
Abstract
The present study examined heart rate and heart rate variability (i.e., respiratory sinus arrhythmia [RSA]) in a sample of 48 general population parents (41.7% fathers), who were either at high risk (n = 24) or low risk (n = 24) for child physical abuse. During baseline assessments of heart rate and RSA, parents sat quietly for 3 min. Afterward, parents were presented with a series of anagrams (either easy or difficult) and were instructed to solve as many anagrams as possible in 3 min. As expected, high-risk (compared with low-risk) parents evinced significantly higher resting heart rate and significantly lower resting RSA. During the anagram task, high-risk parents did not evince significant changes in heart rate or RSA relative to baseline levels. In contrast, low-risk parents evinced significant increases in heart rate and significant decreases in RSA during the anagram task. Contrary to expectations, the anagram task difficulty did not moderate the study findings. Collectively, this pattern of results is consistent with the notion that high-risk parents have chronically higher levels of physiological arousal relative to low-risk parents and exhibit less physiological flexibility in response to environmental demands. High-risk parents may benefit from interventions that include components that reduce physiological arousal and increase the capacity to regulate arousal effectively.
Etiological theories of child physical abuse (CPA) risk propose that a variety of risk factors (including physiological, cognitive, emotional, and social factors) coalesce to explain why some parents respond with aggressive, and in some cases abusive, behavior toward their children (e.g., Azar, Reitz, & Goslin, 2008; Milner, 1993, 2000). With respect to physiological functioning, it has been hypothesized that high-risk/abusive parents experience greater increases in arousal in response to aversive events and environmental challenges, which some have referred to as physiological “hyper-reactivity” (e.g., Knutson, 1978). Greater physiological reactivity in response to stressors/challenges may be indicative of stronger negative emotional reactions, lower levels of impulse control, and increased risk for aggression (for reviews, see McCanne & Hagstrom, 1996; McCanne & Milner, 1991).
Reactivity Hypothesis
Several studies support the hypothesis that high-risk and abusive parents display greater sympathetic activation in response to stressors. For example, Frodi and Lamb (1980) reported that abusive, compared with nonabusive, parents displayed greater acceleration in heart rate and higher magnitude skin conductance following exposure to a 2-min video segment of a crying infant. Similarly, Crowe and Zeskind (1992) found that high CPA risk undergraduates, compared with their low CPA risk counterparts, evinced marginally higher heart rates, as well as greater changes in heart rate (relative to baseline), following exposure to a series of 10-s audio recordings of infant cry sounds. Interestingly, Casanova, Domanic, McCanne, and Milner (1992) extended these findings by demonstrating that high, compared with low, risk mothers displayed significantly greater increases in skin conductance during a nonchild-related stressor (i.e., a cold pressor task). Collectively, these studies support the notion that abusive and at-risk individuals experience greater sympathetic activation in response to a variety of stressors (i.e., infant crying, a painful task).
Chronic Arousal Hypothesis
Although the studies described above provide evidence consistent with the reactivity hypothesis, it is noteworthy that several studies failed to support the notion that high-risk/abusive parents respond to stressors with greater increases in arousal than low-risk/nonabusive parents. Indeed, findings from several studies indicate that high-risk parents are not more reactive to stressors but rather experience chronic levels of physiological arousal (i.e., high levels of arousal across situations). In one of the earliest studies on the topic, Disbrow, Doerr, and Caulfield (1977) examined heart rate among 22 physical abusers, 24 neglectors, and 50 control parents. Consistent with the chronic arousal hypothesis, the mean heart rate of abusers/neglectors was higher than that of controls across a series of video segments that depicted neutral, pleasant, and unpleasant parent–child interactions. Moreover, Disbrow et al. reported that nonmaltreating parents showed significant changes in heart rate across the neutral, pleasant, and unpleasant video segments, whereas the abusive parents’ heart rates “showed no significant differentiation” (p. 290) across the video segments.
Similarly, Pruitt and Erickson (1985) examined whether high-risk parents and low-risk parents differed in their physiological responses to video recordings of an infant who was quiescent, smiling, or crying. Pruitt and Erickson reported that the “high abuse potential group had a consistently higher peak heart rate throughout the videotape presentations” (p. 110), with no significant differences in peak heart rate across the video segments. In keeping with the findings of Disbrow et al. (1977), the low-abuse potential group experienced significant changes in peak heart rate across the quiet/smiling/crying infant video segments, suggesting that the low-risk parents were more physiologically responsive to the different infant states.
In a related study, Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al. (2013) examined physiological responses of mothers classified as either high in sensitivity or low in sensitivity based on observational ratings of parent–child interactions. Joosen and colleagues presented parents with a series of 10-s audio-recorded segments of infant cry sounds and found that parents classified as low in sensitivity evinced higher baseline heart rates and higher heart rates across the cry paradigm compared with highly sensitive parents. Similar to the findings of Disbrow et al. (1977) and Pruitt and Erickson (1985), Joosen and colleagues found that more sensitive parents, compared with less sensitive parents, evinced more pronounced increases in heart rate following exposure to the infant cry sounds.
Thus, although several studies provided evidence consistent with the notion that high-risk/abusive parents display greater sympathetic activation in response to stressors (e.g., Casanova et al., 1992; Crowe & Zeskind, 1992; Frodi & Lamb, 1980), there is accumulating evidence that high-risk/abusive parents may present with chronic states of physiological arousal (e.g., Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013; Pruitt & Erickson, 1985) and display limited variability in arousal in response to environmental stressors (e.g., Disbrow et al., 1977; Pruitt & Erickson, 1985; Reijman et al., 2014). Additional research is needed to better understand these contrasting findings.
Respiratory Sinus Arrhythmia (RSA): An Index of Parental Regulatory Capacity
Another indicator of physiological reactivity to stressors is heart rate variability (HRV; also known as vagal tone). Although heart rate (e.g., beats per minute) provides an indication of arousal level, an examination of the time intervals between heart beats (i.e., interbeat intervals) provides information about the relative influences of the sympathetic and parasympathetic nervous systems on the heart (Berntson et al., 1997). A variety of indices may be used to quantify different aspects of HRV. A growing body of research on self-regulation has focused on HRV as it occurs over the respiratory cycle, which is referred to as RSA. High RSA is indicative of higher levels of parasympathetic inhibitory control within the autonomic nervous system and is associated with greater self-reported emotion regulation, lower levels of negative emotional arousal in response to stress, and more effective coping (for reviews, see Appelhans & Luecken, 2006; Porges, 2011; Thayer & Lane, 2000).
Research examining patterns of RSA in parents as they respond to caregiving challenges is still in its early stages and findings have been mixed. The initial studies on this topic proposed that parents who exhibit more adaptive caregiving behaviors tend to evince higher baseline RSA (e.g., Perlman, Camras, & Pelphrey, 2008) and experience decreases in RSA in response to parenting challenges (e.g., child negativity, infant crying; for example, Mills-Koonce et al., 2007; Moore et al., 2009).
Baseline RSA
Results reported by Joosen and colleagues (Joosen, Mesman, Bakermans-Kranenburg, & IJzendoorn, 2013; Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013) support the prediction that parents who display more adaptive caregiving behaviors (i.e., high sensitivity, low harshness) exhibit higher levels of baseline RSA. Specifically, Joosen and colleagues reported two studies in which they observed parents interacting with their preschool-age children. Based on these observations, parents were classified as (a) high or low in sensitivity (Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013) and (b) high or low with respect to harsh parenting (Joosen, Mesman, Bakermans-Kranenburg, & IJzendoorn, 2013). Consistent with the view that higher baseline RSA is associated with more adaptive caregiving, the more sensitive/less harsh mothers exhibited higher resting RSA.
In contrast, Skowron and colleagues (Skowron, Cipriano-Essel, Benjamin, Pincus, & Van Ryzin, 2013; Skowron et al., 2011) assessed baseline RSA in samples of maltreating (i.e., substantiated for physical abuse and/or neglect) and nonmaltreating mothers and failed to find expected differences in baseline RSA. Nonetheless, the patterning of the baseline RSA means was as expected (i.e., maltreating < nonmaltreating) and power was limited due to small sample sizes (e.g., physically abusive mothers, n = 17). Moreover, presentation of a calming “bedtime” video during the baseline assessments in the Skowron et al. studies may have reduced the likelihood of detecting differences in baseline RSA between the maltreating and nonmaltreating groups.
In another recent study, Reijman et al. (2014) also failed to find baseline differences in RSA when comparing mothers substantiated for maltreatment (neglect only, n = 20; neglect with physical abuse, n = 22) and a sample of nonmaltreating mothers (n = 38). However, as pointed out by Reijman et al., the use of an “at risk” nonmaltreating group (i.e., mothers of children with at least one clinical diagnosis) may have reduced the likelihood of finding differences between the maltreatment and control groups. Clearly, findings from studies examining RSA in at-risk and maltreating parents are mixed, and additional research examining RSA in parents at risk for CPA is warranted.
RSA Change in Response to Stressors
Studies examining RSA change in response to stressors (e.g., infant crying) also have produced mixed results. Joosen and colleagues found that parental sensitivity moderated the pattern of RSA change exhibited in response to a series of 20-s audio recordings of infant cries played at various frequencies (Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013). Specifically, more sensitive mothers exhibited significant RSA withdrawal (i.e., reductions in RSA relative to baseline) in response to infant cry sounds; however, RSA withdrawal in response to infant cry sounds was not observed among less sensitive parents.
However, Reijman et al. (2014) utilized the same infant cry procedure as Joosen and colleagues (i.e., 20-s audio recordings of infant cries played at various frequencies; Joosen, Mesman, Bakermans-Kranenburg, & IJzendoorn, 2013; Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013) and found that neither maltreating nor nonmaltreating mothers exhibited changes in response to the infant cry sounds. As noted above, the fact that the nonmaltreating mothers recruited in the Reijman et al. study were considered an “at risk” comparison group (given that all mothers had children who had at least one clinical diagnosis) may have reduced the likelihood of detecting differences between the maltreating mothers and the nonmaltreating mothers.
Synopsis and Limitations
Early theories of CPA risk suggested that high, but not low, CPA risk parents experience greater increases in physiological arousal in response to stressors, such as infant crying (i.e., Knutson, 1978). However, findings across studies are mixed, and some have observed that high CPA risk parents experience chronic states of physiological arousal (e.g., for a discussion, see McCanne & Milner, 1991), with little to no change in arousal in response to changes in environmental demands (e.g., Disbrow et al., 1977; Pruitt & Erickson, 1985; Reijman et al., 2014). Chronic states of physiological arousal may reflect lower levels of parasympathetic control within the autonomic nervous system (i.e., poor vagal tone). Researchers recently began examining RSA (as an index of vagal tone) in at-risk/abusive parents; however, results to date are mixed (e.g., Joosen, Mesman, Bakermans-Kranenburg, & IJzendoorn, 2013; Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013; Reijman et al., 2014; Skowron et al., 2013; Skowron et al., 2011).
The present study sought to extend our understanding of how parents at risk for CPA respond physiologically to environmental challenges. Specifically, we assessed heart rate and RSA in parents during a 3-min baseline period as well as during a cognitively challenging task (i.e., an anagram task). Although most studies examining physiological reactivity in at-risk/abusive parents focused on infant crying as a stressor, the findings reported by Casanova et al. (1992) indicated that CPA risk group differences in physiological functioning may extend to nonchild-related stressors (e.g., a cold pressor task). In our study, the anagram task served as a nonchild-related cognitive challenge that was either easy or difficult, allowing us to examine whether cognitive challenges of varying difficulty moderate CPA risk group differences in physiological functioning. Moreover, the anagram task was designed to be challenging but was not expected to be especially aversive, thus mimicking the types of cognitive problem solving that parents engage in routinely. We designed the present study to extend prior research by examining RSA in parents classified as either high risk or low risk using a validated risk screening tool designed to assess CPA potential. Consistent with the chronic arousal hypothesis, we predicted the following:
Method
Participants
The data presented herein were drawn from a larger study on pain tolerance and CPA risk (Hiraoka et al., 2014). The heart rate and HRV data reported in the present study are not included in any prior publication. An initial pool of 133 parents (81 mothers and 52 fathers) was recruited to participate in the parent study. Among the initial pool of 133 parents, we excluded 28 parents due to invalid responding on the Child Abuse Potential (CAP) Inventory (22 faked good, 1 faked bad, 2 randomly responded) or because they had excessive missing data (i.e., greater than 10% missing on any measure; n = 3). Collection of the heart rate and respiration rate data was initiated midway through the larger study, resulting in heart rate and respiration rate data being obtained from only the last 62 parents. Among the 62 parents who provided physiological data, 14 were excluded due to the fact that their respiration rates (during either the baseline or the anagram task) fell outside of the standard respiration frequency band (i.e., 0.12-0.40 Hz; see Berntson et al., 1997). Thus, the final sample for the present study was 48 parents. The demographic characteristics (i.e., gender, age, race/ethnicity, educational attainment, annual household income, marital status, number of children) of the 48 parents included in the present analyses did not differ significantly from the demographic characteristics of parents who were recruited into the parent study but were not included in the present study (all ps > .10).
Of the 48 parents (20 fathers and 28 mothers) included in the present analyses, 58.3% were African American, 39.6% were Caucasian, and 2.1% were Latino. The mean age was 37.7 years (SD = 11.4). Mean highest level of education completed was 13.4 years (SD = 2.0). The median annual household income was US$20,000, and the mean annual household income was US$27,701 (SD = US$26,471). With regard to marital status, 43.8% were single, 37.4% were married/cohabitating, and 18.8% were separated/divorced. Mean number of children was 2.6 (SD = 1.6).
Measures
CAP Inventory
The CAP Inventory (Milner, 1986) is a 160-item, agree–disagree, self-report questionnaire designed to screen for CPA risk. Scores on the physical abuse scale range from 0 to 486, with higher scores reflecting greater potential for CPA. The CAP Inventory contains three validity indices (i.e., random responding, faking good, and faking bad) that were used to detect response distortion. We classified respondents as low CPA risk if their CAP abuse scores were below the signal detection theory cut score (i.e., 166; Milner, 1986), and no validity indices were elevated. We classified respondents as high CPA risk if they obtained CAP abuse scores at or above the signal detection theory cut score of 166, and the CAP validity indices indicated that they had not faked bad or randomly responded.
Research on the CAP Inventory has documented adequate internal consistency estimates (ranging from .92 to .95 for general population and maltreating parents) and adequate test–retest reliabilities in general population samples (.91 for 1-day, .90 for 1-week, .83 for 1-month, and .75 for 3-month intervals; Milner, 1986). Internal consistency for the CAP abuse scale for the present sample was .95. Numerous studies report construct validity data for the CAP abuse scale (see Milner, 1986, 1994, 2004). For example, CAP abuse scores are significantly associated with measures of aggression in parents (Crouch, Irwin, et al., 2012; Rodriguez, 2010). Classification rates based on discriminant analysis of child physical abusers and matched comparison parents are in the mid-80% to low-90% range (Milner, 1986, 1994). Studies examining the CAP abuse scale’s specificity indicate 100% correct classification of nurturing foster parents, low-risk mothers, and nurturing mothers. Prospective research revealed a significant association between CAP abuse scores and subsequent CPA (Chaffin & Valle, 2003; Milner, Gold, Ayoub, & Jacewitz, 1984).
Heart rate and RSA
Electrocardiographic (ECG) activity was recorded using two Ag-AgCl electrodes (one placed over the right collar bone and the other over the lower left rib) and a ground electrode placed over the lower right rib. Data were acquired via Mindware Technology’s ambulatory ECG MW5000A and sampled at a rate of 500 Hz. The ECG signal was transmitted via wireless signals through Mindware Technology’s BioNex 50-3711-02 four slot mainframe to a Dell Precision T2500 personal computer (Intel® Xeon®, 2.8 GHz, 6.00 GB RAM) running Mindware Technology’s BioLab 3.0.10 software (Gahanna, OH). We inspected the ECG signals using Mindware Technology’s HRV 3.0.21 software. More specifically, successive R spikes (identified by an automatic beat detection algorithm) were visually inspected and edited for irregularities. Successive interbeat intervals (in ms) were written to text files, and the text files were analyzed using the Mindware HRV module, which generates both the time domain and frequency domain HRV indices. RSA estimates were computed using a Fast Fourier Transform (FFT) to derive the spectral distribution (Mindware RSA Module, Gahanna, OH). RSA was quantified as the natural logarithm of the integral power within the respiration frequency band (0.12-0.40 Hz). Resting levels of RSA have been shown to be stable over time, although stress-invoked levels of RSA are less stable (Berntson, Quigley, & Lozano, 2007; Li et al., 2009).
Respiration rate
Respiration rate was monitored by a thoracic band, and the respiration signals were wirelessly transmitted as described above. The respiration signal was processed by FFT and examined to ensure that the respiratory frequencies were within the designated respiratory frequency band. Data from participants whose respiratory frequencies were outside the designated frequency band were removed from subsequent analyses (Berntson et al., 1997).
Positive Affect and Negative Affect Scale (PANAS)
The PANAS (Watson, Clark, & Tellegen, 1988) consists of 20 items developed to assess positive/negative affective states. Respondents were asked to think about how they were feeling at this moment and to respond to each of the PANAS items using a 5-point scale ranging from 1 (very slightly or not at all) to 5 (extremely). We assessed ratings of positive/negative affect before and after the anagram task.
Anagram task
Participants completed a computerized task in which they had 3 min to solve as many anagrams as possible. Participants were randomly assigned to one of two versions of the anagram task (i.e., easy or difficult). In the difficult anagram condition, we presented participants with five-letter anagrams that have been shown to have a high degree of difficulty with respect to forming words (Gilhooly, 1978). Variations of this task have been shown to reliably induce negative mood (e.g., MacLeod, Rutherford, Campbell, Ebsworthy, & Holker, 2002). In the easy anagram condition, we presented participants with three- or four-letter anagrams of high-frequency words (Fry, Kress, & Fountoukidis, 2000). Prior to the start of the anagram task, we informed participants in both anagram conditions that most people solve six anagrams during the 3-min time limit. Participants were told that performance on this task was a reliable indicator of intelligence. This information was expected to serve as negative feedback in the difficult anagram condition (in which participants were expected to solve fewer than six anagrams) and as positive feedback in the easy anagram condition (in which participants were expected to solve more than six anagrams).
Procedure
The institutional review board at the first author’s institution reviewed and approved the following procedures. To recruit parents for the study, we distributed informational flyers through businesses and agencies (e.g., day cares, churches, social service agencies) in the communities surrounding a Midwestern university. To ensure that an adequate number of high-risk participants were recruited, we distributed flyers to agencies and programs that served families with risk factors for abuse (e.g., voluntary home visiting programs, shelter services). The informational flyers stated that parents must have at least one child younger than 18 years of age living in their home to be eligible. Participants were told that the study would take approximately 90 min and that they would receive US$30.
After providing written consent, three electrodes were placed (one over the right collar bone and one over each of the lower ribs) and the respiration belt was placed around the participant just below the sternum. Once ECG and respiration signals were registered, participants sat quietly for 3 min while their baseline heart rates/respiration rates were recorded. Upon completion of the baseline period, participants completed the demographic questionnaire and the PANAS (i.e., to assess baseline negative affect). Participants then completed one of the two versions of the anagram task (i.e., easy or difficult). To assess the impact of the anagram task on negative affect, participants completed the PANAS for a second time (i.e., to assess postanagram task negative affect). Participants then completed other study procedures and tasks (as reported in Hiraoka et al., 2014). Finally, participants completed the CAP Inventory. Upon completion of these procedures, each parent was thanked, debriefed, and given US$30 for his or her participation.
Results
Of the 48 parents included in the planned analyses, 24 were classified as low CPA risk and 24 were classified as high CPA risk. Twenty-five parents were randomly assigned to the difficult anagram condition (13 low risk and 12 high risk) and 23 parents were assigned to the easy anagram condition (11 low risk and 12 high risk).
Anagram Condition Manipulation Check
As expected, parents assigned to the difficult anagram condition completed significantly fewer anagrams compared with parents in the easy anagram condition, F(1, 44) = 45.60, p < .001,
Demographic Analyses
We conducted a series of ANOVAs and chi-square analyses to examine the demographic characteristics of the CPA risk groups/anagram conditions. CPA risk groups did not differ significantly (ps > .05) with respect to age, gender, educational attainment, or marital status (coded married/cohabitating or single/separated/divorced). CPA risk groups differed with respect to number of children, racial composition (coded White/Caucasian or Black/African American), and annual household income. Specifically, high-risk parents, compared with low-risk parents, reported marginally more children, F(1, 43) = 3.75, p = .059,
To determine whether demographic factors were significantly associated with the dependent variables (i.e., heart rate/RSA at baseline/during the anagram task), we conducted four regression analyses. In each regression, we simultaneously entered each of the demographic factors (age, gender, race [coded Caucasian/African American], educational attainment, marital status [coded married/cohabitating or single/separated/divorced], and number of children) as predictors of heart rate/RSA at baseline/during the anagram task. Results revealed that only age and gender were independently associated with baseline RSA (age β = –.46; gender β = .25), as well as RSA during the anagram task (age β = –.56; gender β = .25). To explore the potential influence of age and gender on our results, we conducted the planned analyses with and without age and gender as covariates. The pattern of results was unchanged by the inclusion of the covariates; therefore, the results reported below describe the analyses without covariates.
Heart Rate
Heart rate data were analyzed using a 2 (CPA risk: low, high) × 2 (Anagram task: easy, difficult) × 2 (Time: baseline, anagram task) ANOVA, with repeated measures on the last factor. Results revealed that none of the effects involving the anagram condition were significant (ps > .10). As expected, the CPA risk group by time interaction was significant, F(1, 44) = 6.40, p = .015,
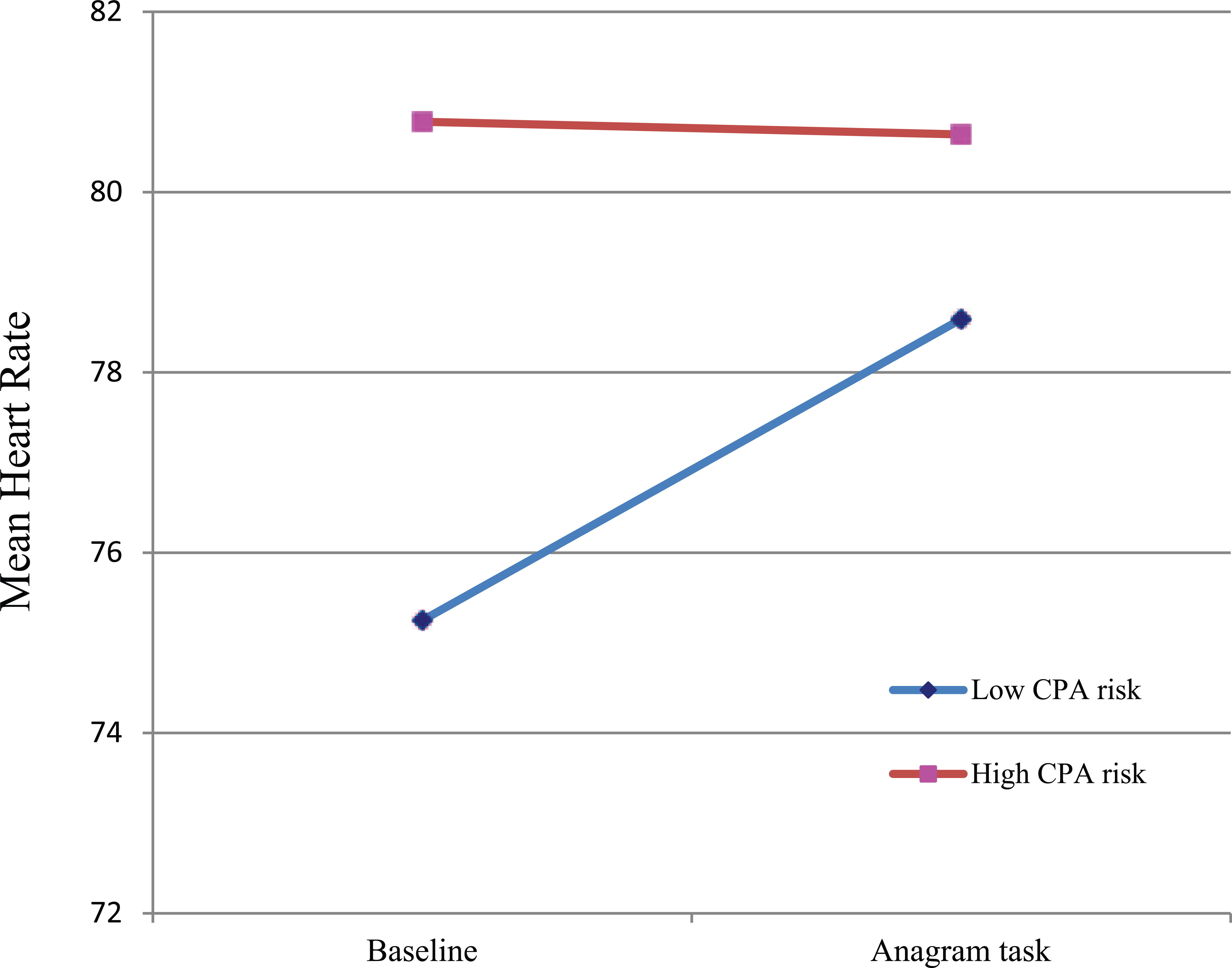
Mean heart rate for low/high CPA risk parents at baseline and during the anagram task.
RSA
RSA data were analyzed using a 2 (CPA risk: low, high) × 2 (Anagram task: easy, difficult) × 2 (Time: baseline, anagram task) ANOVA, with repeated measures on the last factor. Results revealed that none of the effects involving the anagram condition were significant (ps > .05). As expected, the CPA risk group by time interaction was significant, F(1, 44) = 6.06, p = .018,
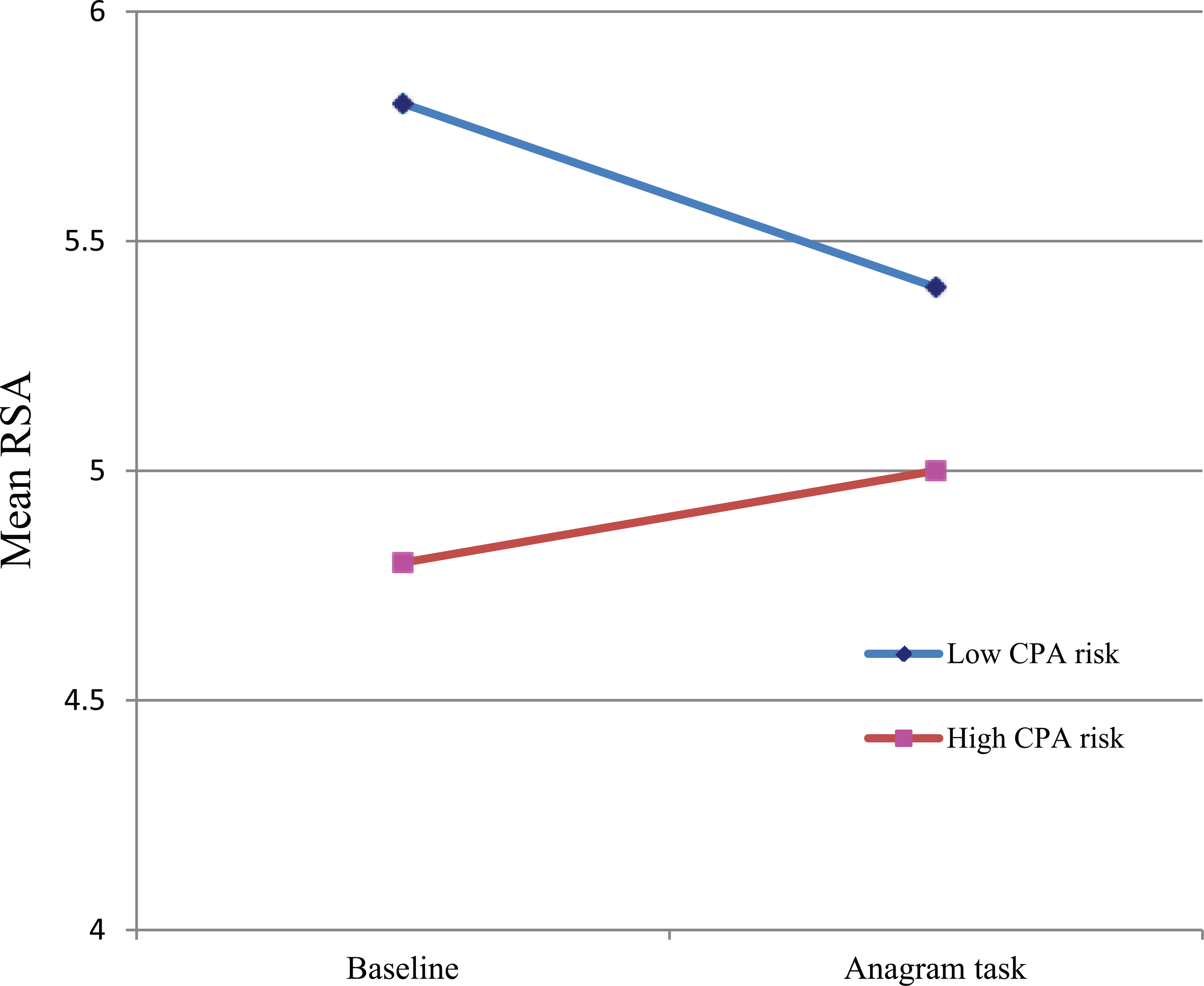
Mean RSA for low/high CPA risk parents at baseline and during the anagram task.
Discussion
Collectively, findings from the present study support the notion that high-risk parents experience elevated physiological arousal regardless of the demands of their immediate environment. As expected and consistent with the chronic arousal hypothesis, high-risk (compared with low-risk) parents demonstrated higher levels of resting heart rate and lower levels of resting RSA and they did not exhibit significant changes (relative to baseline) in heart rate or RSA during the anagram task. In keeping with prior research (e.g., Disbrow et al., 1977; Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013; Pruitt & Erickson, 1985), low-risk parents in the present study evinced more physiological flexibility, allowing them to more effectively modulate their heart rate and RSA in response to environmental demands.
Prior research suggests that the lower levels of resting RSA observed among high-risk parents may be linked to difficulties with emotion regulation and affect instability (for a review, see Appelhans & Luecken, 2006). Koval and colleagues (2013) found that individuals with lower levels of resting RSA tend to experience more affect instability in their daily lives (i.e., more extreme fluctuations of positive and negative affect during routine activities). Prior research suggests that negative affective states are often precursors to harsh/coercive parenting behaviors (e.g., Ateah & Durrant, 2005; Holden, Coleman, & Schmidt, 1995). For example, Ateah and Durrant (2005) surveyed a sample of mothers regarding their use of physical punishment in the past 2 weeks and found that maternal anger was a significant predictor of use of physical discipline (even after controlling for parental belief in the value of corporal punishment and perceptions of the seriousness/intent of the child’s misbehavior). The role of RSA in affective and behavioral regulation as it relates to risk for CPA warrants additional investigation.
It is also noteworthy that lower levels of baseline RSA (such as that evinced by high-risk parents in the present study) are associated with lower levels of cognitive executive functioning (Hansen, Johnsen, & Thayer, 2003; see also the Model of Neurovisceral Integration, Thayer, 2007; Thayer, Hansen, Saus-Rose, & Johnsen, 2009; Thayer & Lane, 2000; and the Polyvagal Theory, Porges, 2007, 2009, 2011). Executive functions allow an individual to engage in goal pursuit and exert “top down” influences on attention, behavior, and emotion. Moreover, executive functions serve to inhibit prepotent behavioral and emotional responses that are either not relevant to current goals or may be counterproductive (e.g., responses that may contribute to increased negativity in response to parenting challenges; Deater-Deckard, Sewell, Petrill, & Thompson, 2010). Research examining executive functions among parents at risk for CPA suggests that high-risk parents exhibit less inhibitory control (as indicated by higher interference scores on the Stroop task; Nayak & Milner, 1998) and lower levels of self-reported attentional control (Crouch, Shelton, et al., 2012).
The present results are consistent with findings reported by Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al. (2013), in that low-risk parents (compared with maltreating/at-risk parents) exhibited higher baseline RSA and evinced significant RSA withdrawal (i.e., reductions in RSA relative to baseline) in response to a challenging task (e.g., anagram task). Although baseline differences in RSA have not always been observed when comparing maltreating parents and nonmaltreating parents (e.g., Reijman et al., 2014; Skowron et al., 2013), the present study adds to accumulating evidence that high-risk/maltreating parents do not exhibit significant RSA withdrawal in response to stressors/cognitive challenges (e.g., Joosen, Mesman, Bakermans-Kranenburg, Pieper, et al., 2013; Reijman et al., 2014; Skowron et al., 2013).
Although most studies examining physiological functioning in high-risk/maltreating parents focused on child-related stimuli (e.g., infant cry sounds, video recordings of parent–child interactions), the present findings support the notion that high-risk/maltreating parents may differ from low-risk/nonmaltreating parents in how they respond to nonchild-related stressors and challenges (Casanova et al., 1992). However, the pattern of findings obtained in the present study differs somewhat from that reported by Casanova and colleagues. For example, Casanova et al. included an unsolvable anagram condition and reported that heart rate increased significantly during the anagram task, but this effect was not moderated by CPA risk status. In the present study, heart rate increased significantly among low-risk parents (but not high-risk parents) during the anagram task. Differences in the pattern of results obtained in the present study (compared with the Casanova et al. study) could be due to the fact that the unsolvable anagram task used in the Casanova et al. study may have been experienced as more difficult and/or more frustrating than the solvable anagrams used in the present study. However, it is noteworthy that the level of difficulty of the anagram task used in the present study (i.e., easy vs. difficult) did not appear to affect physiological functioning. It also is possible that limited statistical power in the Casanova et al. study may have precluded detection of differential heart rate changes among the high-risk parents (n = 15) and low-risk parents (n = 15) during the unsolvable anagram task.
Moreover, it should be noted that the use of the solvable anagram task in the present study differs from the types of stimuli used in prior studies examining physiological functioning in high-risk parents and low-risk parents. Specifically, prior studies have attempted to expose parents to stimuli intended to be aversive (e.g., the cold pressor task and watching videos of industrial accidents, Casanova et al., 1992; watching videos of negative interpersonal interactions, Disbrow et al., 1977; listening to infant cry sounds, Crowe & Zeskind, 1992). In contrast, the solvable anagram task used in the present study represented a cognitive challenge that was not expected to be especially aversive, thus mimicking the types of cognitive problem-solving challenges that parents negotiate on a daily basis (e.g., deciding what to do when a child seems uncomfortable, stretching a limited budget to meet household needs).
The present findings suggest that low-risk parents experience less physiological arousal as they approach everyday problem-solving tasks and display an increase in arousal (and withdrawal of RSA) as they engage in solving problems. In contrast, high-risk parents may approach routine problem-solving tasks with initially high levels of physiological arousal (and low levels of RSA) and exhibit little physiological adjustment as they engage in problem solving. As a result, high-risk parents may more quickly experience depletion of problem-solving resources and may experience greater fatigue and frustration in response to day-to-day challenges. It also is interesting to speculate whether the chronic levels of arousal in high-risk parents are linked to their greater propensity to perceive events as threatening (e.g., attribute more hostile intent in challenging situations), which in turn may lead the parents to remain physiologically prepared to respond to threats to their well-being (i.e., maintain heightened levels of arousal).
Limitations
A number of limitations warrant consideration when interpreting the findings from the present study. It should be noted that this study focused on CPA potential and, thus, does not inform questions about physiological functioning in parents at risk for other forms of child maltreatment (e.g., neglect, sexual abuse). Although the present study revealed CPA risk group difference in baseline heart rate and baseline HRV, it does not inform us as to why high CPA risk parents differ from low CPA risk parents on these physiological variables. A number of factors (e.g., genetic predispositions, poor overall physical health, comorbid psychological conditions, and prior trauma/maltreatment) may explain the development of chronic levels of physiological arousal and/or diminished physiological flexibility in response to environmental demands. Additional research is needed to explore the etiological underpinnings of CPA risk group differences in resting heart rate and HRV.
As noted earlier, methodological differences may explain variable findings across studies. To better understand these mixed findings, a meta-analysis of the literature examining autonomic functioning in maltreating/at-risk parents may be useful. Specifically, a meta-analysis would allow for a systematic comparison of effect sizes across studies and as well as an examination of whether study characteristics (e.g., parents vs. nonparents, maltreating vs. at risk, child-related vs. nonchild-related stressor) moderate patterns of results across studies.
Although the present study possessed adequate power to detect the hypothesized CPA risk group × Time interaction effects, it lacked power to detect small-medium 3-way (i.e., CPA risk × Anagram task difficulty × Time) interaction effects. Indeed, a small CPA risk × Anagram task difficulty × Time interaction effect for heart rate was observed (
It also should be noted that CPA perpetration was not directly assessed in the present study; therefore, caution should be used when attempting to generalize the findings from this study to abusive parents. As noted in the introduction, studies examining RSA in maltreating parents and nonmaltreating parents have failed to find differences in baseline heart rate/RSA (e.g., Reijman et al., 2014; Skowron et al., 2013); however, methodological differences (e.g., nature of the comparison groups, baseline assessment procedures) may explain the variability in outcomes across studies. Replication of the present study in a sample of maltreating parents (utilizing a resting baseline and a low-risk comparison group) is needed.
Another intriguing question to be addressed in future research is whether there are subtypes of high-risk/maltreating parents that differ in their physiological responses to stressors. Gottman and colleagues (1995) examined heart rate reactivity in male batterers and found that the majority of batterers (approximately 80%) exhibited an increase in heart rate (from baseline to the first 5 min of a conflictual interaction with their partners); however, approximately 20% of batterers exhibited a decrease in heart rate over the same time period. Examination of the psychosocial characteristics of the batterers who exhibited decreases in heart rate revealed that they possessed more antisocial traits and were more generally violent toward others. Additional research is needed to explore the extent to which at-risk and maltreating parents are heterogeneous with respect to their physiological responses to stressors.
Clinical Implications
Information imparted during parent education/parent skills training programs (e.g., “never shake a baby,” “take a break,” or “call someone for help”) may be difficult for high CPA risk parents to implement to the extent that they experience chronic levels of physiological arousal, which in turn may be associated with reduced cognitive executive functioning. Indeed, as has been previously suggested (Acton & During, 1992), high-risk parents may benefit from interventions that include components that focus on reducing physiological arousal and increasing the capacity to regulate arousal efficiently and effectively. Emerging literature on mindfulness-based interventions (e.g., Kabat-Zinn, 1990; Khoury et al., 2014; Nyklicek, Mommersteeg, Van Beugen, Ramakers, & Van Boxtel, 2013) suggests that mindfulness practice is associated with reductions in negative affective states as well as improvements in HRV. For example, Ditto, Eclache, and Goldman (2006) reported that mindfulness-based stress reduction techniques (e.g., body scan exercises) were associated with increased HRV in healthy young adults. Moreover, Heeren, Van Broeck, and Philippot (2009) found that mindfulness practices are associated with improved cognitive flexibility and increased capacity to inhibit prepotent cognitive responses.
Although several studies indicate that mindfulness-based interventions are associated with reductions in negative affective states in high-risk parents (Duncan & Bardacke, 2010; Perez-Blasco, Viguer, & Rodrigo, 2013; Vieten & Astin, 2008); no study to date has examined the impact of mindfulness-based interventions on heart rate/HRV in high-risk parents. Additional research is needed to examine whether improvements associated with mindfulness skills training are (at least in part) the result of improved physiological functioning (e.g., lower resting heart rate and higher resting RSA) in high-risk parents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.