
Abstract
The current study investigated the influence of anger problems on partner violent men’s long-term response to treatment, as indicated by criminal recidivism during an 8-year period after treatment initiation. Participants were 132 men who presented for treatment services at a community-based domestic violence agency. Results indicated that individuals with extensive anger problems had more charges for general violence (GV) offenses and more ongoing problems with protection orders than did those with Normal Anger (NA) profiles. Examinations of specific anger scales indicated that low Anger Control (LAC) and high Anger Expression predict GV recidivism. These findings indicate that a standard cognitive-behavioral treatment program may not adequately reduce the recidivism risk of partner violent men with pronounced anger problems, stress the importance of further research to understand the role of anger problems in partner violence treatment, and highlight the need to develop and evaluate new intervention approaches for partner violent men with serious anger dysregulation.
Keywords
One primary social response to the widespread problem of intimate partner violence (IPV) involves group psychoeducational programs for perpetrators. Unfortunately, these interventions have yielded only modest effects based on meta-analytic reviews of treatment studies (Arias, Arce, & Vilariño, 2013; Babcock, Green, & Robie, 2004; Feder & Wilson, 2005). Clearly, there is a need to strive for a better understanding of factors underlying treatment response of IPV perpetrators to guide future efforts to develop new intervention strategies and enhance the effectiveness of IPV interventions.
Research suggests that anger problems may be an important focus in understanding IPV intervention effects, as anger is a robust correlate of IPV. Norlander and Eckhardt (2005) found that partner violent men reported more anger and hostility than their nonviolent counterparts, including nonviolent control groups experiencing significant relationship distress. In addition, greater anger and hostility scores differentiated perpetrators of more severe IPV from those who perpetrate less severe IPV. Similarly, Barbour, Eckhardt, Davison, and Kassinove (1998) compared State–Trait Anger Expression Inventory (STAXI, Spielberger, 1988) scores from a community sample of violent, dissatisfied-nonviolent, and satisfied nonviolent married men. They found statistically significant differences on all STAXI scales with IPV perpetrators reporting higher State Anger, Trait Anger, Anger In, Anger Out, and lower Anger Control than maritally satisfied nonviolent men. Maritally violent men scored significantly higher than maritally dissatisfied nonviolent men on Trait Anger and Anger Out, and significantly lower on Anger Control. Altogether, it appears that partner violent men have greater reported anger problems than nonviolent men in terms of the general propensity to become angry and a greater tendency toward problematic styles of responding to and expressing anger.
Despite these findings, some scholars in this field dispute the notion that anger is an important factor in IPV perpetration (see Gondolf, 2011; Pence & Paymar, 1993). In fact, many state standards specifically ban or caution against the use of anger management as a primary focus of IPV intervention (Maiuro & Eberle, 2008; Maiuro, Hagar, Lin, & Olson, 2001) based on the idea that anger is a rationalization for losing control and IPV is an expression of control. In addition, a treatment focus on problems such as anger, substance abuse, histories of trauma, or other mental health concerns is thought to absolve perpetrators of personal responsibility for abuse. The Duluth Model (Pence & Paymar, 1993), one of the most widely used approaches to perpetrator treatment, aligns with this notion (Corvo, Dutton, & Wan-Yi, 2009). These debates highlight a need for conceptual and treatment models that can uphold offenders’ personal responsibility without ignoring or suppressing research on emotional and behavioral factors that may contribute to IPV, including problems with anger.
In addition to being an important correlate of IPV, anger problems also appear to be a significant predictor of treatment response for IPV offenders. Murphy, Taft, and Eckhardt (2007) conducted a cluster analysis on a sample of 139 partner violent men using STAXI scores to explore the link between anger and treatment response. The cluster analysis revealed three groups, labeled Pathological Anger (PA), Low Anger Control (LAC), and Normal Anger (NA). The PA group reported the most pronounced anger problems, with average scores on the STAXI scales upward of the 80th percentile for Anger In; above the 90th percentile for Trait Anger, Anger Out, and Anger Expression; and below the 10th percentile for Anger Control. The LAC group reported above average levels of Anger Expression (a composite score of Anger Out, Anger In, and Anger Control), with the group mean at the 76th percentile, below average levels of Trait Anger (below the 40th percentile), and very low levels of Anger Control (group mean below the 10th percentile). Finally, the NA group had average scores on Anger Expression (group mean at the 39th percentile) and relatively low scores on Trait Anger (group mean below the 20th percentile). Data gathered from their victim partners revealed that both the PA and LAC groups perpetrated significantly more physical assault than those in the NA group during the 6 months after group cognitive-behavioral therapy for IPV. This difference remained even after controlling for the level of treatment exposure. Although these findings indicate that anger problems inhibit treatment response in the months after IPV intervention, it is also important to determine whether anger problems are associated with treatment response in the long term.
The purpose of the current study is to investigate the long-term influence of anger problems on partner violent men’s likelihood of criminal recidivism over an 8-year period after initiation of services at a community-based IPV treatment program. The data derive from an archival analysis of participants in a previous study of anger problems within a treatment program using a group cognitive-behavioral intervention (Murphy et al., 2007). The first hypothesis was that individuals with PA profiles would have more instances of long-term criminal recidivism than offenders with other anger profiles. The second hypothesis was that those with more severe anger problems—as assessed by the specific STAXI scale scores (i.e., lower Anger Control and higher Trait Anger, Anger Expression, Anger In, and Anger Out scores)—would have higher rates of criminal recidivism.
Method
Participants
Participants were 132 men who presented for treatment services at a community-based domestic violence agency between February 1999 and January 2001. Seven cases were dropped from the original sample of 139 (see Murphy et al., 2007) due to missing criminal history data. Participants reported an average age of 35.75 years at program intake (SD = 8.79). They averaged 13.11 years of formal education (SD = 2.49) and reported an average annual income of US$28,716 (SD = US$22,411); 81.06% were employed full-time, 12.12% employed part-time, 0.76% were laid off but returning, and 6.06% were unemployed at the time of intake; 50% identified as White (non-Hispanic), 43.9% Black, 2.3% Asian American, 1.5% American Indian, 1.5% Hispanic, and 0.8% as other. Mean session attendance was 10.57 (SD = 6.15). Most participants (80.3%) had a court recommendation for treatment. Some had a pending court case at the time of intake (6.8%), and the rest had no active court involvement related to partner abuse (12.9%). Due to missing data, the N for specific analyses varied from 130 to 131. Study procedures were approved by The University of Maryland, Baltimore County Institutional Review Board.
Measures
State–Trait Anger Expression Inventory
The STAXI (Spielberger, 1988) is a 44-item measure comprising five scales. The scales measure State Anger (which is not included in the current study), Trait Anger (the general propensity to experience anger), and three measures of anger expression, which together form the Anger Expression Composite Index: Anger In (the tendency to hold anger in and “stew” or “boil” without expressing it), Anger Out (external and often dramatic expressions of anger), and Anger Control (efforts to calm one’s self and regulate angry feelings). Participants indicate the extent to which items describe themselves on a 4-point scale from “almost never” to “almost always,” with the Trait Anger instructions focused on how individuals generally feel, and the anger expression instructions focused on how they generally react or behave when angry. In a previous analysis of this sample, Trait Anger and the three anger expression scales were used to create anger problem profiles using cluster analysis described above (Murphy et al., 2007).
In initial work with the current sample, internal consistency values for the STAXI scales were adequate: Anger In (α = .74), Anger Out (α = .77), Anger Control (α = .90), and Trait Anger (α = .89). These values are consistent with previous research, which has reported values ranging from .74 to .90 for Anger In, Anger Out, and Anger Control, and .82 to .89 for Trait Anger (Denson, Pedersen, & Miller, 2006; Forgays, Forgays, & Spielberger, 1997; Fuqua et al., 1991; Spielberger, 1988). Studies support the convergent and discriminative validity of the STAXI (Deffenbacher et al., 1996) as well as the measure’s proposed factor structure (Forgays et al., 1997; Fuqua et al., 1991). STAXI scales (Trait Anger, Anger Out, and Anger Control) reliably differentiate maritally violent men from maritally discordant, but nonviolent men (Barbour et al., 1998).
Criminal recidivism
The Maryland Judiciary Case Search was utilized to determine participant criminal recidivism. This publicly available search tool allows users to find criminal records for individuals whose offense occurred in the state of Maryland. Recidivism status over an 8-year follow-up interval was evaluated for each participant. Participant information was used to discriminate between individuals with the same name and to account for instances of multiple case records for an arrest. Specifically, a participant’s date of arrest and date of birth and/or additional information (e.g., address) available in the clinical file were utilized to identify and match criminal records. If multiple criminal record entries were linked to one criminal incident, only the original charges were coded.
Criminal incidents were coded into four mutually exclusive categories using a hierarchical decision rule: Intimate Partner Abuse (IPA) included charges of assault, battery, sexual assault, stalking, or other crimes against an intimate partner; General Violence (GV) included charges of assault, battery, malicious destruction of property, or other violent crime against a person or persons who could not be identified as an intimate partner; Other Protection Order Involvement (OPOI) included issuance of a new civil order of protection or peace order or violation of an existing protection or peace order in the absence of other criminal charges; and Other Crimes (not examined in the current study). If a criminal record could be placed into more than one category, precedent was given to a higher ordered category with the following succession: IPA, GV, and OPOI. In addition to coding recidivism during the 8 years after program intake, the same variables were also coded for the 5-year period prior to program intake to evaluate the extensiveness of criminal histories before treatment.
Procedure
STAXI scores were obtained during the second of two intake sessions at the agency research site. Clients were then assigned to a 16-week group cognitive-behavioral program (Murphy & Scott, 1996) consisting of weekly 2-hr sessions. Groups were closed-ended, meaning that they had a specific beginning and end date, with a fixed membership consisting of 9 to 12 clients at the outset of group. During sessions, a team of two therapists (one woman and one man) covered the following general topics: motivation to change, crisis management, anger-management, and relationships skill alternatives to coercion and violence. At least one therapist in each group had previous experience with intimate partner violence (IPV) treatment for perpetrators and held a master’s degree in psychology or equivalent training. More details on procedures for the pre-treatment data collection, the treatment protocol, and treatment uptake and completion can be found in a previous publication (Murphy et al., 2007). Trained undergraduate and graduate research assistants obtained criminal recidivism data using participant names and other identifying information in the Maryland Judiciary Case Search as described above.
Data Analyses
ANOVA was used to test for anger group differences in recidivism and correlations were used to examine associations between STAXI scale scores and recidivism. Criminal recidivism variables were logarithmically transformed if skew or kurtosis values reflected substantial deviation from normality (skewness above 2.0 and/or kurtosis above 7.0; Curran, West, & Finch, 1996). Variables with distributions that continued to contain pronounced skew or kurtosis after logarithmic transformation were rank order transformed. Using these guidelines, for the 8-year period after treatment initiation, IPA was not transformed, GV was logarithmically transformed, and OPOI was rank order transformed in all subsequent analyses. None of the criminal history variables coded for the 5 years prior to treatment initiation were transformed. OPOI during the 5 years before treatment exceeded skew of 2.0 and kurtosis of 7.0 (Curran et al., 1996). However, transformation was not an option to reduce skew or kurtosis as OPOI incident counts ranged only from 0 to 1, and therefore logarithmic or rank order transformations did not alter skew or kurtosis.
Results
During the 5 years prior to treatment initiation, 37.12% of participants had one or more instance of IPA, 50% had one or more of GV, and 4.55% had one or more instance of OPOI. Over the subsequent 8-year period, 25.76% of participants had one or more instance of IPA, 23.48% had one or more instance of GV, and 13.64% had one or more instance of OPOI.
Analyses identified an overall significant group difference among the three Anger Problem Profile groups in two of the three measures of recidivism. Omnibus differences between groups were found for GV and OPOI but not for IPA (see Table 1). In follow-up analyses, the PA group, in contrast to the NA group, had significantly more instances of GV recidivism, t(127) = 2.48, p = .02, and OPOI recidivism, t(127) = 2.80, p = .01. Other group contrasts for GV indicated no significant differences between the LAC and NA, t(127) = 0.85, p = .39, or PA, t(127) = −1.65, p = .10 groups. Additional group contrasts for OPOI indicated no significant differences between the LAC and NA, t(127) = 1.62, p = .11, or PA, t(127) = −1.37, p = .17, groups.
Analysis of Variance for Anger Group Differences in Recidivism.
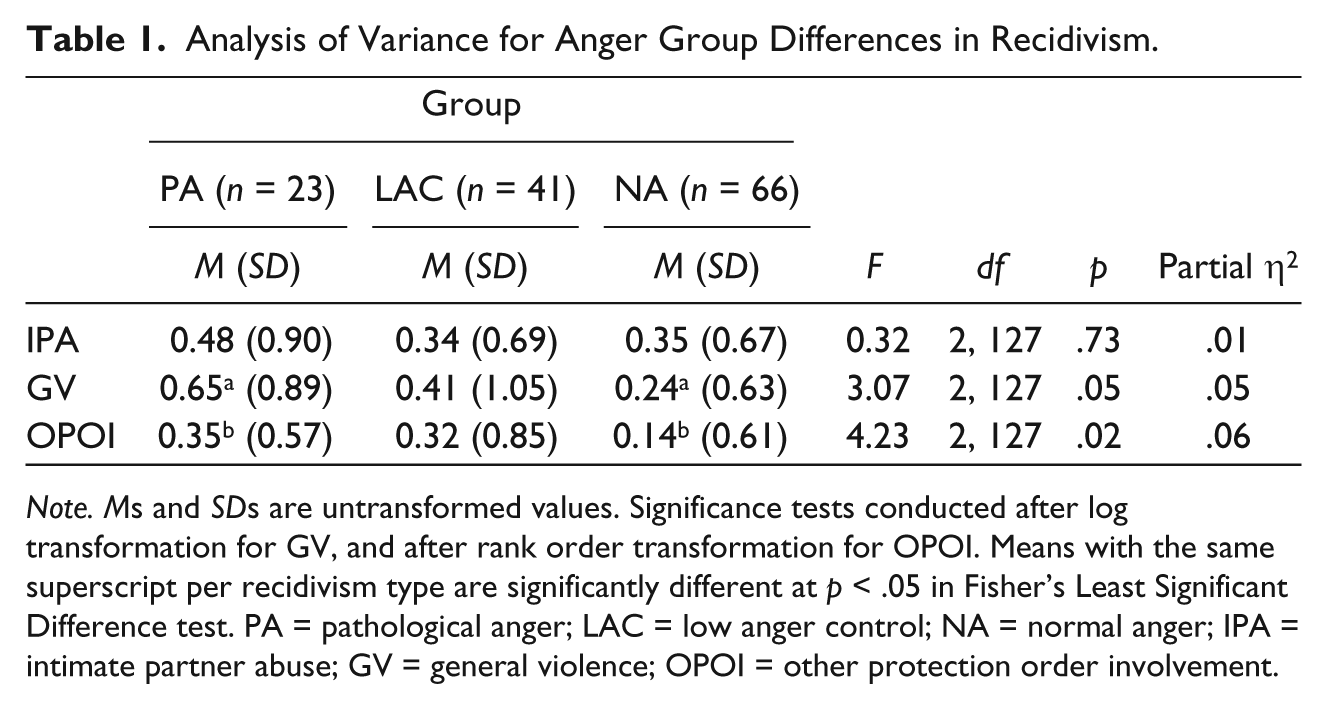
Note. Ms and SDs are untransformed values. Significance tests conducted after log transformation for GV, and after rank order transformation for OPOI. Means with the same superscript per recidivism type are significantly different at p < .05 in Fisher’s Least Significant Difference test. PA = pathological anger; LAC = low anger control; NA = normal anger; IPA = intimate partner abuse; GV = general violence; OPOI = other protection order involvement.
For the correlations between STAXI scales, assessed as continuous variables, and criminal recidivism, 12 of 15 correlations were in the predicted direction (see Table 2). Eleven correlations were greater than the .10 threshold for a small effect (Cohen, 1988), 2 correlations can be thought to display a trend toward statistical significance (i.e., had a p value between .05 and .10 in a two-tailed test with the effect in the expected direction), and 2 correlations were significant at p < .05. The specific associations interpreted as trends were Trait Anger with GV and Anger Out with OPOI. The significant correlations were Anger Control with GV and Anger Expression with GV. Overall, the results for continuous variable measures of anger were mixed but provide some support for the predicted association between anger problems measured at program intake and criminal recidivism over the subsequent 8-year period. In general, the associations with STAXI scales appear to be stronger for GV than for the two indicators of relationship-specific offenses.
Relations Between STAXI Scales and Long-Term Recidivism.
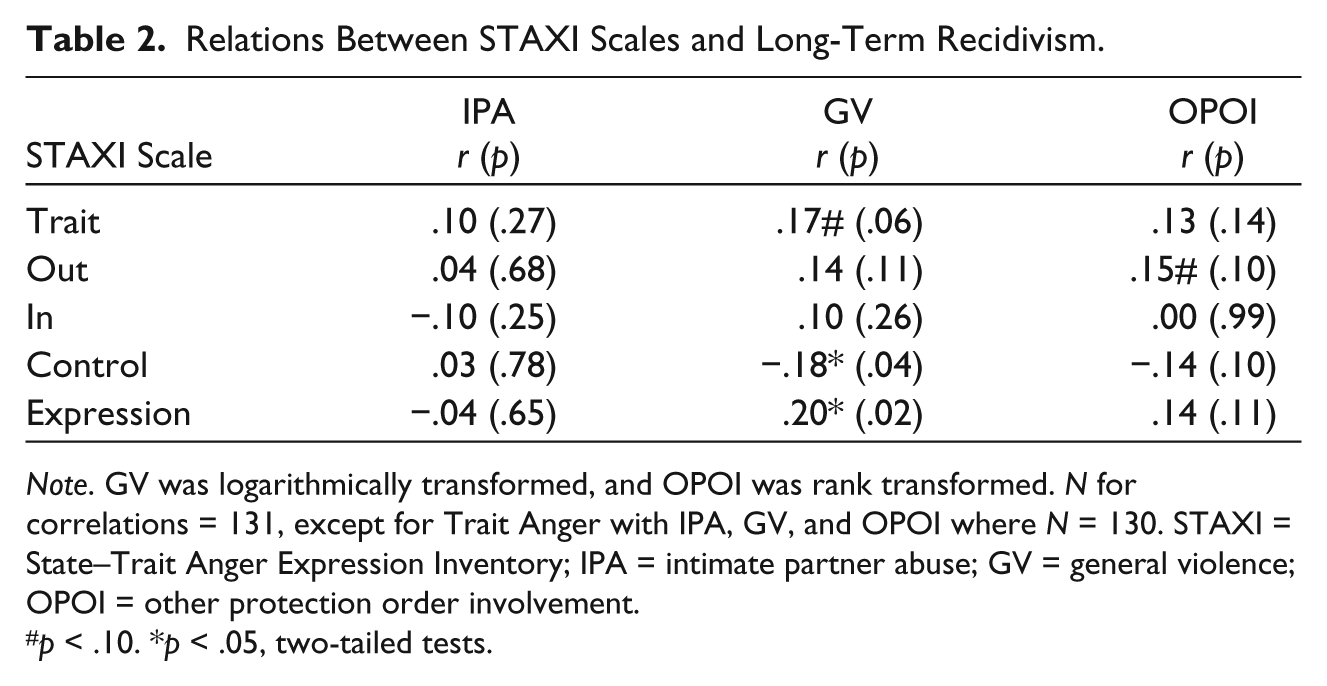
Note. GV was logarithmically transformed, and OPOI was rank transformed. N for correlations = 131, except for Trait Anger with IPA, GV, and OPOI where N = 130. STAXI = State–Trait Anger Expression Inventory; IPA = intimate partner abuse; GV = general violence; OPOI = other protection order involvement.
p < .10. *p < .05, two-tailed tests.
Additional analyses were conducted to investigate associations between anger problems at program intake and criminal involvement before treatment initiation. Analyses indicated no significant or marginally significant differences among Anger Problem Profile groups for any of the three measures of criminal history (see Table 3). In addition, there were no statistically significant or marginally significant correlations between STAXI scales at program intake and prior criminal history (rs = −.14 to .11). These findings suggest that anger problems assessed at program intake are a specific indicator of treatment response, not merely a marker for long-standing and persistent criminal difficulties.
Analysis of Variance for Anger Group Differences in Criminal History Prior to Treatment Initiation.
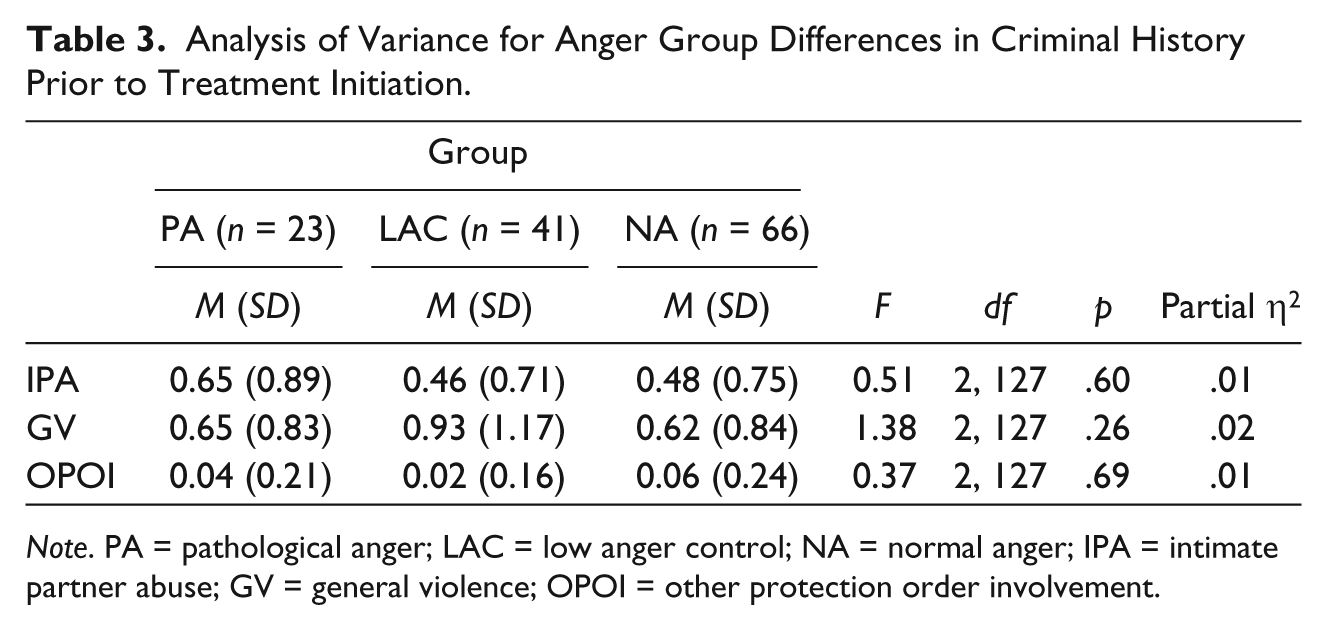
Note. PA = pathological anger; LAC = low anger control; NA = normal anger; IPA = intimate partner abuse; GV = general violence; OPOI = other protection order involvement.
Discussion
The main goal was to determine whether anger problems, assessed at program intake, predict partner violent men’s response to a group cognitive-behavioral intervention for IPV perpetration. The study provides a unique contribution by examining criminal recidivism during an 8-year period after the initiation of IPV treatment services. The results identified important differences in long-term treatment outcome among groups with distinct anger problem profiles. Specific anger scales from STAXI also had predictive associations with criminal recidivism in the hypothesized direction, although only a small number of correlations were statistically significant.
As hypothesized, individuals with a PA profile on the STAXI had more criminal recidivism than those with NA, specifically a greater number of incidents of generalized violence and greater involvement with protection orders and protection order violations that were not accompanied by other criminal charges. These findings are consistent with previous research showing that individuals with problematic profiles across several anger scales engage in higher levels of partner abuse during a short-term follow-up after treatment (Eckhardt, Samper, & Murphy, 2008; Murphy et al., 2007). The current study extends previous findings by indicating that Anger Problem Profiles are relevant predictors of treatment outcome assessed through criminal justice involvement over an 8-year follow-up interval.
The standard agency treatment program available to current study participants used several common cognitive-behavioral therapy strategies to address conflict escalation, including time out, self-monitoring of thoughts, feelings, and behaviors in anger-inducing situations, and discussion of anger coping and re-appraisal strategies. Despite these efforts, treatment was least effective for individuals in the PA group in terms of preventing continued involvement with the criminal justice system.
It is important to note that significant prediction was found for GV and protection order involvement but not for criminal offenses that could be directly identified as partner abuse. The most likely explanation for this pattern of results involves limitations in the coding of partner abuse from available data in the criminal record. Specifically, criminal incidents were coded as partner abuse only when an intimate partner could be confirmed as the victim from the available information. It is likely that many relevant incidents were coded as GV due to incomplete or inadequate information on the victim in the criminal database. Although GV is not a primary focus of the intervention, many elements of the program address cognitive and behavioral changes that promote nonviolence both outside and within intimate relationships.
However, it is also possible that the treatment program, which focused primarily on relationship skills designed to prevent conflict escalation with intimate partners, disrupted the association between anger problems and IPA without altering the risk of more general forms of violence. However, the fact that anger problems also predicted future difficulties with protection orders (in the absence of other criminal charges to substantiated abuse) is inconsistent with this explanation, or may indicate that treatment had an intended effect on conflict escalation without sufficiently altering other less violent problem behaviors, such as unwanted contact after imposed separation.
Overall, the results comparing distinct anger profile groups were more impressive than predictive correlations for specific STAXI scales, suggesting that a general pattern of anger difficulties may be more important than specific anger dimensions in predicting recidivism. Overall, the magnitude of predictive correlations for STAXI scales was low. However, several interesting interpretations also arise from the specific STAXI scale correlations with the three indicators of recidivism. Similar to the anger profile findings, the strongest findings emerged for GV recidivism. Individuals with low scores on the Anger Control scale and high Anger Expression Composite scores had more GV recidivism. Interestingly, all these scales focus on how individuals respond when angry, rather than the general impression of one’s self as an angry person (measured by the Trait Anger scale), highlighting the need for greater attention to anger coping strategies in treatment. In addition, individuals with high anger expression may require extended monitoring or more intensive intervention services than other IPV perpetrators. Although less robust, four of five STAXI correlations were also in the predicted direction with protection order involvement, with the strongest association found for Anger Out and the weakest for Anger In. Our hierarchical coding strategy isolates protection order involvement that was not accompanied by other charges (e.g., assault) that would substantiate violence. This type of legal involvement may result from emotionally abusive or other adverse behavior during contact that is allowed by the protection order (e.g., during pickup or drop-off for child visitation), from adverse behavior during contact that was initiated or accepted by the victim (which is quite common despite the presence of a protection order), or from unwanted and disallowed contact experienced by the victim as harassing or intimidating, but not sufficient to have resulted in a specific charge of harassment, assault, or stalking. The results suggest that individuals who express their anger outward are at highest risk of ongoing complications related to protection orders.
In contrast, the lack of clear findings regarding STAXI scale prediction of IPA recidivism is somewhat surprising given theory suggesting that anger increases the likelihood of violence (Berkowitz, 1983, 1988, 1989) and consistent research linking anger and IPA (Barbour et al., 1998; Norlander & Eckhardt, 2005). A goal of treatment is to disrupt the link between anger and intimate partner violence and it is possible that treatment alters this association. Also, not all components of anger may be relevant to recidivism risk. Specifically, Anger In was inversely associated with IPA recidivism, suggesting that tendency to bottle up and suppress anger may not be as important in predicting recidivism as is the inability to control angry reactions (LAC) and the tendency to express anger outward.
Several notable limitations warrant consideration. First, the level of statistical power was modest for prediction of behavior over a lengthy follow-up period. In addition, correlations not reaching statistical significance must be interpreted with considerable caution, and patterns of findings are more important than isolated associations. Second, limitations in the available data on criminal recidivism compound the predictive challenge. Specifically, the recidivism data only assessed legal problems within the State of Maryland, and therefore acts of recidivism in other states and abusive incidents that did not come to the attention of the authorities were not detected. Along similar lines, no long-term data were available on participants’ residential status (e.g., whether and when they moved out of state), relationship status, or other changes (e.g., death) that may alter the probability of recidivism. Whereas detection of recidivism provides an affirmative indication of poor treatment outcome and ongoing societal costs, the absence of recidivism is an ambiguous indicator of favorable clinical outcome. Third, the predictive variable was limited to self-report. Future research should consider other sources of data on anger problems such as partner report or structured clinical interviews. Fourth, variables other than anger problems are likely important in predicting recidivism. However, a more extensive multivariate analysis of recidivism predictors was beyond the scope of this study. Finally, as a predictor of recidivism, anger may not be unique to partner violence offenders but may also predict recidivism in a variety of other criminal offenders. In fact, the extent to which intimate partner violence offenders are similar to general criminal offenders remains an important topic of debate among criminologists (Richards, Jennings, Tomsich, & Gover, 2014).
Conclusion and Future Directions
Together with previous research (Eckhardt et al., 2008; Murphy et al., 2007), the current study suggests that anger problems are an important factor underlying treatment response for perpetrators of IPV. These findings challenge policies banning the use of anger management as a key focus of partner violence intervention (Maiuro & Eberle, 2008; Maiuro et al., 2001). In substitution of ideology, empirical research on anger should guide policies regarding IPV interventions for perpetrators.
Many questions remain with respect to the specific mechanisms that can explain the poor treatment response for individuals with PA profiles. Early work using a social information processing framework identified distortions in the interpretation of partner intentions and biases favoring aggressive responses to challenging relationship situations as key factors in IPV perpetration (e.g., Holtzworth-Munroe & Anglin, 1991; Holtzworth-Munroe & Hutchinson, 1993). In the intervening years, important conceptual developments in social information processing have more explicitly integrated emotional processes (e.g., Crick & Dodge, 1994; Lemerise & Arsenio, 2000). These models help identify how anger arousal contributes to problematic social information processing and impedes the performance of adaptive and socially competent responses in line with interpersonal goals (Murphy, 2013). Future research is needed to elucidate specific processes relevant to the role of anger in IPV, including more molecular studies of how anger can disrupt relationship skill performance.
In addition, research is needed to determine whether treatments that specifically target emotion dysregulation may help IPV perpetrators with pronounced anger problems. Notably, Dialectical Behavior Therapy (DBT; Linehan, 1993) targets emotion regulation through mindfulness, distress tolerance, and interpersonal effectiveness skills. Researchers have argued for the usefulness of DBT in targeting partner abuse. Although we know of no controlled trial work, preliminary data from uncontrolled studies of DBT for partner violence are promising (Fruzetti & Levensky, 2000; Rathus, Cavuoto, & Passarelli, 2006). Acceptance and Commitment Therapy also supports emotion regulation and has been adapted for individuals with problematic anger (Eifert, McKay, & Forsyth, 2006). Both treatments use strategies to enhance mindfulness, which, when assessed as a trait dimension, is negatively correlated with both anger and aggression (Heppner et al., 2008). The present findings highlight the need for further research to elucidate the ways in which anger dysregulation negatively affects IPV intervention success, to refine clinical strategies to reduce anger dysregulation in this population, and to investigate these strategies in controlled clinical trials.
Footnotes
Acknowledgements
Special thanks to John Persampiere and Brian Jobe for organizing and supervising the coding of criminal outcome data, and to the many graduate student clinicians and undergraduate research assistants who provided support for the clinical service provision and data collection that made this project possible. We gratefully acknowledge the support of the staff of HopeWorks (formerly the Domestic Violence Center) of Howard County, Maryland. Special thanks to David Schultz and Robin Barry for their valuable feedback and suggestions for this project.
Authors’ Note
Portions of this project were presented at the 2013 annual convention of the Association for Behavioral and Cognitive Therapies, and the results were submitted by the first author in partial fulfillment of the requirements for the Masters of Arts Degree in Psychology at the University of Maryland, Baltimore County.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.