
Abstract
Intimate partner violence (IPV) is a major public health problem in the United States. While our understanding of this form of violence has grown substantially over the past several decades, the majority of research involving victims of IPV has focused almost exclusively on female heterosexual victims. Unfortunately, little attention has been paid to how this form of violence affects specific populations, such as gay and lesbian victims. It is possible that gay and lesbian victims may experience more maladaptive outcomes as a result of unique components of same-sex IPV, their sexual minority status in American society, and the lack of appropriate services tailored to victims of this violence. Using data from the second wave of the National Longitudinal Study of Adolescent to Adult Health, this study contributes to the research on gay and lesbian victims of IPV by investigating same-sex and opposite-sex adolescent victims’ experiences with depression, alcohol-related problems, marijuana use, violent delinquency, and property delinquency. Results indicate that opposite-sex victims experienced more depressive symptoms, alcohol problems, and marijuana use than non-victims and engaged in higher levels of violent and property delinquency than non-victims. IPV within the context of same-sex relationships led to more depressive symptoms and greater involvement in violent delinquency, with the impact of IPV on violent delinquency being greater for victims of same-sex IPV compared with opposite-sex IPV. The implications of this study could inform interventions for victims of same-sex IPV and lead to more comprehensive services to address the needs of gay and lesbian victims of this violence.
Keywords
Intimate partner violence (IPV) is a major public health problem in the United States. More than one in three women (35.6%) and more than one in four men (28.5%) have experienced rape, physical violence, and/or stalking by an intimate partner in their lifetime (Black et al., 2011). Unfortunately, determining the violence experienced by adolescents in dating relationships is more difficult, as studies have reported quite disparate estimates. For studies using separate measures of physical and sexual victimization, estimates of physical victimization among girls range from 8% to 57% and 6% to 38% among boys. For sexual victimization, estimates fall between 14% and 43% for girls and 0.3% and 36% for boys (Hickman, Jaycox, & Aronoff, 2004). Fortunately, our understanding of this form of violence has grown substantially over the past several decades. Despite the large body of research devoted to the causes and consequences of IPV, the majority of research involving victims of IPV has focused almost exclusively on female heterosexual victims. Less is known about how this form of violence affects specific populations, such as gay and lesbian victims.
Research is beginning to emerge that examines the experiences of gay and lesbian victims of IPV. Much of this research has focused on the incidence and/or prevalence of this sort of violence in lesbian, gay, bisexual, and transgender (LGBT) communities (Alexander, 2002; Freedner, Freed, Yang, & Austin, 2002; Houston & McKirnan, 2007; Messinger, 2011; Turell, 2000; Walters, Chen, & Breiding, 2013) and the circumstances and obstacles victims of same-sex IPV may face that are unique to their sexual minority status (Brown, 2008; Elliot, 1996; Rohrbaugh, 2006; Sorenson & Thomas, 2009). While the results of these inquiries are promising in discovering the experiences of same-sex victims, more research needs to be done to develop this knowledge base.
For example, numerous studies have discovered that many heterosexual victims of IPV experience psychological and behavioral problems; however, very few studies have examined these phenomena for same-sex victims of IPV. It is possible that gay and lesbian victims may experience more maladaptive outcomes as a result of unique components of same-sex IPV, their sexual minority status in American society, and the lack of appropriate services tailored to victims of this violence. Using data from the second wave of the National Longitudinal Study of Adolescent Health (hereafter referred to as Add Health), this study contributes to the research on gay and lesbian victims of IPV by investigating same-sex and opposite-sex adolescent victims’ experiences with depression, alcohol-related problems, marijuana use, violent delinquency, and property delinquency. The implications of this study could inform interventions for victims of same-sex IPV and lead to more comprehensive services to address the needs of gay and lesbian victims of this violence.
Same-Sex IPV
The term “intimate partner violence” describes physical violence, sexual violence, threats of physical or sexual violence, and/or psychological/emotional abuse by current and former spouses and dating partners (Black et al., 2011; Centers for Disease Control and Prevention [CDC], 2012). This is inclusive of any intimate relationship regardless of the couples’ marital status, age, or gender. Thus, this type of violence can occur among heterosexual or same-sex couples and does not require sexual intimacy (Saltzman, Fanslow, McMahon, & Shelley, 2002). Similarly, dating violence is physical, sexual, or psychological violence that occurs within the context of a dating relationship (CDC, 2014). Although empirical research of IPV and dating violence between heterosexual partners has steadily increased since the 1970s, research regarding this type of violence between same-sex partners did not emerge until many decades later (Renzetti, 1992). Since then, there has been slow development of this knowledge base. Research that has emerged has generally examined the prevalence of same-sex IPV (often comparing these rates with heterosexual couples) and discussed the unique circumstances and obstacles victims of same-sex IPV may experience due to their minority status.
Prevalence of Same-Sex IPV
To date, research exploring same-sex IPV has reported inconsistent results regarding the extent of this problem in the LGBT community. This is likely due to the difficulty researchers have studying this marginalized population. For example, prevalence of IPV in same-sex relationships can vary depending on study methodologies (L. Burke & Follingstad, 1999). This includes whether or how violence is defined and measured, the time frame examined, specific partners, sampling techniques, and sample size. Furthermore, these estimates may be affected by how sexual orientation is defined. The most challenging aspect of studying this type of violence is obtaining a representative sample, as even studies with large samples have relied on non-random sampling methods (Alexander, 2002; L. Burke & Follingstad, 1999; T. Burke, Jordan, & Owen, 2002). For example, typical recruitment of study participants is done through LGBT publications, organizations, and activities (L. Burke & Follingstad, 1999; Eaton et al., 2008; Freedner et al., 2002; Houston & McKirnan, 2007). Therefore, this may exclude potential participants within the community who are not involved in or exposed to those entities or activities as well as individuals who are not “out” as gay or lesbian but are involved in the same-sex relationship.
Despite these methodological issues, important research has emerged to illuminate the prevalence of IPV among gay men, lesbians, and bisexual women. These studies illustrate that prevalence rates of same-sex IPV are comparable with or higher than those of heterosexuals (Alexander, 2002; Freedner et al., 2002; Houston & McKirnan, 2007; Messinger, 2011; Turell, 2000; Walters et al., 2013). For example, Balsam, Rothblum, and Beauchaine (2005) investigated the prevalence of self-reported psychological, physical, and sexual abuse in childhood and adulthood in a sample of 557 lesbian/gay, 163 bisexual, and 525 heterosexual adults. Sexual orientation was found to be a significant predictor of most of the victimization variables. Specifically, LGB participants reported more lifetime psychological maltreatment as adults than their heterosexual counterparts, and were more likely to report at least one physical assault by a partner (Balsam et al., 2005).
Although these studies provide us an alarming picture of the victimization experiences of LGB individuals, there remain issues regarding how generalizable these results are due to non-probability samples. To address this, several studies have emerged that examine nationally representative samples (Halpern, Young, Waller, Martin, & Kupper, 2004; Messinger, 2011; Walters et al., 2013). For instance, Halpern and colleagues (2004) used the Add Health data to investigate the prevalence of psychosocial and physical IPV between adolescents in same-sex relationships. Almost a quarter of the respondents experienced any violence and 21.3% of the respondents experienced psychological victimization. Thirteen percent of respondents reported only psychological victimization and 11% reported only physical victimization or both.
In further support of the gravity of the issue, another nationally representative survey collected the experiences of sexual violence, stalking, and IPV among adult men and women in the United States (Walters et al., 2013). The study found that 32.3% of heterosexual women, 56.9% of bisexual women, and 40.4% of lesbian women had reported experiencing physical violence within the context of an intimate partner relationship at least once in their lifetime. For men, 28.7% of heterosexual men, 37.3% of bisexual men, and 25.2% of gay men had experienced physical violence by an intimate partner at least once during their lifetime (Walters et al., 2013).
This study also examined lifetime prevalence of psychological aggression by an intimate partner. Examples of psychologically aggressive behaviors included: being called names such as ugly, fat, crazy, or stupid; witnessing an intimate partner act angry in a way that seemed dangerous; being insulted, humiliated, or made fun of; and made threats to physically harm the victim. Nearly one half of heterosexual women (47.5%), 7 in 10 bisexual women (76.2%), and 6 in 10 lesbian women (63.0%) experienced this form of aggression. Furthermore, approximately 49% of heterosexual men, 53% of bisexual men, and 60% of gay men reported experiencing psychological aggression in an intimate relationship (Walters et al., 2013). While these studies provide evidence that IPV is a serious public problem for both the heterosexual and LGBT communities, they speak very little to the unique circumstances that may occur in an abusive relationship that are exclusive to gay and lesbian victims (Brown, 2008; Elliot, 1996; Rohrbaugh, 2006; Sorenson & Thomas, 2009).
Unfortunately, most studies of IPV in the LGBT community focus exclusively on adults, and most studies of teen dating violence fail to take into account respondents’ sexual orientation or gender identity. The availability of limited data on lesbian, gay, bisexual, transgender, queer (LGBTQ) teen dating violence, however, is cause for concern. For example, Dank, Lachman, Zweig, and Yahner (2014) conducted a cross-sectional anonymous survey of 5,647 youth (51% female, 74% White) from 10 schools, of which 3,745 reported currently being in a dating relationship or having been in one during the prior year. The results showed significantly higher rates of dating violence among LGB youth than among non-LGB youth. While 29% of heterosexual youth surveyed reported being physically abused by dating partners, approximately 43% of LGB youth reported the same. The rates of sexual victimization for LGB respondents were nearly double those of heterosexual youth (23.2% vs. 12.3%, respectively).
Another study conducted by Freedner and colleagues (2002) set out to describe the prevalence of dating violence experienced by gay, lesbian, bisexual, and heterosexual youth. A convenience sample of 521 adolescents who self-identified as gay, lesbian, bisexual, or heterosexual were asked to complete a survey regarding lifetime dating violence. Results indicated that dating violence was prevalent in all groups, regardless of sexual orientation, with very few statistically significant differences. When gender and sexual orientation were taken into account, bisexual males were at a greater risk of at least one form of IPV (57.1%) compared with their gay male (44.6%) and heterosexual male (28.6%) counterparts. The examination of the women in the sample revealed that there were no significant differences between lesbians (43.4%), bisexual women (38.3%), and heterosexual women (32.4%) for at least one type of IPV.
The Unique Experiences of Same-Sex Victims
Beyond the discovery and comparison of prevalence rates of IPV in the LGBT community, one must examine this violence in the context of a same-sex relationship. Due to heterosexism and societal homophobia, same-sex victims of IPV experience situations that are not experienced by heterosexual victims (Brown, 2008; Elliot, 1996; Rohrbaugh, 2006; Sorenson & Thomas, 2009). Unlike heterosexual victims, same-sex victims of IPV may contend with a societal belief that their lives and relationships are not acceptable (Balsam & Szymanski, 2005). The impact of this oppressive cultural belief on an individual has been referred to as “minority stress” (Balsam & Szymanski, 2005; Brown, 2008; Carvalho, Lewis, Derlega, Winstead, & Viggiano, 2011; DiPlacido, 1998; Meyer, 2003). In the LGBT community, minority stress is a psychological strain that results from being a member of a sexual minority that is stigmatized and marginalized (Brooks, 1981). For LGBT individuals, minority stress can result from external stressors, such as the denial of civil rights, discrimination, and hate crimes, as well as internal stressors, such as internalized homophobia and identity concealment (Balsam & Szymanski, 2005; Carvalho et al., 2011; DiPlacido, 1998; Meyer, 2003; Rohrbaugh, 2006).
Internalized homophobia involves an individual internalizing society’s negative messages about one’s sexual orientation (Carvalho et al., 2011). Concealing one’s identity as gay, lesbian, or bisexual is associated with internalized homophobia (Herek, Gillis, & Cogan, 2009; Lewis, Derlega, Griffin, & Krowinski, 2003). One may conceal his or her identity as a sexual minority for fear of the denunciation of family members, friends, coworkers, and society in general. However, while concealing one’s identity may reduce the likelihood of rejection from others, it also restricts access to support and puts pressure on the individual to live a life in isolation (Bornstein, Fawcett, Sullivan, Senturia, & Shiu-Thornton, 2006; Carvalho et al., 2011; Elliot, 1996).
Some research has emerged that investigates the role of minority stress in same-sex IPV perpetration and victimization (Balsam & Szymanski, 2005; Carvalho et al., 2011; Freedner et al., 2002). Balsam and Szymanski (2005) examined how stress as living as a lesbian or bisexual woman correlated with relationship quality and domestic violence in a sample of 272 predominantly White lesbian and bisexual women. Results indicated that minority stress variables (internalized homophobia and discrimination) were associated with lower relationship quality and both domestic violence perpetration and victimization.
Minority stress, internalized homophobia, and identity concealment are factors that may affect the perpetration and victimization experiences of same-sex IPV. For example, perpetrators may use the awareness of fear and hatred of gays and lesbians by mainstream society to convince the victim that it would be dangerous to reach out to others for help. They may also perpetuate and utilize the invisibility of homosexual relationships to define relationship norms. Furthermore, the perpetrator may employ this cultural invisibility to isolate the victim and reinforce control (Roe & Jagodinsky, n.d.).
Another behavior the perpetrator may engage in is threatening to “out” the victim if his or her family, friends, or coworkers are not aware of his or her sexual orientation (Elliot, 1996; Kubicek, McNeeley, & Collins, 2015; Roe & Jagodinsky, n.d.; Rohrbaugh, 2006; Sorenson & Thomas, 2009). For example, Freedner and colleagues (2002) conducted the first study to specifically examine threats of outing as a type of abuse unique to LGBT populations. They found that bisexual males were more than 5 times more likely and bisexual females were more than 4 times more likely than either gay male or lesbian adolescents to report being threatened with outing by a partner (Freedner et al., 2002). Following this, if the victim has children, the perpetrator may threaten to reveal the victim’s sexual orientation to children to jeopardize the parent–child relationship or threaten to tell an ex-spouse or authorities that he or she is gay or lesbian, so they will take the children (Roe & Jagodinsky, n.d.; Rohrbaugh, 2006).
Perpetrators may also use techniques that invalidate the experience of the victim. The abuser may accuse the victim of “mutual abuse” or if the violence occurs in the context of a lesbian relationship, the victim may be told that “women can’t abuse women.” Furthermore, the victim may be told that no one will believe them because they are gay or lesbian (Roe & Jagodinsky, n.d.). Indeed, these unique circumstances may affect the help-seeking behaviors of these victims (Bornstein et al., 2006; Elliot, 1996; Kubicek et al., 2015; Renzetti, 1992; Rohrbaugh, 2006; Sorenson & Thomas, 2009) and may contribute to LGBT victims having different or worse reactions to IPV than their heterosexual counterparts.
Consequences of IPV
Research indicates that IPV victims can experience various psychological and behavioral problems. For example, IPV can lead to psychological issues for the victim, including low self-esteem, fear of intimacy, anxiety, inability to trust others, post-traumatic stress disorder (PTSD) symptoms, emotional detachment, sleep disturbances, flashbacks, and suicidal behavior (in females)(Black, 2011; CDC, n.d.; Coker et al., 2002; Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002; Silverman, Raj, Mucci, & Hathaway, 2001; Tjaden & Thoennes, 2000; Trevillion, Oram, & Howard, 2013). However, depression appears to be the most prevalent mental health sequela of IPV (Black, 2011; Campbell, 2002; Campbell, Kub, Belknap, & Templin, 1997; Campbell & Soeken, 1999; Cascardi, O’Leary, & Schlee, 1999; Golding, 1999; Krug et al., 2002; T. Roberts, Klein, & Fisher, 2003; Silva, McFarlane, Soeken, Parker, & Reel, 1997; Trevillion et al., 2013).
Much evidence exists that suggests there is an association between IPV victimization and depression. For example, Coker and colleagues (2002) assessed the physical and mental health consequences of IPV for men and women using data from the National Violence Against Women Survey (NVAWS). Results showed physical IPV victimization to be associated with an increased risk of depressive symptoms and chronic mental illness for men and women (Coker et al., 2002). In another study, Ehrensaft, Moffitt, and Caspi (2006) employed a prospective longitudinal research design to examine psychiatric disorder at age 18, partner abuse at ages 24 to 26, and psychiatric disorder again at age 26. Results revealed that partner abuse was a contributing source of psychiatric disorders among women but not among men. Specifically, controlling for previous mental health diagnoses, the authors found that involvement in a clinically abusive relationship predicted women’s risk of major depressive episodes (Ehrensaft et al., 2006). Research also suggests that there is a causal association between IPV and depression. T. Roberts and colleagues (2003) analyzed the longitudinal effect of abuse by an intimate partner on risk behavior among adolescents. They found significant associations between abuse by an intimate partner and longitudinal increases in depressed mood for both female and male adolescents (T. Roberts et al., 2003). In another study, Golding (1999) conducted a meta-analysis of research on IPV as a risk factor for mental health problems and discovered that the severity and duration of physical IPV are associated with the frequency and severity of depression. Furthermore, rates of depression decrease as time since the cessation of violence increases (Golding, 1999). While research has clearly established an association between IPV and mental health issues, particularly depression, there are other risk behaviors that have also been linked to IPV, such as substance abuse.
Many studies have shown that IPV is related to an increased risk of victim substance abuse (Black, 2011; CDC, n.d.; Coker et al., 2002; Krug et al., 2002; Plichta, 2004; T. Roberts & Klein, 2003; T. Roberts et al., 2003; Silverman et al., 2001). For example, T. Roberts and Klein (2003) examined the Add Health data to assess the association between abuse by an intimate partner and risk behaviors and found that history of abuse was significantly associated with substance abuse for females. Furthermore, abuse by an intimate partner had a significantly stronger association with substance abuse for females than for males (T. Roberts & Klein, 2003). Later, T. Roberts and colleagues (2003) used this same dataset to determine the longitudinal effect of abuse by an intimate partner. Results were similar to the previous study in that abuse by an intimate partner was associated with increased substance abuse for females (T. Roberts et al., 2003).
As the previous research indicates, in many cases, individuals who experience IPV victimization are more likely to engage in behavior that will cause harm to them or may bring them into contact with the juvenile or criminal justice system. Some studies have shown an association between a history of abuse by an intimate partner and violent behaviors (T. Roberts & Klein, 2003). For example, in a cross-sectional analysis of Wave 2 of the Add Health data, T. Roberts and Klein (2003) discovered that males and females who reported a history of abuse by an intimate partner were significantly more likely to report violent behavior. A longitudinal analysis of Waves 1 and 2 of these same data, however, found that IPV was not associated with increased violent behavior in either sex (T. Roberts et al., 2003).
Although the above research has reported important information regarding the effects of IPV, these studies did not take same-sex relationships into account. By not doing this, this may have confounded the results by assuming that all respondents were experiencing intimate partner violence in a heterosexual relationship. Of the few studies that exist, it has been found that gay and lesbian victims suffer similar, if not more serious, maladaptive outcomes than their heterosexual counterparts (Eaton et al., 2008; Houston & McKirnan, 2007; Walters et al., 2013). For instance, a study that examined the psychosocial characteristics and health problems of gay and bisexual men (n = 817) who experienced intimate partner abuse found that abused men were more likely to engage in substance abuse and to report depression and other mental health problems (Houston & McKirnan, 2007). In another study, Walters and colleagues (2013) assessed the impact IPV had on gay, lesbian, bisexual (male and female), and heterosexual (male and female) victims and found that approximately a third of heterosexual women (28.2%), more than half of bisexual women (57.4%), and a third of lesbian women (33.5%) who experienced IPV in their lifetime reported at least one negative impact (e.g., missed at least one day of school or work, were fearful, were concerned for their safety, experienced at least one PTSD symptom). Unfortunately, the sample sizes for gay and bisexual men were too small to calculate reliable estimates for the impact IPV had on this segment of the population (Walters et al., 2013).
The Current Study
This study endeavors to understand the consequences of IPV victimization for same-sex and opposite-sex victims. Previous studies that have used the Add Health data have examined victim risk behaviors associated with opposite-sex dating violence (T. Roberts & Klein, 2003; T. Roberts et al., 2003) and examined the prevalence of same-sex dating violence (Halpern et al., 2004). The current study is the first to disaggregate these data to examine maladaptive outcomes for same-sex and opposite-sex victims of IPV. This study seeks to determine whether experiencing IPV affects victims’ depression symptoms, alcohol-related problems, marijuana use, violent delinquency, and property delinquency and whether the findings differ for same-sex versus opposite-sex victims.
Method
Sample
The data for the current study come from the in-home interviews of Waves 1 and 2 of the Add Health. Add Health is a longitudinal, prospective study of youth in the United States from adolescence into adulthood. There are currently four waves of data available, with Waves 1 (ages 11-19) and 2 (ages 12-20) being collected predominantly during adolescence, and Waves 3 (ages 18-26) and 4 (ages 24-32) during early adulthood. The sample was selected through multi-stage sampling where researchers first targeted students from 132 middle and high schools, and then employed stratified sampling methods to select students for in-home interviews. A total of 20,745 youth completed in-home interviews in Wave 1, approximately 15,000 in Wave 2, and a total of 15,170 respondents in Wave 3. More information on the sampling techniques of the Add Health study is available from Harris et al. (2003). The current study examines the effects of adolescent IPV in Wave 2 on adolescent depressive symptoms, substance use, and delinquency in Wave 2 among non-married respondents reporting opposite-sex relationships (n = 9,602) and any involvement in same-sex relationships (n = 261). Approximately 32% of respondents (n = 4,778) did not report a romantic or sexual relationship within the past 18 months and were thus removed from the analytic dataset.
A note should be made on the temporal ordering of the variables. We chose to concurrently examine IPV and maladaptive behaviors since the stressful life events literature shows that interpersonal violence often has an immediate effect on one’s behavior and psychological functioning (Kendler, Karkowski, & Prescott, 1999); thus, one would expect the effects of IPV to emerge shortly after the incident or to occur within Wave 2. Also, IPV was not assessed during the Wave 1 interviews. As there were no multiple measurements in Wave 2, it is quite possible that drug use and antisocial behavior preceded one’s victimization. To account for this possibility, we included control variables for problematic behavior in Wave 1.
Measures
IPV in same-sex and opposite-sex relationships
IPV for same-sex and opposite-sex relationships was measured using three pieces of information in the dataset: (a) information on youth’s romantic and sexual relationships within the past 18 months (no relationship vs. a relationship reported), (b) the gender of respondents’ partner(s), and (c) five items from the Conflict Tactics Scale for each romantic and sexual relationship reported within the past 18 months. Identification of same-sex or opposite-sex relationships was made using information on the participant’s gender and the gender of their last three romantic partners and last three sexual partners (i.e., a total of six relationships). If the gender of the reported partner was the same as the gender of the respondent, then the relationship was classified as same-sex relationship. If the gender of the reported romantic or sexual partner was opposite to the gender of the respondent, then the relationship was classified as opposite-sex relationship. We chose to identify opposite sex and same sex as a characteristic of the relationship, rather than a characteristic of an individual because (a) approximately 100 individuals had reported relationships with members of the opposite sex and same sex (thus same sex and opposite sex were not mutually exclusive) and (b) anecdotally, there are questions on how individuals may identify their sexual orientation when they typically prefer one sex but have had relationships with members of the other sex; some individuals may identify as bisexual, whereas other individuals may identify themselves as heterosexual (who had a same-sex relationship or vice versa). Approximately 97% (n = 9,602) respondents reported that they only had opposite-sex relationships for their last three romantic relationships or sexual relationships, whereas 2.6% (n = 260) youth noted that they had any same-sex relationship. Of the 260 respondents, 120 individuals (46%) noted that they had both opposite-sex and same-sex relationships, whereas 141 youth (54%) reported that they only had same-sex relationships.
During Wave 2, respondents were asked whether they had been insulted, sworn at, threatened with violence, pushed or shoved, and had something thrown at them from their last three romantic partners and last three sexual partners (who were not considered romantic partners) within the past 18 months. For each of the five items from the six relationships, we identified whether the IPV event (a) occurred or did not occur and (b) occurred (or did not) within the context of an opposite-sex or same-sex relationship. This information was then used to create two variables: (a) same-sex IPV and (b) opposite-sex IPV (0 = did not experience any IPV in any of the possible six relationships; 1 = experienced at least one form of IPV in at least one of their relationships).
Depressive symptoms
Depressive symptoms were assessed using a modified version of the Center for Epidemiologic Studies–Depression (CES-D; Radloff, 1977) scale. The original CES-D is a 20-item scale that has been shown to be a reliable and valid measure of depressive symptoms across age groups (Radloff, 1991) and across ethnicities (R. E. Roberts, 1980). The modified CES-D scale used in the current analyses uses 19 measures from the original scale. The original item that was not asked by Add Health researchers was the item “My sleep was restless.” Youth were asked to rate on a 4-point scale (0 = never, 1 = sometimes, 2 = a lot of the time, 3 = most of the time or all of the time) how often they had experienced various negative affect, interpersonal problems, somatic complaints, and a lack of positive affect within the past 7 days. Responses were summed to form a composite scale of depressive symptoms (ranging from 0-56), where higher scores reflected greater depressive symptoms (αfull = .87).
We also created a dichotomous variable to categorize those respondents only involved in heterosexual relationships and those with any involvement in same-sex relationships. This variable was then used to examine whether the measurement properties of the scales varied by individuals’ romantic and sexual involvement with same-sex and opposite-sex youth. The factor structure and reliability of the scale did not appear to vary between those reporting any involvement in same-sex relationships (αsame = .87) and those reporting only opposite-sex relationships (αopposite = .87).
Alcohol-related problems
Alcohol-related problems were assessed with items inquiring about the negative and harmful consequences that resulted from youth’s consumption of alcohol. This conceptualization of alcohol abuse is similar to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria for alcohol abuse. During Wave 2, respondents were asked how often during the past 12 months have they had the following nine problems because of drinking: gotten into trouble with parents, problems at work or school, problems with friends, problems with their dating partner, did something you later regretted, being hung over, being sick to one’s stomach, getting into a physical fight, and placing oneself in a sexual situation that they later regretted. Responses were rated on a 4-point scale: 0 = never, 1 = once, 2 = twice, 3 = 3 to 4 times, 4 = 5 or more times. Responses to the nine items were summed to form a composite scale of alcohol-related problems, where higher scores reflected more frequent alcohol-related problems (αfull = .82, αsame = .83, αopposite = .82).
Marijuana use
Adolescent marijuana use was assessed by asking youth how often they had smoked marijuana within the past 30 days. Responses were coded 0 to 30 times per month.
Violent delinquency
Youth were asked if within the past 12 months they had pulled a knife or gun on someone, they had shot or stabbed someone, or if they had threatened someone with a weapon (0 = no, 1 = yes).
Property delinquency
Property delinquency was measured with seven items, asking youth whether they had painted graffiti, damaged property, shoplifted, stolen a car, stolen something worth more than US$50, stolen something worth less than US$50, and burglarized a building within the past 12 months. Responses to the seven items were summed up to form a composite scale (αfull = .75, αsame = .82, αopposite = .75). To increase comparability between violent and property delinquency, the property delinquency scale was dichotomized (0 = no involvement, 1 = committed at least one type of property crime).
Control variables
The analyses controlled for ethnicity, gender, age, and prior levels of problematic behaviors. For ethnicity, we created two dummy variables, where Caucasians were the reference group: (a) Caucasian non-Hispanic = 0, African American non-Hispanic = 1 and (b) Caucasian non-Hispanic = 0, Hispanic = 1. Gender was coded as 0 = female and 1 = male. Age in Wave 2 was measured as a metric variable, with respondents ranging from 11 to 21, with an average age of 16.44. Finally, depressive symptoms, alcohol-related problems, marijuana use, violent delinquency, and property delinquency were assessed in Wave 1 with the same questions as those employed in the Wave 2 measures above. Due to the significant correlations between the Wave 1 measures (r = .110-.400), we conducted a factor analysis with principal components analysis in SPSS. A one-factor solution emerged explaining 45% of the variance between the measures and factor loadings of .50 to .78. The factor scores using the regression method were saved from the analyses and were used to summarize prior levels of problematic behavior as one variable.
Results
Univariate and Bivariate Statistics
The average age of the sample was 16.44 (SD = 1.57), with 47.6% of respondents being male, 22.1% African American non-Hispanic, and 17% Hispanic. Approximately 31% of the respondents reported experiencing IPV in an opposite-sex relationship, and 27.8% reported IPV in the same-sex relationship. Among the 105 respondents who had relationships with both same-sex and opposite-sex partners, 41.9% reported no victimization in either type of relationship, 15.2% reported victimization in same-sex relationships only, 31.4% reported victimization in opposite-sex relationships only, and 11.4% experienced dating violence in both opposite-sex and same-sex relationships.
In terms of the dependent variables, 8% of all respondents engaged in some form of violent delinquency during Wave 2, with a higher percentage (34.4%) reporting involvement in property delinquency at Wave 2. On average, youth used marijuana approximately 2 times within the past month (M = 1.87, SD = 5.95) and reported low levels of alcohol-related problems (M = 1.91, SD = 3.77, median = 0). The average level of depressive symptoms was 11.74 (SD = 7.72, median = 10), which is an average that is significantly lower than what was found in Radloff’s (1991) studies of high school students (M = 17.88) and junior high school students (M = 16.60), suggesting low levels of depression within the current sample. Overall, the descriptive statistics suggest that the majority of youth in the analytic sample are in the middle of adolescence and exhibit low to moderate levels of problematic behavior.
Table 1 shows the zero-order bivariate associations between IPV and concurrent problematic behaviors. Independent t tests from SPSS and effect sizes (ESs) from G*Power (Faul, Erdfelder, Lang, & Buchner, 2007) showed that the average level of depressive symptoms (t = 17.89, p < .001; ES = .40), alcohol-related problems (t = 14.21, p < .001; ES = .33), and marijuana use (t = 8.94, p < .001; ES = .21) was higher for youth who reported IPV within opposite-sex relationships compared with youth who did not experience violence. Furthermore, the prevalence of violent delinquency (χ2 = 130.55, p < .001; ES = .29) and property delinquency (χ2 = 184.79, p < .001; ES = .30) was higher among youth experiencing IPV in heterosexual relationships than those who did not report partner violence. The odds of engaging in violent delinquency or property delinquency were approximately 2 times higher for adolescents who experienced IPV in heterosexual relationships. According to Cohen’s (1988) criteria for small (t = .20, χ2 = .10), medium (t = .50, χ2 = .30), and large (t = .80, χ2 = .50) ESs, one can see that there is a small to moderate effect of IPV within heterosexual relationships on problematic behavior.
Zero-Order Associations Between Intimate Partner Violence and Problematic Behaviors.
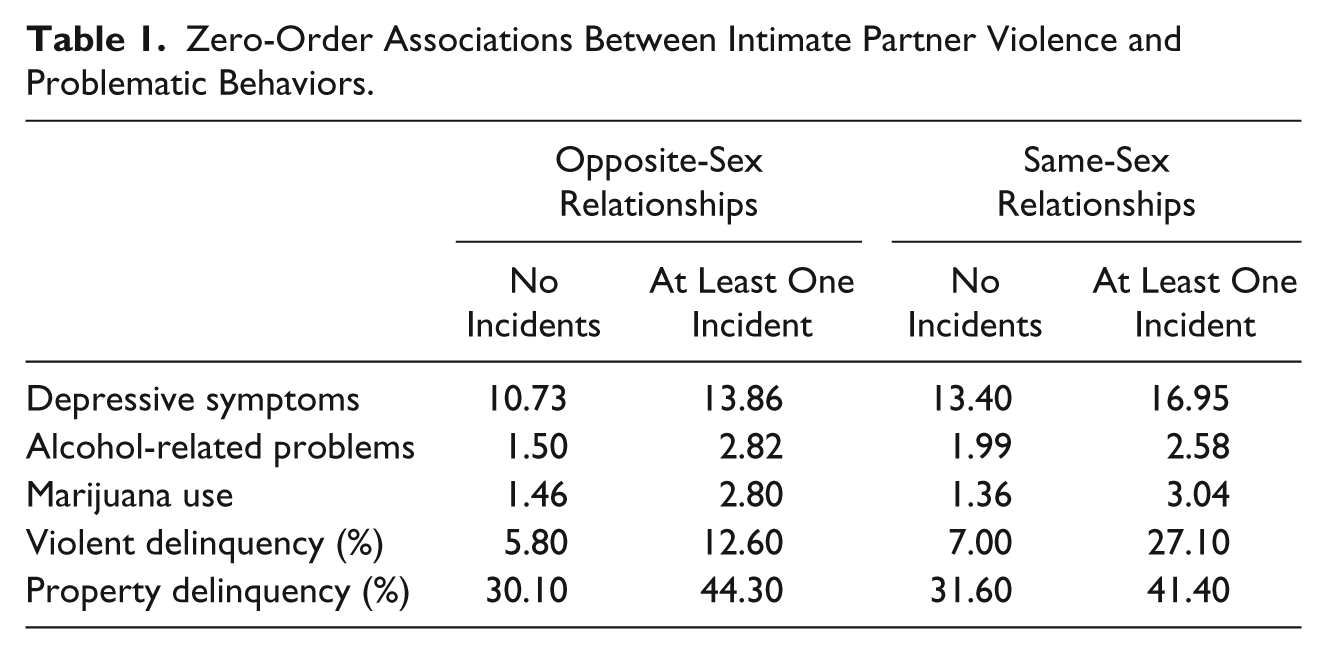
For those respondents with any involvement in same-sex relationships, t tests showed that IPV was only statistically associated with significantly higher levels of depressive symptoms (t = 2.50, p = .014; ES = .37), but not with higher levels of marijuana use (t = 1.79, p = .076; ES = .27) or alcohol-related problems (t = 1.02, p = .306; ES = .13). While analyses from G*Power revealed that the analyses were underpowered to detect significant differences in marijuana use (51% power for .27 ES) and alcohol-related problems (16% power for .13 ES) in t-test analyses, post hoc analyses of the nine alcohol problem items showed (a) no association of partner violence in same-sex relationships and the nine alcohol problem items using chi-square tests, and (b) all of the chi-squares were adequately powered (80+%) to detect an association if it did exist. Together, this suggests that there is a marginal association between same-sex partner violence and marijuana use, but partner violence is not related to higher levels of alcohol-related problems.
Turning to the delinquency measures, youth who reported IPV in same-sex relationships were almost 5 times more likely to engage in violent delinquency than youth who were not victimized (χ2 = 19.04, p < .001; ES = .78), 1 but prevalence of property offending was not higher among victims in same-sex relationships (χ2 = 2.20, p = .137; ES = .21). G*Power showed that the test for property offending was adequately powered (92% power) to detect a significant difference, and so it appears that violence within same-sex relationship does not translate into higher levels of property delinquency. Overall, same-sex IPV is associated with higher levels of depressive symptoms, violent delinquency, and perhaps marijuana use, but it does not significantly affect alcohol-related problems and property delinquency. 2
Multivariate Statistics
Regression models in STATA 9.1 were employed to examine whether IPV led to higher levels of problematic behaviors, after controlling for demographics and prior levels of antisocial behaviors. Poisson’s regression was used for depressive symptoms, negative binomial for alcohol-related problems and marijuana use, and logistic regression for violent delinquency and property delinquency. The results from the regression models are displayed in Tables 2 and 3. As shown in Table 2, IPV within heterosexual relationships was associated with increases in depressive symptoms, alcohol-related problems, marijuana use frequency, and prevalence of violent and property delinquency, above and beyond the effects of earlier involvement in maladaptive behaviors. In regard to the control variables, African American and Hispanic respondents reported greater depressive symptoms and violent delinquency, but lower levels of alcohol-related problems and marijuana use, relative to Caucasians. Older youth exhibited more symptoms of depression and more alcohol-related problems, but were less likely to engage in violent and property offending. Furthermore, males (relative to females) reported using marijuana more frequently, fewer depressive symptoms, and greater involvement in violent and property delinquency.
Multivariate Associations Between Intimate Partner Violence in an Opposite-Sex Relationship and Problematic Behaviors.
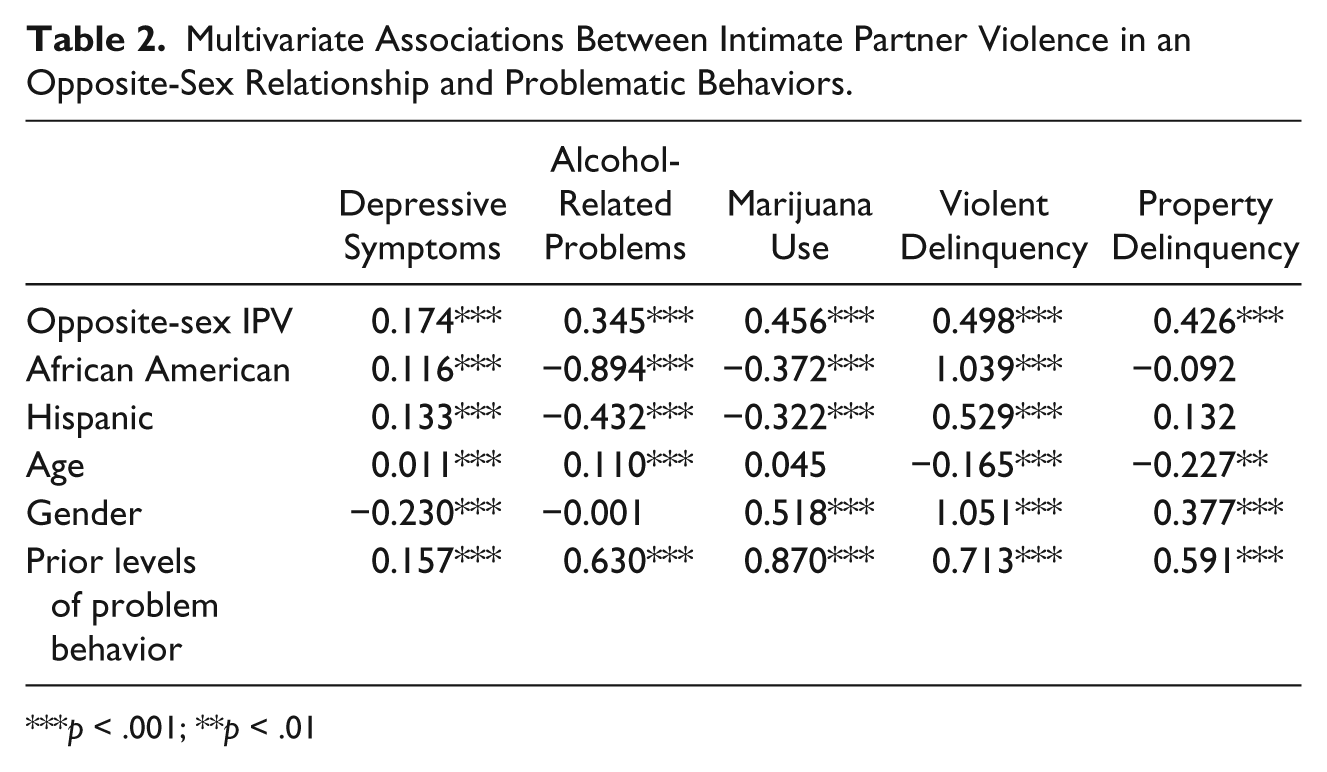
p < .001; **p < .01
Multivariate Associations Between Intimate Partner Violence in the Same-Sex Relationship and Problematic Behaviors.
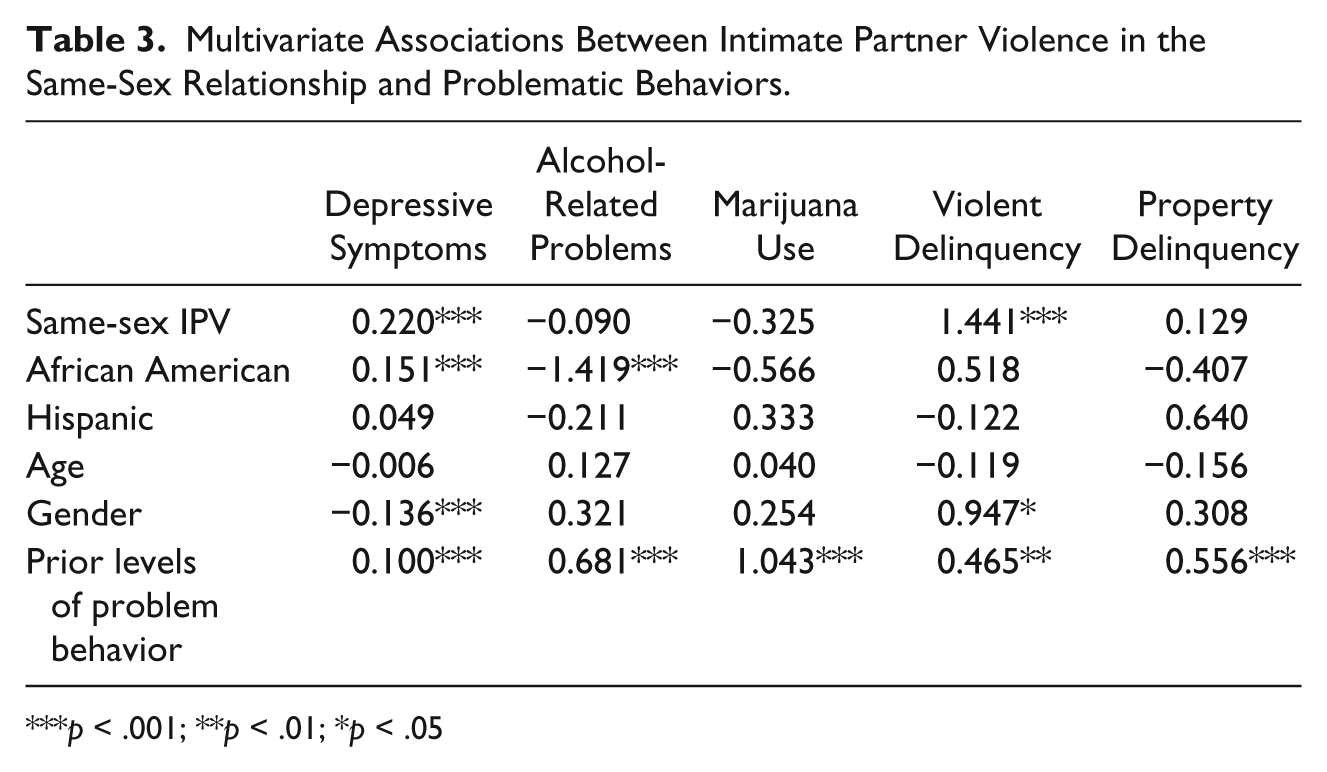
p < .001; **p < .01; *p < .05
Table 3 displays the regression results for the same-sex relationships. Similar to the bivariate analyses, IPV is associated with higher levels of depressive symptoms and violent offending controlling for demographics and prior behaviors, but it is not related to substance use or property delinquency. Among those who had same-sex relationships, males reported fewer depressive symptoms and greater involvement in violent delinquency than did females. Also, African Americans exhibited higher levels of depression than Caucasians and reported fewer problems related to alcohol consumption.
Discussion
The present study’s main focus was to examine the impact of IPV on same-sex and opposite-sex victims. As predicted, the consequences of IPV were contingent on whether the victim was in an opposite-sex or same-sex relationship. Furthermore, opposite-sex and same-sex victims differed in terms of which maladaptive outcomes were more prevalent.
Opposite-sex victims of IPV had more depressive symptoms, alcohol problems, and marijuana use than non-victims. These findings are consistent with previous research (Black, 2011; Campbell, 2002; Campbell et al., 1997; Campbell & Soeken, 1999; Cascardi et al., 1999; CDC, n.d.; Coker et al., 2002; Golding, 1999; Krug et al., 2002; Plichta, 2004; T. Roberts et al., 2003; Silva et al., 1997; Silverman et al., 2001; Trevillion et al., 2013). Furthermore, it was discovered that these victims also engaged in higher levels of violent and property delinquency, outcomes that have not been extensively explored in the previous research.
The consequences of IPV within the context of a same-sex relationship were somewhat different than the consequences of IPV in a heterosexual relationship, thus suggesting that there is an association between the type of relationship and the consequences of IPV. For those respondents with any involvement in a same-sex relationship, IPV was statistically associated with significantly higher levels of depression symptoms and violent delinquency, but not property offending and substance use. Youth who reported IPV in same-sex relationships were almost 5 times more likely to engage in violent delinquency than youth who were not victimized. These conclusions are further supported by secondary analyses (see Note 2), which showed that bisexual respondents experienced higher levels of depression and violent delinquency if IPV occurred within the same-sex relationship, but not within an opposite-sex relationship.
It is possible that the increased depressive symptoms and violent delinquency for same-sex victims may be a result of coping with victimization when very few resources are available to them. Indeed, research has found that current practices engaged in by domestic violence shelters may exclude lesbian and gay victims of IPV. For most programs and shelters, there is a tendency to use a heterosexual model as a reference for relationships. By doing so, the majority of battered women’s programs and shelters around the country serve only heterosexual female victims of IPV and are hesitant or not qualified to address the unique issues resulting from violence within lesbian relationships (Brown, 2008; Elliot, 1996; Sorenson & Thomas, 2009). In addition to female same-sex victims, there are little to no programs or shelters available to gay men (Lyon, Lane, & Menard, 2008). Furthermore, it has been found that many service provider staff have had little or no training in LGBT IPV and agencies/programs typically lack staff who have dedicated responsibilities to dealing with LGBT IPV (Ford, Slavin, Hilton, & Holt, 2013).
In addition to a lack of community resources for same-sex victims, many may become depressed because they cannot turn to counselors, teachers, family, or friends for support or help. Same-sex IPV may not be a topic that is openly discussed in a school setting; because of this, victims may be hesitant to seek help from adults at their school. Furthermore, school counselors and teachers may not be trained to address the victimization and related issues that are specific to LGBT relationships. In addition to this, friends or family may not know that the person is engaged in a same-sex relationship, so asking for help would consequentially “out” the person. Therefore, increased depression of these victims may be a result of the belief that there is little to no help available to them.
The increase of violent delinquency of same-sex victims may also be a product of believing that they cannot turn to police for help. Some research has found that police have often failed to recognize that incidents have occurred in the context of an intimate partnership, or police may misidentify the incident as “mutual battering” due to the misconception that the determination of an IPV incident is based on the sex of the victim (i.e., female heterosexual victim; Ciarlante & Fountain, 2010). Therefore, the “violent delinquency” the same-sex victims engaged in in this study may actually be acts of self-defense. Prior violent behavior was a control variable for the subjects in the sample, so this “violent delinquency” may be tapping into these victims fighting back against their abusers.
The current study expands on the literature base by showing that the consequences of IPV may differ whether it occurs within the context of a same-sex or opposite-sex relationship. While this is an important and timely discovery, there are a number of caveats to our findings. First, Wave 2 of the Add Health did not include information on respondents’ perpetration of IPV, and thus we were not able to explore how perpetration intersected with victimization. Research has shown that IPV may be perpetrated by both or just one partner, and that the risk factors and consequences of IPV may differ based upon one’s gender and whether the respondent is a victim, a perpetrator, or both (Magdol et al., 1997; Swan & Snow, 2003; Weston, Temple, & Marshall, 2005). Given that the data at this wave did not include information on perpetration, we were unable to examine the intersections between type of relationship, gender, and mutual IPV. Second, the current study did not explore how these findings varied by gender and ethnicity. A growing body of research shows that IPV experiences and consequences may depend upon one’s gender and ethnicity (Garcia, 2015).
With consideration to these precautions, the findings in the current study can be used to inform interventions and programs that have been developed or need to be developed for all victims of IPV, regardless of the type of relationship. Interventions that would help mitigate the consequences of IPV victimization for both opposite-sex and same-sex victims could include mental health treatment (in this case, for depression) as well as programs that teach effective coping skills, so individuals do not turn to substance abuse or violence to cope with their victimization. Although experiencing IPV victimization produced negative consequences for both groups examined in the study, same-sex victims experienced more severe consequences that were occurring in relationships treatment providers are just beginning to address and understand. Because of this, it is important to develop interventions for this population that incorporate an understanding of internalized homophobia and power relationships in same-sex relationships (Kubicek et al., 2015).
With such little attention being given to the victims of same-sex IPV, this study is one that can contribute to a small yet growing knowledge base and bring this issue “out in the open.” Regardless of the reason why these victims have been ignored by mainstream research and service providers, it is time to shed light on them and the difficulties they face, so that we may better tailor interventions and support networks to address this violence. By doing so, we will reduce IPV in the LGB community and the serious consequences that result from experiencing this sort of victimization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.