
Abstract
Homicide-suicide represents one of the rarest forms of lethal violence but often precipitates calls to revise social, health, and justice policies. However, there is little empirical information about this type of violence. The current study uses two unique data sets to examine a wide range of individual and situational characteristics of homicide-suicide, with particular emphasis on establishing whether and how homicide-suicide differs from homicide-only and suicide-only. Findings suggest homicide-suicide may have unique characteristics that set it apart from both homicide-only and suicide-only, as well as sharing certain other characteristics with those two types of events.
Homicide-suicide (whereby an individual takes the life of at least one other person, followed by their own life shortly after) represents one of the rarest forms of lethal violence. Despite their rarity, homicide-suicide events can have far-reaching and long-lasting impacts on individuals, families, and communities. Such events often receive significant public and media attention, which in turn can drive changes to social, health, and justice policies, particularly in the areas of family justice (e.g., child custody arrangements and/or responses to family violence) and mental health. However, there is limited empirical information about this specific type of violence, which raises the possibility that policies implemented in reaction to homicide-suicide events may be improperly designed, poorly targeted, and based on guesswork and speculation rather than evidence.
While representing a small and variable proportion of all homicides or all suicides, it appears that homicide-suicide occurs at similar rates across different countries, irrespective of variations in those countries’ homicide-only or suicide-only rates over time (e.g., Large, Smith, & Nielssen, 2009; Liem, Barber, Markwalder, Killias, & Nieuwbeerta, 2011). Homicide-suicide events seemingly share many common features across different countries, including perpetrator age and sex (commonly older males; for example, Bossarte, Simon, & Barker, 2006; Comstock et al., 2005; Galta, Olsen, & Wik, 2010), perpetrator–victim(s) relationship (frequently intimate partners; for example, Easteal, 1994; Yip, Wong, Cheung, Chan, & Beh, 2009), offender ethnicity (generally Caucasian; for example, Belfrage & Rying, 2004; Rosenbaum, 1990), weapon use (typically a firearm; for example, Carcach & Grabosky, 1998; Roma, Pazzelli, et al., 2012), and location of the homicide component of the incident (usually a private location, such as a residence; for example, Sillito & Salari, 2011). However, emerging studies suggest greater regional and cultural variation in homicide-suicide characteristics than previously recognized (Bell & McBride, 2010; Roberts, Wassenaar, Canetto, & Pillay, 2010; Yip et al., 2009), underscoring the importance of a region-specific approach to studying homicide-suicide, rather than extrapolating findings from one country to another.
Theoretical Context
Theoretical frameworks proposed to apply to homicide-suicide include attribution theories (Starzomski & Nussbaum, 2000), masculinity theories (Gregory, 2012), strain theories (Harper & Voigt, 2007), social integration theories (stemming largely from Durkheim, 1897/1966), psycho-dynamic theories (Palermo, 1994), and stream analogy theories (Stack, 1997; Unnithan, Huff-Corzine, Corzine, & Whitt, 1994). 1 These theories accord with typology-based explanatory frameworks for homicide-suicide, which incorporate factors such as mental illness, motivational state (e.g., jealousy, frustration), and relational distance between offender and victim(s) (e.g., Harper & Voigt, 2007; Liem & Nieuwbeerta, 2010; Marzuk, Tardiff, & Hirsch, 1992; Palermo, 1994). A common characteristic across these frameworks is that they typically view homicide-suicide from either a suicidology perspective (viewing the event as primarily explainable through suicidological concepts, and attempting to adapt those theories to take into account the homicide event), or from a criminological perspective (conceptualizing the event as primarily explainable through theories of homicide, and attempting to apply those theories to the suicide component). In an applied setting, this dichotomy is mirrored by the common practice of government agencies to treat homicide and suicide as two very distinct issues, requiring different policy responses from completely separate agencies (Harper & Voigt, 2007).
This dual approach suffers from difficulties in fitting theory and evidence together satisfactorily, which has been neatly illustrated by considering how attributional/stream analogy theory has been applied to homicide-suicide (Liem, 2010; Liem & Nieuwbeerta, 2010). Those theories provide a useful framework for understanding whether violence will be directed outwardly (to others) or inwardly (to the self), but are unable to satisfactorily account for situations where both outward and inwardly directed aggression occur (Liem, 2010). In situations where both outwardly and inwardly directed “streams” of aggression occur, theoretical frameworks that seek to conceptualize homicide-suicide have typically resorted to explaining homicide-suicide as being “more like” one particular “stream” than the other “stream,” based on empirical observations about whether homicide-suicide perpetrators have “more in common” with suicide completers or homicide perpetrators. As discussed in the following sections, however, there are shortcomings in empirical studies against which theories of homicide-suicide have been contextualized.
Literature Overview
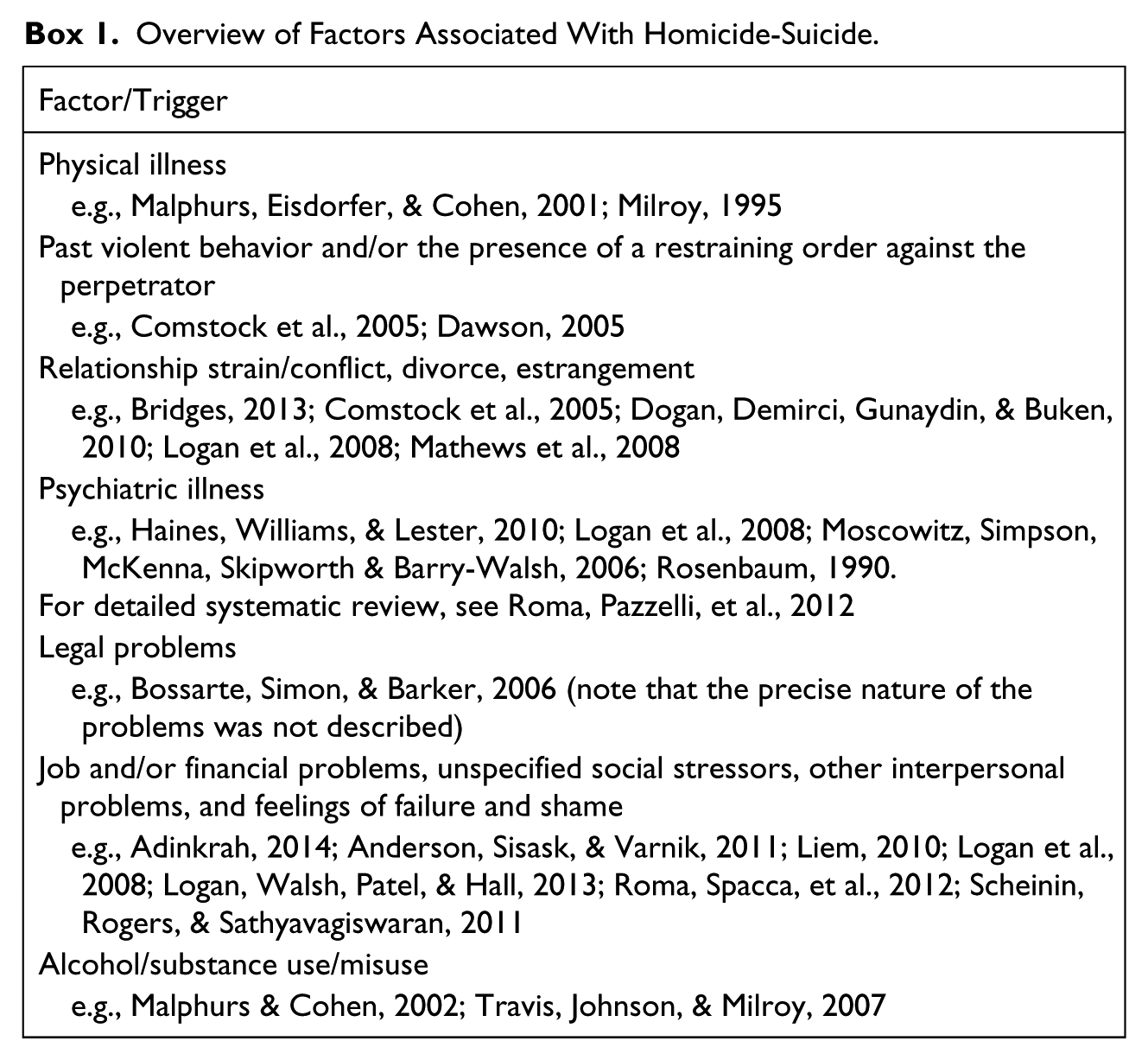
Many studies take an epidemiological or descriptive approach focusing on demographic/relational factors, but some consider a broader range of individual/situational factors or “triggers” for homicide-suicide (a non-exhaustive overview is given in Box 1). To date, little research provides insight into whether there are “unique” risk factors for homicide-suicide. A particular knowledge limitation is that many factors implicated in homicide-suicide are also well documented in relation to homicide-only or suicide-only incidents. Relationship breakdown and alcohol use, for example, are recognized as triggers for both homicide-only and suicide-only (e.g., Bagge, Littlefield, Conner, Schumacher, & Lee, 2014; Batterham et al., 2014; Dobash, Dobash, Cavanagh, & Lewis, 2004; Eriksson & Mazerolle, 2013; Ide, Wyder, Kolves, & De Leo, 2010; Kuhns, Exum, Clodfelter, & Bottia, 2014; Ooi, Foong, & Casey, 2006; Zaridze et al., 2014), whereas mental illness is a significant risk factor for suicide-only (see Baxter, Charlson, Somerville, & Whiteford, 2011).
Overview of Factors Associated With Homicide-Suicide.
Comparative Studies
There is no consensus within literature on whether homicide-suicide has certain characteristics of both homicide-only and suicide-only that may combine in a unique way, or whether homicide-suicide shares characteristics with homicide-only and suicide-only and also has its own distinct features (Eliason, 2009; Panczak et al., 2013). It is unclear whether homicide-suicide perpetrators have more characteristics in common with suicide completers, or homicide perpetrators (e.g., Buteau, LeSage, & Kiely, 1993; Cooper & Eaves, 1996; Palmer & Humphrey, 1980; Rosenbaum, 1990). Studies attempting to answer these questions have typically compared homicide-suicide with either homicide-only or suicide-only, not both (e.g., Banks, Crandall, Sklar, & Bauer, 2008; Bridges & Tankersley, 2010; Haines, Williams, & Lester, 2010; Liem & Roberts, 2009; Lund & Smordinsky, 2001).
Relative to homicide-only perpetrators, there is evidence that homicide-suicide perpetrators are likely to be older (Banks et al., 2008; Lund & Smordinsky, 2001; Rosenbaum, 1990; Stack, 1997), married or separated (see Panczak et al., 2013), and to have had a depressive disorder and history of making suicidal threats (Liem & Roberts, 2009). Homicide-suicide appears less likely than homicide-only to involve an unemployed perpetrator (Liem & Roberts, 2009), or the influence of alcohol (although findings vary—see Panczak et al., 2013, for a systematic review and meta-analysis of accumulated findings). There are mixed findings about domestic violence history; for example, Bourget, Gagne, and Moamai (2000) found markedly higher occurrence of domestic violence among intimate partner homicide-only cases relative to intimate partner homicide-suicide cases, whereas Koziol-McLain et al. (2006; who also focused on intimate partner violence) found comparable levels of historic violence. Using meta-analysis, Panczak et al. (2013) found that, overall, a history of domestic violence appeared less common among homicide-suicide perpetrators relative to homicide-only perpetrators. This contradicts common assumptions about partner violence and homicide-suicide. However, it must also be noted that there is considerable heterogeneity among studies that compare homicide-suicide with homicide-only (Panczak et al., 2013).
In comparison with suicide-only cases (based on a smaller number of studies than comparisons with homicide-only), homicide-suicide perpetrators appear to be around the same age (Flynn et al., 2009; Malphurs, Eisdorfer, & Cohen, 2001), but other findings are mixed. Whereas Malphurs and Cohen (2005) and Malphurs et al. (2001) observed lower likelihoods of past suicidal ideation among older male homicide-suicide perpetrators, Haines et al. (2010) did not find significant differences in a general sample of male homicide-suicide perpetrators relative to suicide-only cases. Homicide-suicide cases may more commonly involve past histories of domestic violence or family discord, relative to suicide-only cases (Logan et al., 2008; Malphurs & Cohen, 2005; Malphurs et al., 2001), but this has not been well established in a general sample. Findings on alcohol use vary, as do findings for a past suicide attempt (Panczak et al., 2013).
It is probable that inconsistency in extant studies arises from the characteristically small samples examined. Also, along with different methodological approaches, data sources, and samples selected, the restricted comparison groups used may partially explain inconsistencies in findings about similarities and differences between homicide-suicides and other types of intentional deaths. This limitation can be redressed by comparing homicide-suicide with both homicide-only and suicide-only, which—at the time of writing—only limited studies have attempted (e.g., Liem et al., 2011; Liem & Nieuwbeerta, 2010; Logan et al., 2008; Saleva, Putkonen, Kiviruusu, & Lonnqvist, 2007). These comparative studies represent a methodological step forward in understanding homicide-suicide, but were able to examine only a small number of variables (age, sex, race, ethnicity, methods/weapons) and do not consider psychiatric history and life circumstances.
Study Objectives
To develop the international evidence base and enhance the ability of policymakers to develop tailored responses to lethal violence, further research into homicide-suicide is needed in regions where little evidence has been collected to date. Given the lack of studies comparing homicide-suicide with both homicide-only and suicide-only, factors which may differentiate between homicide-suicide and those other two categories of intentional deaths have not been well identified. The current study builds the evidence base upon which policy and intervention strategies can be developed, by comparing homicide-suicide with homicide-only and suicide-only events on a range of demographic, psychiatric history, stressful life events, and alcohol and drug variables, and considering whether and how homicide-suicide differs from homicide-only and suicide-only.
Method
Data Sources and Definitions
Two separate data sources were used. Data on homicide-only cases were drawn from the Australian Homicide Project (AHP) data set (see Eriksson, Mazerolle, Wortley, & Johnson, 2014), which involved structured face-to-face interviews with 302 men and women convicted of murder or manslaughter, from correctional facilities across all Australian states and territories. Interviews were based on established scales with sound psychometric properties. Measurement areas include demographic factors, alcohol and drug use experiences, violence perpetration, and victimization in prior relationships including family of origin, situational factors, experiences with the criminal justice system, and social welfare agencies. Life events in the 12 months prior to the homicide event were recorded using a life event calendar (see Roberts & Horney, 2010, for a detailed description of this methodology). Information on suicide-only and homicide-suicide cases was drawn from the Queensland Suicide Register (QSR) data set. The QSR contains detailed information about Queensland suicide cases from 1990 onwards (see De Leo & Sveticic, 2012, for details). Information in the QSR is drawn from post-mortem, coroners, police, and psychological autopsy reports, and includes a wide range of demographic, medical, and psychiatric information regarding the deceased.
Following earlier studies, homicide-suicides were defined as an incident involving one or more homicides followed by the suicide of the suspected perpetrator. Existing research often incorporates a time span between the homicide and suicide events, generally ranging between 24 hr (e.g., Bossarte et al., 2006; Logan et al., 2008) and several days (e.g., Comstock et al., 2005). Initial examination of QSR cases showed that most suicides that followed a homicide event occurred within 24 hr of the homicide event. In one instance, the time between the homicide and suicide could not be established; however, autopsy findings were highly suggestive that the suicide event occurred within a few days of the homicide event.
Sample Refinement and Creation of Different ‘Type of Death’ Categories
QSR data indicated most homicide-suicide cases (88%) involved males aged 18 years and above as the alleged perpetrator. To increase the comparability of cases considered, and given the small number of female homicide-suicide perpetrators (n = 8), the suicide-only and homicide-only cases included in the current study were restricted to those where the deceased/perpetrator was a male aged 18 years and above. 2 The QSR classifies suicides as “possible,” “probable,” and “beyond reasonable doubt (BRD),” depending on the apparent degree of intent of the deceased person to end their own life. For the current study, only those suicides considered “probable” or “BRD” were included; all homicide-suicide cases fell within those two categories. The final sample under study consisted of three categories of deaths: the homicide-suicide group (60 males), the homicide-only group (251 males from an initial total of 260 males; nine were excluded due to being below 18 years of age), and the suicide-only group (8,014 males from an initial total of 8,251 males; 237 were removed due to being below 18 years of age).
Variables
Demographic
An individual’s age at the time of the incident, employment status (employed, unemployed, or not in the labor force; examples of the latter include students, retirees, homemakers, and pensioners), and marital status (married/de facto, divorced/separated, single/never married, or widowed) at the time of the incident were examined. Aboriginal and/or Torres Strait Islander status was coded dichotomously. Non-English speaking background (NESB) was also coded into a dichotomous variable.
Psychiatric history, life stressors, alcohol, and drugs
Two psychiatric history indicators were examined: whether the focus individual had been in contact with a mental health professional in the 3 months prior to the incident, and whether that person had a history of suicide attempts in the year leading up to the incident. The presence of various life stressors around the time of the incident was examined. The stressors were the presence of a domestic violence order (DVO), 3 financial problems, a child custody dispute, and a recent or pending relationship separation. It should be noted that within the QSR data a response of “no” on a life stressor does not necessarily indicate that the stressor was not present. It may denote that the stressor was not explicitly recorded, or that there was no information available. The study also considered whether the focal individual had alcohol problems, and whether they had used alcohol or illicit drugs immediately before the incident.
Comparability of the Data Sets
The AHP and QSR data sets were designed independently of one another, for different purposes, using different data collection methods and information sources. In the AHP, self-reported information is provided during an in-depth interview with living persons convicted of murder or manslaughter, a methodology that may introduce bias due to exaggeration or concealment of behavior. In the QSR, data come from reports provided by third parties, and are therefore limited to the information reported and recorded on file. In addition to possible differences in data reliability due to the two different collection methods, the completeness and level of detail of available data varies between data sets. Not all variables could be directly compared, as there were differences between data sets in how certain information was operationalized. Although some indicators (e.g., age, employment status, marital status) could be easily compared, variables such as drug and alcohol use, in particular, required additional manipulation to create derived variables. Table 1 shows key differences in data set wording, and gives information about how derived variables were created.
Summary of Comparability Between the Australian Homicide Project and Queensland Suicide Register on Relevant Variables.
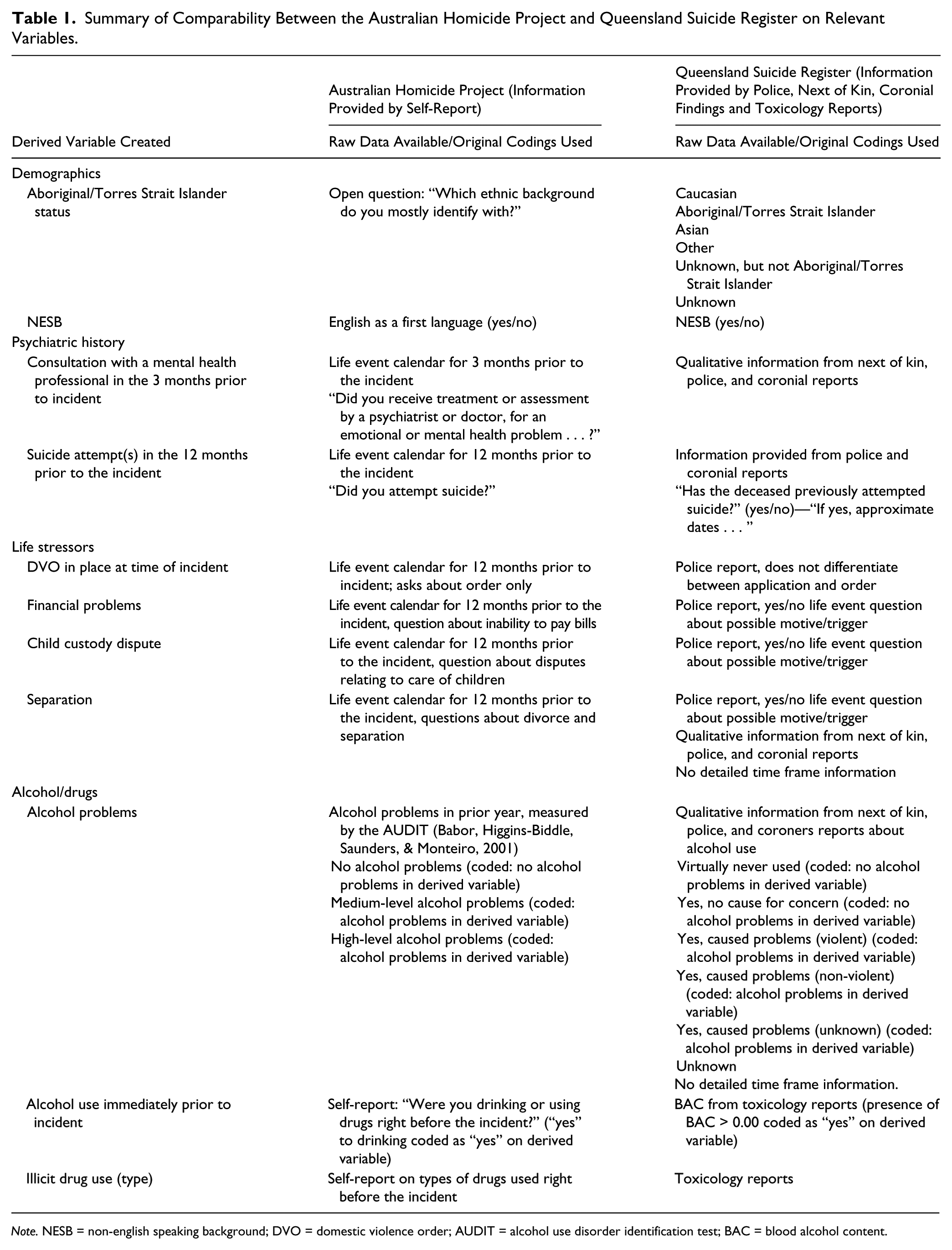
Note. NESB = non-english speaking background; DVO = domestic violence order; AUDIT = alcohol use disorder identification test; BAC = blood alcohol content.
Analysis
Analyses consisted of chi-square and ANOVA tests, with follow-up pairwise comparisons (t tests) and Bonferroni corrections (e.g., Benjamini & Hochberg, 1995) applied as necessary. With regard to chi-square tests, following McDonald (2014), analyses were conducted only in instances where there were five or more cases per cell.
Results
Demographics and Incident Site
The homicide-only group was significantly younger on average (M = 31.0 ± 10.1 years) than either the suicide-only (M = 42.3 ± 17.3 years) or homicide-suicide groups (M = 47.3 ± 16.6 years); the latter two groups did not differ from one another (F = 56.3, p < .01). As per Table 2, homicide-suicides were more likely than homicide-only or suicide-only events to occur in residential settings, and homicide-suicide perpetrators were more likely to be in a marital-type relationship.
Demographic Comparisons Between Groups.

Note. Each superscript letter (a, b, and c) indicates a subset of group categories whose proportions do not differ from one another at the .05 significance level. Percentages shown are calculated on the basis of number of cases where information was available, rather than the total number of cases. Percentages may not sum to 100 due to rounding error. NESB = non-English speaking background.
Includes three incidents in institutions (e.g., prison, hospital) among the homicide-only group, and 153 incidents in institutions among the suicide-only group.
Results are presented primarily for illustrative purposes and contain too few values to enable reliable analysis of between-group differences. Due interpretive caution should be applied in these instances.
In other respects, such as employment status, the characteristics of homicide-suicide were shared with the suicide-only group, and both groups differed from homicide-only. For example, the homicide-suicide and suicide-only groups included a higher percentage of cases where the perpetrator/decedent was out of the labor force, relative to the homicide-only group. The homicide-suicide group had a noticeably high proportion of cases in that category (although not at the level of statistical significance when compared with suicide-only). Given the “not in the labor force” group includes categories such as retirees, this observation relates strongly to the relative mean age of each group. 4
In some instances, homicide-suicide resembled both other groups. For instance, the percentage of persons in the homicide-suicide group who were divorced or separated sits between the homicide-only and suicide-only groups. On other variables, the lack of any significant differences between homicide-suicide and the two other groups is likely to be a result of the relatively small sample size, also exacerbated by missing data. This applies, for example, to NESB and Aboriginal and Torres Strait Islander status. Table 2 shows more detailed information.
Psychiatric History
In cases where the information was available, comparable proportions of people in the suicide-only and homicide-suicide groups had contact with a mental health professional in the three months before their death. The homicide-only and suicide-only groups differed in terms of past suicide attempts in the year before the incident, whereas homicide-suicide cases did not differ from either of those two groups.
Life Stressors
Examination of life stressors revealed one of the few areas where the homicide-suicide group was distinct from either of the other two groups: the higher percentage of perpetrators who had in place against them, at the time of the incident, a DVO. In terms of separation from a partner, the homicide-suicide group resembled the suicide-only group. Those two groups, in turn, were less likely to have experienced a separation than the homicide-only group. Regarding financial problems and child custody disputes, homicide-only had the highest percentage of persons experiencing those events and suicide-only had the lowest. The homicide-suicide group again fell between the two other groups and did not significantly differ from either. Table 3 provides additional detail.
Psychiatric History and Life Stressors.
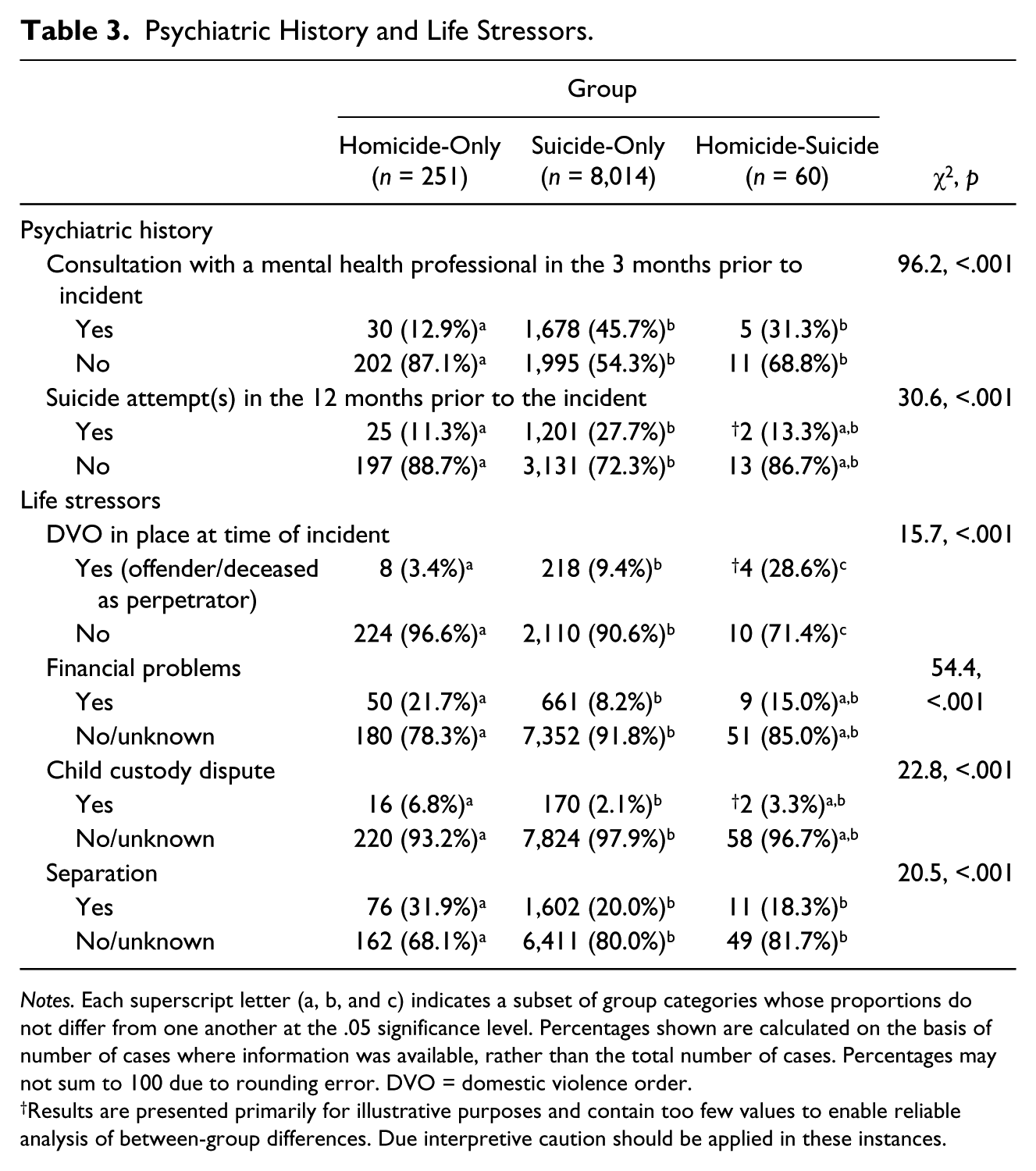
Notes. Each superscript letter (a, b, and c) indicates a subset of group categories whose proportions do not differ from one another at the .05 significance level. Percentages shown are calculated on the basis of number of cases where information was available, rather than the total number of cases. Percentages may not sum to 100 due to rounding error. DVO = domestic violence order.
Results are presented primarily for illustrative purposes and contain too few values to enable reliable analysis of between-group differences. Due interpretive caution should be applied in these instances.
Alcohol and Drug Use
Alcohol problems, alcohol use before the incident, and the use of cannabis and amphetamines were far more commonly found in the homicide-only group than in either of the other two groups, consistent with earlier literature. Again, the homicide-suicide group did not significantly differ from the suicide-only group. However, the homicide-suicide group had the lowest prevalence of alcohol, cannabis, or amphetamine use before the incident (Table 4).
Alcohol and Drug Use.

Notes. Each superscript letter (a, b, and c) indicates a subset of group categories whose proportions do not differ from one another at the .05 significance level. Percentages shown are calculated on the basis of number of cases where information was available, rather than the total number of cases. Percentages may not sum to 100 due to rounding error. BAC = blood alcohol content.
Results are presented primarily for illustrative purposes and contain too few values to enable reliable analysis of between-group differences. Due interpretive caution should be applied in these instances.
Where BAC information was available and BAC was present at levels of more than 0.05 mg/100 mL, mean BAC for homicide-suicide cases was 0.188 mg/100 mL (SD = 0.062), which did not differ significantly from the mean BAC for suicide-only cases of 0.163 mg/100 mL (SD = 0.084; t = 1.0, p = .341). The small number of homicide-suicide cases in which BAC was detected at levels of greater than 0.05 mg/100 mL should be taken into account when interpreting these results.
Results Summary
As a number of different findings have been presented above, Table 5 summarizes variables where homicide-suicide was unique, where it shared characteristics with only one other type of death, and where it did not differ from either of the two other types of death examined in the study.
Summary of Results.

Note. DVO = domestic violence order.
Caution: Small numbers.
Discussion
The current study—although preliminary in nature—shows a degree of consistency with existing work, and also provides novel observations about homicide-suicide. Compared with prior work that has examined the characteristics of homicide-suicide events, the present study is consistent in regard to the typical location of homicide-suicide events (in private), marital status of the perpetrators (in a relationship), and the presence (in some instances) of mental health issues and/or past suicidal behavior, as well as stressful life events including relationship, financial, and child custody issues. Regarding comparisons between homicide-suicide and suicide-only, and noting that variation in earlier studies makes it difficult to draw strong conclusions about comparability, the present results replicate findings on factors such as age of deceased/perpetrator, prevalence of mental health issues, and alcohol use.
The results accord to a lesser extent with earlier comparisons between homicide-suicide and homicide-only, in terms of finding an older age of homicide-suicide perpetrators, the lower use of alcohol or illicit drugs prior to the event in that group, and marginally—although not statistically significantly—higher prevalence of past suicidal behaviors among the homicide-suicide group. An unexpected finding was that homicide-suicide did not share any characteristics with homicide-only that it did not also share with suicide-only. This contrasts with the observation that homicide-suicide shared various characteristics with suicide-only, but differed from homicide-only. It may be tempting to attribute this to the fact that homicide-suicide and suicide-only cases were drawn from the same data set (and therefore, data collected were directly comparable between those groups). However, this seems an unsatisfactory explanation given the general consistency of findings between the current work and earlier studies comparing homicide-suicide with homicide-only.
Interestingly, the high prevalence of DVO presence within the homicide-suicide group at the time of the event was contrary to earlier studies, which may reflect an outcome of the present study’s use of a different indicator of domestic violence to past research. The present study looked at a formal, legal response to violence at a specific time, whereas earlier studies tend to consider domestic violence in more general terms (such as asking if any violence was ever present). Nonetheless, the general patterns of results observed, and their consistency with various prior studies, provide a level of assurance that the current study, although combining two different data sources, has produced meaningful observations about homicide-suicide in relation to both homicide-only and suicide-only.
The study suggests that homicide-suicides, although in some ways looking “more like” suicide-only than homicide-only, may best be viewed as sharing many characteristics with both homicide-only and suicide-only (even though those two groups may differ from one another in turn). This finding opens the theoretical possibility that— by sharing characteristics with both other types of sudden death events—homicide-suicide should not be interpreted from either a suicidological perspective or a criminological perspective. Rather, it may be beneficial to conceptualize homicide-suicide as an event that involves particular characteristics of both types of events, without definitively resembling either. To further explore this issue, it would be helpful to examine the question of whether, if perpetrators were not determined to kill themselves, they would have gone through with killing other people.
There was tentative support for the possibility of homicide-suicide having characteristics that set it apart from either of the other two types of event. Of these, and noting only a small number of cases had this information recorded, it appears the presence of a DVO may merit further consideration. It may also be beneficial to examine cases where DVOs were in place, to ascertain why those orders were unsuccessful in protecting the victim and whether the DVO may have acted as a catalyst for violence (Liem & Roberts, 2009).
A productive way forward in better understanding homicide-suicide may be to establish particular “typologies” of homicide-suicide perpetrators, based on how various different characteristics of a homicide-suicide event “cluster” in comparison with homicide-only and suicide-only. For example, there may be a “cluster” of homicide-suicide perpetrators who very closely resemble suicide-only cases, except for having a history of violence toward others that may mirror or exceed that found among homicide-only cases. Although typological work on homicide-suicide has been undertaken by others (e.g., Marzuk et al., 1992), the approach proposed above would extend such investigation by adding a crucial comparative element.
Although interpretive caution should be applied, the present results have practical implications, and highlight potential intervention points. For example, the finding that homicide-suicide perpetrators were more likely than homicide-only perpetrators to have had contact with a mental health professional may inform improved health system practices. Gatekeeper training of medical practitioners is recognized as useful in suicide prevention (e.g., Mann et al., 2005), and the current results suggest value in incorporating training about the possibility of violence toward others, as well as to the self. Also, characteristics that may differentiate the homicide-suicide group from either of the other two groups, such as having a DVO in place at the time of the incident, suggest possibilities for intervention through the policing and justice systems; practitioners in these fields may benefit from improved knowledge about violence toward the self, as well as to others. The current findings suggest that policies may need to be built on a fundamentally collaborative basis, bringing together knowledge held by a range of health and justice professionals. An example of how this could look in practice is through more refined and evidence-based risk assessment tools that combine comprehensive knowledge from traditionally disparate fields.
In its introductory section, this article highlighted ongoing uncertainty over whether homicide-suicide events can be best understood from a suicidological perspective, a criminological perspective, or both—as well as whether homicide-suicides have their own unique set of features. The current results hint that homicide-suicide may indeed have some “unique” characteristics setting it apart from homicide and suicide. However, the findings also suggest that it may be prudent for any theoretical framework to treat homicide-suicide as, on various other characteristics, resembling both homicide-only and suicide-only. It is reasonable to suggest that there remains substantial work ahead before a satisfactory theoretical framework can be developed and robustly tested against comprehensive data.
A range of limitations should be acknowledged. For example, the small sample of homicide-suicide cases necessarily entails the use of interpretive caution. Similarly, although a strength of the study is that it improves international knowledge of homicide-suicide, it is still based on a Western population, and the results may not necessarily be generalized to a non-Western population. The data sets used different data collection methods, each with different strengths and weaknesses, which can introduce different forms of response bias. The QSR relies on third-party reports, which may be incomplete, inconsistent, or narrow in focus, whereas the AHP uses self-report data, which may raise concerns over reliability or social desirability bias. A key issue in the homicide-suicide group was how little information had been recorded for many cases, especially regarding risk factors and possible triggering events, relative to homicide-only and suicide-only cases. This cannot be readily explained by reference to the use of different data sets; the homicide-suicide cases were drawn from the same data set as the suicide-only cases, hence it appears the discrepancy in missing data reflects a difference in the types of data sought and recorded by officials during suicide-only cases relative to homicide-only cases. This suggests a need for enhanced data collection, particularly about perpetrator attributes, during homicide-suicide investigations. An important future direction is to explore in more detail the differences between different “types” of homicide-suicide events (e.g., intimate partner homicide-suicides, relative to homicide-suicide events involving acquaintances or strangers); this was out of the scope of the current work, but may assist in strengthening some of the present results. For example, if an intimate partner homicide-suicide group was compared with an acquaintance homicide-suicide group, differences in the relative prevalence of relationship, legal, or mental health issues between each of these groups may become more apparent.
A key question the present study could not address was why many individuals may experience the same circumstances observed among various homicide-only, suicide-only, and homicide-suicide cases, without resorting to violence. There is an obvious need to develop a more detailed comparative methodological approach to understanding potential connections between an individual’s characteristics, personality, and circumstances, including their life history, and the use of violence toward others or the self (or both). It would be beneficial to explore this matter using an in-depth mixed-methods approach, with suitable control groups. Ideally, studies that control for some of the differences between the groups, to isolate the unique contributions of key variables, should be conducted; however, this was not possible in the current study due to the small homicide-suicide sample size. Finally, there may be benefit in conducting qualitative investigations, which would enable the small number of female homicide-suicide perpetrators to be studied.
While predicting the likelihood that a given individual will perpetrate homicide-suicide is undeniably an extremely difficult (if not impossible) task, this should not preclude attempts to develop an improved evidence base about factors—or combinations of factors—that may contribute to such incidents. Despite its limitations, the current study suggests that homicide-suicide may have unique characteristics that set it apart from both homicide-only and suicide-only, as well as sharing certain other characteristics with those other two types of events. In addition to providing new knowledge about homicide-suicide, these findings may assist with practical efforts to develop evidence-based prevention policies.
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of the various correctional departments across Australia for their significant support in the conduct of this research. The authors also thank the QLD Mental Health Commission for its ongoing support of the Queensland Suicide Register.
Authors’ Note
The views expressed in this report are those of the authors and do not represent the policies or views of the correctional departments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Australian Homicide Project was supported under Australian Research Council’s Discovery Projects funding scheme (Project DP0878364).