
Abstract
The global mental health ramifications of political violence and intimate partner violence (IPV) are well established. There also exists a growing body of evidence about the increased risks for IPV within situations of political violence. Yet, except for a few studies, there is little literature that simultaneously examines how political violence and IPV might result in unique risks for particular types of mental health sequela. Delineating possible divergent patterns between specific mental health conditions resulting from political violence and IPV takes on an increased urgency given that, although they are related, the two most commonly reported outcomes of these two types of violence—post-traumatic stress disorder (PTSD) and depression—not only require different types of treatment, but may in fact be generated or maintained by disparate paths. Using survey data from adult women in Palestine (n = 122), this study explores the relationships between IPV and political violence (both lifetime and past-month exposure) and tests their independent relationships to PTSD and depressive symptomology. After controlling for the other form of violence exposure, political violence was correlated with PTSD and not with depressive symptomology, while IPV was correlated with depressive symptomology and not with PTSD. Findings demonstrate that distinct forms of violence exposure might indeed be associated with specific mental health outcomes. Results illustrate the need to assess for both political violence and IPV when researching and designing interventions related to violence.
Introduction
In 2002, the World Health Organization (WHO) issued its first “World Report on Violence and Health,” which recognized violence as a major global public health issue. In the report, WHO defined violence as the deliberate use of power, physical force, or intentional deprivation (WHO, 2002). This rather broad definition of violence put forth by WHO reflected a move within violence research to acknowledge that violence not only causes injury and death but also poses fundamental burdens on physical and mental health, along with general quality of life (Krug, Mercy, Dahlberg, & Zwi, 2002; WHO, 2002). Among other types of violence, the report highlighted the implications of political violence, or violence aimed at achieving particular political goals, and intimate partner violence (IPV), or violence that occurs in the home within families and partnerships.
Since the Second World War, there have been almost 200 armed conflicts in the world (WHO, 2002). Estimates suggest that one third to one half of people exposed to political violence will endure some type of mental distress, particularly post-traumatic stress disorder (PTSD), although political violence is also implicated in other mental health sequela such as depression (de Jong, Komproe, & Van Ommeren, 2003; WHO, 2001). The mental health risks of political violence may be particularly acute for women, perhaps due in part to the differential threats women face within conflict settings, including increased stress related to care-giving (Al Gasseer, Dresden, Keeney, & Warren, 2004; Hobfoll, Mancini, Hall, Canetti, & Bonanno, 2011; Norris et al., 2002; United Nations Research Institute for Social Development [UNRISD], 2005).
Like political violence, IPV is a major concern for global mental health. In the first international systematic review of scientific data from 79 countries and 2 territories on the prevalence of physical or sexual IPV against women, WHO (2013a) concluded that one in three women have experienced either physical and/or sexual IPV. IPV significantly increases the odds of mental health disorders, particularly PTSD and depression (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Campbell, 2002; Cerdá, DiGangi, Galea, & Koenen, 2012; Fischbach & Herbert, 1997; García-Moreno, Jansen, Ellsberg, & Heise, 2005; Golding, 1999; Haj-Yahia, 2000a; Kaminer, Grimsrud, Myer, Stein, & Williams, 2008). An early meta-analysis of 18 studies of women exposed to IPV found a prevalence rate of depression of 47.6% (Golding, 1999). More recently, WHO’s (2013) meta-analysis of 6 studies concluded that IPV almost doubled the odds of depression (pooled odds ratio [OR] = 1.97, confidence interval [CI] = [1.56, 2.48]). Similarly, studies report rates of PTSD symptomology among women who have suffered from IPV that range, on the low end, from almost one in three all the way to 80%; Golding’s (1999) meta-analysis of 11 studies among women exposed to IPV found an overall prevalence rate of PTSD of 63.8%.
A small but increasing body of evidence suggests that political violence and IPV tend to co-occur (Al-Krenawi, Graham, & Sehwail, 2007; Human Rights Watch, 2006; Stark & Ager, 2011; Usta, Farver, & Zein, 2008; Vinck & Pham, 2013). In separate studies in South Africa and with immigrants in Boston, men who had been exposed to political violence were more than twice (and in one study, up to 6 times) as likely to perpetrate IPV than men who had not been exposed to political violence (Gupta et al., 2009; Gupta, Reed, Kelly, Stein, & Williams, 2012). In Palestine, a large-scale epidemiological study of more than 3,800 households found that men who were exposed to political violence, both direct and indirect (i.e., family exposure or affected economically by political violence), were between 40% and 123% more likely to perpetrate IPV, respectively, compared with men without the exposure (Clark et al., 2010). Scholars have drawn on multiple theories to explain the links between political violence and IPV from a variety of settings, including Palestine. These theories encompass ideas from social learning theory about the importance of social and cultural norms and the emphasis within stress and coping theories on how chronicity and overlapping adversity, along with accompanying loss of instrumental and psychological resources (Hobfoll, Hall, & Canetti, 2012), deteriorates mental health and overwhelms healthy modes of coping (Annan & Brier, 2010; Clark et al., 2010; Heath, Hall, Canetti, & Hobfoll, 2013; Jewkes, 2002; Nikolic-Ristanovic, 1996; WHO, 2002; Zannettino, 2012). Scholarship on the topic also draws together these two perspectives, highlighting how war (particularly its disempowering nature) interacts with existing structural factors (such as gender inequalities, poor infrastructure, unemployment, police system corruption, and poverty) to exacerbate IPV (Annan & Brier, 2010; Clark et al., 2010; Nikolic-Ristanovic, 1996). Whatever the explanation for the links between political violence and IPV (and likely there are several, interrelated causes), it appears these phenomena are highly prevalent, profoundly detrimental to women’s mental health, and tend to co-exist.
Despite the connections between, and health ramifications of, political violence and IPV, little is known about how political violence and IPV co-exist for the women who might experience them. Furthermore, we know little about how, after controlling for one form of violence exposure, the other form might pose unique risks to particular outcomes within women’s mental health. Two outcomes that are of particular interest are PTSD and depressive symptomology, which are often reported as consequences of violence. Although PTSD and depression often seem to be related, with one condition tending to increase the risk of the other (Breslau, Davis, Peterson, & Schultz, 2000; Devries et al., 2013), scholarship suggests that PTSD and depression may be generated or maintained by disparate paths (Cascardi, O’Leary, & Schlee, 1999; Shalev et al., 1998). For instance, Cascardi et al. (1999) found that, among women exposed to IPV, although the frequency of severe abuse predicted both PTSD and depression, tactics of dominance and isolation more readily predicted PTSD. On the contrary, low levels of marital accord (measured by indicators such as trust, closeness, and agreement on small and large matters) predicted depression (Cascardi et al., 1999).
Information on the potentially varied paths of the sequela of depression and PTSD resulting from distinct experiences of violence is an important area of investigation, for although both political violence and IPV are commonly connected to depression and PTSD, these two outcomes differ quite a bit with regard to both the nature and treatment of the respective problem. Depressive symptomology is a mood disorder characterized, in part, by the loss of interest or pleasure in daily activities, feelings of excessive guilt or worthlessness, fatigue, and changes in sleep, concentration, and activity (American Psychiatric Association [APA], 2000). Treatment for depression often focuses on cognitive behavioral techniques to address the ego dystonic thought processes contributing to depressed mood and group, individual, and family therapy to process adverse life events. PTSD, on the other contrary, is an anxiety disorder characterized by the re-experiencing of an extremely traumatic event accompanied by symptoms of increased arousal and by avoidance of stimuli associated with the trauma (APA, 2000). For PTSD, the treatment is targeted to address the underlying anxiety triggered by an external stimulus. Exposure therapy is often used to confront feared but otherwise safe objects, situations, thoughts, sensations, and memories with the goal of reducing fear and learning the external stimulus is not intrinsically dangerous (Foa, 2011).
Given the increased risk of IPV for women who are exposed to political violence, coupled with the varied implications for treatment of the distinct conditions of PTSD and depression, delineating the possible divergent patterns between the various mental health conditions resulting from both political violence and IPV takes on an increased urgency. Yet, with few exceptions (Kaminer et al., 2008; Vinck & Pham, 2013), there are limited studies that attempt to simultaneously examine how exposure to both political violence and IPV might result in unique risks for particular types of mental health sequela. In one of the few studies (a large-scale study of more than 4,000 adults in Liberia) that tested the relationship of both political violence and IPV to different mental health outcomes, each form of violence was independently associated with both PTSD and depression (Vinck & Pham, 2013). Using survey data from adult women in Palestine, this study explores the relationships between IPV and political violence and tests their independent relationships to distinct mental health outcomes: depressive symptomology and PTSD. We also explore the independent effects of IPV and political violence on a third outcome, distress, which reflects a variety of mental health conditions, including depression, PTSD, panic disorders, and substance abuse with serious impairment (Spies et al., 2009; Sunderland, Slade, Stewart, & Andrews, 2011).
Design and Method
The project is a collaborative research effort between a U.S.-based researcher and the Palestinian Medical Relief Society (PMRS), one of the oldest and largest health care nongovernmental organizations (NGOs) in Palestine. The Institutional Review Board at the University of Washington approved all study procedures. Surveys were collected in 2007 and 2008 from adult Palestinian women in eight districts in the West Bank (N = 122). The West Bank is well known for its history of protracted conflict and ongoing Israeli occupation of civilian areas (for a timeline of the issues and their relationships to health, see, for instance, Giacaman et al., 2009, and other articles in the ongoing Lancet series on health in Palestine). Respondents were recruited from Birzeit University and from general health and women’s clinics belonging to PMRS and the Palestinian Ministry of Health. Staff at these locations approached the potential participants with a prepared script that explained the study and its potential benefits and risks. Participants were recruited if they met the criteria of being a Palestinian woman over the age of 18. Random selection was not used in this study; this is purely a convenience sample. Those approached to participate in the study were told it was strictly voluntary and declining to take part will not affect their services in any way. Those who agreed to participate were consented following a standard script. Per data sharing agreements, data belong jointly to the entire research team.
Measures
The survey tool consists of 9 constructs and 150 questions. Professional translators in the West Bank translated the survey from English into Arabic; several PMRS staff members checked the accuracy of the translation. Survey development took 1 year and included consultation with a diverse international pool of experts in the fields of trauma and violence, resilience, the Israeli/Palestinian conflict, and mental health. The process of survey development included a focus group with Palestinians from the West Bank who were living temporarily in Seattle, Washington. Participants in this focus group pilot tested the survey and gave input on the items, the translation, the time required for completion, and ethical or emotional issues regarding the survey. To develop a sufficiently broad and detailed measure of political violence, focus group participants were asked to list the most influential experiences Palestinians encounter under the occupation. These answers were analyzed against those items in the survey.
IPV
The survey tool includes a 12-item measure of women’s exposure to IPV within the past 12 months; items are on a scale of 1 to 5 (1 = never; 2 = 1-2 times; 3 = 3-5 times; 4 = 6-10 times; 5 = 11 or more times). This measure is a modified index of that used with Palestinian women in the West Bank by Haj-Yahia (2000). Items include acts of control (in the past 12 months, has your husband not allowed independent behavior on various occasions?), acts of ridicule and humiliation (. . . ridiculed you, your behavior, relationships, or attitudes, or accused you of being a failure), threats of physical violence (. . . threatened to hit or throw something at you), and actual physical violence toward the woman, her environment, or the children (attacked you physically; thrown, smashed, hit, or kicked something; threatened to or actually beat up the children). The 12 items were summed up to create a composite index of exposure to IPV in the previous 12 months. All who filled out the IPV scale were included in the analyses, regardless of their marital status. This is because, for example, someone might not yet be married, and thus identify as single, but could already be experiencing abuse from a fiancé. Cronbach’s alpha for this scale as used in this study is .864.
Political violence
Within the 30-item index of exposure to political violence, questions focus on impingements to movement and activities of daily life (e.g., military checkpoints, having to change plans for school, wedding or travel due to the occupation or interrupted access to health and educational services due to the occupation). The index also includes acts that directly threaten physical and psychological well-being, such as home demolitions, witnessing or experiencing arrest or detainment, and being the victim of beatings or strip-searching by Israeli police or military. From the 30-item tool, two indices of political violence were developed: a measure consisting of 12 lifetime experiences of political violence (α = .745 for this study) and a measure of the frequency of 7 acts within the last month (α = .809 for this study).
The IPV and both indices of political violence were positively skewed, so that log transformations were applied to both of them to normalize the distribution; a natural logarithm (LN) was applied to the IPV measure and political violence in the last-month measure. A base-10 log transformation with the addition of a constant (2) was used with the lifetime measure, due to problems with negative and zero values when attempts were made to apply the natural logarithm (McDonald, 2009). A full list of the items and their frequencies has been reported in a previous study (Sousa, 2013).
Outcome measures
This research focused on three mental health outcomes: a mental health summary score, distress, and PTSD. The Mental Component Summary (MCS), a summary measure of four scales—vitality, social functioning, role-emotional, and mental health—was derived from the SF-12, version 2, an abbreviated version of the Short Form Health Survey 36 (SF-36) (Ware, Kosinski, & Keller, 1996). The SF-36 has been widely used to assess health, including mental health, and its use has been validated with Arab populations (Al Sayah, Ishaque, Lau, & Johnson, 2013; Sabbah, Drouby, Sabbah, Retel-Rude, & Mercier, 2003). The SF-12 asks respondents to rate various dimensions of health using three- or five-item Likert-type scales, with higher scores indicating better health. Although not a direct measure of depression, MCS has been shown to effectively identify depressive symptomology (Kim et al., 2007; Vilagut et al., 2013; Walsh et al., 2006). Cronbach’s alpha for this scale, as used in this study, was .642, which was acceptable.
The 10-item distress scale (Kessler’s 10, or K-10), used in health and mental health surveys in the United States and Canada, and globally by the WHO (Kessler et al., 2002), measures nonspecific psychological distress symptoms in the prior 4 weeks on a scale of 10 to 50 (α = .889 for this study). Higher scores represent higher distress. Items include feeling tired “for no good reason,” nervous, depressed, worthless, and “so restless that you could not sit still.” The distress scale was skewed so a natural log transformation was applied to it. The K-10 adequately identifies depressive symptomology, and it also has been shown to effectively identify PTSD, panic disorders, and substance abuse with serious impairment (Spies et al., 2009; Sunderland et al., 2011).
A four-item Primary Care PTSD (PC PTSD) screen was used to assess PTSD symptoms (Prins et al., 2003). This tool does not document the diagnostic criteria for PTSD, but rather measures the core symptoms of PTSD (re-experiencing, numbing, avoidance, and hyper-arousal; Nemiah, 1995; North, Suris, Davis, & Smith, 2009). Cronbach’s alpha for this scale in this study was .854.
Covariates
Several covariates were included in the regression models. These covariates were as follows: the district in which data were collected, age (a continuous variable that ranged from 19 to 78), educational level (their highest completed level: no education, primary school, secondary school, or university), relative income level (measured with scores of 1-5, which indicated monthly incomes of less than 1,000 shekels to more than 3,500 shekels), and type of residence (village, town, or refugee camp).
Analyses
Descriptive statistics on the prevalence of political violence (lifetime and prior 30 days) and IPV, along with the bivariate connections between our variables were run using SPSS (v21). Next, we ran regression analyses to determine the unique effects of political violence and IPV, after controlling for the other form of violence and several potential demographic covariates (age, income, district of the West Bank, type of residence, and education level). To account for missing data, this set of analyses was run using Mplus, version 7; we specified that all predictor variables be included in the model and used the maximum likelihood (ML) estimator (Allison, 2009; Muthén & Muthén, 1998-2012; UCLA: Statistical Consulting Group, n.d.).
Results
A full list of the frequencies of political violence has been presented in a previous study with the full sample (Sousa, 2013), and are not reported here in detail. In short, regarding lifetime political violence, about half of our study sample reported they had lost income due to the occupation, more than one fourth reported their ability to access health care suffered due to the occupation, and about one in five had been strip-searched, while one in three had been threatened by Israeli police and military forces. Regarding political violence in the past 30 days, a quarter of all participants reported that they had been prevented from visiting family at least once due to the occupation, and a quarter reported they had seen a house or business demolished. Seventy percent of the study population reported they had to pass through an Israeli military checkpoint at least once in the past 30 days, with 15.6% responding they had to do this 10 or more times in the past 30 days.
Analysis of the summary score of IPV indicated that half the respondents reported that they had experienced at least 1 of the 12 IPV experiences in the past 12 months. Table 1 shows IPV broken down by type. By far, the most common form of IPV was control; 38% of the respondents indicated that their husband had not allowed independent behavior on various occasions. Almost one in four of the respondents reported at least one act of emotional or psychological abuse: 23.5% reported that their husband insulted them or yelled or swore at them; 21.8% reported that their husbands had ridiculed them or accused them of being a failure; 13.9% reported that their husbands had ridiculed or insulted their friends; and 11% reported that their husbands had threatened to hit or throw something at them. After control and emotional or psychological abuse, abuse of the children was the next most common type of abuse, with almost 20% reporting their husband had either beaten up or threatened to beat up the children at least once. In addition, 13.9% reported that their husbands had thrown, smashed, hit, or kicked something; 10% reported that their husbands had attacked them physically at least once; and 6% reported that their husbands had attacked them with a harmful object. Two percent reported that their husband had threatened to or actually used a lethal weapon against them or strangulated them at least once.
Frequency of IPV in Last 12 Months (“In the Past 12 Months, Has Your Husband . . .”).
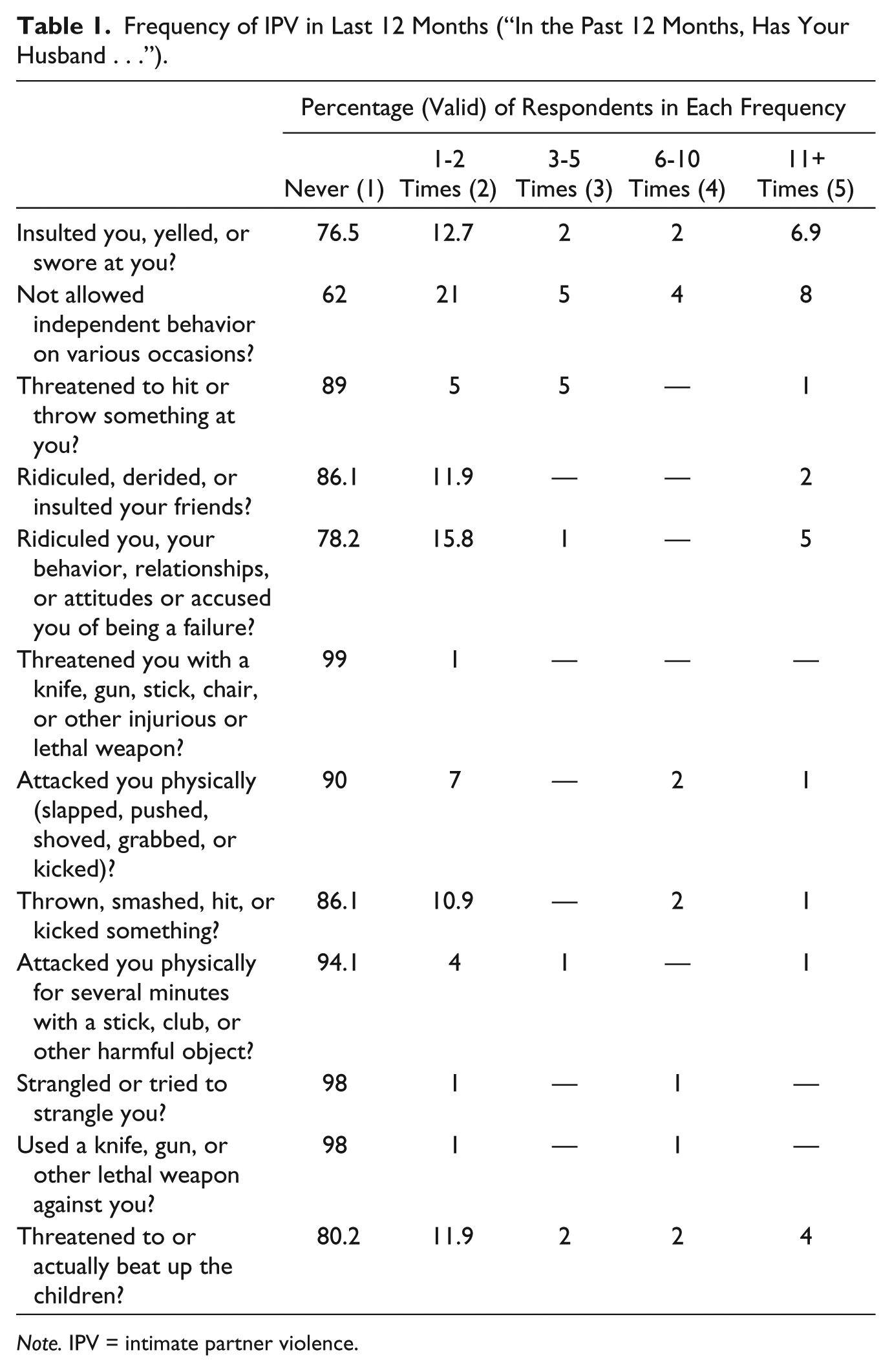
Note. IPV = intimate partner violence.
Table 2 shows the correlations among experiences of political violence, IPV, and the health outcomes, using the log transformed independent variables. IPV was positively related to lifetime experiences of political violence (r = .333, p < .001), though not to past-month experiences of political violence. Political violence in the past month was positively correlated with distress (r = .242, p < .05). Both past 30 day and lifetime measures of political violence were correlated with PTSD at around .30 (p < .01). IPV was correlated with both MCS (r = −.292, p < .01) and distress (r = .290, p < .01), though not with PTSD.
Zero-Order Correlation Matrix.
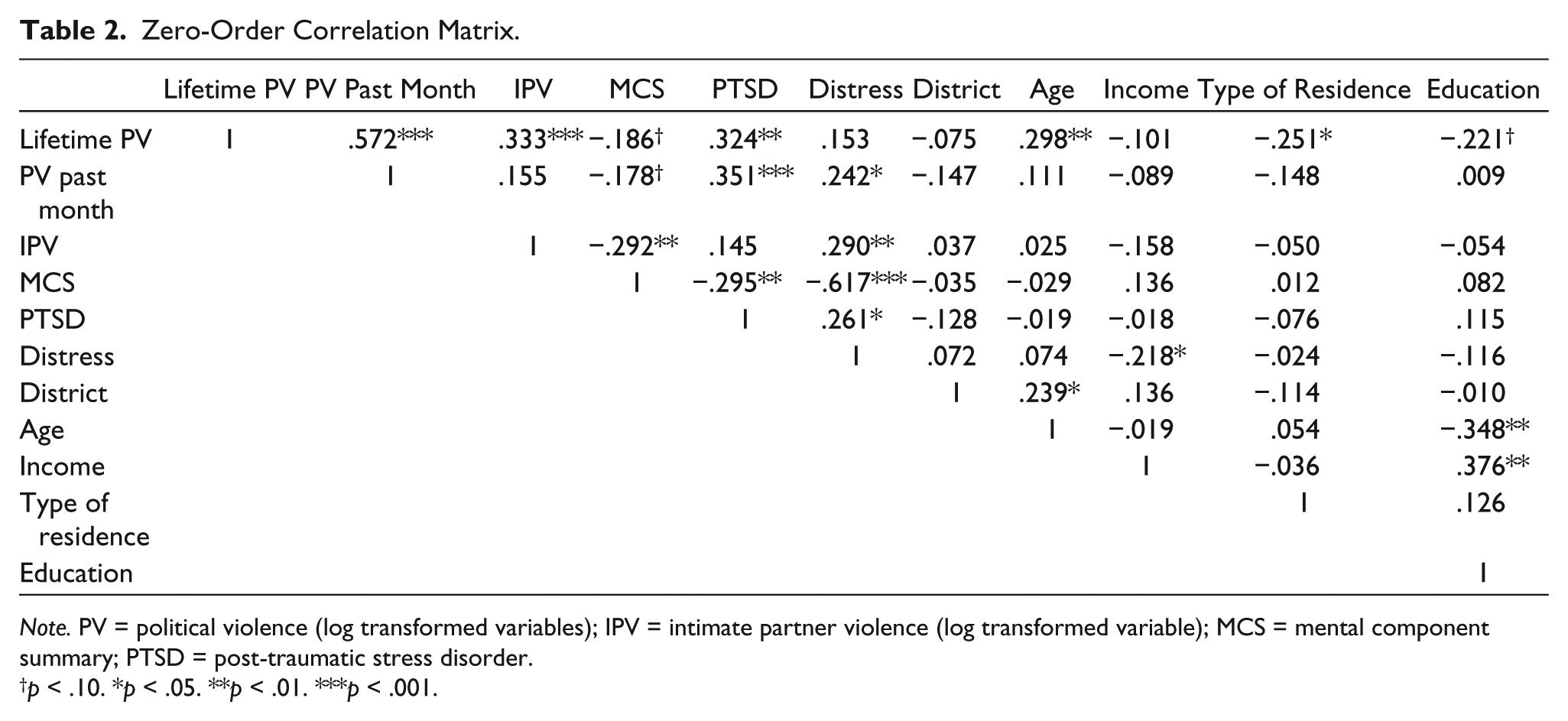
Note. PV = political violence (log transformed variables); IPV = intimate partner violence (log transformed variable); MCS = mental component summary; PTSD = post-traumatic stress disorder.
p < .10. *p < .05. **p < .01. ***p < .001.
Relative Contributions of Political Violence and IPV to Mental Health Outcomes
We used two separate models to test the relative contributions of IPV and political violence on each of our three mental health outcomes; one model tested lifetime experiences of political violence and another tested past-month experiences of political violence. Results of the models for each of the three mental health outcomes are shown in Tables 3 to 5.
Regression of Political Violence and IPV on MCS Rating.

Note. IPV = intimate partner violence; MCS = mental component summary.
Regression of Political Violence and IPV on Distress Rating.
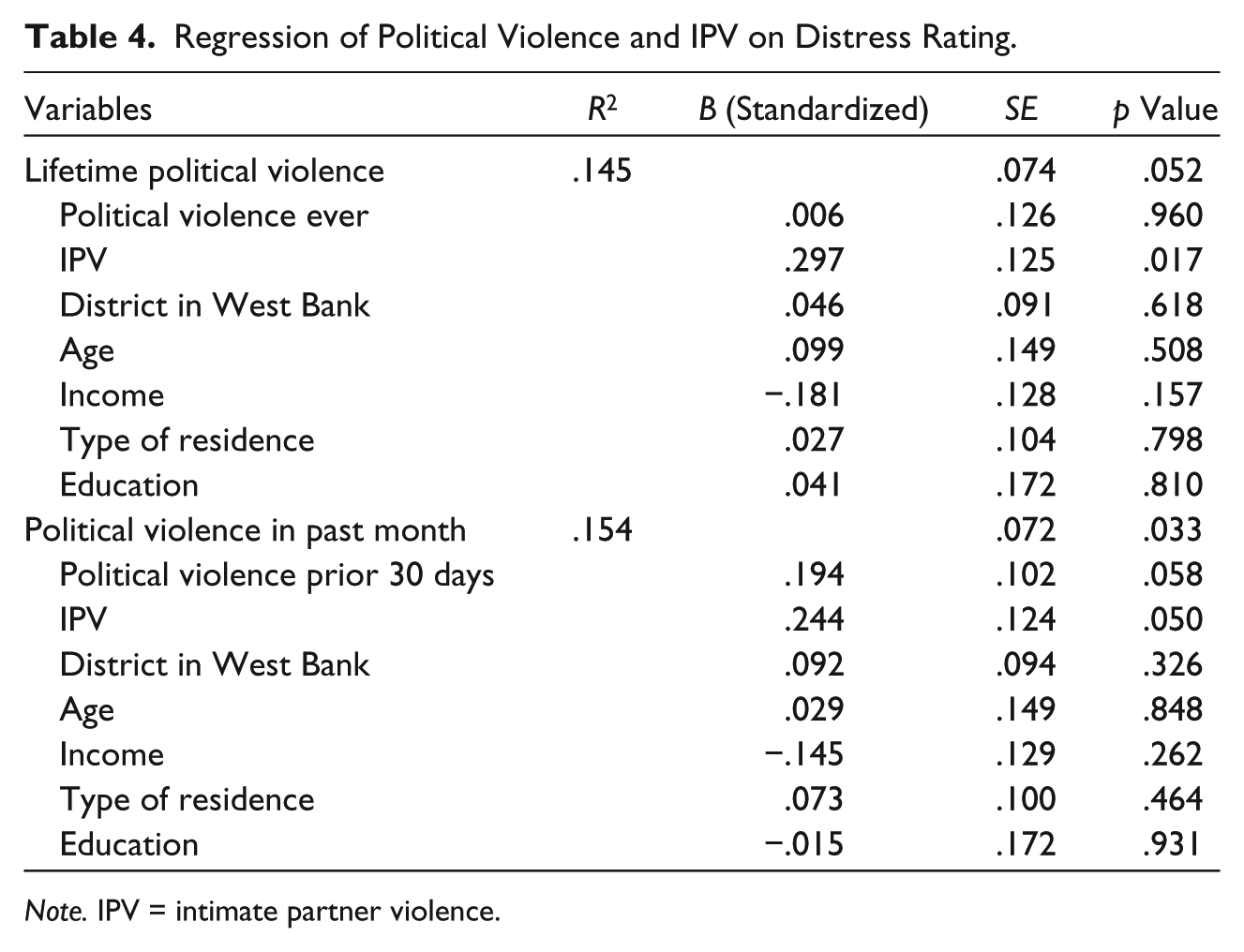
Note. IPV = intimate partner violence.
Regression of Political Violence and IPV on PTSD Rating.
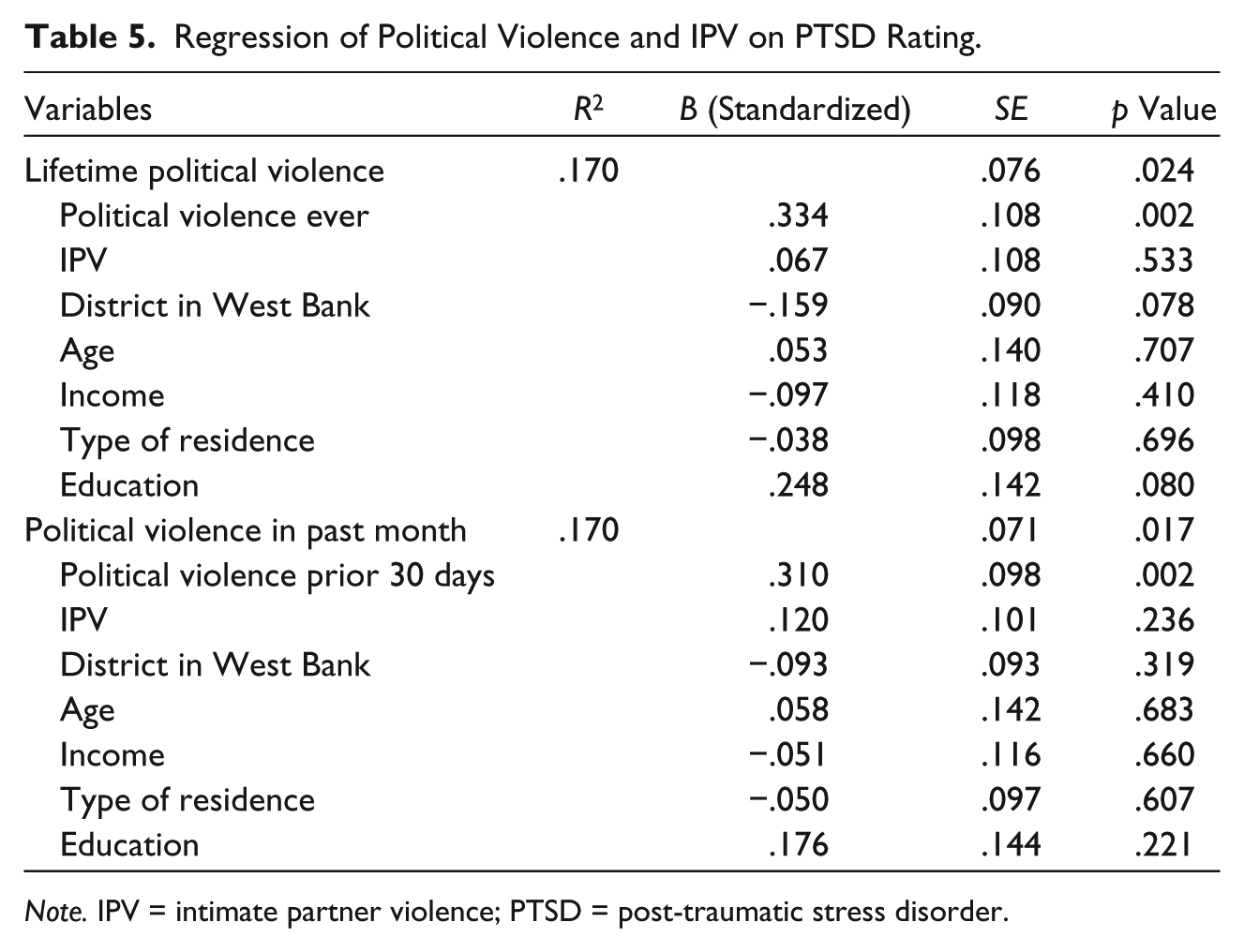
Note. IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
As shown in Table 3, in the two models for the mental health summary score from the SF-12 (MCS), neither lifetime nor past-month political violence had an independent effect on MCS. IPV was independently correlated with lower MCS scores, which indicates worse mental health, in both the model with lifetime political violence (β = −.254, p = .015) and the model with past-month political violence (β = −.259, p = .009). Together, lifetime political violence and IPV, along with our covariates, accounted for 10.7% of the variance in MCS. Political violence in the past month and IPV, along with our covariates, accounted for 11.7% of the variance in MCS.
Table 4 lists the results for the two separate models examining distress. Increased scores of IPV were independently related to increased distress in the model with lifetime political violence (β = .297, p = .017). In the model with IPV and past-month political violence, IPV had a significant independent relationship to distress, and the effect of past-month political violence on distress approached significance (β = .244, p = .050; β = .194, p = .058, respectively). The variables in the model with IPV and lifetime political violence accounted for 14.5% of the variance in distress, and those in the model with IPV and past-month political violence accounted for 15.4% of the variance in distress.
Finally, for the two models examining PTSD (Table 5), there was no significant independent relationship of IPV to PTSD. Lifetime and past-month political violence were significantly independently correlated to PTSD in a positive direction (β = .334, p = .002; β = .310, p = .002, respectively). The variables in the models with lifetime political violence and political violence in the last month accounted for 17% of the variance in PTSD (see Table 5).
Discussion
In line with other studies, both global and specific to the geographic area, we found a high prevalence of political violence in our sample, with participants reporting considerable exposure to a variety of acts of violence and repression by Israeli police and military forces (reported here only briefly; for more details, see Sousa, 2013).
Comparing rates of IPV across studies is notoriously difficult due to differences in definitions of IPV, reporting periods, and study methods (Stark & Ager, 2011; WHO, 2002). Nonetheless, it is important to note that the rates of physical IPV reported within our sample, although lower than some global and regional estimates (Haj-Yahia, 2000; WHO, 2013), do align with multiple studies that report a rate of physical IPV of around 10% (Boy & Kulczycki, 2008; Eisikovits, Winstok, & Fishman, 2004; García-Moreno et al., 2005; Stark & Ager, 2011; WHO, 2002). Similarly, there is a great deal of variance in global estimates of verbal abuse and control that characterize IPV; global estimates range from 20% to 90% (García-Moreno et al., 2005). In our sample, this type of IPV was fairly common among our participants (with 38% reporting control and about 20%-25% reporting some type of emotional or psychological abuse). Although our rates on some items (particularly some verbal abuse items) are on the lower end of the spectrum, by and large our results reflect those from systematic wide-scale regional studies done in Israel and Palestine (each with samples of around 2,000), in which rates of controlling behavior and emotional or psychological abuse ranged from around 20% to 50% (Eisikovits et al., 2004; Haj-Yahia, 2000).
Like others on the topic, our study demonstrated a strong relationship between political violence and IPV (Al-Krenawi et al., 2007; Clark et al., 2010; Stark & Ager, 2011; Usta et al., 2008; Vinck & Pham, 2013). In light of the regularity with which political violence and IPV tend to co-occur, our final study question about the unique effects of each form of violence on particular mental health symptomology takes on increased importance.
Studies examining trauma in general, as well as studies that specifically examine the mental health effects of either political or IPV, suggest both PTSD and depressive symptomology result from exposure to extreme experiences (Carlson & Rosser-Hogan, 1991; Cascardi et al., 1999; de Jong et al., 2003; Shalev et al., 1998). Although some studies have been able to establish independent relationships between both political violence and family violence and mental health (Al-Krenawi et al., 2007), few studies provide insight into how exposure to political violence and family violence (especially IPV) might have dissimilar effects on particular mental health outcomes. In one of the rare studies that considered the differential impacts of these forms of violence on diverse types of mental health symptomology, both political violence and IPV were independently associated with both PTSD and depression (Vinck & Pham, 2013). In contrast to this finding, our results suggest that political violence and IPV may be correlated with distinct mental health sequela.
In our study, political violence was independently related only to increased rates of PTSD, not to MCS, the measure that more adequately reflects mood disorders including depressive symptomology. These findings stand in contrast to those from studies focused on the mental health consequences of political violence that have concluded that political violence contributes to both PTSD and depressive disorders (Carlson & Rosser-Hogan, 1991; de Jong et al., 2003). Our findings do reflect those from a much earlier study, which examined both PTSD and depression among Vietnam veterans and found that exposure to atrocities during war predicted PTSD but not depression (Breslau & Davis, 1987). Furthermore, there is general agreement that PTSD is the most commonly reported consequence of political violence, above mood disorders such as depression, and our results align with these conclusions (de Jong et al., 2003; Neria, Nandi, & Galea, 2008; Norris et al., 2002; WHO, 2001).
On the other hand, in our study, IPV, and not political violence, was independently related to a poorer mental health summary score and increased distress, but not to PTSD. This finding differs from the findings from multiple studies that indicate that PTSD is a common outcome of IPV (Golding, 1999). However, literature on PTSD associated with exposure to IPV seems to indicate that PTSD tends to result from severe experiences of violence, where people confront considerable horror, threats to life, and physical injury (Dutton-Douglas, 1992; Houskamp & Foy, 1991; March, 1993). Indeed, within one of the rare studies that have explored the sequela of PTSD among women by simultaneously investigating exposures to IPV and to political violence, PTSD was a significant outcome of IPV—in this study, however, IPV was measured by severe beatings (Vinck & Pham, 2013). In contrast, in our sample, very few respondents indicated physical abuse, and those who did report physical abuse reported that it happened with low frequency. Reports of psychological abuse were far more frequent in our sample. Our findings regarding the associations of IPV with depression rather than PTSD might best be understood within the large body of literature suggesting the particular effects of psychological abuse characterized by emotional and verbal assaults (i.e., ridicule, control, threats, and degradation) on overall emotional well-being (Follingstad, Rutledge, Berg, Hause, & Polek, 1990; Walker & Lenore, 2009), including a significantly increased risk for depressive symptoms in particular (Migeot & Lester, 1996; Orava, McLeod, & Sharpe, 1996; Vitanza, Vogel, & Marshall, 1995).
Possible explanations for the findings regarding the disparate mental health sequela associated with political violence versus IPV include the idea that, unlike depression, PTSD is precipitated by an event that is understood to be a chaotic, unexpected threat to one’s life that fundamentally challenges one’s perceptions of safety, along with undermining his or her sense of control and power over his or her environment (Foa, Zinbarg, & Rothbaum, 1992), which is quite distinct from the psychological sequela resulting from other stressful life events that may be experienced on a more daily basis, within, for instance, one’s job or family life (APA, 2000). In contrast to these more acute events, the emotional response to stressful experiences that one might understand as being more routine or expected may manifest as depressive symptoms (Breslau et al., 2000). According to this framework, depression associated with psychological IPV in particular may be explained by how psychological IPV undermines self-esteem (Anguilar & Nightingale, 1994; Nixon, Resick, & Nishith, 2004) and may contribute to the abused woman’s view of herself as inadequate, unlovable, deficient, and worthless (particularly if the woman believes that her partner’s psychologically abusive behavior is warranted; Follingstad et al., 1990), ultimately leading to depression (Murphy & Cascardi, 1999).
Although our findings contribute to literature on a rarely examined but vitally important topic, the relationship between and differential mental health effects of co-occurring forms of violence, there are several limitations that warrant attention. First, our sample was purely a convenience sample and as such there was no random selection; results thus should not be understood to be reflective and representative of the population as a whole. The relatively small sample size affected our statistical power and raised our odds of Type 2 errors so that there may in fact be correlations that we were simply unable to detect. In addition, our sample may well suffer from selection bias. We had a high level of missing data (particularly on the IPV scale) that we had to account for in our analyses. This could have been due to the fact that participants were filling out the forms in a health care setting, sometimes were accompanied by their significant others, and sometimes knew the providers well (because some of the settings were in small communities). Although we used analysis methods that took into consideration the missing data, it might well be that if we had collected data where participants felt more privacy, we would have had more data points for our IPV scale, and our measure of IPV might have captured more incidents, types, and levels of severity of IPV. Future studies should work to capture this information while particularly attending to the complexities of collecting this type of data, especially, though not only, if the research takes place in health care settings, as did our study (WHO, 2013b; Zink & Putnam, 2005).
Furthermore, due to the cross-sectional nature of the data, it is impossible to determine the direction of our findings. This limitation is particularly important given the suggestion from various sources about the diverse ways that depression, PTSD, and IPV relate to each other (Devries et al., 2013). For instance, major depression has also been associated with PTSD and several PTSD symptoms (diminished interest or participation in significant activities, difficulty concentrating) are similar to symptoms of depression (APA, 2000; Shalev et al., 1998). Scholars suggest that depression is often “secondary” to PTSD (Breslau et al., 2000; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995; Mellman, Randolph, Brawman-Mintzer, Flores, & Milanes, 1992), although considerable controversy remains on this topic, as others have concluded that depression does not necessarily follow PTSD (Shalev et al., 1998). To examine the possibilities that our findings are due to some spurious series of relationships, we did a series of post hoc analyses via a new set of regression equations, which controlled for the other form of mental distress. In these equations, the independent effects of the distinct forms of violence on distinct mental health symptomology held up, even after controlling for the other mental health outcome. Nonetheless, particularly in light of the literature above, future research should consider the ways that one form of mental distress (for instance, PTSD) might precipitate and affect the other (for instance, depression). It should also be noted that we used screening tools to measure mental health symptoms regarding PTSD and depressions rather than directly measuring these problems. Findings should thus be understood as an indication of the mental health consequences due to these types of violence. Future empirical work on the topic might utilize other measures of mental health.
In this discussion, we have provided some potential theories regarding why political violence may be interpreted in a specific way that could lead to symptoms of PTSD, whereas IPV (particularly psychological IPV) may be interpreted differently, and thus increase one’s risk for depression. In light of the limitations presented above, the theoretical mechanisms suggested are highly speculative. Differences in how individuals and collectives understand and respond to IPV, political violence, and the relationship between these two phenomena (e.g., Johnson, 2008; McWilliams, 1997) might account, at least in part, for the unique consequences of these types of violence. Without deeper exploration of these processes, however, the effects of various forms of violence remain under examined. Scholarship on the topic thus necessitates additional research into the meanings and consequences of the differential experiences of violence; this will require not only understanding the distinct mental health sequela of varied types of violence from a quantitative, epidemiological approach (Vinck & Pham, 2013) but also more nuanced, qualitative explorations of how people interpret and make meaning of the various forms of violence they encounter within conflict settings (see, for instance, Annan & Brier, 2010). Given the mental health ramifications of both political violence and IPV, along with evidence from this and other studies about the relationships between these two types of violence (Stark & Ager, 2011; Usta et al., 2008; Vinck & Pham, 2013), particular attention should indeed be paid to women’s subjective experiences of these two types of violence. Furthermore, given the co-occurrence of the two forms of violence studied here, future studies should examine how political violence and IPV might work in conjunction with each other to affect well-being (for instance, with one mediating or moderating the effects of the other).
Regarding practice implications, the results reported here highlight the need to carefully assess the various types of violence that people encounter, to allow them to narrate for themselves how these experiences affect their well-being, and to use not only sound practice knowledge (Inter-Agency Standing Committee [IASC], 2007; WHO, 2013b) but also people’s own expertise to determine what strategies might be most effective to address the violence they encountered. We must prioritize people’s own wisdom regarding the effects of and treatments for the violence they experience. This is especially important given the risks of using mental health outcomes, particularly PTSD, without a nuanced understanding of the limitations this lens provides into people’s lived realities and their choices about what would best help them re-claim wellness (Mezey & Robbins, 2001; Summerfield, 1999, 2001). Finally, the results reported here provide yet more evidence of the importance of global initiatives aimed at preventing both political violence and IPV (de Jong, 2010; WHO, 2010), as well as to the particular need to assess, prevent, and treat IPV within settings of mass conflict and disasters (WHO, 2005).
Footnotes
Acknowledgements
The authors wish to acknowledge the Palestinian Medical Relief Society, particularly the front-line staff from the local clinics around the West Bank who diligently arranged for data collection and thus enabled this project.
Authors’ Note
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by NIMH Grant T32MH20010. The funding organizations played no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of this manuscript.