
Abstract
Sexual Assault Response Teams (SARTs) are multidisciplinary teams that coordinate multiple systems (e.g., medical, law enforcement, prosecutors, and rape crisis center advocates) to provide comprehensive care to victims and to collect high-quality forensic evidence to facilitate investigation and prosecution. Relatively little guidance is provided about effective teamwork strategies in resources on forming SARTs. Using in-depth surveys with the SART coordinators and telephone surveys (including close-ended and open-ended questions) with 79 professionals involved in three active, formal SARTs in one state, this study examined structural, organizational, and interpersonal factors that influence interprofessional collaboration on SART. Study findings indicate that perceived structural factors and interpersonal factors were significantly associated with SART members’/responders’ perceptions of the quality of interprofessional collaboration on their SART. Findings suggest that individuals’ perceptions of professionalization and power disparities between professions pose challenges to perceived interprofessional collaboration on SART. Compared with criminal justice and medical professionals, victim advocacy rated the level of collaboration on their SART significantly lower. The overall picture from the data was that SART professionals perceived mutual respect, trust, and commitment to collaboration to be pervasive on their SARTs, even though recognition of professional conflicts was also prevalent, suggesting that professionals understood that interpersonal conflict was distinct from professional conflict. Initial SART trainings should address the benefits of the team response, professional roles, and communication and conflict resolution skills, and ongoing training should provide professionals the opportunity to raise positive and negative examples of their collaborative efforts to explore existing tensions and constraints on the team for conflict resolution.
More than 18 million women and 3 million men report having been raped in their lifetime (Tjaden & Thoennes, 2008), and every year in the United States, it is estimated 1.27 million women are raped (Black et al., 2011). Inadequacies and limitations of the responses of the medical system, criminal justice system, and advocacy organization to victims including low reporting and prosecution rates, failure to provide comprehensive services to victims, and interactions that harm victims (such as victim blaming and not believing the victim) are well documented (Campbell, 2008; Campbell, Wasco, Ahrens, Sefl, & Barnes, 2001; Lonsway & Archambault, 2012; Martin & Powell, 1994; Spohn & Holleran, 2001; Wasco et al., 2004). Many communities have developed multidisciplinary teams, Sexual Assault Response Teams (SARTs), to coordinate responses of the medical system, criminal justice system, and victim advocacy organizations to sexual assault victims (U.S. Department of Justice, 2013). SARTs have dual purposes: (a) to provide comprehensive, timely care to victims to minimize trauma and to promote victims’ use of community services, and (b) to collect high-quality forensic evidence to facilitate investigation and prosecution of offenders (U.S. Department of Justice, 2004). Coordinated community responses to sexual violence are supported by the Violence Against Women Act (VAWA), with the rationale that a coordinated community response provides victims more comprehensive care, minimizes victim trauma by providing support persons, reduces the number of times a victim must recount the sexual assault to professionals, as well as facilitates the criminal processing of the case through improved evidence collection, documentation, and communication between agencies (U.S. Department of Justice, 2004). Yet, empirical research on how collaboration may influence victim and criminal case outcomes is lacking (Moylan, Lindhorst, & Tajima, 2015). Moreover, there is heterogeneity in the structure and level of functioning of SARTs (National Sexual Violence Resource Center [NSVRC], 2011; Zajac, 2009). Two national surveys of SARTs have found that the degree to which SARTs engage in collaborative processes (e.g., multidisciplinary case review, joint policy/protocol review, multidisciplinary training) varies (Greeson & Campbell, 2014; Zajac, 2009).
Differences in philosophical assumptions, theoretical perspectives, and methods among professions, which occur on any multidisciplinary team, may be particularly salient to the collaboration among professionals on SARTs. Evidence suggests that conflicts between key players such as advocates, medical providers, and law enforcement may occur and are largely attributed to a confusion or disagreement about professional roles or to differences in philosophies, values, and perspectives on sexual assault and victim needs (Cole & Logan, 2008; Crandall & Helitzer, 2003; Maier, 2012; Martin, 2005). Unresolved conflict on teams is associated with decreases in team effectiveness and team member satisfaction (Behfar, Peterson, Mannix, & Trochim, 2008; Lemieux-Charles & McGuire, 2006; Tekleab, Quigley, & Tesluk, 2009). Yet, relatively little guidance is provided about effective teamwork strategies in resources on forming SARTs (NSVRC, 2011). Systematic assessment of the quality of coordination or collaboration among key community responders to sexual assault victims has received limited attention in the literature (Greeson & Campbell, 2012; Martin, 2005).
To examine whether greater collaboration among the community responders leads to improvements in attaining the dual objectives of SARTs, the first step is to better understand variability in interprofessional collaboration and the factors that may influence collaboration on SARTs (Sicotte, D’Amour, & Moreault, 2002). Most of the conceptual frameworks that have been used to examine teamwork have been based in organizational theory and are based on a logic model, incorporating input-process-output-outcome factors (McNamara, 2000; San Martin-Rodriguez, Beaulieu, D’Amour, & Ferrada-Videla, 2005; Sicotte et al., 2002). A review of the literature on interprofessional collaboration, 1 which is largely based on multidisciplinary teams of health care professionals, reveals various attributes conceptualized to be dimensions of interprofessional collaboration and hypothesized factors that influence the quality of collaboration among professionals (Henneman, Lee, & Cohen, 1995; McCallin, 2001; Pence & Wilson, 1994; Reese & Sontag, 2001; Sands, Stafford, & McClelland, 1990). Interprofessional collaboration is a multidimensional construct, representing a group work process (Petri, 2010) with various attributes (Henneman et al., 1995). A review of the literature reveals conceptual ambiguity with regard to dimensions of collaboration and antecedents that influence collaboration. For example, trust is depicted as a dimension of interprofessional collaboration in at least one conceptual definition (D’Amour, Goulet, Pineault, Labadie, & Remondin, 2004), whereas in other models, it is depicted as an antecedent of collaboration (Bronstein, 2003; San Martin-Rodriguez et al., 2005). Because collaboration is typically viewed as a process, with “multilevel, overlapping, and interrelated subprocesses that often take place not only sequentially, but also simultaneously” (Billups, 1987, p. 147), feedback loops likely exist in the teamwork or collaborative process. Nevertheless, commonalities in the defining attributes exist between the various conceptual definitions such as team members having a common purpose, interdependence, flexibility, and group rules (Bronstein, 2003; D’Amour, Ferrada-Videla, San Martin Rodriguez, & Beaulieu, 2005; Ovretveit, 2000; World Health Organization [WHO], 2010).
Bronstein’s (2003) model of interdisciplinary collaboration was based on four theoretical frameworks (e.g., multidisciplinary theory of collaboration, services integration, role theory, and ecological systems theory). The conceptual definition of interprofessional collaboration that Bronstein used was taken from Bruner (1991): “an effective interpersonal process that facilitates the achievement of goals that cannot be reached when individual professionals act on their own” (Bronstein, 2003, p. 299). The conceptual framework then served as the foundation for a multidimensional measure of interprofessional collaboration for multidisciplinary team with health professionals and social workers—a type of team that is more closely related to a SART. The multiple dimensions of collaboration included in Bronstein’s model are interdependence, newly created professional activities, flexibility, collective ownership of goals, and reflection on process. Bronstein’s model also postulated several factors (e.g., personal, professional role, structural characteristics) to influence interprofessional collaboration.
Several structural factors, which are “conditions outside the organization, such as components of social, cultural, educational, and professional systems” (San Martin-Rodriguez et al., 2005, p. 134) are included in the study to examine their association with SART members’ perceptions of the quality of interprofessional collaboration. First, professionalization is a social process that promotes autonomy, dominance, and control over the profession’s realm, as well as competition and exclusivity in relation to other professions (Bronstein, 2003; Hall, 2005; San Martin-Rodriguez et al., 2005; Sicotte et al., 2002). Professionalization also inculcates individuals into the philosophical assumptions, theoretical perspectives, values, and methods of the profession (Clark, 1997). Significant differences exist between professions in their worldviews, which can lead to conflict when professionals engage in interprofessional work (San Martin-Rodriguez et al., 2005). One difference in values that may apply to SARTs is the degree of importance different professions place on client confidentiality (Hall, 2005). Moreover, greater status may be given to certain professions within the team, which can render power differentials between team members (Hall, 2005) and inhibit collaboration (Baggs & Schmitt, 1997; Irajpour & Alavi, 2015).
Organizational factors are “attributes of the organization that define the work environment of the team, such as its structure and philosophy, team resources, and administrative support, as well as communication and coordination mechanisms” (San Martin-Rodriguez et al., 2005, p. 138). Optimal conditions for interprofessional collaboration include a nonhierarchical organizational structure, shared and centralized leadership that supports collaboration, time and space for collaboration to occur, protocols and policies that help to coordinate efforts, and regular and unimpeded communication between team members (Allen, 2005; Baggs & Schmitt, 1997; Costa, Barg, Asch, & Kahn, 2014; D’Amour et al., 2004; Henneman et al., 1995; Ovretveit, 2000; San Martin-Rodriguez et al., 2005; Silén-Lipponen, Turunen, & Tossavainen, 2002).
The process variables pertain to the interpersonal interactions between team members. Conceptual and empirical work supports the importance of communication and conflict resolution skills, trust and mutual respect among members, and a commitment to collaboration as important influences of the quality and level of interprofessional collaboration (Henneman et al., 1995; McCallin, 2001; Ovretveit, 2000; Pfaff, Baxter, Jack, & Ploeg, 2013; San Martin-Rodriguez et al., 2005; Sicotte et al., 2002; Silén-Lipponen et al., 2002; Wachs, 2005).
Nonetheless, it is unclear how well these findings from multidisciplinary health care teams generalize to SARTs, which bring together even more disparate professionals and systems (e.g., medical, law enforcement, prosecutors, and victim services). Multidisciplinary teams in health care are primarily concerned with promoting the health of patients. Even with this common objective in mind, differences in the philosophies and values of the various professionals may conflict (Jones, 2006). Yet, the dual objectives of SARTs, which can be in conflict at times, and the markedly different philosophies and values of the professionals comprising the SART (e.g., nurse, victim advocate, and law enforcement) may pose an even greater challenge to the collaboration of the multidisciplinary team than may be found in a health care multidisciplinary teams.
The purpose of this study is to examine SART members’ ratings of interprofessional collaboration as well as to examine the relationship of structural, organizational, and interpersonal factors to SART members’ ratings of interprofessional collaboration. Conducting this project contributes to the literature in a number of ways. First, this study systematically evaluates interprofessional collaboration on SARTs, which has received limited research attention. Second, structural, organizational, and interpersonal factors that influence the quality of collaboration among SART professionals are examined using not only quantitative measures based upon prior empricial work on multidisciplinary health care teams, but also using exploratory, qualitative data collection to examine factors that may be unique to SARTs. The research questions are as follows:
Method
The proposed project is a multiple case study, using concurrent mixed-methods procedures.
Participants
The only three active SARTs with formal memoranda of agreement in the state, located in three different communities (A, B, C), were selected for the study. At the beginning of the study, face-to-face, semistructured interviews were conducted with each of the SART coordinators. Survey participants for the three selected SARTs were identified and recruited with key informant sampling, which is described in the “Procedure” section. A total of 89 possible participants were identified with the key informant sampling, and a total of 79 surveys were completed. Four individuals declined to participate, and the remaining six were never successfully contacted or completed the survey. The response rate was 89.8%.
The sample was composed of the following percentages of individuals from the sampled professional groups: 27.8% (n = 21) medical, 30.4% (n = 24) law enforcement, 13.9% (n = 11: prosecutor, n = 8, or victim advocate in the prosecutor’s office, n = 3), and 27.8% (n = 22) rape crisis victim advocate. Victim advocates in the prosecutor’s office were included in the group of prosecutors because their comments indicated they were more closely aligned with prosecutors than with victim advocates in community-based agencies. The majority of the sample was female (82.3%). The sample was highly educated, with 46.8% reporting that their highest level of education was a bachelor’s degree, and 32.9% had a master’s degree or other professional degree. Participants reported a mean of 11.6 years in their current profession and working on sexual assault cases for a mean of 8.8 years.
Measures
Output variable: Interprofessional collaboration
The quantitative measure that was used is a summated scale of a modified version of the Index of Interdisciplinary Collaboration (IIC; Bronstein, 2002). The original index was developed to examine the extent of collaboration of social workers with other professions, and was a 49-item scale, with five Likert-type scale responses. Internal consistency reliability analysis was conducted on the 42 items that loaded on one of the five factors (Cronbach’s α = .92). There was support for construct validity, with greater levels of collaboration being associated with greater organizational support, informal relationships between collaborators, trust, and a positive history of collaboration. Bronstein’s IIC is scored so that lower scores represent greater collaboration. Bronstein (2002) stated that the scale was adaptable for use by other professions through wording changes. The version used in the current study had 33 items: Nine items were dropped because they had low face validity when applied to SARTs. For example, one item on the IIC states that collaborators encourage the involvement of family members in the treatment process. Because the convention is for scales to be scored so that higher values represent greater degrees of the measured construct, the response set for items was altered to be 1 (strongly disagree) to 5 (strongly agree) on the positively worded items. Therefore, a higher score represents greater collaboration in the current study. The internal consistency reliability was good in this sample (Cronbach’s α = .832). All Likert-type scale items used in the survey used the same response options. The IIC is composed of five summated subscales: Interdependence (11 items), Flexibility (six items), Collective Ownership of Goals (six items), Group Innovation/Newly Created Professional Activities (four items), and Reflection on Process (six items).
Input variable: Structural factors
Professional role was operationalized in two ways. First, the construct was measured with one Likert-type scale item that was included in a study of health care teams (Sicotte et al., 2002), “Professionals working on sexual assault cases have strong allegiances to their professions that sometimes create problems with working with other professionals.” Second, participants were asked whether miscommunication or conflict occurs between team members because of differences in professional philosophies, theoretical perspectives, and values, and if so, participants were asked to provide an example. A Likert-type scale item asked participants to rate how much maintaining victim confidentiality posed particular challenges to professionals coordinating work. Power disparity was measured with three Likert-type scale items taken from research studies on multidisciplinary teams (MDT) (Bronstein, 2002; McCallin, 2001; Sicotte et al., 2002) that were summed. The statement, “Hierarchical status among professional groups on SART is evident” (Sicotte et al., 2002) was followed by an open-ended question about the order of the professional groups in the hierarchy.
Input variable: Organizational factors
Agency support was measured with an item that asked participants how much their parent agency provided them with support to work with other team members, using a scale from 0 (0%) to 100 (100%). Shared leadership was measured with a Likert-type scale item “Leadership tends to be shared equally by representatives of particular agencies or institutions” (D’Amour et al., 2004).
Process variables: Interpersonal factors
Mutual respect was measured with three Likert-type scale items on the survey, which were based on items included in Sicotte et al.’s (2002) study; for example, “Different professional groups recognize the competence of others on the team.” Ratings were summed, so that higher scores indicate higher respect (Minimum = 3, Maximum = 15). Trust was measured with one Likert-type scale item: “Professionals trust one another to do what they say they will do.” Communication skills was measured with five Likert-type scale items. Two items are focused on conflict resolution skills, for example, “Some disagreements or problems are not addressed by the team in the hopes that they will be resolved naturally” (McCallin, 2001), and the other three items related to communication and group decision making, for example, “Discussion between members tends to be limited to discussion of specific issues after they have arisen” (D’Amour et al., 2004). After the responses were reverse scored, a sum of the items was computed, with a higher score representing greater communication (Minimum = 5, Maximum = 25). Commitment to collaboration was operationalized in the survey with three Likert-type scale items, which were based on items included in Sicotte et al.’s study; for example, “Members have high motivation to work with other professional groups.” A sum of the three items was computed (Minimum = 3, Maximum = 15).
Procedure
The protocol for this proposed project was approved by the university Institutional Review Board (IRB). In-depth, semistructured, face-to-face interviews were conducted with the three SART coordinators on-site to gather information on the historical development, organizational structure and management, and resources of each SART. Participants for the telephone survey were recruited with three strategies. First, names of possible survey respondents involved on the SART (e.g., sexual assault nurse examiners [SANEs], prosecutors, rape crisis center personnel, and law enforcement officers who attended the interagency council meetings) were collected from each SART coordinator at on-site visits. Second, the researcher contacted the rape crisis centers in each community to inform them about the study and to solicit contact information of staff members and volunteer advocates who had experience working as part of a SART within the past 3 months. Third, at the conclusion of each telephone survey, the researcher asked participants to provide the names and contact information of any other professionals who had experience working as a part of or in conjunction with SART. New names were recorded and entered into the sampling frame. The researcher attempted to contact these referred individuals to tell them about the study and to ask if they would be willing to participate in the telephone survey. No identifying information was written on the surveys. The first author conducted all of the telephone surveys, which lasted between 25 and 50 min each (M = 31).
Data analysis
Responses to close-ended questions from the telephone surveys were entered into SPSS for descriptive and bivariate analysis. Independent-samples t test was used to examine interprofessional collaboration by professional group. Bivariate statistical tests were conducted to examine the relationship between structural, organizational, and interpersonal factors with interprofessional collaboration (e.g., Pearson coefficient, Kendall’s tau, and chi-square test of independence). Responses to open-ended questions were coded in several phases, using NVivo to organize the data. First, coding began with the author reading all of the open-ended questions and responses, then creating codes to capture the responses. Second, the codes were grouped into more abstract categories (Straus & Corbin, 1998). Third, the author did line-by-line coding of a randomly selected sample of cases to further refine the coding categories (Creswell, 2003). Fourth, using the codes created in the previous step, a research assistant conducted line-by-line coding of all the open-ended responses. Fifth, a randomly selected 25% of cases were coded independently by the first author and the research assistant. For any question that yielded intercoder reliability less than .90, the team discussed how to clarify the codes, and then they independently coded a new sample of randomly selected cases; the process was repeated until intercoder reliability was .90 or higher. The author trained the research assistant on coding open-ended data for approximately 8 hr before the research assistant began coding. Themes identified in the qualitative analysis were analyzed by group (i.e., the three SART programs), and the results were not statistically significantly different by program. Therefore, to render the results more easily interpretable by readers, the results presented here are combined for all three SART programs.
Results
Background on SARTs
All three SARTs had been operating for 6 or 7 years when data were collected. SART (A) covered four counties with an estimated population of 393,530 (U.S. Census Bureau, 2010), wherein approximately 30 law enforcement agencies operated. Medical-forensic exams were conducted in two private, competing hospitals that worked out an agreement that their staff would act together under the umbrella of one SANE program, permitting nurses employed at one hospital to provide care to victims in the other hospital. The second site (B) is located in a metropolitan area with an estimated population of 295,803 (U.S. Census Bureau, 2010). The SANE program is located in the police department and exams are conducted in the emergency department of a Level I trauma center. The third site (C) includes a metropolitan area with an estimated population of 741,096 (U.S. Census Bureau, 2010). Exam sites are in the emergency department of a Level I trauma center and in a nonprofit organization for individuals who are medically cleared to be seen outside of the emergency department setting and who choose this location. At all three sites, victims must be 14 years old or older, and present for care within 96 hr of the sexual assault to receive the medical-forensic exam. The number of medical-forensic exams conducted annually ranged from 75 to 170 for the three sites. The SART coordinators for each of the sites were the SANE program managers.
Interprofessional Collaboration
Comparisons of participants’ scores on the IIC and the five subscales of the index by professional group were analyzed with one-way ANOVA. The results are presented in Table 1. Victim advocacy professionals had significantly lower scores on the IIC and the interdependence, group innovation, and reflection on process subscales compared with medical and criminal justice professionals. Also, victim advocacy professionals had a significantly lower score on the collective ownership of goals subscale compared with medical professionals. There were no significant differences in scores between medical and criminal justice professionals on any of the subscales.
Ratings of Interprofessional Collaboration and Dimensions by Profession.
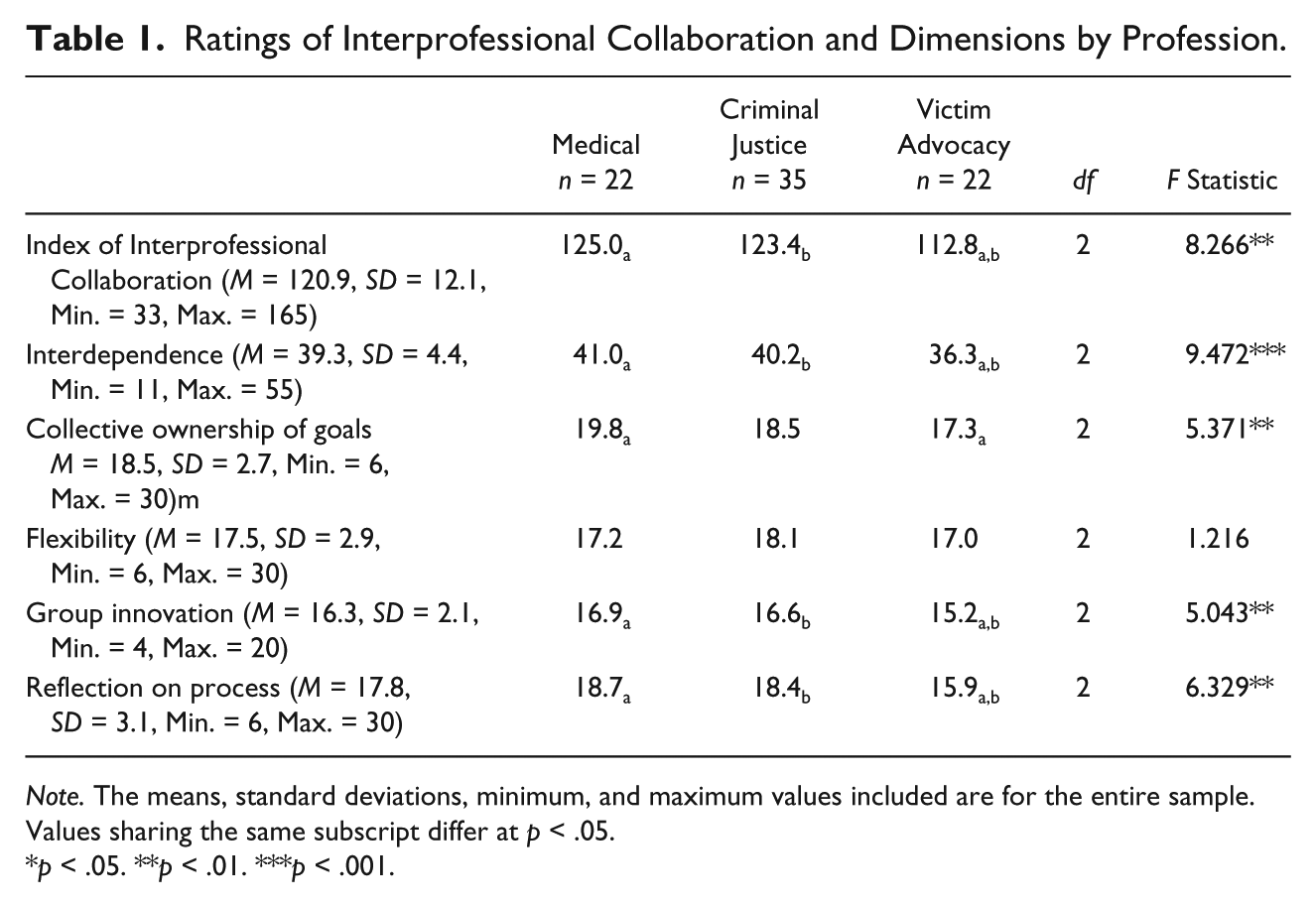
Note. The means, standard deviations, minimum, and maximum values included are for the entire sample. Values sharing the same subscript differ at p < .05.
p < .05. **p < .01. ***p < .001.
Structural, Organizational, and Interpersonal Factors and Interprofessional Collaboration
Individuals who perceived that professionals had strong allegiances to their own professions had lower scores on the IIC. In addition, survey participants were asked whether there were conflicts between professionals that they attributed to differences in professional philosophies, values, and methods. The majority of participants (74.7%, n = 59) responded that there were conflicts due to professional differences. There was no significant association between the perception of conflicts that were due to professional differences and IIC scores. Three t tests were conducted to examine whether there was an association between the most frequently mentioned themes (Not mentioned/Yes mentioned) that emerged from participants’ descriptions of the types of professional conflicts and the IIC scores: professional focus, 122.5 versus 119.5, t(77) = 1.107, p > .05; orientation to the victim, 121.3 versus 120.2, t(77) = 0.398, p > .05; and victim blaming, 121.3 versus 115.8, t(77) = 1.063, p > .05.
Different professional focus, including different orientations to the victim, were the most frequently cited explanation for conflicts between professionals:
Different biases people have about rape victims. It can be due to their profession or their gender or other beliefs. For example, law enforcement, because they are there to investigate and because of what they see in their jobs, they are more cynical. They always ask me, “Is it real?” The advocate is just there to believe the victim. They don’t question what happened. (SANE)
Of the 59 individuals who stated there were professional conflicts, 32.2% reported that victim advocacy was involved (12.5% of medical, 29.2% of criminal justice, and 52.6% of victim advocates). The same percentage (32.2%) mentioned law enforcement was involved in professional conflicts (50.0% of medical, 20.8% of criminal justice, and 31.6% of victim advocates).
Law enforcement’s goals are very different—what they are after. Partly due to training, they have less sensitivity to the victim. They say they are trying to find out the truth, but it seems like they rush to disbelieve the victim. (Rape crisis advocate) The rape crisis center is there to solely focus on the victim. I understand their role but I don’t think they understand that we need certain things for the case to proceed. You can’t build a case by not asking questions. (Patrol officer)
Some participants’ discussion of the conflict among professions also pointed out how the different professional perspectives were also the source of strength of the SART:
The nature of any MDT. SANEs fundamentally see the victim as a patient, law enforcement sees the victim as a crime victim and source of information, and rape crisis sees the victim as someone to support. The interagency council helps to bridge the gaps and allow one to see the larger picture that we are all there for the same reasons: To help the victim and to get the bad guy. (Police officer)
Individuals who agreed that maintaining victim confidentiality posed a challenge to collaboration gave lower ratings of interprofessional collaboration on their SART (see Table 2). Among those individuals who reported that victim confidentiality did pose a challenge to coordinating among professionals (n = 25), almost all (92%) stated the challenge was that information sharing was limited (not depicted in a table). A common scenario described in this category was that because victim advocates have a different statutory obligation to maintaining victim confidentiality than SANEs and criminal justice personnel, other team members sometimes viewed victim advocacy as a roadblock to information exchange that would help team members work more effectively. Cole (2011) presented a detailed analysis of the issue of victim confidentiality on SARTs for this study.
Associations of Structural, Organizational, and Interpersonal Factors and Interprofessional Collaboration.
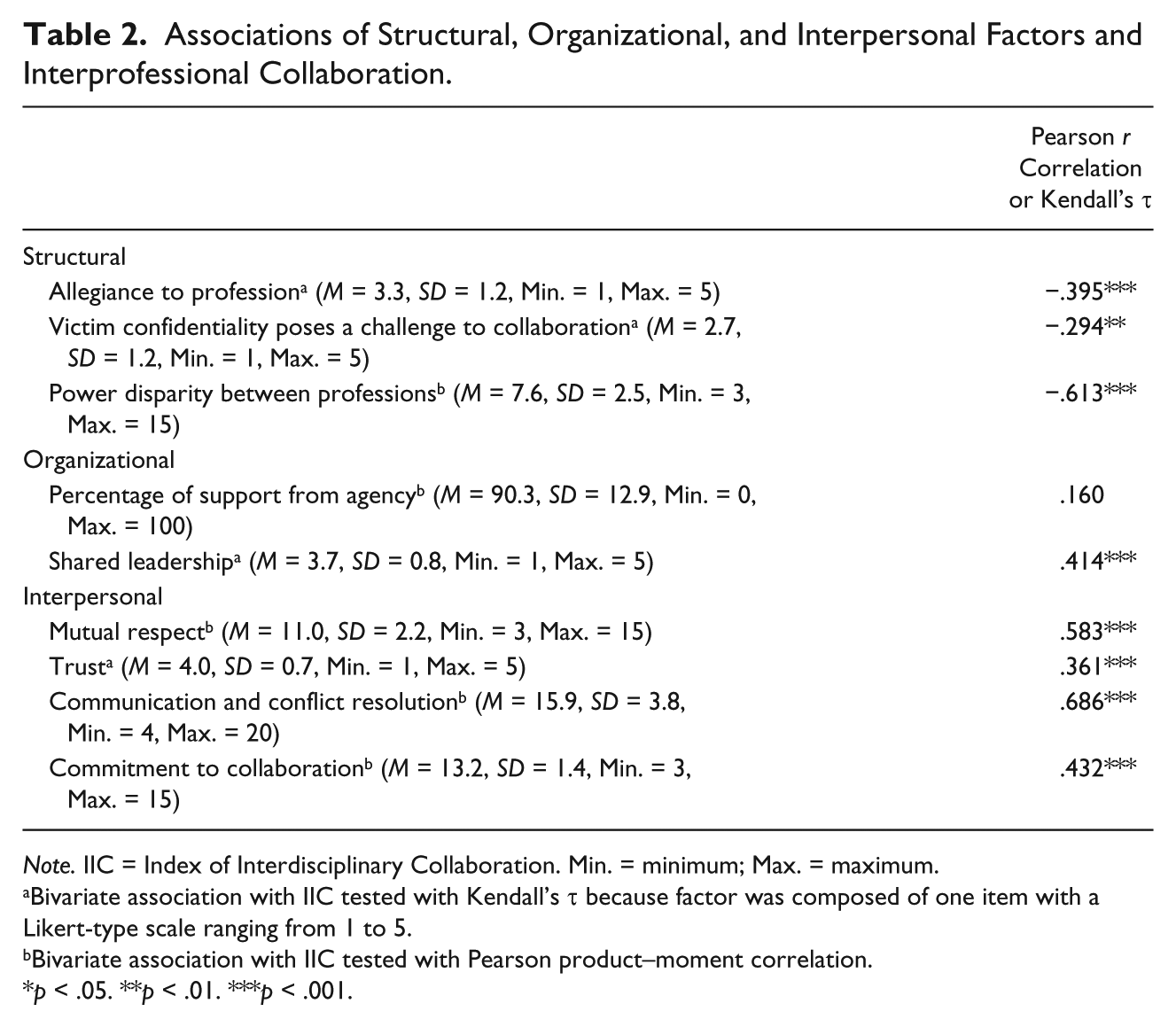
Note. IIC = Index of Interdisciplinary Collaboration. Min. = minimum; Max. = maximum.
Bivariate association with IIC tested with Kendall’s τ because factor was composed of one item with a Likert-type scale ranging from 1 to 5.
Bivariate association with IIC tested with Pearson product–moment correlation.
p < .05. **p < .01. ***p < .001.
Individuals’ perceptions of greater power disparity were correlated with lower ratings of interprofessional collaboration (see Table 2). When asked whether there was a hierarchy in the SART, a small number of participants referred to professionals devaluing the contributions of volunteer advocates. All of the victim advocacy organizations used volunteers to provide hospital advocacy during off business hours. For instance, a rape crisis center administrator responded, “No hierarchy at the leadership dimension of SART, but more with the initial response. The use of volunteer advocates adds to this.”
As another indicator of power disparity, participants’ perceptions that a hierarchy exists on the SART were examined in relation to IIC scores. Because only 12.8% (n = 10) reported a neutral response, these cases were excluded from the analysis. Participants who believed that a hierarchy was evident on the SART (38%) had lower IIC scores than participants who did not believe there was a hierarchy, 115.6 versus 125.7, t(47.6) = 3.398, p < .01. When perceptions of the order of the hierarchy were examined in a matrix by profession, a few interesting findings were evident. First, most law enforcement officers stated that law enforcement was at the top of the hierarchy, SANE was in the middle, and victim advocacy at the bottom. Second, only two SANEs believed that there was a hierarchy on the SART, and these two individuals stated that SANEs or the medical director were at the top of the hierarchy. Third, all victim advocates who believed that a hierarchy among professionals existed stated that either law enforcement or SANEs were at the top, followed by SANEs, law enforcement, or prosecutors, and that victim advocates were at the bottom. Thus, victim advocates who perceived of a hierarchy all believed that victim advocates were in the position of least authority or power.
Interviews with the SART coordinators revealed that the ways in which participating agencies contributed human and material resources to SARTs were similar across sites. None of the resources for each of the SARTs was devoted to the SART as a team, but instead were made available to the SART through the individual participating agencies. Survey participants’ quantitative ratings of the support they received from their parent agencies for their work on SART, which were high (M = 93.35, Minimum = 50, Maximum = 100), were not significantly associated with IIC scores (see Table 2). However, the restricted variance of the values for the percent of support from parent agencies is problematic when computing the Pearson correlation coefficient. The majority of participants agreed or strongly agreed that leadership was shared equally by representatives of different agencies. Individuals who agreed/strongly agreed that leadership was shared equally by representatives of different agencies had higher IIC scores (see Table 2).
The univariate statistics for the interpersonal factors reveal that participants, on average, perceived of high levels of mutual respect, trust, and communication and conflict skills on their SARTs: the means are high, and standard deviations reveal low variance (see Table 2). Individuals who perceived of greater mutual respect, greater trust, greater communication and conflict skills between professionals on the SART, and greater commitment to the team of SART professionals rated the quality of interprofessional collaboration on their SART as higher.
Discussion
Study findings indicate that SART members’ perceptions of structural factors (including professional differences) were significantly associated with their perceptions of the quality of interprofessional collaboration. Consistent with other studies, this study’s findings suggest that professionalization poses a challenge to interprofessional collaboration on SART (D’Amour et al., 2005; Jones, 2006; Sicotte et al., 2002). For example, victim advocates across the three sites gave lower ratings of interprofessional collaboration compared with the ratings given by criminal justice and medical personnel. Second, individuals’ perceptions that SART professionals have strong allegiances to their own professions were associated with perceptions of lower collaboration on SARTs. Furthermore, professionals’ differing levels of obligation to maintaining confidentiality has been found in a small number of studies as a potential obstacle to interprofessional collaboration (Darlington, Feeney, & Rixon, 2004, 2005; Ovretveit, 2000; Reese & Sontag, 2001). Some professionals viewed the one-way information on clients that stemmed from the rape crisis workers’ privileged communications with clients, as evidence of a lack of reciprocity, which engendered frustration. Because sharing information is the most visible aspect of collaborative work (Darlington et al., 2004), when there is a breakdown in information sharing, there may be detrimental ripple effects on the collaborative relationships.
The findings revealed an association of the perception of power disparity among the professions with lower ratings of interprofessional collaboration. Even though only a minority of participants (38.5%) perceived of a hierarchy among professionals on SART, the patterns of individuals’ rankings of professions in the hierarchy were telling. All of the participants who reported there was a hierarchy on the SART placed victim advocacy at the bottom of the hierarchy with law enforcement and/or SANEs at the top or middle. Unlike the health care and criminal justice systems, which have statutory obligations for responding to sexual assault victims, rape crisis centers participate in the community response to sexual assault with the permission of those other systems (Martin, 2005; Moylan et al., 2017). Victim advocacy organizations may perceive their place in the community response to sexual assault victims as tenuous. Furthermore, because all of the victim advocacy organizations used volunteers to provide hospital advocacy during off business hours, difference in professional/volunteer status may contribute to a devaluing of victim advocacy.
Many participants expressed the idea that professional conflicts were to be expected, and are perhaps unavoidable, because of the different foci and orientations to victims that the different professions have. Part of the strength of multidisciplinary work is that each profession has a unique contribution to make. If conflicts are inevitable, it is reasonable to assume that successful teams will use conflict resolution skills to transform the conflict into a beneficial outcome, such as improved services, innovation, and greater interagency understanding. Not all conflicts are equal; some conflicts are constructive whereas other conflicts are destructive to the group effort (De Dreu, 1997). Constructive conflict may be more likely to occur in settings where frequent and open communication occurs, including direct communication about conflicts, conflict resolution strategies are firmly in place, and there is no power disparity between participants (Assael, 1969). Moreover, the nature of the conflict may affect the outcome of the conflict. For example, De Dreu (1997) asserted that cognitive conflict enhances problem solving, whereas affective conflict increases contention.
Study participants, on average, perceived of shared leadership on their SARTs and participants who perceived of shared leadership among agencies on SART rated the quality of interprofessional collaboration on SART as higher. Shared leadership may be particularly important when the participating agencies function independently and do not answer to a shared authority such as an umbrella agency. Some research suggests that shared decision making may be even more important to collaboration than leadership (Allen, 2005; Nicholson, Artz, Armitage, & Fagan, 2000).
The overall picture from the data was that SART members perceived that mutual respect, trust, and commitment to collaboration were pervasive on the SARTs, even though recognition of professional conflicts was also prevalent, suggesting that professionals understood that interpersonal conflict was distinct from professional conflict. Interestingly, identification of professional conflicts was not associated with perceptions of collaboration. Ignoring or minimizing professional differences weakens the team. Ovretveit (2000) posited that individuals on MDTs minimize professional differences for a variety of reasons, including fear that differences will destroy the team, professional competition and jealousy, and fear of one profession becoming more dominant. A well-functioning MDT has members who acknowledge professional differences without amplifying them, possesses the means to recognize common ground, and possesses the means to work through differences (Ovretveit, 2000). Thus, acknowledgment of professional differences is seen as a positive element of MDT work, particularly when interpersonal differences are minimal (Tekleab et al., 2009). Along with that recognition is the necessity of professionals exploring and understanding the organizational and professional cultures of the other MDT members (Johnson, Zorn, Tam, Lamontagne, & Johnson, 2003).
Study Limitations
The study findings must be discussed within the context of the limitations of the study. First, the three SARTs selected into the sample—the only three active SARTs in the state—may not be representative of SARTs in other states. In addition, it is possible that the key informant purposive sampling may have missed individuals with divergent perspectives on SARTs. Second, the small sample size limited the statistical analysis that could be performed. The small sample size and number of study variables rendered the data unsuitable for multivariate analysis, which would have added statistical control to the analysis. The bivariate analysis of associations among study variables must be interpreted with the caveat that statistical control is lacking. Nonetheless, the small sample size allowed for the inclusion of some qualitative methods, which added to the understanding of the contexts in which SART professionals work. Third, examining collaboration on SARTs with the primary unit of analysis at the level of individual has some problems. The measures of structural, organizational, and interpersonal factors as well as the output variable of interprofessional collaboration measured participants’ perceptions of these factors and constructs. A certain amount of shared variance between the input, process, and output variables is expected. More objective measures of these factors may reveal different relationships. Furthermore, inferring findings from individuals to group phenomenon may result in misinterpreting findings, in other words, ecological fallacy. However, conducting multiple case studies of SARTs without examining within-group differences may also result in misinterpretation of findings (Allen, 2005). Conducting future studies on the quality of collaboration with larger samples of individuals in a larger number of SARTs would allow for hierarchical linear modeling (HLM) analysis, which would allow for a multilevel analysis of nested data (Allen, 2005).
Implications
Study findings support the need for initial and ongoing joint training among professionals working on SART. Because significant associations with lower perceived collaboration on the SARTs in this study were related to SART members’ perceptions of professional factors such as allegiance to professions, hierarchy between professions, and power disparities, initial training should address the benefits of the team response, professional roles, and communication and conflict resolution skills. Ongoing training should provide professionals the opportunity to raise positive and negative examples of their collaborative efforts, and explore existing tensions and constraints on the team. Furthermore, the apparent lower status of victim advocates on some SARTs should be openly addressed in trainings to counteract this dynamic.
Greater attention to the conditions that maximize constructive conflict and minimize destructive conflict is needed in the research and practice literature on SART. A better understanding of how professional groups on SARTs acknowledge, discuss, and resolve conflicts—in particular ones that result from the varied ways the professions orient themselves to the social problem of sexual assault and victims of sexual assault—is crucial for improving community responses to sexual assault. Future research could identify the ways in which SARTs are able to convert professional conflicts into improved service delivery to victims and more successful prosecution of offenders (Moylan et al., 2017).
In light of the fact that the move toward victim-centered care was the impetus behind the development and establishment of SANE/SART models of service delivery (U.S. Department of Justice, 2004), the lack of systematic evaluation of victims’ perspectives on the SANE/SART response versus the traditional community response to sexual assault victims is a significant gap in the literature that future research should address. Moreover, future research should endeavor to link collaborative practice to team outcomes, such as victim’s experiences with the SART process and criminal justice system outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project was funded through the University of Kentucky Center on Drug and Alcohol Research Petite Research Grant.