
Abstract
This study compares the association of histories of childhood emotional, physical, and sexual abuse, and physical neglect with revictimization among adolescent girls, and investigates the role of posttraumatic stress and symptoms of depression as mediators. Participants were 234 girls aged 12 to 19 years, who have been involved with the child welfare system in a Midwestern urban area. Data were collected from baseline surveys of a trauma-focused group program to which the participants were referred. The majority of participants were youths of color (75%) who were primarily African American (70%), and the remaining participants were White, non-Hispanic (25%). Data were collected through surveys that assessed histories of child abuse and neglect, symptoms of posttraumatic stress and depression, and experiences of physical, verbal, and relational revictimization in the last 3 months. All types of abuse and neglect were significantly associated with higher frequencies of revictimization and higher levels of posttraumatic stress and depressive symptoms. Parallel mediation analyses demonstrated that both posttraumatic stress and depression fully mediated the relationships between emotional abuse and revictimization, and sexual abuse and revictimization. Physical abuse was fully mediated by posttraumatic stress, but not by depression. Results also indicated that neither posttraumatic stress nor depression were mediators for the relationship between neglect and revictimization. There were similar pathways to revictimization in adolescents from emotional and sexual abuse through posttraumatic stress and depression. Evidence is mounting for the deleterious effects of emotional abuse. There is evidence that treatment of both posttraumatic stress and depression in emotionally and sexually abused adolescents involved in child welfare is warranted to prevent future revictimization.
Childhood abuse and neglect are common in the United States. The most recent prevalence rates indicate that one in eight children under 18 years of age has experienced at least one form of child maltreatment (Wildeman et al., 2014). Childhood maltreatment has been associated with a number of negative outcomes. One serious consequence of child maltreatment is the increased risk for multiple types of revictimization during adolescence and adulthood (Desai, Arias, Thompson, & Basile, 2002; Irwin, 1999; Schaaf & McCanne, 1998; Widom, Czaja, & Dutton, 2008). In addition, there are some serious mental health consequences to childhood abuse and neglect such as posttraumatic stress and depression. Adolescents involved in the child welfare system have high rates of serious mental health disorders compared with the general adolescent population, and females have higher rates of depression and other internalizing behavior disorders than males within the child welfare system (Auslander et al., 2002; McMillen et al., 2005). Although there is research about the negative consequences of child maltreatment, there is limited knowledge of the mental health pathways linking childhood maltreatment to physical, verbal, or relational revictimization among adolescents in the child welfare system.
There is a growing literature of the association between childhood abuse and revictimization as reported by adult women retrospectively (West, Williams, & Siegel, 2000; for a review, see Classen et al., 2002). In some cases, specific types of maltreatment have been found to be more likely to lead to later revictimization than others; however, the research is inconclusive. There is also some evidence for a link between childhood maltreatment and revictimization in adolescence. Boney-McCoy and Finkelhor (1995) found that victims of childhood sexual abuse were almost 12 times as likely to be revictimized when compared with nonabused counterparts. Moreover, children who were maltreated were 20% more likely to experience peer or sibling victimization and 30% more likely to be physically assaulted (Finkelhor, Ormrod, & Turner, 2007). Physical abuse, sexual abuse, and physical neglect have all been associated with peer victimization (Duncan, 1999). One of the only studies in a child welfare population found that emotional abuse was predictive of dating violence among female adolescents engaged with child protective services (Wekerle et al., 2009).
In addition to the evidence for the association between childhood abuse and revictimization during adolescence, research has demonstrated the linkages between posttraumatic stress and revictimization. A national longitudinal sample of adolescents found that posttraumatic stress disorder (PTSD) symptoms at baseline significantly predicted interpersonal revictimization, controlling for the effects of prior victimization (McCart et al., 2012). Likewise, in a study of adolescent dating relationships over 1 year, trauma-related symptoms were a significant predictor of dating violence in a community sample (Wolfe, Wekerle, Scott, Straatman, & Grasley, 2004).
Information-processing models of memory provide one framework for how symptoms of mental health problems, particularly PTSD and depression resulting from child maltreatment, may contribute to revictimization (Beckham, Moore, & Reynolds, 2000). Research on cognitions associated with memory has recently focused on ways individuals with intrusive PTSD symptoms have difficulty ignoring trauma-related stimuli (Pineles, Shipherd, Mostoufi, Abramovitz, & Yovel, 2009), which hampers their ability to perceive new threats and may render them vulnerable to revictimization (Cougle, Resnick, & Kilpatrick, 2009; Messman-Moore & Long, 2003). A diminished cognitive capacity to detect threat is also theorized to result from depression (Cougle et al., 2009), such that symptoms of depression hinder the ability of an adolescent with a history of child maltreatment to avoid revictimization (Wekerle et al., 2001). Maltreated children may also fail to develop secure attachment patterns with caregivers, interrupting affect regulation, or the ability to handle negative emotions in the face of danger or distress (Mikulincer & Shaver, 2012; Schore & Schore, 2008). These children may be more vulnerable to anxiety, depression, and PTSD as adolescents and adults (Mikulincer & Shaver, 2012). Children with insecure attachment patterns may harbor feelings of unworthiness, be unable to correctly interpret traumatic experiences, and, as a result, may be unable to prevent harmful interpersonal interactions such as revictimization (Tanaka, Wekerle, Schmuck, Paglia-Boak, & MAP Research Team, 2011).
Recent studies provide evidence for the mediating role of PTSD and depression in revictimization with adult samples, the majority of which have focused on the pathways between childhood sexual abuse and sexual revictimization among females (Fortier et al., 2009; Messman-Moore, Brown, & Koelsch, 2005; Risser, Hetzel-Riggin, Thomsen, & McCanne, 2006). Research on pathways between types of maltreatment and revictimization in adolescents is more limited, particularly with child welfare samples. For example, a study with a sample of students from 10 high schools demonstrated that trauma-related symptoms mediated the relationship between child maltreatment and of adolescent dating violence (Wolfe et al., 2004). Another study that included a sample of juvenile offenders found that depression provided a pathway between childhood emotional abuse and peer victimization (Day et al., 2013). The only study that focused on adolescents involved in child welfare found that posttraumatic stress symptoms mediated the relationship between child maltreatment and dating violence victimization in girls (Wekerle et al., 2001).
The current study extends prior research by comparing multiple types of child maltreatment among girls in child welfare and their association with physical, verbal, and relational revictimization. Because pathways from childhood abuse and neglect to revictimization have been shown to be gender-based (Wekerle et al., 2009), and females are more vulnerable to mental health problems and revictimization, the current study examined girls. Moreover, we operationalized revictimization more broadly than dating violence to capture the experiences of adolescent girls who may be experiencing interpersonal revictimization from a variety of perpetrators and in multiple contexts. Therefore, to further our knowledge of the mental health pathways by which histories of child maltreatment lead to revictimization (physical, verbal, and relational) among adolescent girls in child welfare, the following questions were addressed: (a) What is the association between different types of childhood abuse and neglect (emotional, physical, sexual abuse, and physical neglect) and revictimization among adolescent girls involved in the child welfare system? and (b) Do posttraumatic stress and depression mediate this relationship among these adolescents? Findings will contribute to our understanding of the mechanisms by which childhood abuse and neglect increases the risk of revictimization during adolescence, and highlight potential modifiable factors to target for preventing future revictimization in female adolescents and young adults.
Method
Participants
Participants were 234 girls, ages 12 to 19 (M = 14.9, SD = 1.6), who were involved with the child welfare system. Participants were recruited through referrals from the state’s child protective agency (Children’s Division), other agencies that provide services to adolescents in the child welfare system, and from caregivers. Inclusion criteria for the study included (a) adolescent girls who were formally investigated or substantiated for child maltreatment by Children’s Division and (b) girls 12 to 19 years old. Girls were excluded if they were unable to read or write, or if they had behaviors that would prohibit participation in either a structured interview or group treatment focused on abuse and neglect. It was not necessary for girls to meet diagnostic thresholds for PTSD or depression to be included in the study.
Seventy-five percent of participants were youths of color, of whom the majority (70%) were African American, and the other 5% self-identified as Native American, Hispanic, Asian/Asian American, or “Other.” The remaining participants (25%) were non-Hispanic, White. The living situations of the participants was as follows: 60% lived with biological parent(s), relatives, or an adoptive family, 27% lived with a foster family, and 13% living in a group or other congregate care facility. Of the participants, 72% were currently receiving one or more types of services such as outpatient, health, social, behavioral, mental health, and/or school-based services (M = 1.35, SD = 1.14).
Informed Consent and Interview Procedures
Baseline data collected for a trauma-focused cognitive-behavioral intervention study were used for the current analysis. The study protocol was first approved by the Human Subjects Institutional Review Board of the two collaborating universities. Second, a Certificate of Confidentiality was issued by Centers for Disease Control and Prevention (CDC; the funding agency) to protect the privacy of research participants by withholding their identities from all persons not connected with the research. In addition, the Research Committee of the state office of child protective services approved the research protocol.
The consent procedures included several steps. After a referral was made to the study team, and the adolescent expressed interest in participating, written consent was obtained from the legal custodian. In addition, to the fullest extent possible, written consent was secured from all members of the youth’s Family Support Team (e.g., Guardian ad litem, Deputy Juvenile Officer, child’s current therapist). All adolescents under the age of 18 provided written assent to participate in the study. Participants were given a US$20 gift card to compensate them for their time.
Data were collected by surveys verbally administered by interviewers who were master’s level or doctoral level social work students who participated in 8 hours of interview training. The training included background knowledge of the population, basic interviewing skills, confidentiality and ensuring privacy during the interview, procedures for reporting abuse, and procedures for participants who endorsed items related to suicide. The surveys were administered in participant homes or a community-based mental health agency and took approximately 1 hr to complete.
Variables and Measures
Child maltreatment
The Child Trauma Questionnaire (CTQ; Bernstein & Fink, 1998) was used to obtain participant reports of the types and severity of child maltreatment experienced. Four subscales from the 28-item scale were used in the present study: Emotional Abuse, Physical Abuse, Sexual Abuse, and Physical Neglect. Items are rated from never true (1) to very often true (5). Previous research has demonstrated the validity and reliability of the CTQ (Bernstein & Fink, 1998). In addition, guidelines for classification of CTQ scores are provided according to the following categories: none or minimal, low–moderate, moderate–severe, and severe–extreme (Bernstein & Fink, 1998). Internal consistency alpha coefficients for the current sample were as follows: emotional abuse (α = .86), physical abuse (α = .87), sexual abuse (α = .92), and physical neglect (α = .81).
PTSD symptoms
Posttraumatic stress symptoms were assessed using the Child PTSD Symptom Scale (CPSS; Foa, Johnson, Feeny, & Treadwell, 2001). Seventeen items (e.g., Having bad dreams or nightmares; Trying not to think about, talk about, or have feelings about the trauma) assessed domains of reexperiencing, avoidance, and arousal. Participants rated the frequency of posttraumatic stress symptoms over the past month using a 4-point scale from “not at all” (0) to “five or more times a week” (4). The CPSS has previously demonstrated convergent validity, correlating highly with a similar PTSD scale, as well as good internal consistency and test–retest reliability (Foa et al., 2001). For the present study, internal consistency reliability was α = .90.
Depression
The Child Depression Inventory (CDI; Kovacs, 2003) was used to measure depressive symptoms over the previous 2 weeks. The 27 items were rated from 0 to 2 and summed, with higher scores indicating more severe symptoms. Concurrent, discriminative, and criterion validity have been demonstrated (Kovacs, 2003; Saylor, Finch, Spirito, & Bennett, 1984). Good internal consistency and test–retest reliability have been demonstrated for a child welfare population (Kolko et al., 2010). The internal consistency alpha coefficient for the current sample was α = .89.
Interpersonal revictimization
The Problem Behavior Frequency Scale (PBFS; Farrell, Kung, White, & Valois, 2000) consisting of 18 items was originally developed to assess peer aggression toward others among school-aged children and adolescents. For the current study of girls with prior histories of maltreatment, the items were modified to assess the girls’ experiences of being revictimized (i.e., aggressive behaviors targeting them in the past 3 months). Example items from the three subscales included Physical Revictimization (e.g., Another person hit or slapped you), Verbal Revictimization (e.g., Someone teased you to make you angry), and Relational Revictimization (e.g., Another person tried to keep others from liking you by saying mean things about you). The language of each item did not specify who was the perpetrator (e.g., “another person” or “someone”) to capture the wide range of possible individuals who may revictimize the girls. Items were rated to indicate the frequency with which they had happened over the past 3 months on a 6-point scale coded as follows: 1 = “0 times,” 2 = “1-2 times,” 3 = “3-5 times,” 4 = “6-9 times,” 5 = “10-19 times,” and 6 = “20+ times.” Items were summed to yield a total revictimization score with a possible range of 18 to 108. Previous studies have shown adequate to good internal consistency (Farrell et al., 2000; Miller-Johnson, Sullivan, & Simon, 2004), and the alpha coefficient for the current sample was α = .93.
Potential control variables
Several control variables were investigated because they have been shown in previous research to predict poor mental health and behavioral outcomes among child welfare populations, such as placement instability, use of services, age, and race (0 = youths of color; 1 = White). The number of services used in the participant’s lifetime was measured using the Service Assessment for Children and Adolescents (SACA; Stiffman et al., 2000). This structured interview asks about the number and types of inpatient, outpatient, and school-based social, behavioral, and mental health services the participant has ever received. Placement instability (ever) was measured using a count of the number of different types of placements that the adolescent had lived during her lifetime.
Data Analysis
The mediating roles of posttraumatic stress and depression were tested using the steps established by Baron and Kenny (1986), followed by the bootstrapping technique to test the significance of the indirect effects described by Preacher and Hayes (2004). First, a preliminary analysis was conducted to determine that there were significant correlations among the hypothesized predictors (types of abuse and neglect), mediators (posttraumatic stress and depression), and outcome variable (revictimization). Second, a mediation analysis was conducted using the Hayes (2013) PROCESS SAS macro. Because there is no theoretical causal assumption between the two mediators, and they work relatively independently from each other, parallel mediation models were tested. In addition to calculating the standard a, b, c, and c’ path coefficients, the Hayes macro uses a bootstrap resampling methodology to enable a significance test of the indirect effect (the impact of the predictor on the outcome variable through the mediator).
Results
Descriptive Analyses
Descriptive statistics (means and standard deviations) for the abuse and neglect (independent) variables, mediators (posttraumatic stress, depression), outcome variable (revictimization), and control variables are shown in Table 1. According to the Bernstein and Fink (1998) classification, the mean scores of the Childhood Abuse and Neglect subscales indicated that the girls experienced emotional abuse and physical neglect in the low to moderate range, physical abuse in the moderate to severe range, and sexual abuse in the severe range. Of the 234 adolescent girls in the sample, 83% had experienced childhood emotional abuse, 81% had experienced physical abuse, 64% sexual abuse, and 69% physical neglect (based on endorsing at least one of the items on the subscale).
Means and Standard Deviations of Variables (N = 234).
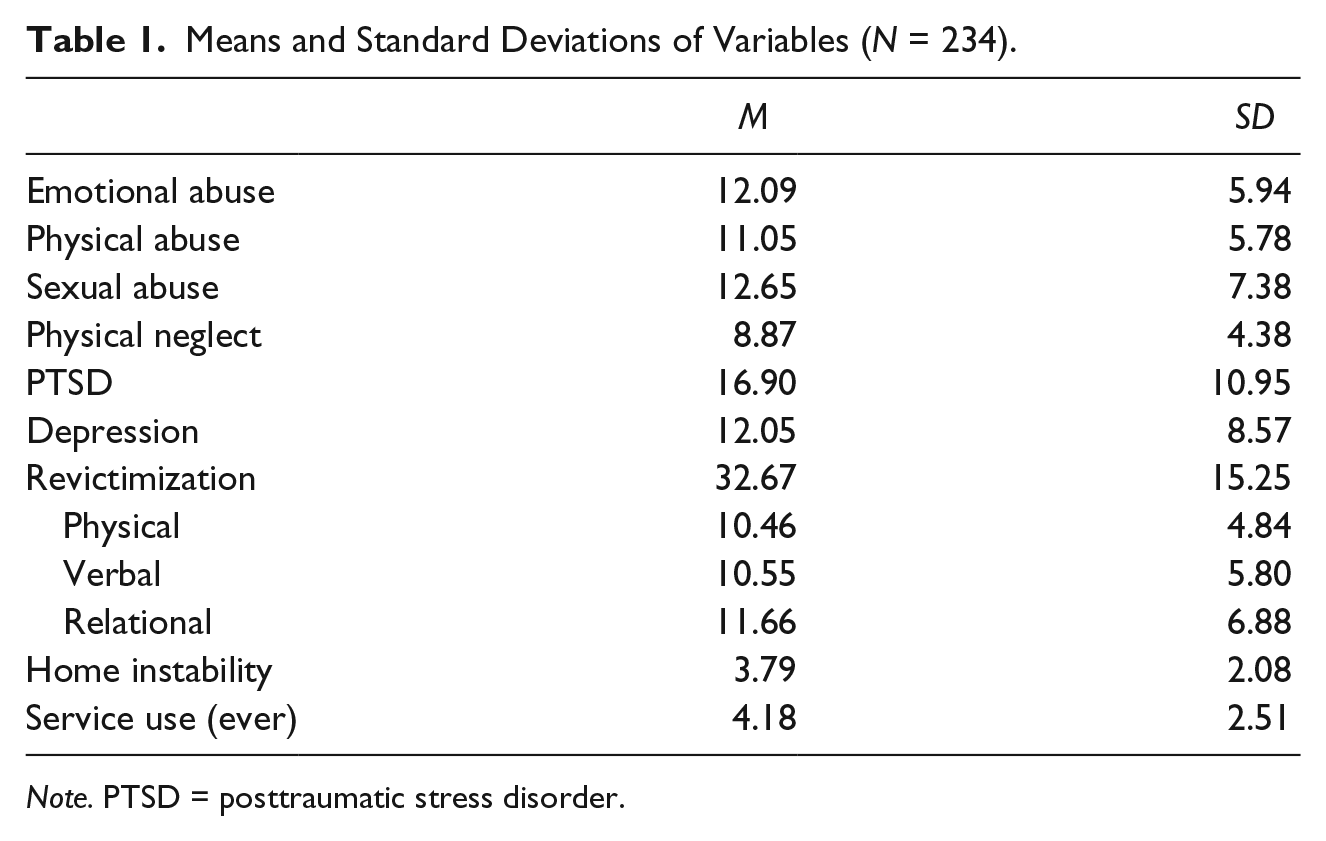
Note. PTSD = posttraumatic stress disorder.
Results indicated that 51% of the girls experienced PTSD symptoms in the clinical range (≥15), with a mean score of 16.90 (SD = 10.95) for the entire sample. The participants’ mean depression score was 12.05 (SD = 8.57). Previous studies have reported CDI cutoff scores for clinically referred samples of ≥13 where higher scores are expected (Kovacs, 2003). In the current study, 35% of the girls had depression scores that were in the clinical range.
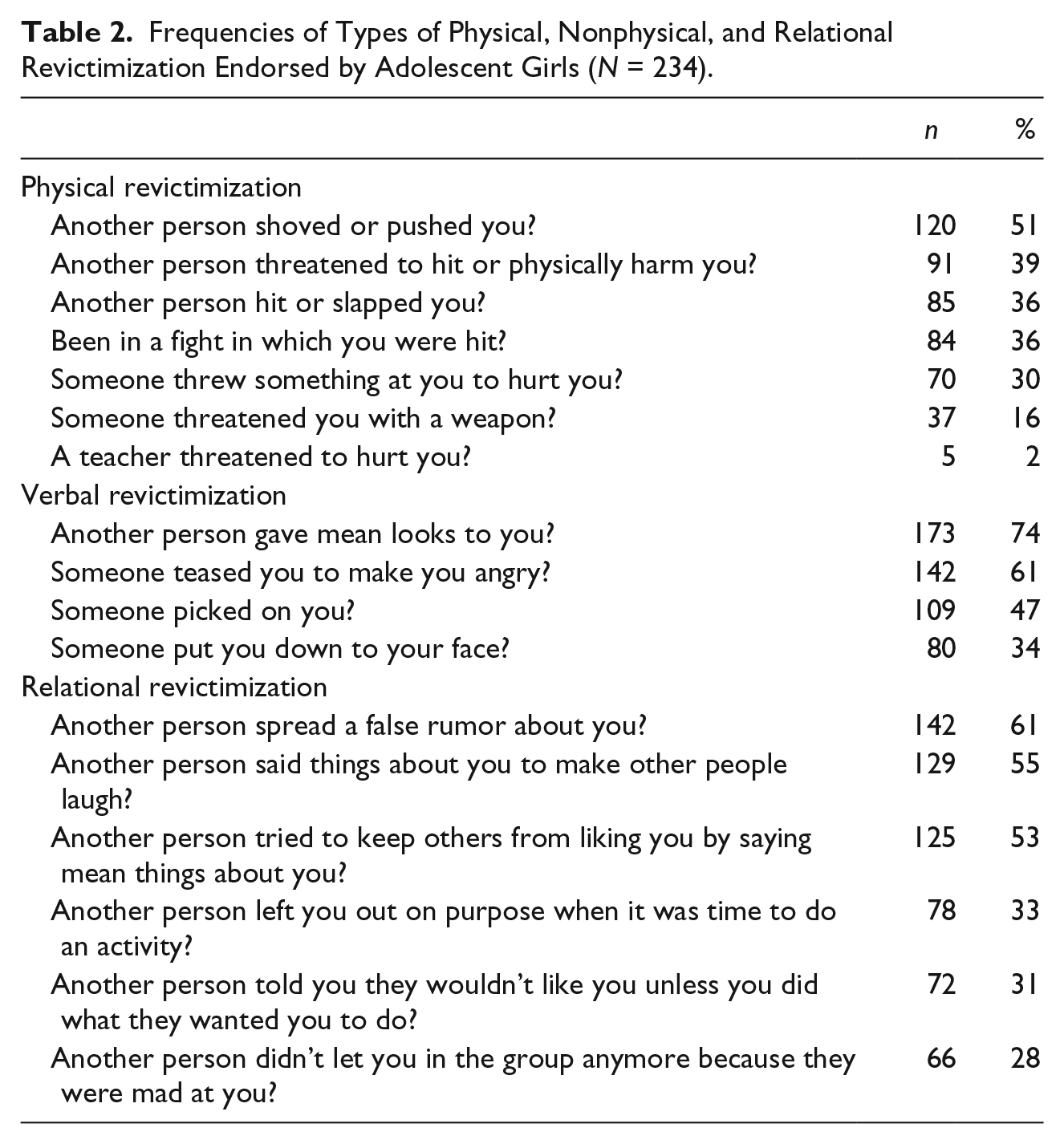
The frequencies of each type of revictimization that were experienced in the last 3 months are shown in Table 2. Notably, among the physical revictimization items, approximately one in six of the girls (n = 37) was threatened with a weapon, over one half were shoved or pushed, and over one third were hit or slapped. Comparisons of different types of revictimization indicated that 84% endorsed at least one item in the Verbal Revictimization subscale, 74% endorsed at least one item in the Relational Revictimization subscale, and 68% endorsed at least one item in the physical Revictimization subscale.
Frequencies of Types of Physical, Nonphysical, and Relational Revictimization Endorsed by Adolescent Girls (N = 234).
Bivariate and Mediation Analyses
Bivariate analyses were conducted between independent, mediating, and dependent variables to determine whether they met the criteria to test a mediating hypothesis. Results shown in Table 3 indicated that significant relationships were found between all forms of abuse and neglect (emotional, physical, sexual abuse, and physical neglect) with revictimization, PTSD, and depression. Compared with other forms of abuse, emotional abuse was most strongly related to mental health symptoms and revictimization, and physical neglect showed the weakest relationships with these variables. Of the mediators, both PTSD and depression were strongly correlated with revictimization. Placement instability and service use were used as control variables because they were significantly associated with the dependent variable and the majority of independent variables, and conceptually may explain the relationship between histories of abuse and neglect and experiences of revictimization as adolescents. Because age and race were not associated with revictimization at the bivariate level, they were not included as control variables in the mediation models.
Bivariate Correlations Between Child Maltreatment Types, Mental Health, Revictimization, and Demographics (N = 234).
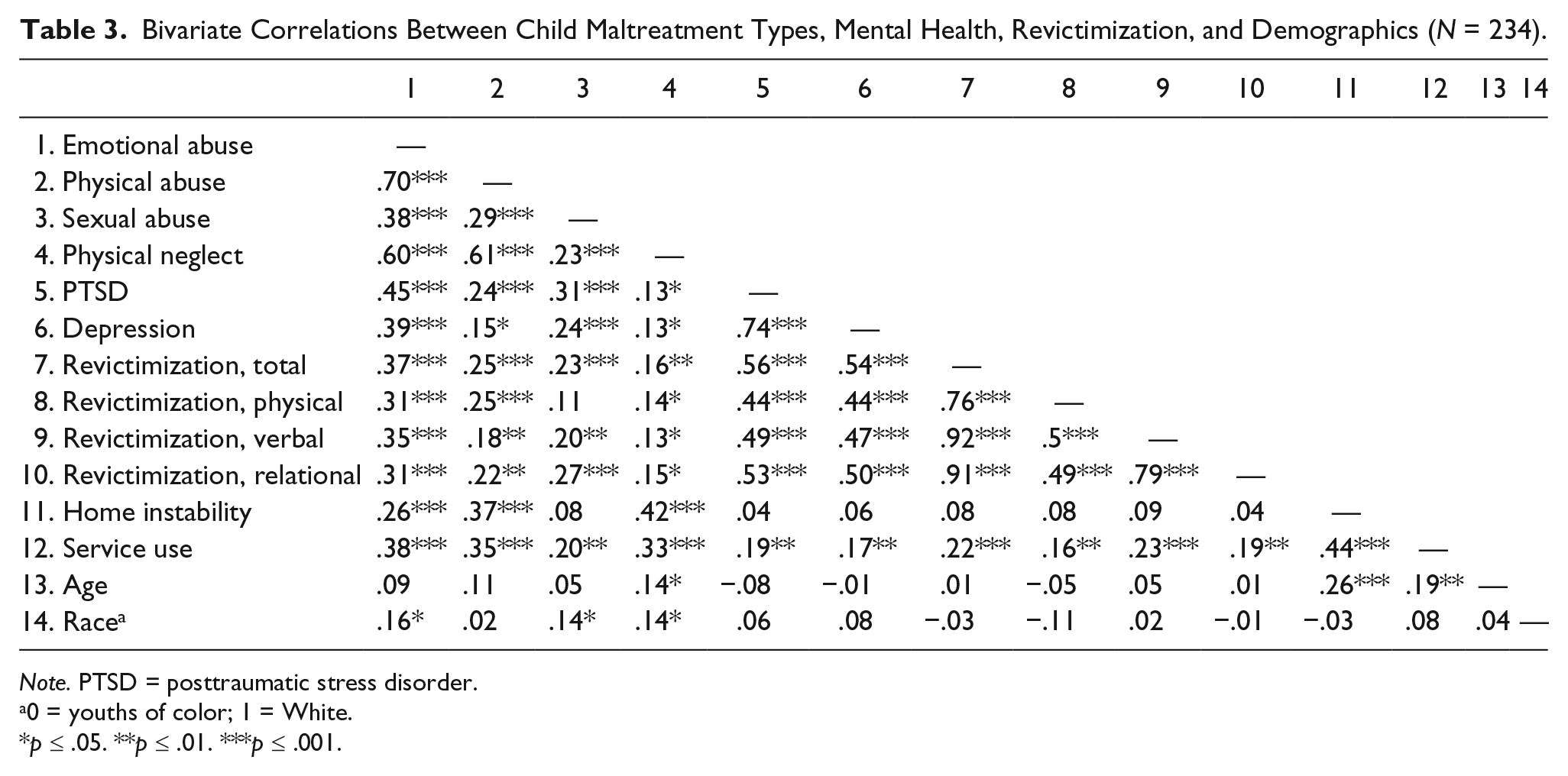
Note. PTSD = posttraumatic stress disorder.
0 = youths of color; 1 = White.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
As shown in Figure 1, mediation analyses indicated that participants with greater emotional abuse were associated with more revictimization, and this relationship was fully mediated by both PTSD and depression. Results of the bootstrapping analysis described by Preacher and Hayes (2004) indicated significant indirect effects of emotional abuse on revictimization via the hypothesized mediators of PTSD (β = .3625; 95% confidence interval [CI] = [0.1139, 0.6476]) and depression (β = .2510; 95% CI = [0.0721, 0.5380]). Likewise, both PTSD and depression were significant mediators of the impact of sexual abuse on revictimization (as shown in Figure 2). Adolescent girls with histories of more severe sexual abuse experienced more revictimization, and this pathway was fully mediated by both PTSD and depression. In both pathways, the a and b paths were significant, and the c′ path was not. Results of the bootstrapping analyses demonstrated a significant indirect effect of sexual abuse on revictimization for both PTSD and depression.
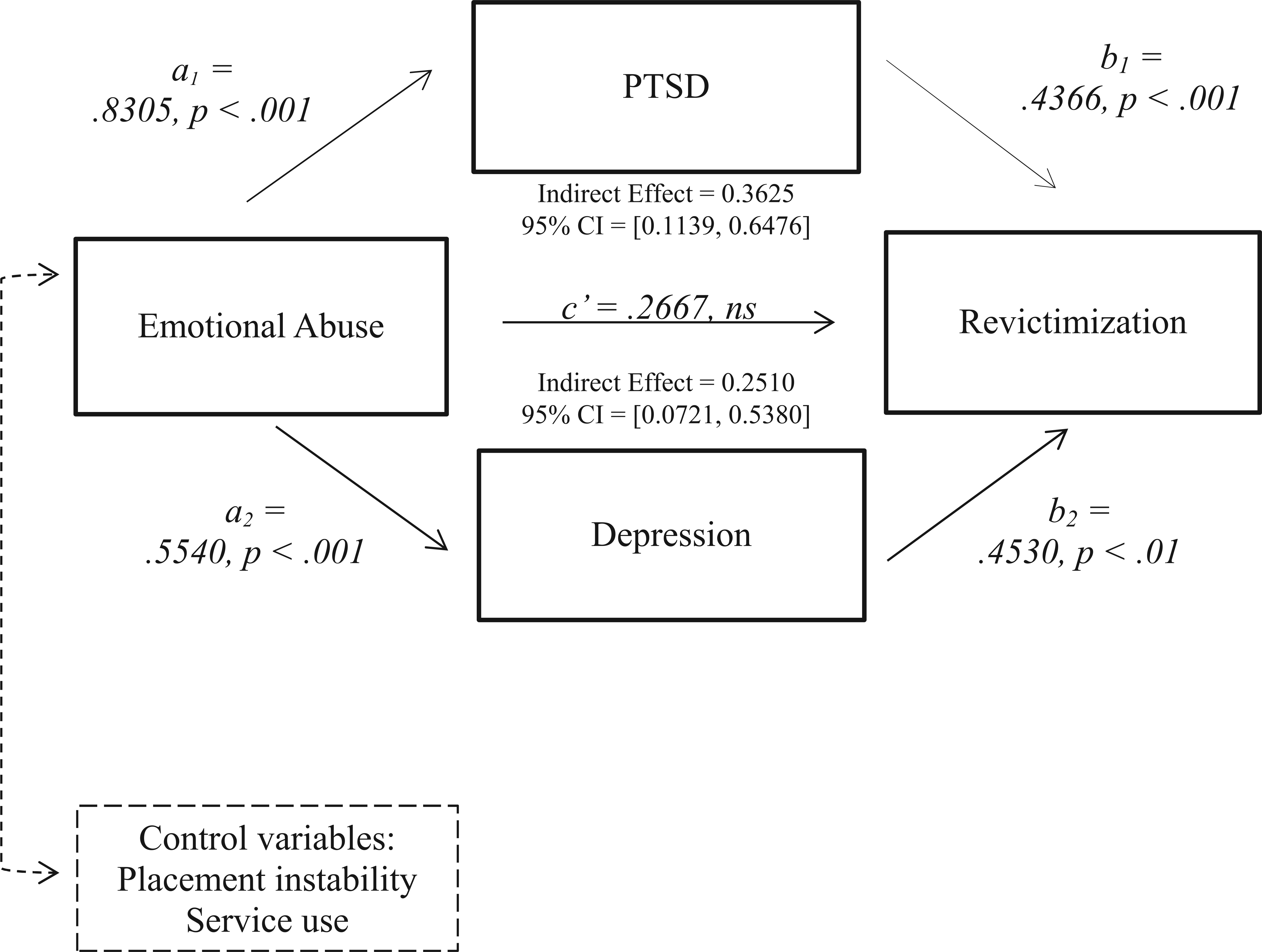
Parallel mediation analysis predicting the impact of histories of childhood emotional abuse on revictimization in adolescent girls.
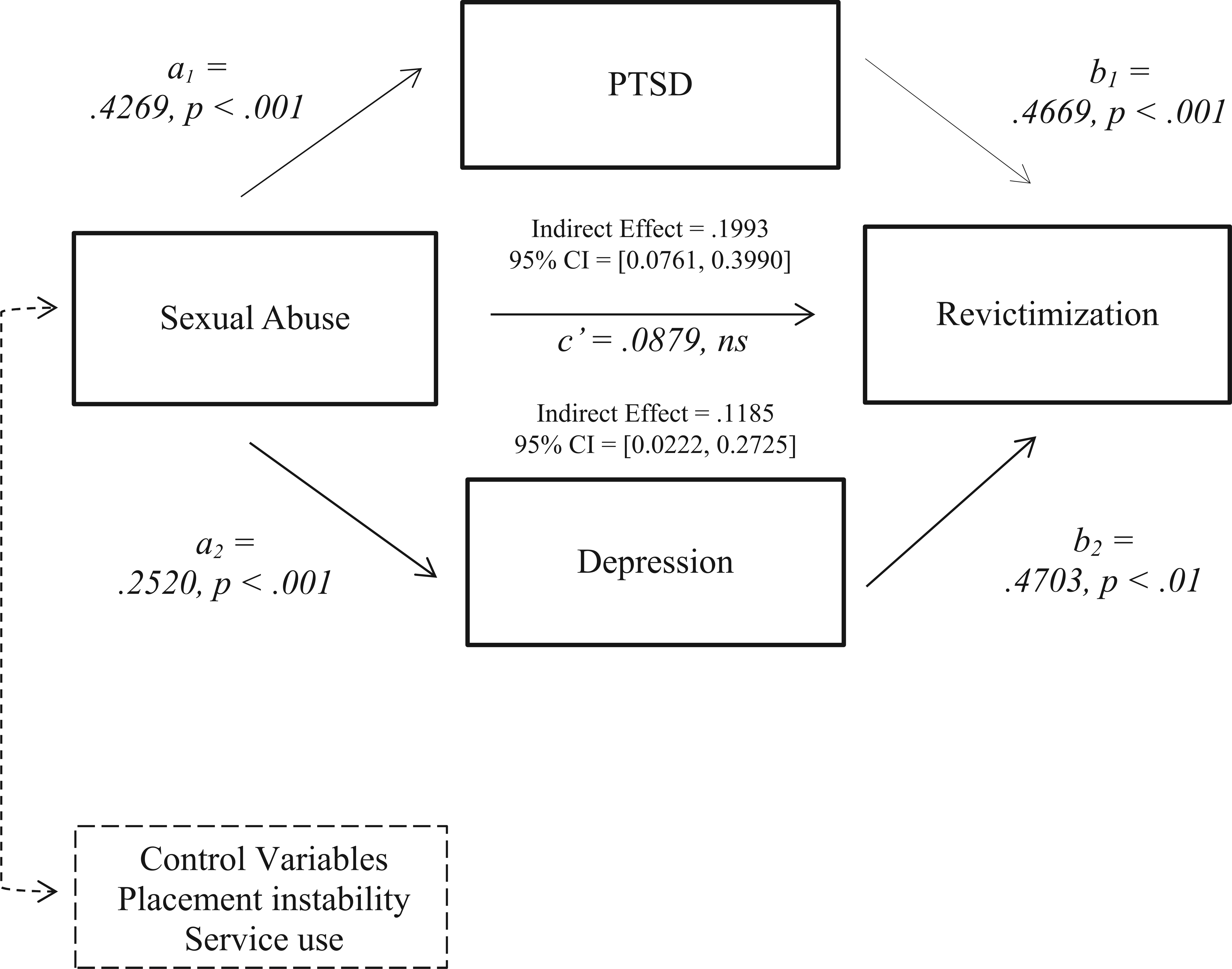
Parallel mediation analysis predicting the impact of histories of childhood sexual abuse on revictimization in adolescent girls.
The parallel multiple mediation analyses testing the relationship between physical abuse and revictimization failed to support the pathway with depression as a mediator. As shown in Figure 3, results showed that the a1 path from physical abuse to depression was not significant (β = .1642, p = .12) nor was the indirect effect of physical abuse on revictimization via depression (β = .0805, 95% CI = [−0.0055, 0.2668]). However, results supported the mediating pathway of PTSD between physical abuse and revictimization.
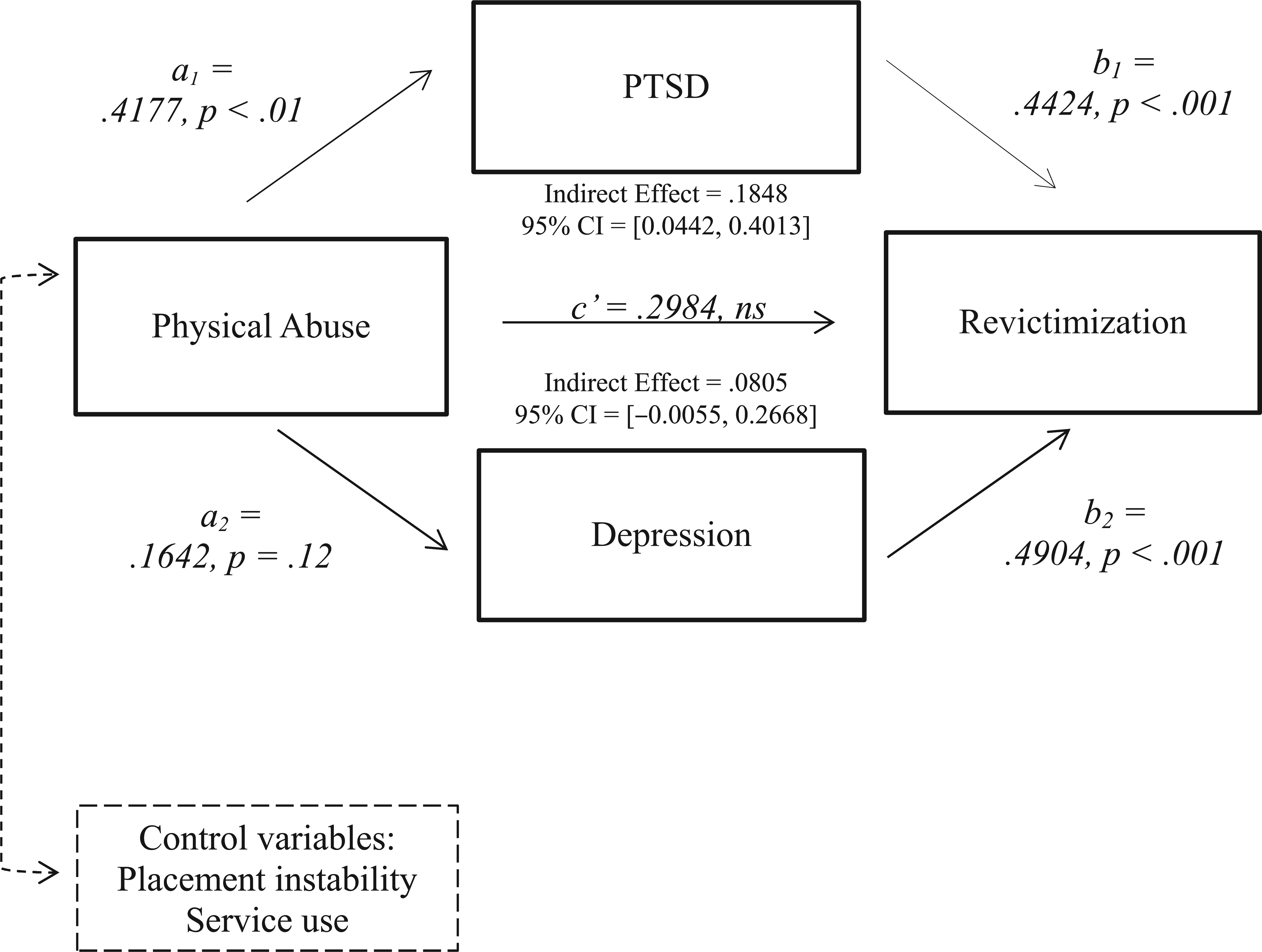
Parallel mediation analysis predicting the impact of childhood physical abuse on revictimization in adolescent girls.
Last, the parallel mediation model for PTSD and depression was not supported for the impact of physical neglect on revictimization. As shown in Figure 4, both a paths (i.e., a1 and a2) from physical neglect to PTSD and depression were not significant, nor were the indirect effects of physical neglect on revictimization (i.e., the confidence intervals contained zero).

Parallel mediation analysis predicting the impact of childhood physical neglect on revictimization in adolescent girls.
Discussion
The results of the current study compared four types of child maltreatment and two different mental health pathways with revictimization among adolescent girls involved in child welfare. Perhaps the most compelling finding was that there are similar pathways to revictimization in adolescents from both emotional and sexual abuse through posttraumatic stress and depression. The importance of this lies in the common assumption that emotional abuse is not as serious or damaging as sexual or physical abuse. Yet for the girls in this study, childhood histories of emotional abuse were significantly associated with posttraumatic stress and depression and increased their vulnerability to physical, verbal, and relational revictimization during adolescence.
In a recent study, Spinazzola and colleagues (2014) found that emotionally abused children experienced similar and in some cases higher rates of PTSD, depression, and other mental health problems than physically or sexual abused children. They found that when children experienced emotional abuse in conjunction with either physical or sexual abuse, they had significantly more severe negative psychological outcomes than those who had been physically and sexually abused without emotional abuse. In fact, both physical and sexual abuse had to occur simultaneously to induce the same negative effects as emotional abuse alone.
Clearly, evidence is growing that demonstrates the deleterious effects of emotional abuse, including an increased vulnerability to revictimization as a consequence of PTSD and depression. However, there is still a tendency in the child welfare system and other systems of care to focus on what are perceived to be more serious forms of child maltreatment—physical and sexual abuse. It is often more difficult to detect, substantiate, and take action in cases involving emotional abuse, especially if that is the only type of abuse occurring. This is further complicated by the definitions of emotional abuse that determine grounds for intervention by state child protective agencies. Most of the states define emotional abuse as “injury to the psychological capacity or emotional stability of the child . . . as evidenced by anxiety, depression withdrawal, or aggressive behavior” (Child Welfare Information Gateway, 2014, p. 3). Consequently, there must already be evidence of the harmful effects of emotional abuse on the child’s behavioral and mental health before a report can be made to child protective services. Practitioners, therefore, outside of the child welfare system may need to be poised to detect this insidious form of abuse and to assess and treat the early symptoms of PTSD and depression that these children and adolescents are likely to be experiencing. Assessment tools are available such as the Childhood Trauma Questionnaire (Bernstein & Fink, 1998) used in the current study and a subscale of the Child Abuse and Trauma Scale (Kent & Waller, 1998).
For both emotionally abused and sexually abused adolescents, trauma-focused cognitive-behavioral therapy in either the individual or group model has been shown to be effective in reducing PTSD and depression (Foa, Keane, Friedman, & Cohen, 2008; National Child Traumatic Stress Network, 2013). Moreover, among adult women, cognitive-behavioral therapy reduced PTSD and depressive symptoms and the likelihood of intimate partner violence (Iverson et al., 2011). Based on the mediating analysis of the current study, treatment of both PTSD and depression in emotionally and sexually abused girls involved in child welfare is warranted to prevent revictimization during adolescence.
It has been suggested that different types of maltreatment may lead to the same negative outcomes through different pathways or processes (Shaffer, Yates, & Egeland, 2009). Such appears to be the case with physical abuse. Posttraumatic stress was a significant mediator or pathway to revictimization, but depression was not. It has been theorized that depressed children can become targets for peer victimization because they are perceived as being less inclined to defend themselves or fight back (Fekkes, Pijpers, Fredriks, Vogels, & Verloove-Vanhorick, 2006). However, in the current study depression was not a significant pathway from physical abuse to revictimization, and in fact, the bivariate correlations indicate a weak significant relationship between physical abuse and depression. Another perspective is that children who are physically abused are more easily angered, have a hyper vigilant interpersonal style, and are more likely to be reactively aggressive with peers (Dodge, Bates, & Pettit, 1990; Messman-Moore et al., 2005). Further investigation comparing the role of depression as a pathway to revictimization and aggression toward others would be useful in designing prevention programs in this population.
The current study adds to the growing evidence that PTSD symptoms are associated with a heightened risk of revictimization and provides support for the mediating role of posttraumatic stress in the relationship between child maltreatment and revictimization (Messman-Moore et al., 2005; Messman-Moore, Ward, & Brown, 2009). Attentional interference to trauma stimuli in adolescent girls with intrusive PTSD symptoms may interfere with their inability to detect and avoid danger and may explain the heightened vulnerability to revictimization (Cougle et al., 2009; Pineles et al., 2009). In addition, in this population of girls who experienced childhood maltreatment, affect dysregulation is likely, with stressful situations leading to negative affective states and a reduced inability to avoid dangerous situations (Tanaka et al., 2011). To prevent revictimization, it is essential that adolescent girls involved in child welfare who have symptoms of posttraumatic stress as a result of physical, sexual, or emotional abuse have access to the most effective evidence-based treatment available such as Trauma-Focused Cognitive-Behavior Therapy (California Evidence-Based Clearinghouse for Child Welfare, 2014).
Neither posttraumatic stress nor depression was a significant mediator of the relationship between physical neglect and revictimization. Although physical neglect is a form of reportable child maltreatment which can lead to removal from the home, the current study indicates that the pathways and interrelationships between physical neglect, mental health outcomes, and revictimization are different from those of childhood emotional, physical, and sexual abuse. In the current study, childhood neglect was measured by items such as “When I was growing up, I didn’t have enough to eat” and “When I was growing up, my parents were too drunk or high to take care of the family.” Potentially, adolescents who experience physical neglect may hold different attributions from those who experience other forms of abuse, that is, youths may believe that their experiences of neglect are neither their fault nor an intentional act by their caregivers (as compared with emotional, physical, or sexual abuse). This may explain the weaker relationships found between childhood neglect, posttraumatic stress, and depression in this population. The current findings indicate that childhood neglect is significantly associated with higher levels of revictimization, yet more research is needed to better understand the pathways involved. One possible modifiable pathway may be negative parenting behavior, which is frequently associated with parental substance and alcohol use.
There are several limitations to the present study. First, cross-sectional data were utilized to determine the relationships between childhood abuse and neglect, symptoms of PTSD and depression, and revictimization, and a longitudinal design would be more rigorous. Second, our measure of physical, verbal, and relational revictimization did not specify who the perpetrator of the aggression was; it could have been a peer, family member, or some other person, as the items use the word “someone” instead of a more specific term. Although many of these items are similar to those used to assess bullying or peer victimization in schools, we cannot assume that this is the case. Third, it is important to note that the adolescents who participated in the current study were not a representative sample of girls served by the child welfare system, but a convenience sample of those who were referred for a trauma-focused group treatment. However, because we did not use a clinical cutoff score for either PTSD or depression as inclusion criteria, the current sample may be more representative of a general child welfare sample of female adolescents than a clinical sample. Furthermore, the majority of the sample was African American, and many of the girls may have experienced racially based revictimization that was not captured by our measures. Although White girls in the current study reported modestly higher rates of maltreatment, no racial differences were found in rates of revictimization, consistent with most of the existing literature (Jackson, O’Brien, & Pecora, 2011; Widom et al., 2008). Future studies of minority populations should consider forms of racially based aggression (e.g., discrimination, stereotyping, and microaggressions) as a type of revictimization that may be experienced by maltreated children. Last, because the purpose of the current study was to compare the mediating pathways of four types of abuse and neglect leading to revictimization, we did not examine the impact of co-occurring types of abuse and neglect. Some may argue that information is lost when maltreatment is classified into single types for analysis because it does not mirror reality. Moreover, we were not able to statistically control for the other types of abuse in each of the mediating models due to the high intercorrelations (i.e., multicollinearity) among the types of abuse. Examining the mediating pathways of polyvictimization and risk for revictimization (Hamby & Grych, 2013) in adolescent girls involved in child welfare would be beneficial in the future, particularly to create tailored treatment strategies for this population.
Despite these limitations, the current study has several strengths. Most importantly, many prior studies have included samples of adults who self-reported experiences of childhood abuse and/or neglect. This may be less accurate than the current study that included a sample that was formally investigated by workers from child protective services. Also, identifying mediating pathways during adolescence provides information that is useful for preventing dating and intimate partner violence in young adulthood. A second strength of the current study is the ability to compare pathways from four different types of maltreatment to revictimization. In particular, the current study includes emotional abuse, which has often been overlooked despite some evidence that the effects of emotional abuse are considered disabling and enduring (Shaffer et al., 2009). The measure of abuse and neglect used a continuous scale instead of a single dichotomous item that allowed us to capture the severity of the abuse and neglect. Last, the current study examined parallel mediator models and was able to control for other significant covariates.
In addition to posttraumatic stress and depression, other researchers have proposed a number of other mediators to explain the relationship between maltreatment and revictimization. For example, emotional dysregulation, anger, and social skills deficits have been identified as potential pathways to negative outcomes (Hong, Espelage, Grogan-Kaylor, & Allen-Meares, 2012). Future research would benefit from including more comprehensive and complex mediation and path models to examine the pathways from childhood abuse and neglect to revictimization in adolescent females and to further investigate gender differences.
Footnotes
Acknowledgements
The authors acknowledge the collaboration of Children’s Division of Missouri of St. Louis City and County, and Jefferson County.
Authors’ Note
Portions of this article were presented at the American Public Health Association Annual Meeting (2012) in San Francisco, CA; the Society for Social Work and Research (2013) in San Diego, CA; and the 13th European Society for Traumatic Stress Studies (2013) in Bologna, Italy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Grant 1R49CE001510 from the Centers for Disease Control and Prevention awarded to Washington University.