poor health.
A marital status of divorced or separated, as opposed to married, prospectively predicts increased risk of early mortality from a variety of causes (Sbarra, Law, & Portley, 2011). It also predicts increased risk of physical morbidity, such as cerebrovascular diseases (Engström et al., 2004). However, health does not suffer for all persons with divorce histories. Thus, factors contributing to this heterogeneity require identification (Sbarra et al., 2011).
Along these lines, it is interesting that research on marital status and physical health has not been widely informed by research on intimate partner victimization (IPV), even though marital status and IPV are linked. In nationally representative samples and other large-scale survey samples, the 12-month prevalence, or average annual rate, of physical or sexual IPV is greater among women who are divorced or separated, compared with those who are married (Brownridge et al., 2008; Harlow, 1991; Vest, Catlin, Chen, & Brownson, 2002). This raises the question of whether IPV history may be contributing to the observed associations between divorce and health, especially given that health problems have been linked to IPV (Coker et al., 2002).
The present article considers this by focusing on one specific health-risk behavior: subjective, or self-reported, sleep quality. Subjective qualities of sleep, particularly qualities characteristic of insomnia, prospectively predict negative health outcomes, such as cardiovascular morbidity and mortality (Sofi et al., 2014). Furthermore, they are hypothesized to be one mechanism connecting divorce with poorer health (Sbarra et al., 2011). Being divorced/separated, compared with married, is correlated with poorer subjective sleep quality (e.g., Doi, Minowa, Okawa, & Uchiyama, 2000; Grandner et al., 2010). Also, divorce prospectively predicts new-onset sleep difficulties that persist for several years beyond the acute aftermath of this stressful life event (Vahtera et al., 2007). Given its relatively greater prevalence among divorced persons, it seems logical to ask whether IPV history contributes to the poor sleep quality that accompanies divorce. Sleep problems have been documented among battered women residing in shelters (Humphreys & Lee, 2005) and among women filing for protective orders (Walker, Shannon, & Logan, 2011), but little is known about them after such acute crises resolve.
To address this, the present cross-sectional study evaluated whether a history of physical IPV predicts poor subjective sleep quality in midlife women with histories of divorce or separation (see Figure 1). We were particularly interested in predicting levels of poor sleep quality indicative of clinically significant sleep problems because such problems are relevant for physical health, the broader topic motivating this research (Sofi et al., 2014). Therefore, using the Pittsburgh Sleep Quality Inventory, subjective sleep quality was classified as either good or poor based on a widely used cut-score for identifying sleep disturbances likely to be clinically significant (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). We focused on physical IPV because only a portion of women in our sample reported such a history (whereas all reported psychological IPV), making it well-suited to address our research question. Also, less prevalent IPV types (e.g., sexual IPV, stalking) typically accompany physical IPV, making the latter a good general indicator of victimization when the number of predictors must be limited for statistical considerations.
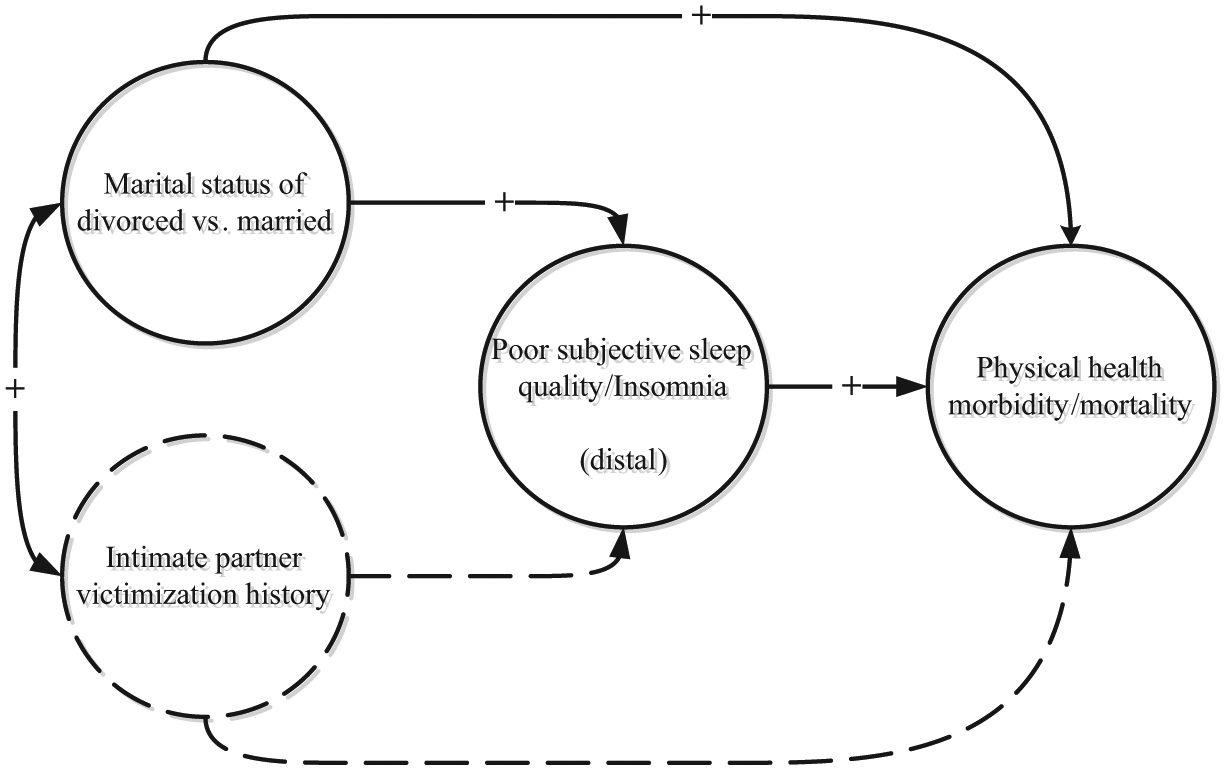
Hypothesized role of IPV in connections among marital status, sleep quality, and physical health.
Our first question concerned incremental validity, or whether physical IPV history predicts poor sleep quality over and above other life stressors that are known to predict poor sleep: distal experiences of childhood trauma (Greenfield, Lee, Friedman, & Springer, 2011) and recent stressful life events independent of, or unlikely to follow from, IPV (LeBlanc et al., 2009). After establishing the incremental validity of IPV history for poor sleep quality, our second question concerned potential explanations for this association. Three separate, conceptually organized explanatory models were evaluated. The socioemotional model tested the roles of current symptoms of depression and posttraumatic stress; sleep disruptions are apparent in both disorders, and both have been connected with IPV history (Ehrensaft, Moffitt, & Caspi, 2006). This model also included recent stressful life events judged to be dependent on, or likely to follow from, IPV or its aftermath (e.g., a period of homelessness). The medical model tested the roles of activity-limiting physical health problems, alcohol consumption, and smoking status, each of which has been associated with disruptions in sleep quality (Blumel et al., 2012; Brook, Rubenstone, Zhang, & Brook, 2012; Foley, Ancoli-Israel, Britz, & Walsh, 2004), and with IPV (Coker et al., 2002; Crane, Hawes, & Weinberger, 2013; Devries et al., 2014). The sociodemographic model tested the roles of current marital status, current annual household income, and number of times divorced. Current marital and financial status have been linked to sleep problems (Grandner et al., 2010; Moore, Adler, Williams, & Jackson, 2002), and IPV history could be reasonably be expected to be related to both. Lifetime history of marital transitions has received increasing emphasis in studies of divorce and health (Hughes & Waite, 2009), and could be particularly relevant in the present study given that women rated their cumulative lifetime IPV. Finally, because vasomotor symptoms contribute to sleep disruption among midlife women (Kravitz et al., 2008), each model was adjusted a priori using a proxy indicator for risk of vasomotor symptoms.
Method
Recruitment and Sample Selection
Using community advertisements and mailings, physically healthy women with histories of divorce or separation from a stressful relationship were recruited as part of a larger investigation of stress and aging in midlife women (Newton et al., 2011). The content of recruitment materials was varied (i.e., “stressful relationship,” “extremely stressful relationship,” or “upsetting thoughts or unwanted memories of a past stressful relationship”) to recruit women with and without IPV, and to include a range of IPV severity. A telephone interview assessed initial eligibility: English language ability, history of divorce or permanent separation, no ongoing divorce-related legal issues, no recent psychiatric hospitalization, no IPV from an ex-partner in the past year, and—if re-partnered—no lifetime IPV by this partner. For determining initial eligibility, IPV was identified by a cut-score of ≥ 1 on a three-item screener; this yields sensitivities and specificities of 94% and 75%, respectively, for detecting lifetime IPV (Paranjape & Jane, 2003), and 95% and 37%, respectively, for detecting past-year IPV (Paranjape, Rask, & Liebschutz, 2006).
Women meeting all initial eligibility criteria were screened for biomedical eligibility: postmenopausal, no chronic medical conditions, no probable alcohol use disorder, and no current use of street drugs or prescription or over-the-counter medications with inflammatory effects. Postmenopausal status was established using the Women’s Ischemia Syndrome Evaluation (WISE) algorithm, and probable alcohol use disorders were assessed with a screener derived from the Alcohol Use Disorders Identification Test (AUDIT-C); both measures are described below. Women were invited to participate in the laboratory phase of the study if they met all biomedical criteria, or in the questionnaire-only phase if they did not. The present report combines questionnaire data from women who participated in either study phase.
Of the 577 callers, 118 did not meet initial eligibility criteria; 246 were uninterested or unable to participate, or lost to contact; and 14 were enrolled in the laboratory phase but were discontinued on additional evaluation of biomedical criteria. The remaining 199 women completed the study. The present report excludes women with missing data for subjective sleep quality (n = 16; any missing item resulted in missing data for the global score) and for predictors included in any of the logistic regression models (IPV history, n = 1; years postmenopausal, n = 7; posttraumatic stress symptoms, n = 1; annual income, n = 3; alcohol use, n = 1). This yielded a sample size of 170 women (n = 61, laboratory phase; n = 109, questionnaire-only phase).
Measures
Women in both study phases completed the following measures. Depression symptoms were assessed via face-to-face interviews. All other measures were completed via computerized self-administration.
Sociodemographics
Women reported their date of birth, ethnicity, highest level of education obtained, employment status, current marital status, years divorced, and number of times divorced. For women employed full- or part-time, work schedule (i.e., day, second, night, or rotating shifts) was assessed and recoded to day shift or other than day shift. Annual household income, assessed using six categories in increments of US$19,999.00 (1 = less than US$20,000.00; 6 = more than US$100,000.00), was recoded to 0 (<US$40,000.00) or 1 (≥US$40,000.00) to guard against sparseness in logistic regression models (Cohen, Cohen, West, & Aiken, 2003). This coding identified incomes less than, or approaching/exceeding, the local median annual household income per U.S. census data.
Health-related characteristics
Postmenopausal status was established using the WISE algorithm, which considers age, menstrual history, and surgical history (Johnson et al., 2004). Compared with other self-report methods, this algorithm improves menopausal status classification as judged against expert opinion. Because the laboratory phase included a blood draw, we were able to biologically confirm postmenopausal status for women who participated in this study phase (i.e., follicle-stimulating hormone levels ≥ 25 mIU/mL).
Number of years postmenopausal was calculated from retrospectively reported date of final menstrual period and was recoded to 1 (<5 years) or 0 (≥5 years). This classification identifies the point (5 years postmenopause) at which bothersome vasomotor symptoms (VMS; for example, hot flashes) decrease by 50% from their most prevalent (Politi, Schleinitz, & Col, 2008). It was used to quantify risk (0 = lower, 1 = higher) for potentially sleep-disrupting VMS (Kravitz et al., 2008).
Three questions from the AUDIT-C assessed alcohol consumption in the past year (Dawson, Grant, Stinson, & Zhou, 2005; values assigned to each response category are shown in parentheses): frequency of drinking, frequency of drinking five or more drinks—never (0), 1 to 2 times/year (1), 3 to 6 times/year (1), 7 to 11 times/year (1), once a month (2), 2 to 3 times/month (2), once a week (2), 2 times/week (3), 3 to 4 times/week (3), nearly every day (4), every day (4); number of alcoholic beverages typically consumed on drinking days—1 or 2 drinks (0), 3 or 4 drinks (1), 5 or 6 drinks (2), 7 or 9 drinks (3), or 10 or more drinks (4). Scores for the three items were summed. A cut-score of ≥5 yields sensitivities ≥71.8% and specificities ≥88.0% for identifying alcohol dependence, alcohol use disorders, and risk drinking in adult women (Dawson et al., 2005). The present study combines AUDIT-C scores from the phone interview (for women in the laboratory phase) and from the research visit (for women in the questionnaire-only phase).
Two items from the Centers for Disease Control and Prevention Health-Related Quality-of-Life measure determined the presence (0 = no, 1 = yes) of activity-limiting physical health problems (e.g., arthritis, back or neck problem, diabetes; Moriarty, Zack, & Kobau, 2003). Four items assessed smoking status: never smoked; smoked just to try it; regular smoker in the past, but no longer; and smoke regularly now, at least once a month (Chassin, Presson, Sherman, & Kim, 2003). Smoking status was classified as never smoker/trier/former regular smoker (0) versus current regular smoker (1).
Subjective sleep quality
The Pittsburgh Sleep Quality Index (PSQI), a 19-item self-report measure, assessed past month sleep quality (Cronbach’s α = .79). Global scores range from 0 to 21, with higher scores indicating poorer quality sleep. Sleep quality was classified as either good (PSQI global score ≤ 5, coded as 0) or poor (PSQI global score > 5, coded as 1). This widely used classification yields excellent sensitivity and specificity for differentiating healthy controls from persons with disturbed sleep due to primary sleep disorders such or insomnia, or depression (Buysse et al., 1989).
Intimate partner victimization
The 12-item physical assault subscale of the revised Conflict Tactics Scale (Straus, Hamby, & Warren, 2003) assessed histories of physical IPV. Items assess minor (e.g., pushed or shoved by partner) and severe (e.g., choked by my partner) physical assaults. For each item, women rated frequency (never, once, twice, 3-5 times, 6-10 times, 11-20 times, more than 20 times) with respect to all prior intimate relationships, collectively. Using standard procedures, frequency ratings were assigned values of 0, 1, 2, 4, 8, 15, and 25, respectively. These values were summed across the 12 items to form an IPV chronicity score. Also, IPV history was classified as either absent (chronicity scores of 0) or present (chronicity scores ≥ 1, coded as 1).
Other life stressors
Childhood trauma was assessed by counting the number of potentially injurious or life-threatening events that occurred before age 18: serious accident, traumatic loss of a family member, forcible rape (up to three incidents), completed sexual molestation (up to two incidents), attempted sexual molestation (up to two incidents), physical attack (up to two incidents), or any other extraordinarily stressful life event (Resnick, 1996).
Using a 48-item checklist (Spurgeon, Jackson, & Beach, 2001), women identified stressful life events that occurred during the past year. Two raters assessed the IPV dependence (yes/no) of each event to differentiate stressful events likely to be dependent on IPV (i.e., likely to be caused by IPV, or observed during its aftermath, such as a period of homelessness) from those likely to be independent of IPV (i.e., unlikely to be caused by it, such as partner starts or stops working). The kappa coefficient (0.59) reflected moderate agreement beyond chance (Landis & Koch, 1977). After resolving disagreements by discussion, 30 IPV-dependent and 14 IPV-independent events were identified (four events were not endorsed by any participant). Each event measure was scored by counting the number of events that occurred during the past year.
Psychological symptoms
The Patient Health Questionnaire 9-item depression module assessed frequency of each of the nine Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) depression symptoms in the past 2 weeks (0 = not at all, 3 = nearly every day; Kroenke, Spitzer, & Williams, 2001). The present study focused on the two-item short-form (Kroenke, Spitzer, & Williams, 2003). The short-form has good construct validity, and good diagnostic sensitivity (.83) and specificity (.90), and omits sleep-related items that could produce criterion contamination when predicting sleep quality. A depression symptom severity score was calculated by summing ratings for both items (Cronbach’s α = .74). Probable syndromal depression was identified using the recommended cut-score of ≥3.
The Posttraumatic Stress Disorder Checklist–Civilian version assessed severity of each of the 17 DSM-IV symptoms in the past month (1 = not at all, 5 = extremely; Weathers, Litz, Herman, Huska, & Keane, 1993). The present study focused on the six-item short-form (Lang & Stein, 2005). The short-form accounts for the majority of the variance in the full 17-item measure, shows good diagnostic sensitivity (.80-.92) and specificity (.72-.76), and omits sleep-related items that could produce criterion contamination when predicting sleep quality. A symptom severity score was calculated by summing ratings for all six items (Cronbach’s α = .84). Probable syndromal posttraumatic stress disorder (PTSD) was identified using the recommended cut-score of ≥14.
Analytic Strategy
Person-mean imputation was used to replace missing values on scale items, as appropriate, when ≤20% of items were missing; when more items were missing, the scale score was coded as missing. For descriptive statistics, median and interquartile range (IQR) are presented because most continuous variables were significantly skewed. Univariate associations between sleep quality classification and categorical variables were analyzed by chi-square tests, or Fisher’s exact tests when cell counts were low. Univariate associations between sleep quality classification and continuous variables were analyzed with independent-samples t tests, or non-parametric Wilcoxon rank-sum tests for skewed variables. Logistic regression was used to model the presence (n = 98) versus absence (n = 72) of poor sleep quality in the past month. A series of conceptually organized models was tested to maintain a reasonable ratio of predictors to cases, where n = 72 was used as the limiting sample size (Babyak, 2004). Bonferroni corrections were not applied because they increase Type II error rate.
Results
Sample Characteristics
Women in this study were midlife, most self-identified as European American/White, about one half had obtained at least a college degree, and about three quarters were employed (see Table 1). Fewer than one half reported annual household incomes that approached or exceeded the median local income. Most women were unmarried. The median number of divorces was two, and the median time post-divorce was 8.5 years. About 20% of women reported the presence of an activity-limiting physical health problem, and about 12% were current smokers. The median alcohol consumption score was 1; 11 (6.32%) women met or exceeded the cut-score of 5 that identifies a probable alcohol use disorder. About one third of the women were high risk for vasomotor symptoms (i.e., within the first 5 years of menopause), with the median time postmenopausal being 6.5 years.
Descriptive Statistics (Median [IQR] or % of Group [n]) by Sleep Quality Classification and for Total Sample.
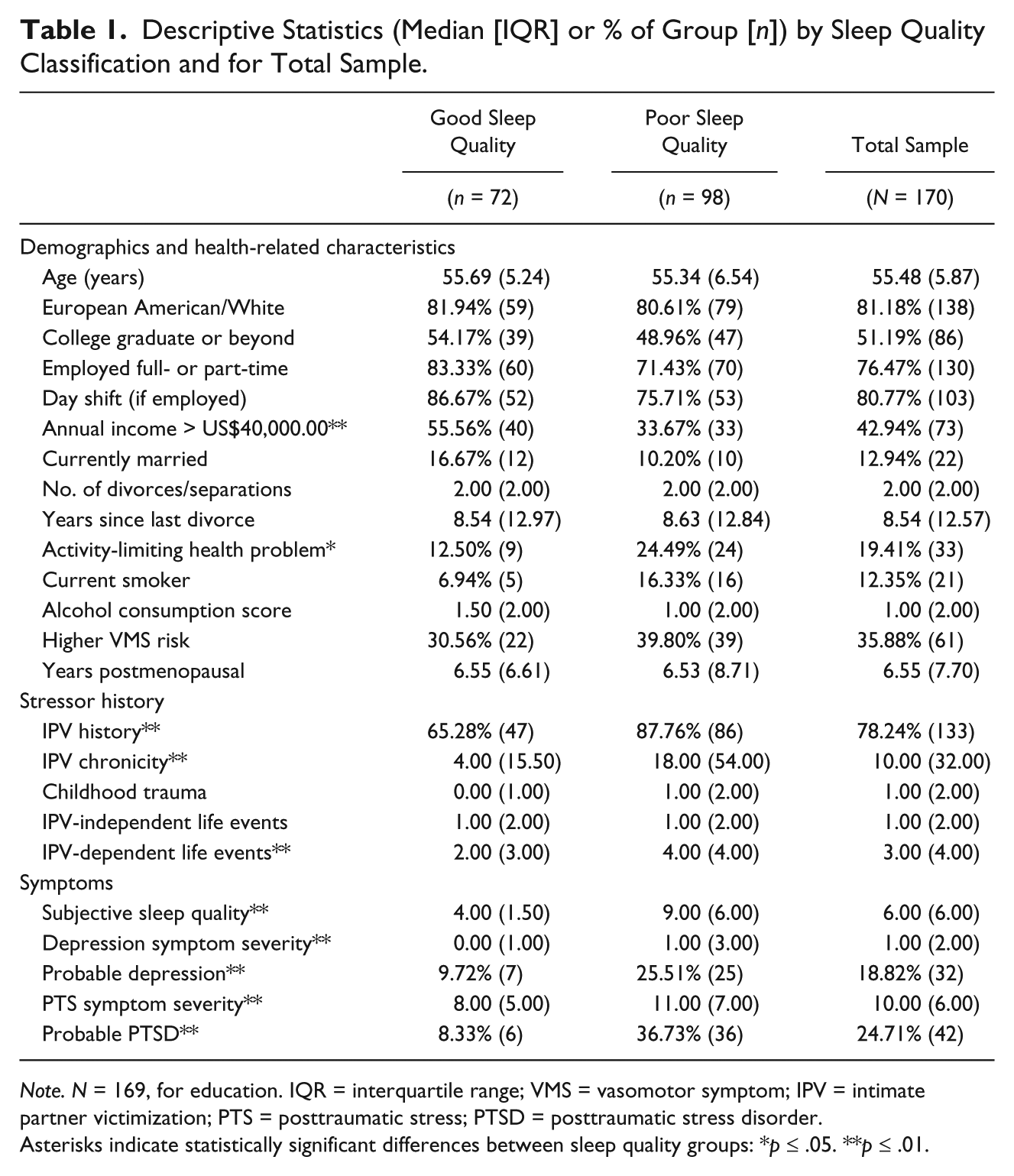
Note. N = 169, for education. IQR = interquartile range; VMS = vasomotor symptom; IPV = intimate partner victimization; PTS = posttraumatic stress; PTSD = posttraumatic stress disorder.
Asterisks indicate statistically significant differences between sleep quality groups: *p ≤ .05. **p ≤ .01.
About three quarters of the sample reported a history of IPV, defined as any occurrence of physical assault by a current or former intimate partner. The median IPV chronicity score approached the mean score reported in a comparison study of community women (Calvete, Corral, & Estevez, 2007). However, this comparison study assessed IPV during 1 year, and excluded women without IPV histories (i.e., those with a chronicity score of “0”) when calculating the chronicity score for the sample. The median number of childhood traumatic events was 1. Women reported a median of one IPV-independent and three IPV-dependent life events during the past year.
The median PSQI global score was 6, 1 point above the median for a sample of midlife community women entering the menopausal transition (Matthews et al., 2010). Probable syndromal depression or PTSD characterized roughly 19% or 25% of the sample, respectively.
There were several statistically significant differences between women with good versus poor subjective sleep quality. Compared with women with good sleep quality, those with poor sleep quality were less likely to report an annual household income nearing or exceeding the local median, and they were more likely to report an activity-limiting physical health problem, and a history of IPV. They also reported greater chronicity of IPV, more IPV-dependent stressful life events, and more severe symptoms of depression and posttraumatic stress, and were more likely to meet criteria for probable syndromal depression and PTSD.
IPV History and Subjective Sleep Quality Classification
Logistic regression was used to evaluate associations between IPV history and sleep quality classification. Table 2 presents the correlation matrix for all variables in these models.
Correlations Among Primary Model Variables.
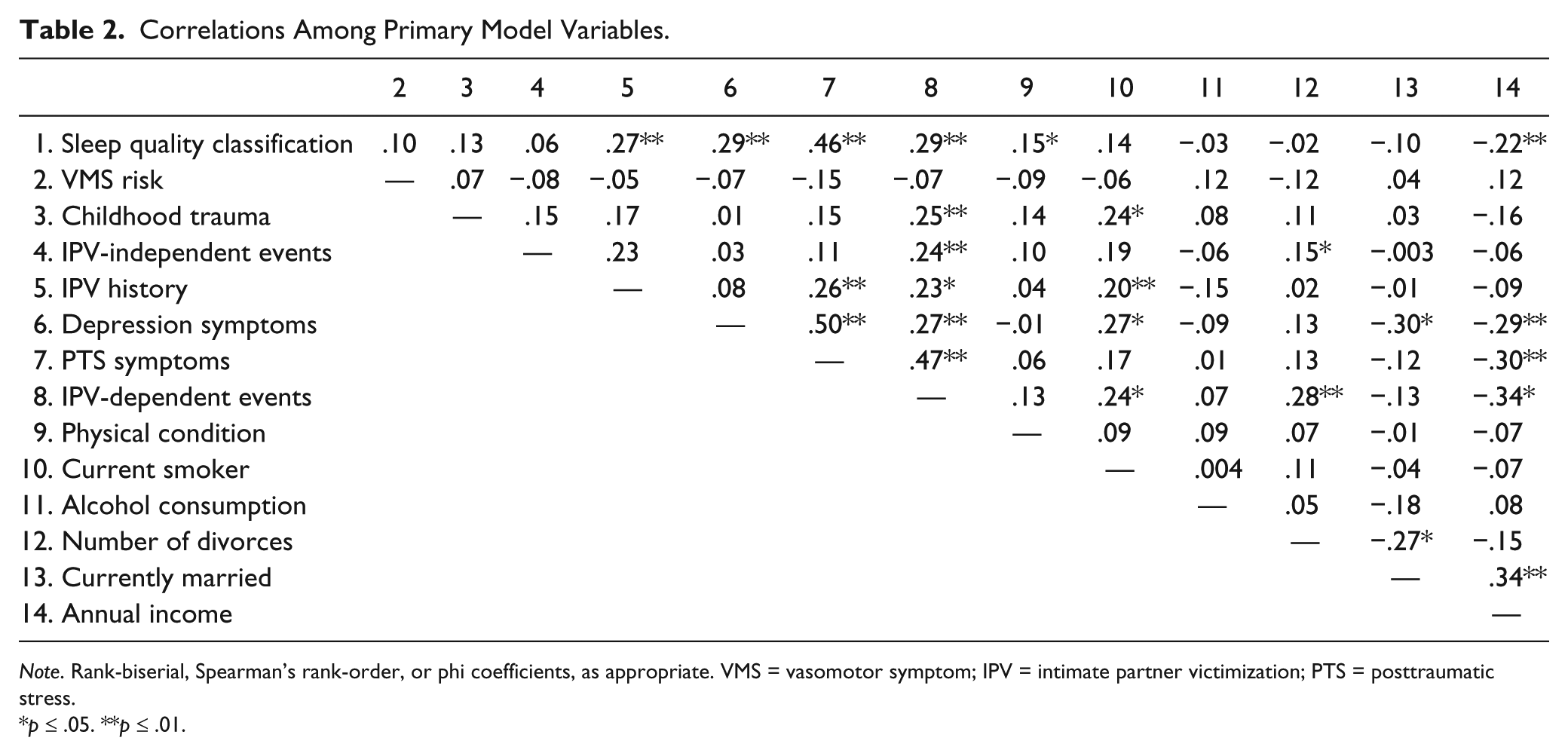
Note. Rank-biserial, Spearman’s rank-order, or phi coefficients, as appropriate. VMS = vasomotor symptom; IPV = intimate partner victimization; PTS = posttraumatic stress.
p ≤ .05. **p ≤ .01.
Incremental validity model
The first aim was to evaluate whether IPV history contributed to poor sleep quality over and above distal experiences of childhood trauma, and recent stressful life events classified as IPV- independent. Results are shown in Table 3. For Step 1, the test for the change in likelihood ratio (ΔLR) did not reach statistical significance, indicating that childhood trauma, recent stressful life events, and VMS risk did not collectively contribute to the prediction of poor sleep quality. Similarly, when considered individually, none of these three predictors reached statistical significance. For Step 2, in contrast, the ΔLR reached statistical significance, indicating that IPV history contributed significantly to the prediction of poor sleep quality. The predicted odds of poor sleep quality for women with a history of IPV were 3.68 times the odds for women with no IPV history, after adjusting for childhood trauma, recent stressful life events, and VMS risk.
Predicting Poor Sleep Quality: Incremental Validity of IPV History (N = 170).
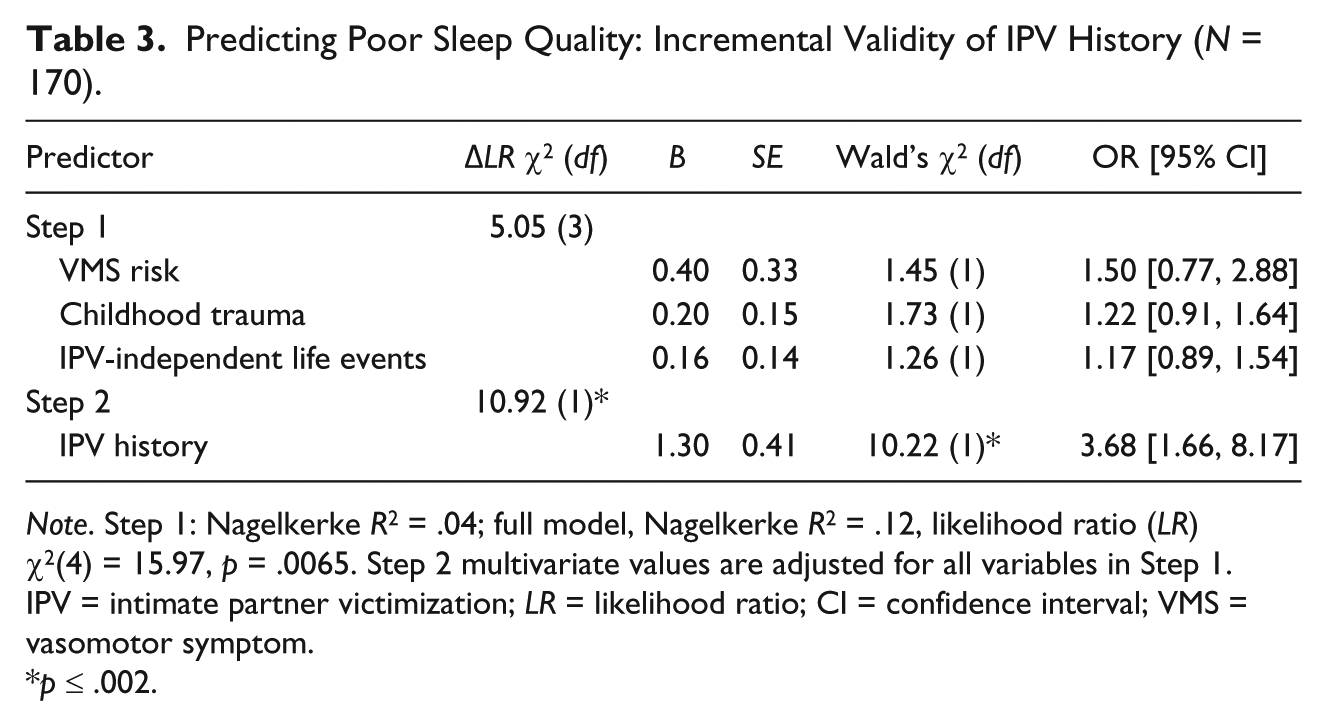
Note. Step 1: Nagelkerke R2 = .04; full model, Nagelkerke R2 = .12, likelihood ratio (LR) χ2(4) = 15.97, p = .0065. Step 2 multivariate values are adjusted for all variables in Step 1. IPV = intimate partner victimization; LR = likelihood ratio; CI = confidence interval; VMS = vasomotor symptom.
p ≤ .002.
Explanatory models
The second aim was to evaluate factors that might account for the observed association between IPV history and poor subjective sleep quality. Three models, each testing a separate set of conceptually organized variables—socioemotional, medical, or sociodemographic—were evaluated. For each model, the contribution of each set of explanatory variables to the prediction of poor sleep quality was evaluated by comparing the likelihood ratio for the model against that of a base model that included only IPV history and VMS risk as predictors. Then, to evaluate whether the explanatory variables accounted for the relationship between IPV history and poor sleep quality, results for IPV history as an individual predictor were compared across the explanatory and base models. Results are shown in Table 4.
IPV History and Sleep Quality: Psychosocial, Medical, and Sociodemographic Explanatory Models (N = 170).
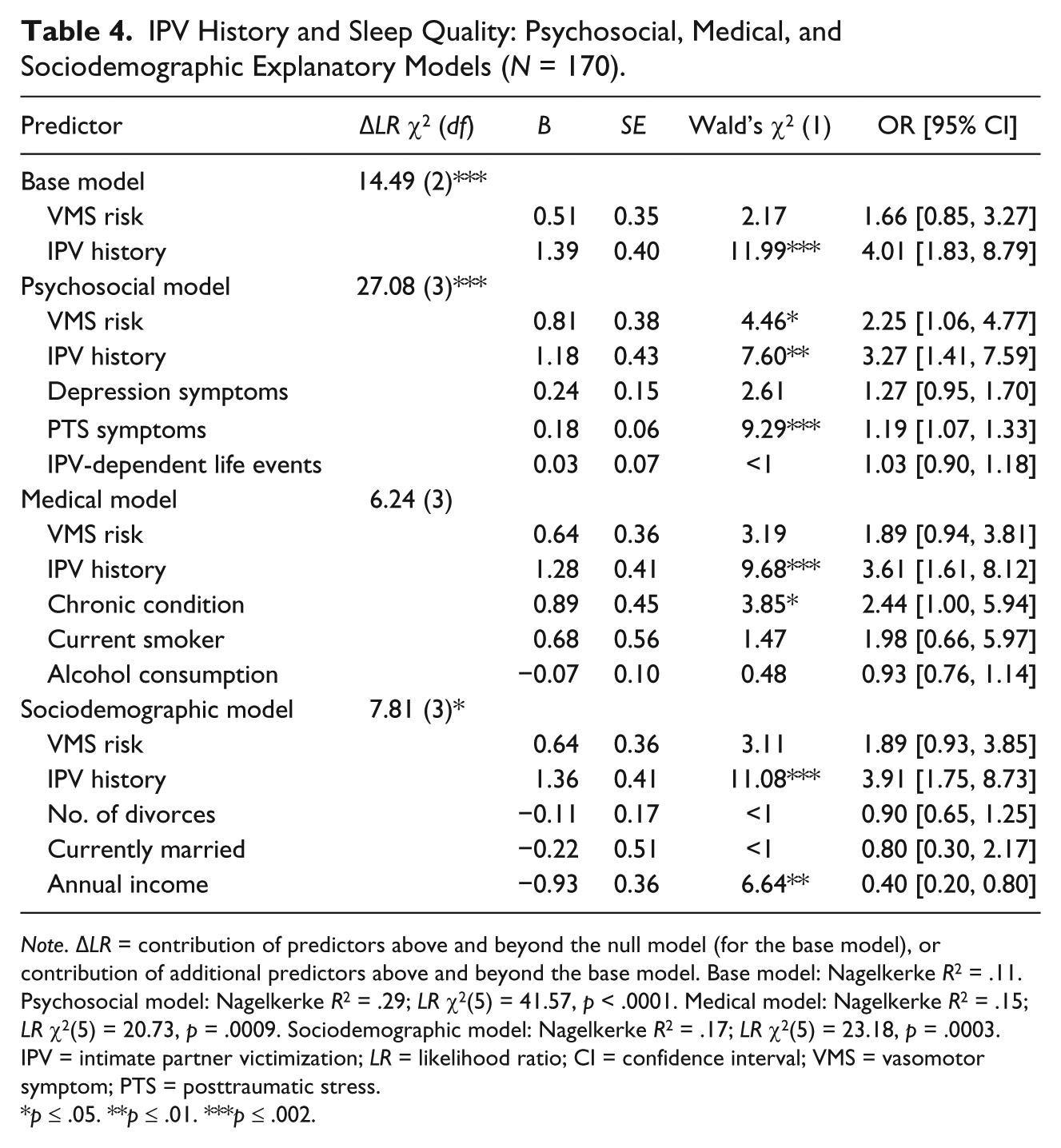
Note. ΔLR = contribution of predictors above and beyond the null model (for the base model), or contribution of additional predictors above and beyond the base model. Base model: Nagelkerke R2 = .11. Psychosocial model: Nagelkerke R2 = .29; LR χ2(5) = 41.57, p < .0001. Medical model: Nagelkerke R2 = .15; LR χ2(5) = 20.73, p = .0009. Sociodemographic model: Nagelkerke R2 = .17; LR χ2(5) = 23.18, p = .0003. IPV = intimate partner victimization; LR = likelihood ratio; CI = confidence interval; VMS = vasomotor symptom; PTS = posttraumatic stress.
p ≤ .05. **p ≤ .01. ***p ≤ .002.
The ΔLR for the base model was statistically significant, indicating that VMS risk and IPV history as a set contributed to the prediction of poor sleep quality. As individual predictors, only IPV history reached statistical significance; the predicted odds of poor sleep quality for women with an IPV history were 4.01 times the odds for women without an IPV history.
For the socioemotional model, the set of three predictors—depression symptoms, posttraumatic stress symptoms, and IPV-dependent stressful life events—contributed significantly to the prediction of poor quality sleep over and above VMS risk and IPV history, as shown by the statistically significant ΔLR. As individual predictors, only posttraumatic stress symptoms reached statistical significance. A 1-point increase in posttraumatic stress symptom severity was associated with a 19% increase in the predicted odds of poor sleep. Also, in this model VMS risk was a statistically significantly predictor; the predicted odds of poor sleep quality for women in the early postmenopausal phase, when VMS risk is greater, were 2.25 times the odds for women in the late postmenopausal phase. After adjusting for the three socioemotional factors, IPV history remained a statistically significant predictor of poor sleep quality, with some reduction in predicted odds compared with those from the base model.
For the medical model, the set of three predictors—activity-limiting physical health problem, current smoker, alcohol consumption score—did not contribute significantly to the prediction of poor sleep quality over and above the base model. Individually, however, the presence of an activity-limiting physical health problem was a statistically significant predictor. The predicted odds of poor sleep quality for women with such a problem were 2.44 times the odds for women without such a condition. In the medical model, IPV history remained a statistically significant predictor of poor sleep quality, with some reduction in predicted odds compared with those from the base model.
For the sociodemographic model, the set of three predictors—number of divorces, current marital status, and annual income category—contributed significantly to the prediction of poor sleep quality over and above the base model. The only statistically significant individual predictor was annual income; having an annual household income approaching or exceeding the local median income, compared with one below the local median, was associated with a 60% decrease in the predicted odds of poor sleep quality. In the sociodemographic model, IPV history remained a statistically significant predictor of poor quality sleep.
Dose–response relationship
To further characterize the relationship between IPV history and poor sleep quality, a dose–response relationship was evaluated. To cast this analysis in a meaningful context, IPV chronicity scores were classified according to published scores for community women and help-seeking women receiving services for victims of violence (Calvete et al., 2007). This yielded a four-level IPV chronicity score: no IPV history (n = 37, coded 0 or referent), IPV chronicity at or below the mean for community women (chronicity scores < 12; n = 54, coded 1), IPV chronicity between the means for community and help-seeking women (chronicity scores from 12 to 65; n = 50, coded 2), IPV chronicity at or above the mean for help-seeking women (chronicity scores ≥ 66; n = 29, coded 3).
This four-level IPV chronicity score was entered as a continuous predictor of poor subjective sleep quality in two logistic regression models. In the first model, after adjusting for VMS risk in Step 1, ΔLR χ2(1) = 1.55, p = .21, IPV chronicity entered in Step 2 made a statistically significant contribution to the predicted odds of poor sleep quality, ΔLR χ2(1) = 14.18, p ≤ .001; odds ratio (OR) = 1.84, 95% CIs [1.32, 2.56]. This full model was re-run with IPV chronicity entered as a classification variable to generate adjusted odds ratios for each level of chronicity. These values are plotted in Figure 2a, which depicts the statistically significant dose–response relationship between IPV chronicity and predicted odds of poor subjective sleep quality.
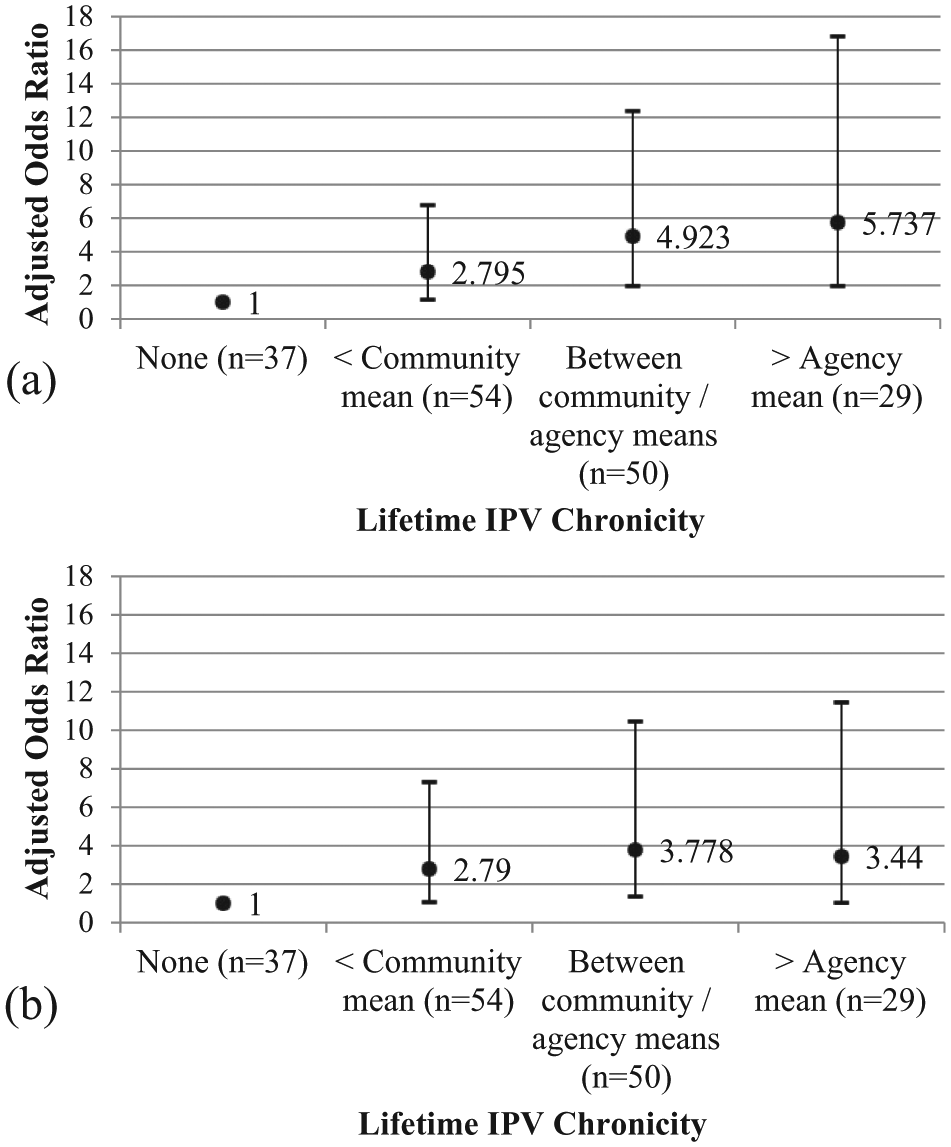
Relationship between lifetime IPV chronicity and predicted odds of poor subjective sleep quality. (a) Model is adjusted for vasomotor symptom risk. (b) Model is adjusted for vasomotor symptom risk, posttraumatic stress symptom severity, presence of activity-limiting physical condition, and annual income.
In the second logistic regression model, VMS risk and the three predictors that emerged as statistically significant in at least one of the explanatory models—posttraumatic stress symptoms, presence of an activity-limiting physical health problem, and annual income—were entered in Step 1. As expected, this variable set made a statistically significant contribution to the predicted odds of poor sleep quality, ΔLR χ2(4) = 38.73, p < .0001, as did each of the individual predictors (OR [95% CI]): VMS risk (2.49 [1.15, 5.20]), PTS symptom severity (1.25 [1.13, 1.38]), presence of an activity-limiting physical health problem (2.59 [1.02, 6.61]), and annual income (0.49 [0.25, 0.997]). When entered in Step 2, the continuous four-level IPV chronicity score made a statistically significant contribution to the predicted odds of poor sleep quality over and above the variables in Step 1, ΔLR χ2(1) = 5.67, p < .05, OR = 1.55, 95% CI [1.07, 2.23]. All Step 1 predictors retained statistical significance except annual income (p < .07). The full model was re-run with IPV chronicity entered as a classification variable to generate adjusted odds ratios for each level of chronicity. As shown in Figure 2b, the additional covariates attenuated the dose–response relationship between IPV history and sleep quality at the highest level of IPV chronicity, somewhat at the middle level of chronicity, but not at the lowest level of chronicity.
Discussion
Sleep problems have been documented among women with IPV histories but primarily during times of acute crisis, such as residence in emergency shelters (Humphreys & Lee, 2005) or when filing protective orders (Walker et al., 2011). The goals of the present study were to determine whether IPV history predicts clinically significant sleep problems after acute crises have subsided and, if so, to evaluate reasons for this association. Our broader goal was to address the fact that IPV has been overlooked in research on marital status, divorce, and health, and to begin to contribute to a research base in this area.
In terms of incremental validity, among midlife women reporting a history of physical IPV, the predicted odds of poor sleep quality in the past month were significantly greater than the odds for women who reported no history of physical IPV. This was observed after adjusting for past-year stressful life events and childhood trauma, but contrary to expectations, neither of these other stressors was a statistically significant predictor of poor quality sleep.
Measurement approaches may have partially contributed to this unexpected pattern of results. Some studies that have documented associations between retrospective reports of childhood stress and adult sleep quality have focused on childhood adversity, a construct that not only includes specific traumatic events but also encompasses parental mental illness, along with parental marital discord, separation, and divorce (Chapman et al., 2011). Although other studies, like ours, have focused on childhood trauma alone, they have typically measured abuse frequency rather than counts of specific traumatic events, and have included assessments of emotional abuse along with physical or sexual abuse (Greenfield et al., 2011).
In terms of the lack of predictive validity of past-year stressful life events, the incremental validity model tested an IPV-independent life events measure that included only 14 items. This is a smaller number and range of stressful life events, compared with event measures that have predicted poor quality sleep in other studies (LeBlanc et al., 2009). Indeed, inspection of the correlation matrix shown in Table 2 reveals that the correlation between sleep quality and the IPV-dependent life events measure, which included 30 stressful events, was statistically significant (coefficient = .29). IPV history predicted poor sleep quality in the model that adjusted for this life events measure (i.e., the socioemotional model), thereby providing some evidence for its incremental validity. In sum, although IPV history predicted subjective sleep quality after adjusting for other stressors, the test of incremental validity was dampened because not all of these stressors predicted sleep quality. This question requires evaluation in future research, with close attention to measurement issues.
Keeping this limitation in mind, the second aim was to evaluate three explanatory models—socioemotional, medical, and sociodemographic—in terms of their ability to account for correlations between IPV history and poorer quality sleep. Across these models, several other statistically significant predictors of poor subjective sleep quality were identified: being in the first 5 years of menopause when risk of vasomotor symptoms is higher, more severe posttraumatic stress symptoms, the presence of an activity-limiting physical health problem, and having an annual income lower than the local median household income. All of these relationships are consistent with prior research, and collectively they emphasize the importance of adopting a biopsychosocial perspective on sleep quality among midlife, postmenopausal women. Yet, no model fully accounted for connections between IPV history and poor quality sleep. Thus, there is a robustness to this connection that is evident across multiple explanatory variables.
When poor subjective sleep quality was predicted by IPV chronicity, rather than its presence or absence, a statistically significant dose–response relationship was observed. The predicted odds of poor quality sleep increased linearly across chronicity levels selected to characterize community women, and women seeking help from agencies serving victims of violence. Adjusting for predictors that were statistically significant in the explanatory models attenuated the dose–response relationship. Thus, at the highest levels of chronicity, associations between IPV history and poor quality sleep are partially accounted for by posttraumatic stress symptom severity, physical health problems, and to a lesser extent by lower income.
Overall, among midlife, postmenopausal women with divorce histories, physical IPV history was an independent predictor of poor quality sleep, with some evidence for a dose–response relationship. Yet, the question of what explains this association remains unanswered. Given that IPV may be considered a potentially traumatic experience, research on posttrauma adaptation may be useful here. It may seem surprising that connections between IPV history and poor sleep quality are not fully accounted for by symptoms of depression and posttraumatic stress, given that difficulties with sleep are core components of both disorders. However, some treatment-outcome studies of PTSD reveal that insomnia and sleeping difficulties do not respond to psychological interventions to the same degree as do other PTSD symptoms. After an otherwise successful treatment, sleep problems often persist, and good sleeper status is not achieved, even when participants no longer meet diagnostic status for PTSD (Galovski, Monson, Bruce, & Resick, 2009; Zayfert & DeViva, 2004). Thus, following trauma exposure, sleep difficulties appear to be more resistant to recovery compared with other psychological symptoms, even when recovery is facilitated by psychological interventions.
The foregoing interpretations assume a causal connection between IPV history and poor subjective sleep quality, but this cannot be established with the cross-sectional design of the present study. Reverse causation may be contributing to the present pattern of results, with poor quality sleep perhaps pre-dating and contributing to experiences of IPV (Rauer & El-Sheikh, 2012). Or, the pattern of results observed here may be a product of one or more third variables—factors that contribute both to IPV experiences and to poor quality sleep, such as difficulties with emotion regulation.
Limitations pertaining to measurement and sample selection should also be considered when interpreting the present results. With respect to measurement, vasomotor symptoms were assessed with a proxy indicator, rather than directly. This may have underestimated the prediction of poor quality sleep from such symptoms. Also, we were able to biologically confirm postmenopausal status for women in the laboratory phase but not for those who participated in the questionnaire-only phase. Finally, the assessment of IPV relied on retrospective reports, which are subject to the fallibility of memory. With respect to sample selection, we recruited a convenience sample of community women, and therefore our participants should not be presumed to be representative of all women with divorce histories. For example, the women we recruited were able to maintain good physical health at midlife. Also, although we did not systematically assess these factors, some women mentioned that the study’s travel and scheduling requirements were prohibitive, and others declined participation because they were uneasy about discussing their relationship experiences. Overall, our sample may be skewed toward women with more tangible and emotional resources, including resources that promote physical resilience. Furthermore, the present findings should not be generalized to premenopausal women, to women of any menopausal status who currently experience IPV, or to men. The sensitivity of sleep quality to menopausal status, marital status, and also to gender (Mallampalli & Carter, 2014) means that additional research is necessary to determine how these factors moderate connections between sleep quality and IPV.
Acknowledging these limitations, the results of the present study have several implications. Clinically, they emphasize the importance of assessing sleep quality, even among women who are many years removed from IPV experiences. Furthermore, sleep quality should receive attention even when disorders such as depression and PTSD have resolved. In terms of research, IPV history deserves more attention for understanding the widely documented connections between marital status and sleep quality. The importance of subjective sleep quality for physical health also argues that assessing IPV history may be one way to identify divorced persons at increased risk of poor health.
Footnotes
Authors’ Note
Vicki Ellison Burns is now at the Lansing School of Nursing and Health Sciences, Bellarmine University, Louisville, Kentucky, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the National Institute on Aging (R21 AG0249002-02).