
Abstract
Informed by the social determinants of health (SDH) framework, this study examined whether women’s attitudinal acceptance of intimate partner violence (IPV) varies according to material circumstances, such as characteristics of their communities. Data were obtained from the sixth Bangladesh Demographic Health Surveys (BDHS) of 2011, a cross-sectional and secondary population-based study that covers the entire population residing in noninstitutional dwelling units in Bangladesh. The sample included 16,480 married women living in 600 communities who were 15 to 49 years old. Results showed that community characteristics were significantly associated with married women’s attitudes toward IPV. The associations, however, were considerably more complicated than previously thought. Community poverty and wife beating justification were inversely related, such that regardless of their socioeconomic status (SES), living in poorer communities increased women’s likelihood of condemning IPV (p < .001). Also, unexpectedly, as illiteracy increased in the community, women’s likelihood of viewing IPV as justified decreased (p < .01). Living in communities with strong patriarchal norms was associated with greater tolerance for IPV (p < .001). Use of the SDH framework in this study provided empirical evidence of the importance of social determinants in determining risk for attitudinal acceptance of IPV among women, which can be targeted for future research and intervention.
Keywords
Introduction
Nearly 30% of ever-partnered women worldwide have experienced intimate partner violence (IPV) in their lifetime (World Health Organization [WHO], 2012). The prevalence of IPV varies among countries ranging from 23.3% in high-income countries to 37.7% in low-income countries. The variation of IPV across countries and its greater prevalence in low-income settings call for extending the epidemiological analysis of IPV from individual risk to societal level risk factors or social determinants of health (SDH) analysis. The SDH framework has increasingly gained attention in public health literature over the last several years (Almeida, Casanova, Caldas, Ayres-de-Campos, & Dias, 2014; Gustafsson et al., 2014; Mumtaz et al., 2014). Particularly since the WHO’s creation of Social Determinants of Health Commission (CSDH) in 2005, identifying and addressing the SDH have become a priority for health researchers (Bell, Taylor, & Marmot, 2010; Dean & Fenton, 2013; Marmot, Friel, Bell, Houweling, & Taylor, 2008). According to this framework, the social condition in which people are born, live, work, and age shape their health. These social conditions are themselves influenced by the distribution of money, power, and resources at the global, national, and local levels (WHO, 2012). The SDH framework highlights the importance of gender inequality as a structural phenomenon that is connected with other dimensions of social stratification, and which has the effect of increasing women’s burden of death, illness, and injury (Bates, Hankivsky, & Springer, 2009).
The SDH framework postulates that social and political mechanisms give rise to social stratification and hierarchies, and based on individuals’ positions in the hierarchies, their exposure and vulnerability to health comprising conditions vary. The social determinants operate through a set of “intermediary determinants”: material circumstances (such as neighborhood quality), psychosocial circumstances (such as psychosocial stressors, social support), and behavioral and biological factors (such as nutrition, physical activity, tobacco consumption; Solar & Irwin, 2010). This study aimed to empirically examine the relevance of the community, which is an “intermediary determinant” of the SDH framework in explaining women’s attitudinal acceptance of IPV.
Although the impact of the behavioral and psychosocial factors on IPV are well documented in IPV literature (Bates, Maselko, & Schuler, 2007; Hindin, Kishor, & Ansara, 2003; Kim et al., 2007; Koenig, Ahmed, Hossain, & Mozumder, 2003; Lawoko, 2006; Waltermaurer, 2012; Yount, Halim, Schuler, & Head, 2013), little is known about the impact of the community environment on one’s IPV acceptance attitudes. Some studies show that permissive norms of IPV in the community may have links with elevated risks for individual perpetration of IPV or individual justification of such behavior (Koenig, Stephenson, Ahmed, Jejeebhoy, & Campbell, 2006; Waltermaurer, 2012). Other studies demonstrate that the influence of individual-level risk factors of intimate partner violence against women (IPVAW) may vary between communities depending on the variation in community-level acceptance of such behavior. For example, Boyle, Georgiades, Cullen, and Racine (2009) found in a study in India that the protective influence of higher education on women’s IPV risks was subdued in the communities that were lenient toward IPVAW (Boyle et al., 2009). Although community-level norms have been examined in these few studies, the influence of community socioeconomic context, such as poverty and illiteracy, has been given inadequate attention.
Research has shown that concentrated disadvantages at the community level may disrupt social cohesion and lead to social disorganization that increases the risks for violence and crimes (Sampson & Wilson, 1995). Drawing on social disorganization theory, studies have documented that community-level poverty positively predicted IPV victimization and perpetration for both men and women (Edwards, Mattingly, Dixon, & Banyard, 2014). Benson, Fox, DeMaris, and Van Wyk (2003) suggested that greater incidences of IPV in disadvantaged neighborhoods may be influenced in part by employment instability and subjective financial strain that reduce men’s sense of self-worth and trigger intimate violence as the stress response. However, most of the evidence of positive association of community-level disadvantages and IPV comes from U.S.-based studies, whereas findings of non-U.S.-based studies are inconclusive. For example, a systematic review of 17 studies conducted between 1990 and 2011 (VanderEnde, Yount, Dynes, & Sibley, 2012) found no consistent support for community poverty and IPV relationship in non-U.S.-based settings, implying that concepts drawn from social disorganization theory, such as concentrated disadvantage, residential stability, and immigrant concentration, may not be applicable to nonurban, non-U.S. settings. Results from a recent study in Bangladesh (VanderEnde, Sibley, Cheong, Naved, & Yount, 2015) demonstrated that the relationship of income and IPV operated only at the household level, and when controlled for household income, the relationship between living in low-income community and women’s risk of experiencing IPV was nonsignificant.
Although existing literature do not clearly show a positive significant association of community-level poverty and IPV, they nonetheless suggest that other community characteristics, such as community-level literacy, gender norms, and empowerment, may operate in determining women’s IPV risks. Across various studies, community gender norms appeared to be a strong correlate of IPV risks for women (Koenig et al., 2006; Yount & Li, 2009). In a recent study in Bangladesh, Azziz-Baumgartner et al. (2014) found that compared with the general population, IPV burden was much higher in the low-income and low-literate communities. In another study, Koenig et al. (2003) demonstrated that women living in communities that are characterized by higher levels of women empowerment were at lower risk of experiencing IPV. While these studies examined the actual occurrences, it is not clear if the characteristics of the community play any role in women’s attitudinal acceptance of such behavior. Research shows that in the low-income countries, women have lower status in society and limited option to leave an abusive husband (Assaf & Chaban, 2013). Domestic violence disempowers them and erodes their self-esteem (Azziz-Baumgartner et al., 2014). In such contexts, women may begin to justify their experiences of IPV and suffer abuse silently (Kishor & Johnson, 2004; Linos, Slopen, Subramanian, Berkman, & Kawachi, 2013).
Informed by SDH framework and the existing literature on influence of community context on health behaviors, this study tested the following hypothesis: Living in disadvantaged communities is positively associated with individual woman’s justification of wife beating.
Data and Method
Dataset
Data for this study came from the sixth BDHS of 2011, which is a cross-sectional and secondary population-based study that covers the entire population residing in noninstitutional dwelling units in the country. The BDHS is part of the Demographic and Health Surveys (DHSs) that is funded by the United States Agency for International Development (USAID) and carried out in about 90 countries. The survey is based on a two-stage stratified sample of households. In the first stage, 600 enumeration areas (EAs) were selected with probability proportional to the EA size. In the second stage of sampling, a systematic sample of 30 households on average was selected per EA to provide statistically reliable estimates of key demographic and health variables for the country as a whole. With this design, the survey selected 18,000 residential households, which were expected to result in completed interviews with about 18,000 ever-married women. After deleting the incomplete and missing observations for each variable in the study, the sample for the study consisted of 16,480 married women who were 15 to 49 years old, currently married, and “usual residents” (i.e., not “visitors”).
Dependent Variable: Wife Beating Attitudes Index
The dependent variable was a wife beating attitudes index, which was assessed with five questions that asked women if they think husbands are justified in beating wives in five different scenarios. The five scenarios were as follows: wife going out without telling him, neglecting the children, arguing with him, refusing to have sex with him, and burning the food. The response “yes” implies that she believes wife beating is justified in that specific scenario, and “no” implies that she does not find wife beating is justified in that specific scenario. The index ranged from 0 to 5 (Cronbach’s α = .78). This index has been widely used by researchers (Boyle et al., 2009; Kishor & Johnson, 2004; Marshal & Furr, 2010).
Independent Variables
Community disadvantages
For assessing community disadvantages, three indicators were used that have been used by previous research (Gustafsson et al., 2014; Jesmin & Chaudhuri, 2013; Stephenson, 2009). The details of these indicators are presented in Table 1. These indicators were (a) proportion of women in the community who live in the poorest households, (b) proportion of women in the community who are illiterate, and (c) mean wife beating score of the community. Mean wife beating score of the community reflects how patriarchal the community is. Prior research has shown that communities that are relatively tolerant of violence against women are likely to limit women’s rights and choices, such as availability and utilization of maternal health care services (Adjiwanou & LeGrand, 2014). The effect of community gender norms on women is so strong that Boyle et al. (2009) found that women’s acceptance of mistreatment at the community level muted some of the protective influence of higher education on their IPV risk. Communities were defined according to the EAs. For the Census purpose, the Bangladesh Census Bureau divides the country in almost 296,718 EAs. Each EA is a delimited area comprising about 120 households. In the DHSs, each EA is considered as a primary sampling unit (PSU). The PSUs are typically urban neighborhoods or rural villages that represent within-country variations that are not attributable to individual, and have been used in previous health research (Stephenson, 2009; Subramanian, Özaltin, & Finlay, 2011). Every respondent in the BDHS was identified by a PSU number. For creating community-level variables, individual responses were averaged and aggregated to the PSU level.
Summary Statistics for Individual-Level and Community-Level Variables in the Analysis.

Note. N = 16,480 married women in 600 communities (PSUs) in Bangladesh. The community-level variables were derived by aggregating the “valid” responses of all women surveyed to the community level. Total number surveyed in a community ranged from 13 to 42, with an average of 29.7. NGO = nongovernmental organization; PSU = primary sampling unit.
Control Variables
Individual-level socioeconomic status (SES) variables
Individual-level demographic and socioeconomic variables such as age, religion, education, and household wealth were adjusted for in the analysis as confounding factors. Prior research shows that younger age (Rahman, Hoque, & Makinoda, 2011), lower education (Linos et al., 2013), living in the poorest households (Rahman et al., 2011; Sambisa, Angeles, Lance, Naved, & Thornton, 2011), and being Muslim (Alam, 2007) are associated with elevated risks of IPV.
Age was measured as a continuous variable. Religion was categorized as Muslims and non-Muslims with non-Muslims as the reference group. Education was categorized into four levels (based on the highest level completed): (a) no schooling, (b) primary education, (c) secondary education, and (d) higher education. Household wealth was categorized in five groups based on the BDHS constructed wealth index: (a) the poorest, (b) the poorer, (c) the middle, (d) the richer, and (e) the richest. The index was constructed in three steps using household asset data via principal components analysis. In the first step, asset indicators were selected based on the most readily observable assets of households (such as refrigerator, car, drinking water amenity), including country-specific assets. In the second step, a principal components analysis was used to assign weights to each asset. In the third step, households were sorted in increasing order of asset ownership and then divided as follows: the lowest 20% of households were coded as poorest; the next 20% as poor, households between 40% and 60% of asset richness were coded as middle, households between 60% and 80% of asset richness as richer, and between 80% and 100% were coded as richest (Table 2).
Multilevel Logistic Regression Models Predicting Wife Beating Attitudes Index. a
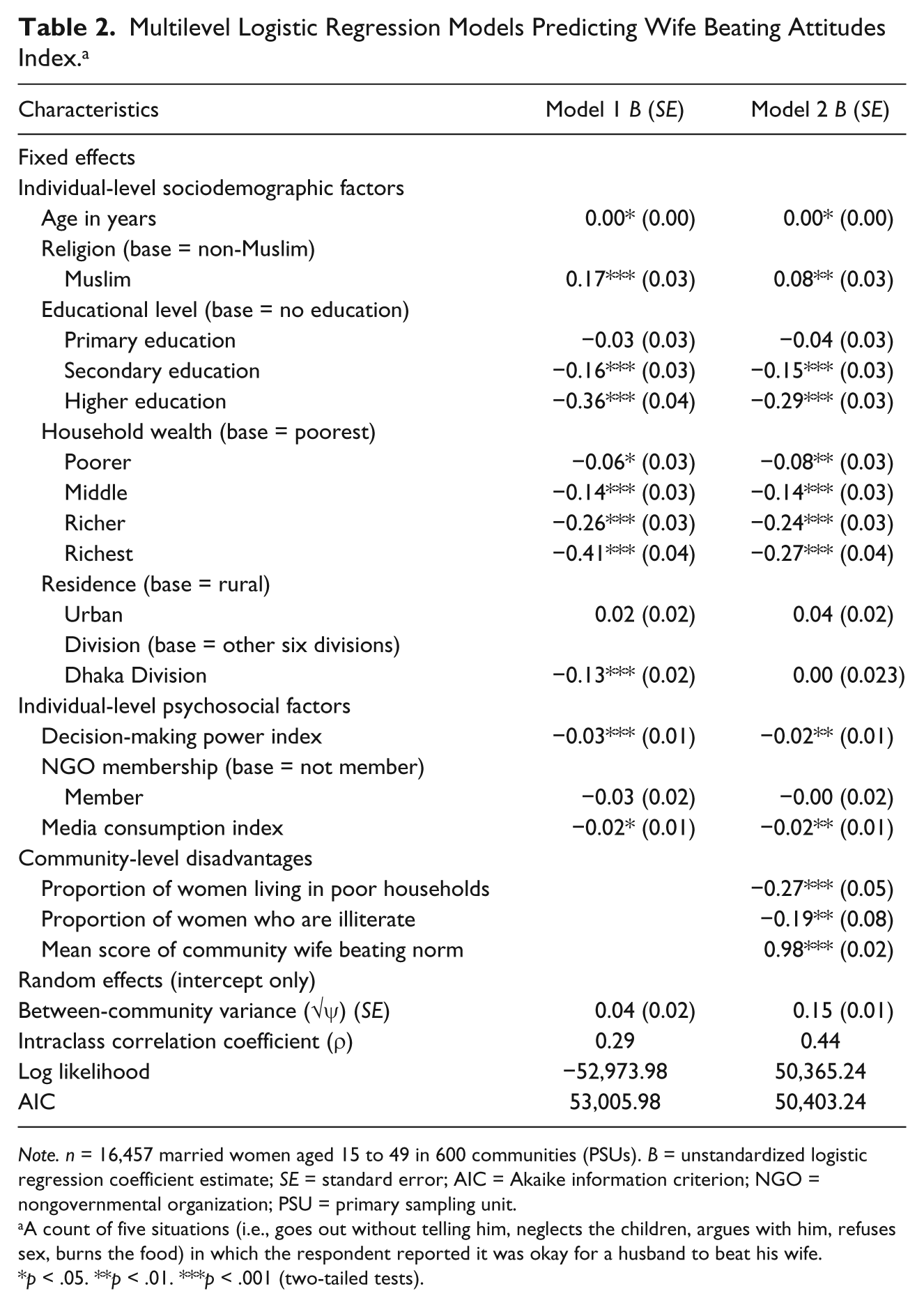
Note. n = 16,457 married women aged 15 to 49 in 600 communities (PSUs). B = unstandardized logistic regression coefficient estimate; SE = standard error; AIC = Akaike information criterion; NGO = nongovernmental organization; PSU = primary sampling unit.
A count of five situations (i.e., goes out without telling him, neglects the children, argues with him, refuses sex, burns the food) in which the respondent reported it was okay for a husband to beat his wife.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
Two residence variables, level of urbanization and division, were included in the analysis. Research shows that due to their greater exposure to corporal punishments and patriarchal gender norms, women in rural areas have higher odds of justifying wife beating (Yount & Li, 2009). Bangladesh has seven administrative divisions: Barisal, Chittagong, Dhaka, Khulna, Rajshahi, Rangpur, and Sylhet. The capital Dhaka City is located in the Dhaka Division, which represents relatively progressive environments and greater opportunities for women in terms of education and employment. Prior research shows that women in Dhaka Division were more likely to have greater control over their sexual and reproductive health (Jesmin & Cready, 2015; Kamal, 2000).
Psychosocial variables
According to the SDH model, psychosocial stressors, stressful living circumstances and relationships, and social support and coping styles (or the lack thereof) may lead to low social cohesion and disintegration of social bonds (WHO, 2010). Three psychosocial variables were examined in this study: decision-making power, membership in nongovernmental organizations (NGOs), and media consumption.
Women’s decision-making power is an indicator of their status in the household that act as a protective factor against their physical and psychological abuse (Assaf & Chaban, 2013; Donta, Nair, Begum, & Prakasam, 2016). Three questions were used to create a decision-making power index: (a) participation in decisions about health care, (b) large household purchases, and (c) visits to family or relatives. Code responses for each item follows: “1” if the woman indicated that she usually made the decision alone or with her husband/partner and “0” if she indicated that she was not involved in making the decision. The recoded responses were summed up across the three items to create a “decision-making power in the household” index. Scores ranged from “0” = no involvement in any of the three decisions to “3” = involved in all three decisions.
Women’s membership in NGOs was examined as a psychosocial variable. According to the SDH model, social support is one of the strongest psychosocial variables. In the developing countries, women’s membership in NGO has been shown to provide women opportunity for peer networking and increasing collective efficacy that plays positive role in adopting and maintaining healthy behaviors (Frumence, Eriksson, Nystrom, Killewo, & Emmelin, 2011). These informal, volunteer groups are instrumental in building trust that gives a woman more confidence in the health education she receives, and greater sense of control over her own as well as children’s health and well-being (Valadez, Hage, & Vargas, 2005).
An additive media consumption index was created that measured the frequency with which women were exposed to any of the three media use: television, radio, and newspaper/magazine. The additive media consumption index took values from 0 through 9, where 0 = no media consumption at all and 9 = used three media almost daily, and it is based on the frequency categories of each of the three media. This was the third psychosocial factor considered. In the non-Western societies, by raising awareness and addressing gender issues, health education programs broadcasted in the media provide role models for new behaviors and create a favorable environment for women. A large number of research has shown that greater media consumption is significantly associated with greater health knowledge, self-efficacy, risk perception, and overall positive attitudes toward women and shift in gender norms among the audiences (Figueroa, 2014; Kaufman, 2014). Media, in these countries, help community mobilization and empower the viewers by enhancing their social networks and social capital (Jesmin & Chaudhuri, 2013).
Data Analysis
This study estimated a series of multilevel regression models using the SPSS for Windows version 22.0 (SPSS, Inc., 2013). Descriptive analyses were performed for the individual-, psychosocial-, and community-level predictors, as well as the wife beating attitude index. Model 1 estimated the relationship between the index of IPV attitudes and individual SES and psychosocial variables only. Model 2 estimated the relationship between the index of IPV attitudes and three community-level variables with controls of individual-level variables. Impacts of the individual-level factors were assessed as the fixed effects, whereas the variations across communities were assessed as random parameters. Two-tailed p values were reported to reflect the statistical significance of effects. Model goodness of fit was assessed using the deviance or likelihood ratio test and Akaike’s information criterion (AIC). All the tolerance levels were above the conventionally accepted “cutoff” of 0.2 (Hamilton, 1992, p. 134), which suggested that multicollinearity was not a problem.
Results
Of the women in this study, median age was 30 years (range = 13-49), 89% were Muslims, 25% had no education, and 67% obtained primary or secondary education. About 8% had higher education. Women living in the poorest, poorer, middle, richer, and richest households accounted for 17%, 19%, 19%, 21%, and 23%, respectively. Average media consumption was 1.5 in the index 0 to 9, where 0 meant no consumption and 9 meant consumption of all three media (TV, radio, and newspaper/magazines) 7 days a week. Average decision-making power was 1.87 in the index 0 to 3, where 0 meant no decision-making power at all and 3 meant involvement in all household decisions. On average, the communities were characterized by having about 36% of women as poorer and poorest, and 24% of women as illiterate (Table 1). Table 1 shows that 68% of the women did not support wife beating in any of the five scenarios presented to them, while nearly 2% of them reported wife beating as justified in all five scenarios. Arguing with husbands was viewed as the major justified reason for wife beating (22.5%), followed by neglecting children (18.3%), and going out without husband’s permission (16.8%). About 8% women reported that wife beating is justified if a wife refuses to have sex with her husband. About 4% of the women believed that husbands are justified to beat wives if they burn foods.
Multivariate Analysis
In Model 1, all socioeconomic and psychosocial variables had significant associations with the index of IPV attitudes. Muslim women were more likely to justify IPV than their non-Muslim counterparts (p < .001). Although primary education had no association with IPV attitudes, having secondary or higher education was significantly associated with women’s greater likelihood of rejecting IPV (p < .001). Compared with the poorest, women living in poorer, middle, rich, or richest asset households were significantly more likely to reject IPV (p < .001). Living in urban areas or in Dhaka Division was not significantly associated with IPV attitudes. Among the psychosocial variables, media consumption and decision-making power were significantly associated with rejection of wife beating attitudes. With increase of media consumption, women were less likely to justify wife beating (p < .05). Also, women who had greater decision-making power in their households were less likely to justify wife beating (p < .001).
In Model 2, when controlled for individual demographic, socioeconomic, and psychosocial factors, all three community-level variables were significant. Unexpectedly, two community disadvantage indicators, percentage of women living in the poorest households and percentage of illiterate women in the community, were significantly negatively associated with women’s wife beating justification attitudes. Within a community with 1 percentage point increase of women living in the poorest households, the likelihood of individual woman’s justification of wife beating decreased by 0.27 points in the wife beating justification index (index value = 0-5; p < .001). Increase of every 1 percentage of women in the community who were illiterate was associated with a decrease in wife beating justification index by 0.19 points (index value = 0-5; p < .01). Community wife beating norm was positively associated with individual woman’s justification of wife beating. Women living in communities that were permissive of wife beating were also more likely to justify wife beating individually (p < .001). With 1 percentage point increase of women in the community who justified wife beating, an individual woman’s justification of wife beating increased by 0.98 points in the attitude index (index value = 0-5 points). In Model 2, all individual-level variables remained statistically significant. Older age (p < .05) and being Muslim (p < .01) increases likelihood of individual women’s justification of IPV. Having secondary and higher education (p < .001) and living in middle, richer, or richest households decreased women’s likelihood of justifying IPV (p < .001). Among the psychosocial variables, decision-making power (p < .01) and consumption of media (p < .01) were inversely associated with wife beating justification.
In summary, this study found that at individual level, women with higher SES and greater psychosocial resources were less likely to justify IPV. However, regardless of their individual SES, community SES indicators significantly influenced their IPV attitudes. Living in communities with greater poverty and illiteracy increased their likelihood of condemning IPV, whereas living in communities with strong patriarchal norms increased their likelihood of justifying IPV.
Discussion
Informed by the SDH framework, this study examined married women’s IPV attitudes in a low-income country. Results showed that community disadvantage was related to IPV justification among married women, even when individual SES characteristics were taken into account. Overall, all the community-level SDH factors were associated with IPV but the associations were considerably more complicated than previously thought. This study contributes to SDH literature by adding new evidence on the links of community-level poverty, illiteracy, and gender norms with IPV justification, particularly in the low-income settings.
In the multilevel analysis, community poverty and wife beating tolerance had an inverse association, such that as poverty increased in a community, IPV tolerance decreased. First, in the economically disadvantaged communities, men may have less control over their wives, as they may not be very successful in providing economic security to their wives. In these communities, women may be less likely to tolerate a violent husband as the husband fails to perform his socially expected breadwinner role (Jesmin & Cready, 2015). Among the poor urban slums in Bangladesh, Jesmin and Salway (2000) found that social control against divorce was loose, family ties were weaker, and women had increased option for participation in (low skill) labor force. These women, therefore, were more able to avoid partner abuse by rejecting unfavorable marital ties. Second, as women’s subordination to their husbands is a norm in Bangladesh, women’s condemnation of husbands’ authority, such as disapproval of wife beating is an indication of weaken trust and disruption of social order. Social disorganization literature suggests that concentration of poverty is associated with social conditions such as crime and social disorder, and risky health behaviors (Sampson & Wilson, 1995). It is possible that the extreme material adversity in these communities weakens the social order and creates an environment where women’s disapproval of husbands’ abusive behavior or disobedience, which would have been otherwise viewed as “maladaptive behavior” or “deviant behavior,” increases. Finally, according to the findings of this current study, IPV justification is likely to be greater in economically privileged communities. This is not surprising as in economically better off communities, women’s economic dependence on the husbands and their fear of poverty if abandoned by the husbands may be a strong reason for tolerating IPV (Akter & Begum, 2012).
The second major finding of inverse association of illiteracy in the community and women’s IPV tolerance is not consistent with prior literature suggesting that IPV occurrences are higher in low-literate communities (Azziz-Baumgartner et al., 2014). It is possible that actual occurrences of IPV may be higher in low-literate communities, but the tolerance for such behaviors may be lower due to the same reasons that explain lower IPV justification in the poor communities. There are two other possible explanations for this finding. First, although in recent years girls’ enrollment in primary and secondary schools has surpassed boys’ enrollment and female education may have become a “norm” in Bangladesh (Schuler, 2007), opportunities for women’s labor force participation in gainful jobs or other alternatives is still limited (Yount et al., 2013). By being and remaining married, women gain prestige and social identity (Alam, 2007). In some cases, education appears to function as a proxy for SES of the family (Desai & Alva, 1998). As being educated to secondary or higher levels may not ensure women’s opportunities to be employed gainfully, many women regardless of being educated to such levels may tolerate wife beating. Many women may report wife beating justified. The second explanation for educated women for justifying wife beating is that female education alone may not be a strong indicator of empowerment. For example, Mahmuda and Tasneem (2014) found that education was perceived as most important only by women who were employed in formal paid jobs and those who were economically inactive. Education was not perceived as important by the rest who were employed in the informal work or engaged in market works inside the homes. Being able to watch TV and having mobile phones were rather the stronger indicators of their empowerment. Other literature suggests that traditional family dynamics such as timing of marriage and childbearing and the influence of mothers and mothers-in-law may play a greater role in young married women’s lives (Bates et al., 2007; Schuler & Rottach, 2010). More pertinently, the study by Boyle et al. (2009) found that women’s acceptance of mistreatment at the community level muted some of the protective influence of higher education on their IPV risks (Boyle et al., 2009).
The third major finding that community norms permissive of wife beating was the strongest predictor of justification of IPV is consistent with prior studies showing positive association of IPV and community norms (Boyle et al., 2009; Koenig et al., 2006). Spousal violence, especially physically forced sex by husbands is perceived as normal and tolerated as girls are socialized from the very early childhood that men are their protectors, and good wives should be submissive to their husbands (Fahmida & Doneys, 2013; Naved, 2013). Therefore, regardless of their individual SES, living in highly patriarchal communities increases their odds of justifying IPV.
Two psychosocial factors examined in this study were significantly associated with wife beating attitudes. Women who have greater decision-making power and access to media were less likely to justify IPV. Women’s control over household decisions and their own health and well-being may increase their confidence and empower them to denounce IPV. Consumption of media may increase awareness of IPV and gender issues in general among the women and empower them to view IPV as unjustified. Women’s SES status influences their attitudes toward IPV. Older women were more likely to justify wife beating. Increasing education and wealth at the individual level were associated with decreased justification of wife beating. Thus, findings of this study indicate that women who have higher SES and lower psychosocial risk are more likely to reject wife beating. But community matters. Regardless of individual woman’s SES and psychosocial circumstances, community SES influences her attitudinal acceptance of IPV.
Because in this study women were interviewed about their perceptions, there may have been social desirability response bias in the data. It is possible that some women may have responded that wife hitting or beating was justified “to appear compliant with perceived norms” (Yount et al., 2013, p. 350). In addition, this study did not consider the effects of cumulative disadvantages that is the accumulation of disadvantages over the life course of an individual that may have influenced the attitudinal acceptance of IPV. Also, because the dataset was very large, some weak associations may have appeared as significant. Furthermore, some of the operationalizations of study variables were limited by the number of items used to assess the variable. Furthermore, actual IPV exposure was not examined. Attitudes about violence often do not map on to actual behavior, and as such, tolerance is not a sufficient proxy to estimate rates of true IPV tolerance. Despite these limitations, findings of this study have important implications for IPV prevention programs in the low-income countries. (a) The finding of inverse association of poverty and IPV attitudes suggests that regardless of their higher SES status, women in richer neighborhoods have risks of tolerating IPV. The recognition of the tendency for IPV tolerance among married women to occur among the privileged communities could lead to design of prevention messages targeted specifically to these types of communities. (b) The finding that IPV tolerance may be greater in higher literate communities indicates that providing women opportunities for education may be insufficient to change their IPV attitudes. For these women, creating opportunities for gainful employment will likely be necessary before the influence of education on their attitudes can be realized. (c) The finding that gender norms prevalent in the community is the strongest predictor of women’s attitudes toward IPV underscores the importance of intervention programs targeted to change gender norms. Finally, use of the SDH framework in this study provided empirical evidence of the importance of social determinants in determining risk for attitudinal acceptance of IPV among women, which can be targeted for future research and intervention. The implications of the findings have direct relevance to recent global discussions and increasing recognition that violence against women hinders progress in achieving development targets, in particular, in the low-income countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.