
Abstract
Previous studies have identified the predictive risk factors of child physical maltreatment (CPM). However, a significant number of these studies assessed risk factors in isolation. The cumulative risk hypothesis postulates that health problems are caused by the accumulation of risk factors, independently of the presence or absence of specific risk indicators. Few studies examined the effect of cumulative risk on CPM potential. This study aimed to test two concurrent models of cumulative risk of CPM potential by investigating whether CPM potential was better predicted by a threshold cumulative risk model or a linear cumulative risk model. Data from the National Representative Study of Psychosocial Context of Child Abuse and Neglect in Portugal were used. Parents of school-age children (N = 796) answered to self-report measures regarding sociodemographic variables, history of child maltreatment, psychological distress, and CPM potential. A cumulative risk index was computed, comprising 10 dichotomized risk factors. Evidence for a threshold cumulative effect was found. Additional bivariate logistic regressions revealed that the odds for high-potential CPM were dramatically higher for those parents with six or more risk factors when compared with parents with any one risk factor. By testing and confirming a threshold cumulative effect on CPM potential, it was possible to find a “trigger point” from which a dramatic increase in child physical maltreatment potential occurs.
Child physical maltreatment (CPM) is considered as a major public health problem in high-income countries (Gilbert et al., 2012; Gilbert et al., 2009). CPM is one of the major risk factors of physical and psychiatric problems during life span. Past research has evidenced that physically abused children report lower educational achievement and more incidence of anxiety, mood, and behavior disorders (Gershoff, 2002; Kim, Cicchetti, Rogosch, & Manly, 2009; Mills et al., 2011). In addition, adults with a history of physical abuse in childhood show more risk of suicide, more chronic health problems (Fuller-Thomson et al., 2010; Springer, Sheridan, Kuo, & Carnes, 2007), obesity (Alvarez, Pavao, Baumrind, & Kimerling, 2007), mental health disorders (MacMillan et al., 2001), substance and alcohol abuse (Anne Lown, Nayak, Korcha, & Greenfield, 2011; Spatz Widom, Marmorstein, & Raskin White, 2006), and more risk of unskilled employment and poverty (Currie & Widom, 2010). Adults physically abused in childhood also have more likelihood of suffering and perpetrating intimate partner violence and more risk to maltreat their children (McKinney, Caetano, Ramisetty-Mikler, & Nelson, 2009; Thompson et al., 2006) as well. Due the well-established individual, family, and social consequences of CPM, understanding the risk process is a main challenge to public health research.
Previous studies have systematically identified the most predictive risk factors of CPM. In a meta-analysis of 155 studies, Stith et al. (2009) found that parents’ characteristics, such as anger/hyperreactivity, psychopathology, depression, experiences of abuse in childhood, and unemployment, are major predictors of CPM risk. Similar findings were reported by other epidemiological, longitudinal, and cross-sectional studies (Euser, van IJzendoorn, Prinzie, & Bakermans-Kranenburg, 2010; Hurme, Alanko, Anttila, Juven, & Svedstrom, 2008; Machado, Gonçalves, Matos, & Dias, 2007; Parrish, Young, Perham-Hester, & Gessner, 2011; Wu et al., 2004). Nevertheless, past research showed that risk factors hardly operate in isolation, so that their combining and cumulative effect should be analyzed. Based on developmental-contextual models, the cumulative risk hypothesis posits that that human development may be jeopardized by “constellations of risk” rather than isolated adverse events (Evans, Li, & Whipple, 2013). This hypothesis asserts that the physical and psychological health outcomes are determined by the accumulation of risk factors, independently of the presence or absence of specific risk indicators (Appleyard, Egeland, Dulmen, & Alan Sroufe, 2005; Rutter, 1979; Sameroff, Seifer, Baldwin, & Baldwin, 1993; Sameroff, Seifer, Barocas, Zax, & Greenspan, 1987). Cumulative risk assessment assumes that the number of risk factors is a more efficient and accurate predictor of health and psychosocial problems than any single risk factor considered individually (Appleyard et al., 2005; Everhart, Fiese, & Smyth, 2008). A limitation of cumulative risk measurement is the absence of a theoretical basis for explaining its predictive power of developmental outcomes (Atkinson et al., 2015; Evans et al., 2013). However, cumulative risk metric is described as a parsimonious procedure for multiple risk measurement with high predictive power of a wide range of developmental outcomes, low sensitivity to risk collinearity, and high statistical power (Evans et al., 2013). This cumulative risk effect was found in a variety of health problems, such as pediatric asthma (Everhart et al., 2008), obesity (Evans, Fuller-Rowell, & Doan, 2012), stroke (Mohan et al., 2011), and psychopathological disorders (Appleyard et al., 2005).
Despite linearity in the cumulative risk:outcome function having been found in many studies, some empirical and theoretical research has also suggested that the function between multiple risk and target outcomes might not be always linear (Appleyard et al., 2005; Obradovic, Shaffer, & Masten, 2012). Also the predictive power of cumulative risk might be explained by an accelerating nonlinear function, indicating a “synergistic influence” on developmental outcomes (Evans et al., 2013). Therefore, previous studies have found two different models to explain the association between cumulative risk and unhealthy outcomes: additive (linear) and threshold (nonlinear-quadratic) cumulative risk models. The additive model defends a progressive linear effect of risk factors, with no multiplicative effect of the risk factor on each other, whereby the greater the number of predictors, the greater the prevalence of the outcome variable (Everhart et al., 2008; Horan & Widom, 2015; Sameroff et al., 1993). Conversely, the threshold cumulative risk model supports that the risk for a physical or psychological problem increases dramatically in the presence of a certain number of risk factors (Appleyard et al., 2005; Rutter, 1979). This quadratic trend model hypothesized that, beyond a certain number, the combined effect of the interactive accumulation of concurrent risk factors is more strikingly adverse than the summation of their effects (Appleyard et al., 2005; Jones, Forehand, Brody, & Armistead, 2002). Nevertheless, in an extensive state-of-the-art review, Evans et al. (2013) concluded that linearity in the multiple risk:outcome function has rarely been formally examined, and they advocated that future research should statistically test the nonlinearity of the cumulative risk:outcome function.
Despite cumulative risk measurement being a widespread procedure to examine the effect of multiple risk factors on specific outcomes in other scientific domains, few studies have tested the cumulative risk hypothesis on CPM and CPM potential (MacKenzie, Kotch, & Lee, 2011; Nair, Schuler, Black, Kettinger, & Harrington, 2003; Parrish et al., 2011; Straus, Gelles, & Steinmetz, 1980; Wekerle, Wall, Leung, & Trocmé, 2007). One cross-sectional study found evidence that the cumulative risk model is more predictive of CPM potential than Belsky’s developmental-ecological model (Belsky, 1993). A previous study with substance abusing mothers also found that mothers with five or more risk factors showed an increased risk of abusive parenting than mothers with fewer risk factors (Nair et al., 2003). In a retrospective population-based cohort study, Parrish et al. (2011) found evidence for a significant relationship between a steady accumulation of risk factors and the likelihood of reports of CPM. Such studies are essential for testing and finding evidence for a cumulative risk model of CPM, but their methodology presents some limitations for the prevention efforts in health services. First, these cumulative risk models (with exception of Parrish et al., 2011; Straus et al., 1980) were constructed based mainly on psychological latent constructs. Assessing these psychological constructs to screen cumulative risk in health care services could be ineffective because it is time-consuming and demands a highly specialized knowledge on scoring and interpreting psychological tests. Second, all of these previous studies only tested the linear cumulative risk model of CPM and, to our knowledge, no previous research assessed the nonlinearity of the cumulative risk:outcome function on prediction of the CPM potential. This is a major limitation as studies in other public health problems found that a quadratic model could better explain the cumulative risk mechanisms than a linear model (Everhart et al., 2008; Long, Marsland, & Alderfer, 2013; Oldfield, Humphrey, & Hebron, 2015; Shukla & Wiesner, 2013).
This study aims to address such limitations. The goal of the present study was to examine the relationship between a cumulative risk model and parents’ CPM potential. We also aimed to extend previous work on cumulative risk and adverse outcomes by assessing and comparing a linear and a quadratic model of cumulative risk in prediction of CPM potential. Based on the limited past research, we specifically hypothesized that cumulative risk index would predict CPM potential in a nonlinear-quadratic manner. Furthermore, as the amount of risk rose, CPM potential would exponentially increase in the presence of a certain number of risk factors.
Method
Participants
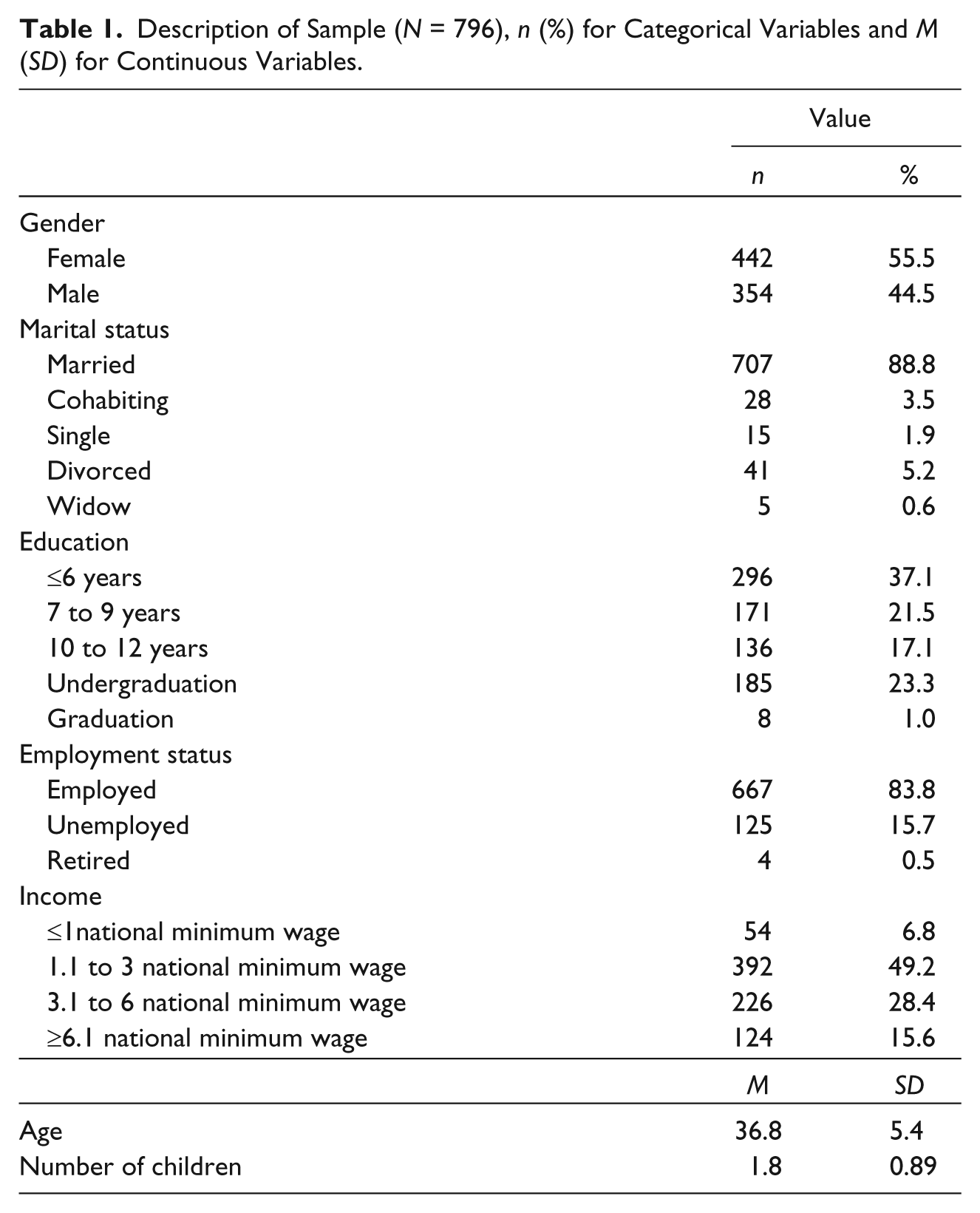
Participants were 796 parents (aged between 22 and 58 years; M = 36.8, SD = 5.4) who were living in Portugal during the year 2000. Demographic data are summarized in Table 1.
Description of Sample (N = 796), n (%) for Categorical Variables and M (SD) for Continuous Variables.
Procedure and Design
For the current study, data from the National Representative Study of Psychosocial Context of Child Abuse and Neglect in Portugal (PCCANP) were used. Participants were mothers and fathers of school-age children randomly selected in five public elementary schools of Northern Portugal. All parents whose children attended the selected schools were invited to participate in PCCANP in the year 2000 by letter. Subsequently, parents were also invited to participate in a meeting with teachers and research team members to elucidate the study’s aims and ethics procedures. In the next 2 weeks, teachers provided the assessment batteries in sealed envelopes to the children who, in turn, handed them to their parents. A total of 971 parents (533 mothers and 438 fathers) who consented to participate in this study completed and returned the assessment batteries in sealed envelopes to the teachers via their children. All participants provided written informed consent. No financial compensation was provided. The overall response rate of parents (i.e., in returning the questionnaires) was 69%. All relevant institutional review boards granted approval for this research. Detailed description regarding participants’ selection procedures is available in an earlier publication (Figueiredo et al., 2004). For current analyses, only participants without missing data were included (176 participants were excluded). No statistical differences between retained and excluded participants were found in main sociodemographic variables, such as age, t(969) = −.46, ns, gender, χ2(1) = .47, ns, marital status, χ2(1) = .009, ns, and number of children, t(969) = 1.71, ns.
Measures
CPM potential
Potential of CPM was assessed by the abuse scale of the Child Abuse Potential Inventory (CAPI; Milner, 1986). The CAPI is one of the most internationally used self-report instruments for screening child physical abuse risk. The CAPI abuse scale measures parents’ attitudes and practices regarding physical forms of discipline and abuse. Comprising a forced-choice format (0, no or 1, yes) the 74-items of the Portuguese version of the CAPI showed very good psychometric properties (Milner, 1986). For the current research, a unit (0/1) scoring procedure was applied, according to the scoring procedures proposed by the authors of the Portuguese version of the CAPI (Gomes, 2010). Total scores on the CAPI abuse scale range from 0 to 74, with higher scores reflecting more risk for child physical abuse. According to the Portuguese version of the CAPI manual, parents with a high potential for CPM are those who score higher than the cutoff value of 32 in the Abuse Scale (Gomes, 2010). The internal consistency for the total score in the current sample was excellent (Cronbach’s α = .91).
Measures of risk factors
Ten parents-related risk factors were included in the calculation of the cumulative risk index. The selection of these risk variables were based on past research (Appleyard, Berlin, Rosanbalm, & Dodge, 2011; Figueiredo et al., 2004; Hurme et al., 2008; Parrish et al., 2011; Stith et al., 2009; Wong, Chen, Goggins, Tang, & Leung, 2009). To compute the cumulative risk index, each of these 10 variables was first transformed into a dichotomous variable. For each variable, the absence or low risk was coded as 0, while the presence of risk was coded as 1. Then, the dichotomous variables were summed into a cumulative risk index for each participant. Total score in the cumulative risk index tabulated for each parent range from 0 (absence of any risk factor) to 10 (presence of all risk factors). Description of higher risk definition and prevalence of each variable are summarized in Table 2.
Risk Factors’ Definitions and Risk Prevalence for Each Risk Variable.

Note. BSI = Brief Symptom Inventory; PSDI = positive symptom distress index.
Risk coded as 1.
Marital status
Marital status assessed parents’ legal marital status at the time of the study and was dichotomized as married/cohabiting (coded as 0) or not married (coded as 1).
Number of children
Number of children was a continuous variable that was dichotomized as less than or equal to three children (coded as 0) or equal or greater than four children (coded as 1). No recommended risk cutoff was found in past research. Therefore, a conservative cutoff of four children was applied to dichotomize this variable.
Education
Education was dichotomized based on the 9 years of compulsory education specified by the Portuguese law. An education equal to or greater than 10 years were coded as 0 and education less than or equal to 9 years was coded as 1.
Income
The Portuguese national minimum wage in 2000 was used as the cutoff criteria to dichotomize the income variable. An income equal to or less than one national minimum wage was considered as higher risk (coded as 1), while an income equal or superior to 1.1 national minimum wage was considered as low risk (coded as 0).
Childhood and adolescence history of maltreatment and sequelae related to maltreatment
The Childhood History Questionnaire (Figueiredo et al., 2004; Milner, Robertson, & Rogers, 1990) is one of the most widely administered self-report questionnaires for screening the prevalence of physical maltreatment behaviors and physical abuse sequelae and injuries during childhood (before 13 years) and adolescence (after 13 years). Physical maltreatment behaviors are defined as whipping, slapping/kicking, poking/punching, and hair-pulling. The presence of bruises/welts, cuts/scratches, dislocations, burns, and bone fractures are considered as physical abuse sequelae/injuries. Only the items related to physical maltreatment and related sequelae were computed for current analyses. For variables dichotomization, the presence of any type of physical maltreatment in childhood and adolescence was coded as 1, while the absence of maltreatment behaviors was coded as 0. In addition, for variables “childhood physical maltreatment sequelae/injuries” and “adolescence physical maltreatment sequelae/injuries,” reports of sequelae/injuries caused by physical maltreatment were coded as 1 and the absence of physical maltreatment sequelae/injuries was coded as 0.
Psychological distress
The Brief Symptom Inventory (BSI) was used to examine nine patterns of clinically relevant psychopathological symptoms (Derogatis & Melisaratos, 1983). BSI instructions ask participants to rate the occurrence of 53 symptoms in the past week on a scale ranging from 0 (not-at-all) to 4 (extremely). The Portuguese version of BSI revealed good psychometric properties (Canavarro, 1999). For current analyses, the positive symptom distress index (PSDI) was computed. According to validation studies of the Portuguese version of the BSI, the BSI-PSDI is the best index to discriminate between the presence and absence of psychopathological disorder in the general population. The variable dichotomization was based on the BSI-PSDI cutoff score recommended in the Portuguese population (1.70; Canavarro, 1999). Accordingly, a score equal to or greater than 1.70 was coded as 1 (high probability of psychopathological disorder) and a score equal or lower than 1.69 was coded as 0 (low probability of psychopathological disorder).
Data Analysis
Descriptive statistics of each variable were generated and correlational analyses were performed to investigate whether all dichotomized risk variables were significantly associated with parents’ CPM potential. The prevalence of higher risk for each variable was determined by computing the percentage of parents that scored 1 in each risk variable. Student’s t test analyses were conducted to examine mean differences between parents classified as low risk (absence of the risk factor) and high risk (presence of the risk factor) in each variable. Cohen’s d effect size was also calculated for statistically significant differences between groups. Hierarchical multiple regression analyses were conducted to test the cumulative risk effect on prediction of CPM potential. The cumulative risk index was entered as a linear term in Step 1 and as a quadratic term in Step 2. Cohen’s ƒ2 effect size for hierarchical multiple regression was also computed to compare the relationship between linear and quadratic cumulative risk models with CPM potential scores. Finally, independent logistic regressions were conducted to compare the odds of child maltreatment potential between the reference group (parents with no risk factors) and the other risk groups. All analyses were conducted using IBM SPSS 19.
Results
Risk Measures and Cumulative Risk Index
Prevalence for each variable included on the cumulative risk index is presented in Table 2. Prevalence of each risk factor among parents ranged from 5.8% in the income variable and 70.9% in childhood maltreatment without sequelae/injuries. Parents’ mean total score of the cumulative risk index was 2.53 (SD = 1.63, range 0 to 9 risk factors). Among the participants, 56 parents (7%) did not present any risk factor, 380 parents (47.7%) had between 1 and 2 risk factors, 317 (39.8%) between 3 and 5 risk factors, and 43 parents (5.5%) between 6 and 9 risk factors. Cumulative risk index differed by parent’s gender, t(794) = 2.8, p = .005; Cohen’s d = .20, with fathers reporting significantly less cumulative risk than mothers (fathers: M = 2.67, SD = 1.76; mothers: M = 2.35, SD = 1.42). Cumulative risk index was not correlated with parents’ age, r = −.03, p = .31.
Parents’ Child Maltreatment Potential
The mean CAPI score was 22.04 (SD = 12.43, range 2-64). Differences in child maltreatment potential were found regarding parents’ gender, t(494) = 4.66, p = .001; Cohen’s d = .30, with mothers reporting higher potential for physically maltreating their children. The mean CAPI scores for fathers was 19.77 (SD = 11.45) and 23.85 (SD = 12.89) for mothers. No association between parents’ age and CAPI scores was found, r = .05, p = .16.
All dichotomized risk variables were positively and significantly associated with CPM potential (Table 3). Parents’ mean CAPI scores differed across all variable risks, with parents in the risk factor group reporting higher scores of CPM potential for each variable (Table 4). Cohen’s d effect size ranged from −0.20 to −1.80. Large effect sizes (Cohen’s d ≥ 0.8) in the mean differences between high risk and low risk groups were found for 5 risk variables: marital status, number of children, income, adolescence physical maltreatment with sequelae/injury, and psychological distress. Conversely, a small effect size (Cohen’s d ≤ 0.2) was found only for childhood physical maltreatment without sequelae/injury variable (Table 4).
Bivariate Correlations Between Each Risk Factor and the Cumulative Risk Index and With the Child Physical Maltreatment Potential.

Note. CAPI = Child Abuse Potential Inventory.
p = .05. **p = .001.
Differences in CAPI Scores in Each Dichotomized Risk Variable.
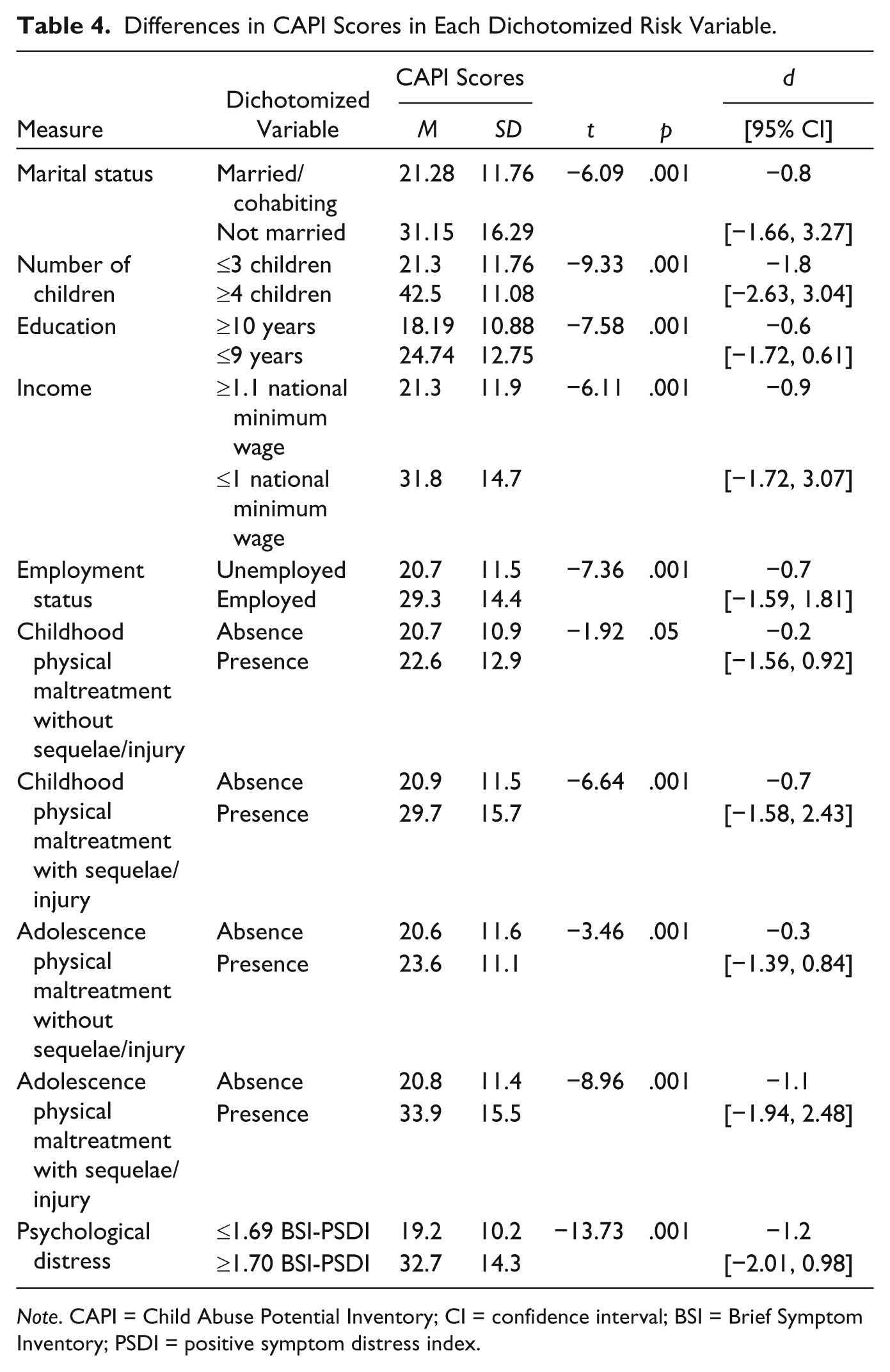
Note. CAPI = Child Abuse Potential Inventory; CI = confidence interval; BSI = Brief Symptom Inventory; PSDI = positive symptom distress index.
Test of Linear Versus Quadratic Models of Cumulative Risk
According to the results presented in Table 5 and Figure 1, the cumulative risk model significantly predicted parents’ CAPI scores as a quadratic function, F(1, 793) = 145.62, p = .001. The addition of the quadratic term to the regression model contributed to a significant improvement in fit over the linear function, ΔF(1, 793) = 17.6, p = .001. Additional variance in parents’ CAPI scores was accounted for the quadratic function beyond that explained by the linear function (R2 = .27, ΔR2 = .02). Moreover, the comparison of Cohen’s effect sizes for the linear (ƒ2 = .33, 95% confidence interval [CI] = [.24, .43]) and quadratic (ƒ2 = .37, 95% CI = [.28, .48]) cumulative risk models showed a stronger association between the quadratic approach and the parents’ CAPI scores. Parents’ CPM potential increased as the presence of cumulated risk increased and a threshold effect was found to exist in the presence six risk factors (Figure 1). Subsequent bivariate logistic regressions revealed that, when compared with parents with no risk factors, the odds of having high CPM potential (CAPI cutoff ≥ 32) were 4.8 times greater for parents with four risk factors (95% CI = [1.73, 13.5]), and were 8.5 times greater for parents with five factor risks (95% CI = [2.84, 25.4]). However, the odds of having CPM potential were 52.5 times greater for those with six or more risk factors (95% CI = [15.4, 178.5]; Table 6). In the current sample, 112 mothers and 54 fathers scored above the CAPI 32-point cutoff.
Hierarchical Multiple Regression Results for Linear and Quadratic Cumulative Risk Models.
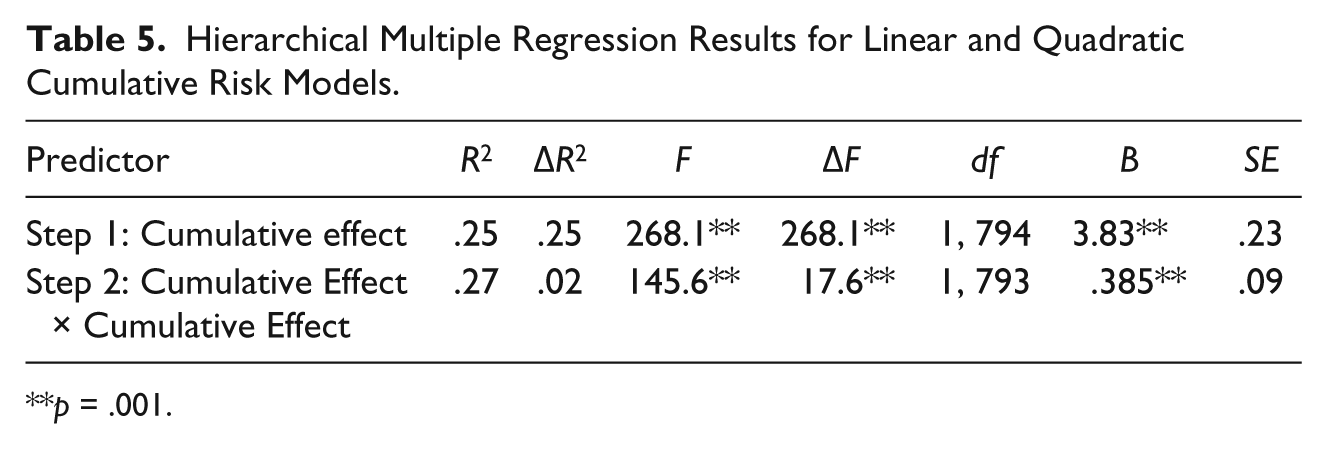
p = .001.
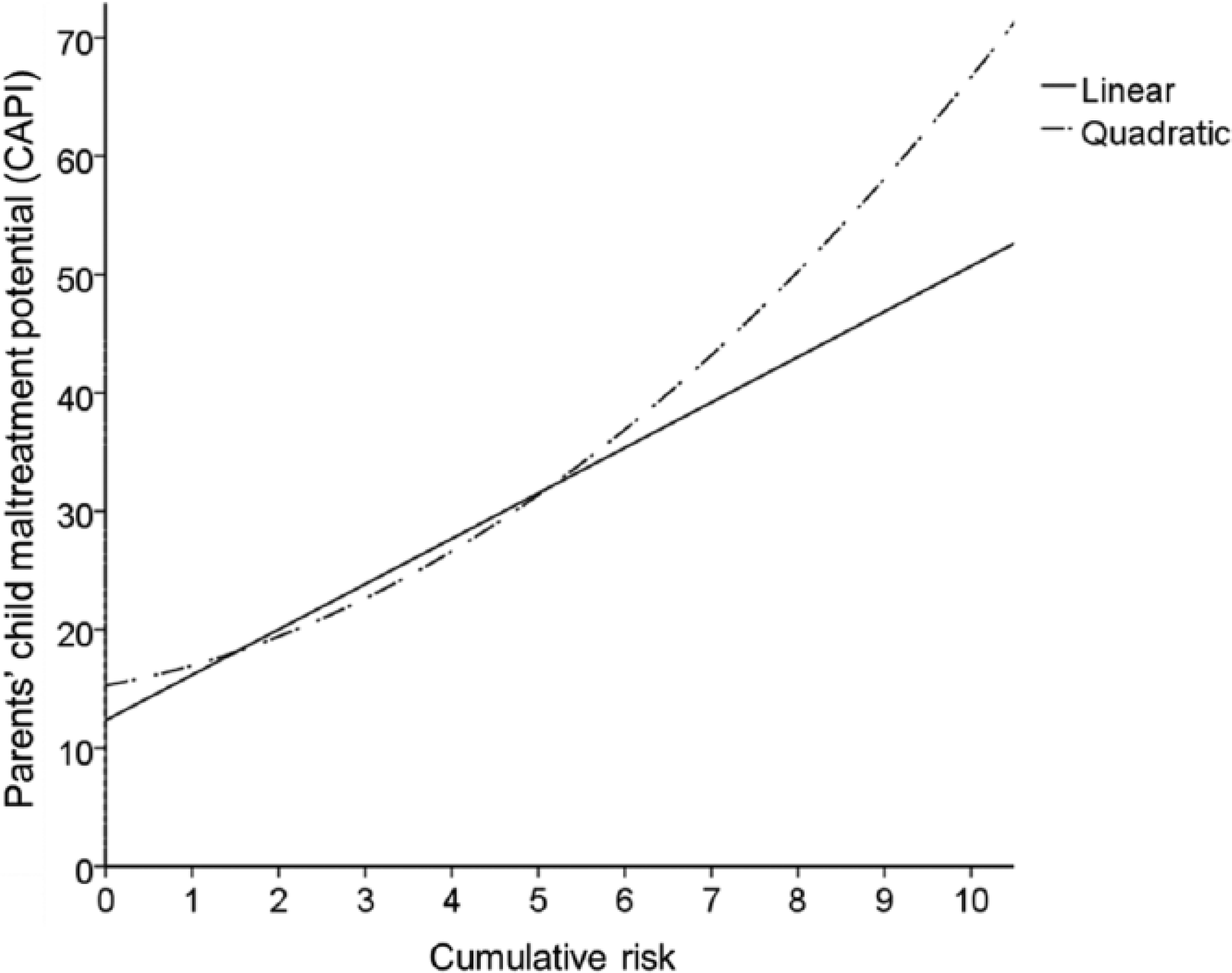
Mean of parents’ child maltreatment potential for each level of the cumulative risk model.
Independent Logistic Regressions.
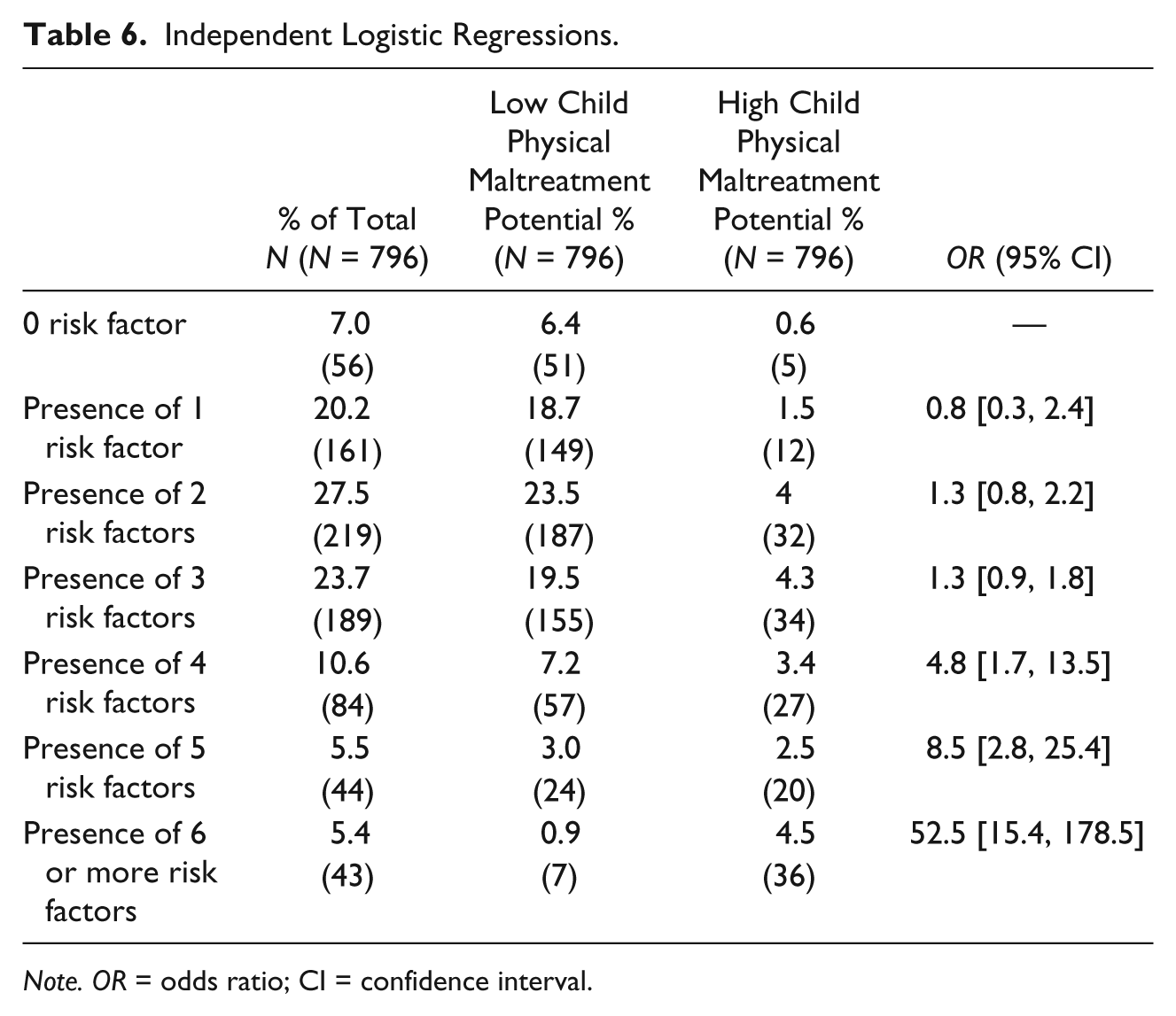
Note. OR = odds ratio; CI = confidence interval.
Discussion
The main aim of the current study was to examine which cumulative risk model (linear vs. threshold) better predicted parents’ CPM potential. Using a low-risk community sample, these results showed evidence for a threshold cumulative effect by demonstrating a dramatic increase of CPM as the risk factors accumulate and interact with one another. As represented in Figure 1, the nonlinear-quadratic cumulative risk model shows a better fit to the data than the linear additive model. In addition, bivariate logistic regressions revealed that the odds for high-potential CPM were substantially greater for parents with four and five risk factors and dramatically higher for those parents with six or more risk factors. The evidence for a threshold cumulative effect of risk factors may assume a major contribution for prevention of CPM. Indeed, current results suggest that a cumulative risk model comprised by parents’ sociodemographic variables and global psychological distress is statistically significant in screening high-risk parents for CPM. Moreover, these results also contribute to prevention science by pointing out that an increased effect on reduction of CPM potential should be produced when prevention strategies tackle several risk factors synchronously. These results may suggest that focusing only on one risk factor could significantly decrease the effectiveness of prevention strategies in the reduction of CPM in high-risk families.
In fact, testing only the linear model, two main findings would be found that would not be the fully representation of how risk accumulation predicts parents’ CPM potential. First, it would be found that CPM potential gradually increases as risk factors increase and, second, a linear model would assume that on average all parents experienced a similar rate of increase of CPM potential. In fact, by testing the threshold model, it was possible to find a “trigger point” at which a dramatic increase in child maltreatment potential occurs. Findings suggest that previous studies that focused on testing risk factors of CPM separately could have overvalued the predictive association between that specific risk factors and parents’ CPM potential. In addition, past research studying the separate effect of particular risk factors on CPM potential could also have underestimated the presence of other risk factors and their combined effect and produced an incorrect assessment of child’s maltreatment risk level.
The results of this research should be interpreted bearing some limitations in mind. Common limitations of cumulative risk models are the assumption of equal weight for each of the risk factors and failure to consider that certain patterns of combined effect of risk factors can contribute to the increased probability of CPM (Everhart et al., 2008). As some studies in other public health problems have suggested that risk factors may not co-occur randomly (Bailey & Scott, 2008; Evans et al., 2013), future research on CPM potential should also apply more sophisticated statistical designs to address this limitation. A second limitation of this study is the dichotomization of the risk variables. Despite not sample-dependent cutoff criteria being applied in the dichotomization of the two continuous risk factors, it is essential to mention that cumulative risk index is specific to the current sample and dependent on mean of the participants on each risk indicator. Therefore, generalization of results should be considered with caution. An additional caveat that should be considered is the wide confidence intervals for odds ratios found in some groups (mainly in the six or more risk factors group). These confidence intervals, which could be explained by the small group sizes (Prel, Hommel, Röhrig, & Blettner, 2009), might decrease the precision of these estimates. Third, although fathers and mothers of the same family could participate in the study, no question was included in the assessment protocol to identify both parents of the same family, precluding a coding strategy to associate answers of fathers and mothers of the same family in the database. This could increase the probability of unmodeled dependencies within data, which could have partially affected the statistical analyses by overestimating the effects of some variables that parents of the same family could have answered in a similar way. However, earlier research suggested that CPM potential scores between mothers and fathers of the same family would be statistically independent (e.g., Miragoli, Camisasca, & Blasio, 2015; Moore & Florsheim, 2008), indicating that interindividual variability in CPM potential found in our study might not be a by-product of unmodeled dependencies. Finally, only CPM potential was assessed rather than actual CPM. Despite CAPI predictive validity of future being relatively well established in the literature (Milner & Crouch, 2012; Walker & Davies, 2010), other studies suggest that CPM potential and actual CPM were only moderately associated (e.g., Rodriguez, 2006). Therefore, no direct and linear inferences about current CPM potential on parents’ actual CPM behaviors should be assumed. Future research should assess actual CPM behaviors, using self-reports (e.g., the Parent-Child Conflict Tactics Scale; Straus, Hamby, Finkelhor, Moore, & Runyan, 1998) and other data collection methods (e.g., Child Protective Services records). Despite these limitations, to our knowledge, this research was the first to demonstrate a threshold cumulative effect of CPM potential. These findings are useful to public health services as they contribute to the increased accuracy in identification of low-, moderate-, and high-risk parents of CPM (Dubowitz & Bennett, 2007), contributing, in this way, to the effectiveness of universal, selective, and indicated prevention strategies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Portuguese Foundation of Science and Technology through a research grant to the second author (POCTI/PSI/14276/1998).