
Abstract
Corporal punishment is a widely used and widely endorsed form of parental discipline. Inter-partner violence places enormous stress upon women. The rate of corporal punishment is higher in homes where other types of domestic violence are also occurring. This study compares two groups: those who participated in an intervention for women exposed to intimate partner violence (The Moms’ Empowerment Program [MEP]) and those in a comparison group. Using standardized measures, women in both groups were assessed at baseline and at the end of the program, 5 weeks later. The 113 mothers who participated in the MEP program had significantly improved their parenting, such that they had less use of physical punishment post-intervention. Findings suggest that a relatively brief community-based intervention program can reduce the use of parental physical punishment even in disadvantaged populations coping with stressful circumstances.
The use of physical punishment in the home is one of the most widely accepted and commonly practiced forms of discipline in the United States. (Lee, Grogan-Kaylor, & Berger, 2014). Although the rates of corporal punishment have decreased between 1975 and 2002, rates of spanking, slapping and hitting with an object still remain relatively high (Zolotor, Theodore, Runyan, Chang, & Laskey, 2011), and rates of spanking/slapping are almost unchanged for children between the ages of 3 and 5 years (Zolotor et al., 2011). In 2002, 79% of children between the ages of 3 and 5 years were slapped/spanked in the past year and 34% of children aged 3 to 11 years were hit with an object by their parent or caregiver (Zolotor et al., 2011). Experiencing corporal punishment in childhood has been associated with various negative outcomes, including increased aggressive behavior and delinquency in both childhood and adulthood (Gershoff, 2002; Grogan-Kaylor, 2004) and poorer mental health throughout the life span (Gershoff, 2002). The negative effects of corporal punishment are related to the frequency of its use. According to a study by Aucoin, Frick, and Bodin (2006), children exposed to high amounts of corporal punishment (three or more times in a 2-week period) had greater depressive symptoms, felt more inadequate, and were more aggressive than children who were exposed to less frequent or no corporal punishment.
Research also suggests that the rate of corporal punishment is higher in homes where other types of violence are also perpetrated (Postmus, Huang, & Mathisen-Stylianou, 2012; Taylor, Lee, Guterman, & Rice, 2010). One such form of violence linked to corporal punishment is intimate partner violence (IPV). IPV is a pressing public health issue, with nearly 15.5 million children exposed to such violence each year (McDonald, Jouriles, Ramisetty-Mickler, Caetano, & Green, 2006). Although IPV affects children of all ages, preschool-age children are at particularly great risk for exposure, given that these children are often in close physical proximity to their mothers (Fantuzzo & Fusco, 2007). Exposure to IPV has been associated with various maladaptive outcomes, including internalizing and externalizing problems (Graham-Bermann, Lynch, Banyard, DeVoe, & Halabu, 2007; Kitzmann, Gaylord, Holt, & Kenny, 2003; Miller, Howell, & Graham-Bermann, 2012) as well as childhood post-traumatic stress disorder (Graham-Bermann, Castor, Miller, & Howell, 2012; Rossman, Hughes, & Rosenberg, 2000) and childhood depression (Graham-Bermann, Gruber, Howell, & Girz, 2009). Individuals who experience IPV in childhood are also at risk for poorer mental and physical health in adulthood (Bair-Merritt, Blackstone, & Feudtner, 2006; Shaw & Krause, 2002) and are more likely to become involved in violent relationships themselves (Cisler et al., 2012; Lansford et al., 2007; Whitfield, Anda, Dube, & Felitti, 2003). Taken together, the effects of exposure to IPV and corporal punishment are largely negative.
Women who experience IPV are at great risk for depression, posttraumatic stress, and high levels of parenting stress (Coker et al., 2002; Graham-Bermann & Miller-Graff, 2015; Laffaye, Kennedy, & Stein, 2003; Taylor, Guterman, Lee, & Rathouz, 2009), all of which have been linked to higher levels of harsh/intrusive parenting, corporal punishment, and maltreatment (Gage & Silvestre, 2010; Gustafsson, Cox, & Blair, 2012; Renner, 2009; Taylor et al., 2009). Given these findings, it is necessary to identify ways to intervene not only to reduce children’s exposure to IPV but also to decrease the use of corporal punishment within those families. However, to date there have been very few studies of parenting interventions to reduce the use of physical punishment among families exposed to IPV.
One such intervention study that did examine parenting and punishment presented research findings on the negative effects of physical punishment on child behavior among parents of preschool- and school-age children. Holden, Brown, Baldwin, and Caderao (2014) found that the intervention decreased positive attitudes toward spanking for 47% of their sample. Although these findings are informative, this study is limited in that parents were university-educated (Holden et al., 2014); In addition, it is unclear whether the changes made due to the intervention persisted for any length of time. Another brief intervention to change attitudes toward corporal punishment used an interactive program that demonstrated alternative discipline strategies and gave a rationale against using physical punishment (Chavis et al., 2013). This intervention was delivered to English- and Spanish-speaking parents of children aged 6 to 24 months. Post-intervention, it was found that parents in the treatment condition were less likely to report having used spanking as a form of discipline in a hypothetical example of child misbehavior and had less positive attitudes toward spanking when compared with a control group (Chavis et al., 2013). Again, this study is limited in that it is unclear whether these attitude changes were maintained over time or resulted in reductions in actual use of spanking. Furthermore, as there were only post-intervention measures, it is difficult to know whether the changes made were due to the intervention itself. Another study examined attitudes toward spanking before and after a brief intervention and found that parents who participated in the intervention changed their attitudes toward the use of spanking such that they reported that they would be less likely to use spanking post-treatment (Scholer, Hamilton, Johnson, & Scott, 2010). This shift in attitudes did not occur for the control group (Scholer et al., 2010). Although these effects persisted 4 months post-intervention, this study is again limited as only attitudes toward spanking were measured, not the actual rates of spanking. Furthermore, these intervention studies do not evaluate intervention effects in an IPV-exposed population, which is a population that may be at high risk for using corporal punishment as they are under significant amounts of stress. Thus, more work is needed to evaluate the effectiveness of interventions, both in the immediate and long term, for caregivers who are exposed to stressors, such as IPV.
Preschool-aged children living in homes where IPV occurs are at great risk for exposure to corporal punishment, which may only serve to increase their risk for experiencing maladaptive outcomes, such as delinquent behavior and poor mental health (Gershoff, 2002; Taylor et al., 2010; Zolotor et al., 2011). Thus, it is critically important to intervene with the caregivers of young, IPV-exposed children in order to reduce the use of corporal punishment. To date, there has been little research on the impact of intervention on the rates of corporal punishment, particularly over time, and no research with IPV-exposed populations.
The Moms’ Empowerment Program (MEP; Graham-Bermann, 2012) is a group-based, 10-session intervention for mothers who have experienced IPV. The MEP endeavors to build self-esteem and reduce distress by providing violence-exposed mothers resources and support. In addition, this program seeks to augment parenting skills to reduce stress within the mother–child relationship. Research has demonstrated that the MEP reduces depressed mood and posttraumatic stress over the course of the 10 sessions, with this effect stable at 6 months post-intervention (Graham-Bermann & Miller-Graff, 2013; Graham-Bermann & Miller-Graff, 2015). The MEP was designed to be implemented in community settings in conjunction with a program designed for children (either the Kids’ Club or Preschool Kids’ Club [PKC]). The MEP is specifically designed to target parenting behaviors of caregivers who are experiencing IPV; thus, it provides a unique opportunity to evaluate the effectiveness of intervention on corporal punishment use in this high-risk population.
The PKC (Graham-Bermann, 2000) is a 10-session intervention for children ages 4 to 6 years who have been exposed to IPV. The PKC was developmentally adapted from the Kids’ Club program (for children ages 7-12 years; Graham-Bermann, 1992), which aims to reduce distress associated with exposure to violence by identifying feelings about violence and teaching coping skills for dealing with such feelings. In addition, the program aims to help children appropriately assess responsibility for violence (i.e., that they are not responsible for violence between their parents/caregivers) as well as give alternative strategies for managing conflict. This program, in conjunction with the MEP, has been shown to reduce behavior problems in children as well as change attitudes about violence, with stable effects up to 6 months post-intervention (Graham-Bermann, Howell, Lilly, & Devoe, 2011; Graham-Bermann et al., 2007; Graham-Bermann, Miller-Graff, Howell, & Grogan-Kaylor, 2015).
The Present Study
The present study provides an evaluation of parenting practices, specifically focused on the use of corporal punishment, before and after the implementation of the MEP. This study seeks to build upon existing literature by providing information on the long-term effects of a parenting intervention on disciplinary practices. Furthermore, this study explores the use of corporal punishment in an IPV-exposed population. Our hypothesis was that participation in the MEP would reduce the use of corporal punishment by the mothers.
Method
Sample
The sample consisted of 113 mother–child pairs from two counties in Southeast Michigan and Southern Ontario, Canada. All families were exposed to significant IPV in the past 2 years. Fifty-three percent of participating children were boys (47% girls) ranging in age from 4 to 6 years (M = 4.93, SD = .86). Gender in the experimental (treatment) group was split evenly, with 29 females and 29 males. There were 28 females and 34 males in the comparison group. Child ethnicity was diverse (38% Caucasian, 37% African American, 20% Biracial, 5% Latino/a), as was the mother’s ethnicity (48% Caucasian, 37% African American, 8% Biracial, 6% Latino/a, 1% from other ethnic groups). The mothers’ mean age was 31.78 years (SD = 7.37), and the families’ average monthly income was low, but variable (M = US$1,414; SD = US$1,549).
Of the women participating in this study, 11% had some high school education, 28% graduated from high school, 39% had a college degree or additional technical training, and 2% obtained a graduate degree. Forty-three percent of women reported that they were single, 7% were living with a partner, 16% were married, and 34% were separated or divorced. Seven percent of the women were living with a violent partner at the time of assessment, while the rest were not. Fifty-two percent of the sample had previously lived in, or were currently living in, a shelter for families exposed to violence, while the rest were not. Demographic statistics for the sample are provided in Table 1.
Descriptive Statistics.

Note. CTS2 = Revised Conflict Tactics Scales; APQ = Alabama Parenting Questionnaire; GED = General Educational Development.
Research Design and Procedures
Following institutional review board approval, participants were recruited through local domestic violence shelters as well as through flyers and brochures posted in local community businesses and clinics. Participants were recruited in Washtenaw County and Jackson County in Michigan and from Windsor, Ontario, Canada. There were no significant demographic differences between locations for mother’s relationship status, age, or household income, nor for her child’s sex or age. Furthermore, assignment to the treatment or comparison conditions did not differ significantly based on location.
Those interested in joining the study called a toll-free number and completed a brief telephone screen to determine their eligibility. Women were able to participate if they had a child in the target age range (4-6 years old) and had experienced IPV in the past 2 years. Study participants were randomly assigned to either a treatment group or a wait-listed comparison group using a block design, meaning that the first five mother–child dyads were assigned to the treatment condition, then the next five mother–child dyads were assigned to the comparison condition, and so on.
Once enrolled in the treatment condition, mothers and children attended biweekly sessions for 5 weeks. Mothers and children met in separate groups, with about 4 to 6 mothers participating in each group. The MEP addresses parenting as a consistent program theme. Parenting particularly emerges in the second session under the theme “parenting under stress.” In this session, group therapists work with mothers to identify how stress affects their ability to parent, explicitly focusing on the relationship between IPV and parenting. Mothers discuss their fears, worries, and hopes about parenting. In the following session, therapists help mothers to identify the effects of IPV exposure on early child development. The core of the intervention around corporal punishment is introduced in the sixth session, where therapists ask women to review their current parenting practices, disciplinary challenges, and then work with the women to replace negative and harsh/intrusive practices with positive parenting practices and non-corporal discipline, such as time-out.
Families assigned to the control condition were invited to participate in the intervention at the end of 5 weeks. All study participants were interviewed at baseline (pre-test), after 5 weeks (post-test), and at a 6- to 8-month follow-up. Eight families from the comparison group chose to participate in the intervention after the post-test. The treatment and comparison groups did not differ significantly at baseline in terms of violence severity and demographic variables. Interviewers were graduate and undergraduate research assistants trained in research ethics and interview methods with at-risk populations.
Attrition Analysis
Families allocated to the intervention program attended an average of 6 sessions (SD = 3). Of the 58 mother–child dyads assigned to this experimental condition, 51 participated in the intervention and 7 did not due to illness, work interference, and other personal commitments. In all, 50 completed both baseline and post-intervention assessments. One family moved and could not be located for the second interview. There were 62 mother–child dyads assigned to the comparison group. Of these, eight could not be contacted for the second interview, and four discontinued their participation in the study. Thus, attrition was 14% for the treatment group and 21% for the comparison group. There was further attrition, from the second interview to the follow-up assessment 8 months later (28% experimental group and 29% comparison group attrition). When compared with those who dropped out of the study at the time of the second interview, analyses indicated no significant difference between groups on any study variables. Therefore, change over time cannot be linked to variance in participant groups due to attrition.
In their interviews, mothers provided demographic information about themselves and their child, including race, relationship status, education, and income. Mothers also reported on their IPV history over the past 2 years, their parenting practices, their mental health, and their child’s mental health. Mothers’ interviews lasted approximately 60 to 90 min, and they received $25 for each interview.
Measures
Exposure to IPV
The Revised Conflict Tactics Scales (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) is a 78-item instrument that measures the severity of IPV, including psychological aggression, physical assault, sexual coercion, and injury, as well the use of negotiation to manage conflict. Items evaluate both violence perpetration and victimization. In deference to the request of participating agencies, only the 39 questions related to partner violence toward the woman were included in the study. Using a 7-point scale (from never occurred to occurred more than 20 times), mothers were asked to estimate the frequency with which they experienced those conflict tactics from a partner in the past year. Internal reliability of the original CTS2 scale is strong with coefficients (α) ranging from .79 to .95. Construct and discriminant validity have also been demonstrated (Straus et al., 1996). Present study reliabilities were (α) .93 for the Total Scale, .84 for Psychological Aggression, .84 for Physical Assault, .87 for Sexual Coercion, and .69 for Injury.
Maternal use of corporal punishment was assessed via in-person interviews of the mothers using the Alabama Parenting Questionnaire (APQ; Frick, Christian, & Wootton, 1999). The APQ consists of 42 items measuring positive and negative parenting practices in six domains, one of which is the use of corporal punishment toward the child. Mothers rated the frequency with which they employed these parenting practices on a 5-point scale ranging from 1 (never) to 5 (always). The APQ has been used successfully in studies of the parenting of preschool-age children, with evidence of sound psychometric properties (Clerkin, Marks, Policaro, & Halperin, 2007). The corporal punishment domain used for the present study analyses includes three questions. These items are “You spank your child with your hand when she/he has done something wrong”; “You slap your child when he/she has done something wrong”; and “You hit your child with a belt, switch or other object when she/he has done something wrong.”
Analytic Plan
Participants were assessed at three time points: pre-test, post-test, and follow-up. Data were structured as repeated measures data, also known as panel data. Observations on the same participant at pre-test and post-test were correlated. A model that failed to account for the correlated nature of these repeated measures data would run the risk of biased standard errors (Singer & Willett, 2003). In particular, in some cases, standard errors might be underestimated which could result in underestimated p values. These underestimated p values could lead to misattributions of statistical significance (i.e., false positives) when such an attribution was in fact not merited. Thus, the analyses employed in this study made use of multilevel models for longitudinal data (Raudenbush & Bryk, 2002). In the present study analysis, the model was essentially:

Here, yit was the outcome variable for individual i, as assessed at time t; β0 was an intercept term; g represented group membership (1 = treatment; 0 = comparison) and β g was the associated regression parameter; t was a measure of time (1, 2, or 3) which was treated as an indicator variable, with Time 1 as the reference category, in order to capture non-linear changes in the time trajectory. Thus, βt2 and βt3 represented changes in the time trajectory at Time 2 or Time 3. g × t was an interaction of group membership with time and represented the association of group membership with changes in the slope of the time trajectory; βgt2 and βgt3 were thus the regression parameters assessing the size of the g × t effect at Time 2 or Time 3. a and s were variables for age and sex of child study participants. ui was a component of the error term unique to each individual i, while eit was the occasion-specific error term for individual i at time t.
Results
Descriptive Statistics
Due to missing data on some variables, seven participants were removed from the data analysis, which resulted in a final study sample of 113 mothers. Mothers in this sample were exposed to a high level of violence, including an average of 95.98 incidents of psychological violence, 54.62 incidents of physical violence, and 25.74 incidents of sexual violence over the past year.
Multivariate Results From Multilevel Model
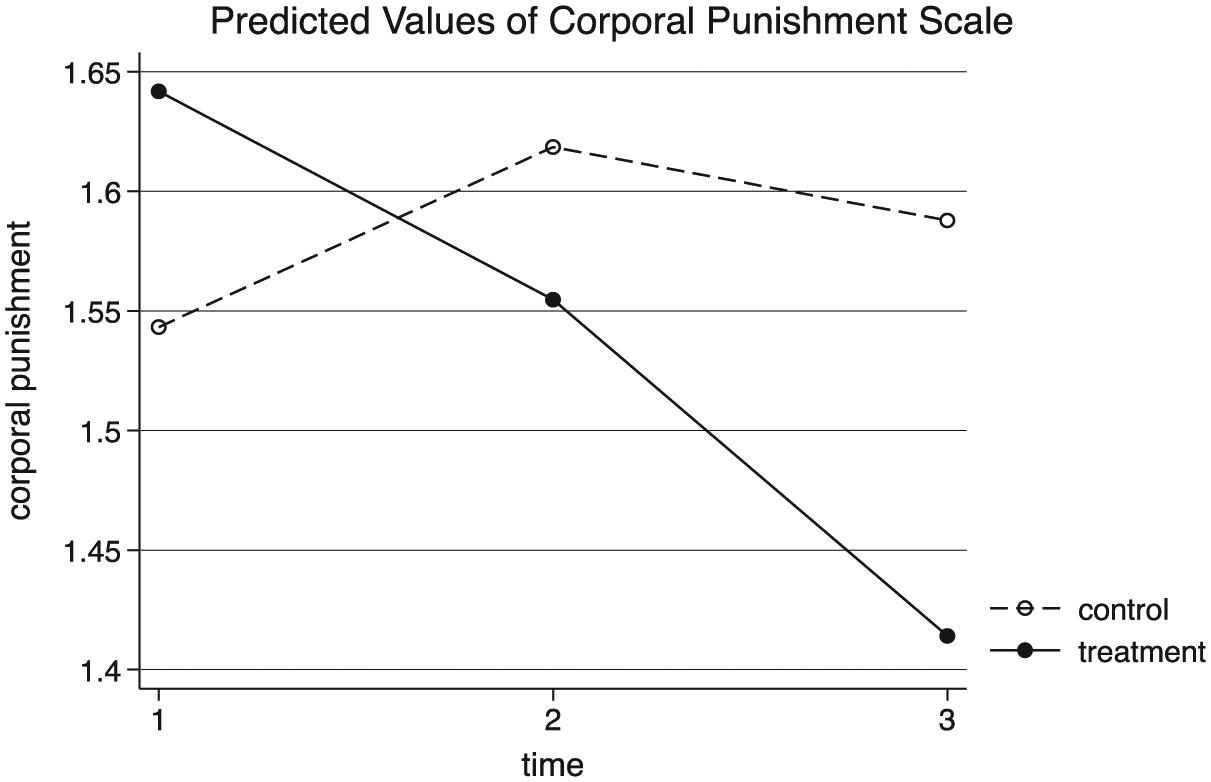
For the treatment group, both of the interactions βgt2 and βgt3 were statistically significant, indicating that membership in the treatment group was associated with a more sharply decreasing slope on the trajectory of maternal use of corporal punishment than for members of the comparison group. For the comparison group, results of the multilevel model (Table 2) indicated that neither of the indicator variables for time were statistically significant, suggesting that members of the comparison group did not experience changes in maternal use of corporal punishment over the course of the intervention. Increases in child age were associated with decreased maternal use of corporal punishment. Child sex was not associated with differences in the use of corporal punishment. A likelihood ratio test (p < .001) suggested that the model was a statistically significant improvement over an ordinary least squares regression model that did not account for the nested nature of these data. Figure 1 provides a graphical interpretation of the results of the multilevel model.
Results From Multilevel Model Examining Use of Corporal Punishment.

Results of multilevel model.
Discussion
This study provided results from a trial of the MEP for mothers exposed to IPV. Results suggested that program participation resulted in a reduction of mothers’ usage of corporal punishment practices, including spanking, slapping, and hitting the child with an object. These reductions were apparent immediately following the intervention and months later at the follow-up assessment. Study results are particularly robust for the post-intervention assessment, as up to that point fidelity in random assignment was maintained. We know that eight participants in the comparison group chose to participate in the intervention after the administration of the post-test. Thus, our assessment of Time 3, which is independent of our assessment of Time 2, cannot be said to be strictly random. However, we believe that participation of only a few members of the comparison group in the intervention would not attenuate the size of any coefficients measuring effects at Time 3. Thus, we believe it is plausible that our regression coefficients for Time 3 may underestimate the gains evident at follow-up.
Results also indicated that as children aged, they endured less corporal punishment. The finding that older children experience less corporal punishment is consistent with trends in corporal punishment use from nationally representative samples (Zolotor et al., 2011). This may be due to the fact that as children get older, they spend less time in close proximity to their mother, thus avoiding situations that may lead to physical punishment. As children age, parents also report a decreasing acceptability of spanking as an appropriate punishment (Flynn, 1998). Older children may also become more behaviorally and emotionally regulated and thus require less discipline than when they were younger.
Of note, no relationship was found between children’s gender and corporal punishment use. These results are consistent with other studies reporting no gender differences in the extent to which children receive physical punishment (Graham-Bermann et al., 2007; Holden, Coleman, & Schmidt, 1995; Regalado, Sareen, Inkelas, Wissow, & Halfon, 2004). Yet some older studies did find such a difference, with boys being the target of corporal punishment more often than girls (Day, Peterson, & McCracken, 1998; Giles-Sims, Straus, & Sugarman, 1995; Maccoby & Jacklin, 1974; Mahoney, Donnelly, Lewis, & Maynard, 2000; Rohner, Kean, & Cournoyer, 1991; Smith & Brooks-Gunn, 1997; Straus & Stewart, 1999). Important evidence also comes from a meta-analysis of physical punishment and child gender studies that showed no difference for boys and girls in both the United States and Canada (Lytton & Romney, 1991).
During the intervention, mothers had the opportunity to explore and process their own violence histories. Furthermore, many sessions focused on discussing general parenting practices and discipline strategies. During group sessions, mothers received resources about disciplinary techniques and also shared effective and ineffective strategies used with their children in the past. Furthermore, mothers were invited to try new parenting skills (such as using time-out as a discipline technique) and troubleshoot challenges they may have encountered in implementing such strategies with group therapists as well as other group members. More broadly, they were supported and reinforced in their efforts to change. This process may have increased understanding of the techniques as well as effectiveness of the techniques, ultimately increasing mothers’ buy-in of the strategies. As has been identified in other research, maternal self-efficacy regarding child discipline is related to a lower likelihood of using corporal punishment (Khoury-Kassabri, Attar-Schwartz, & Zur, 2014), which may explain why the effects of intervention were stable 6 to 8 months post-treatment.
Some research, particularly in developmental psychology, has raised the idea of “child effects” (Gershoff et al., 2010), namely that variations in parental use of corporal punishment may be responses to changes in children’s behavior. In general, research that has rigorously investigated this question, often using cross-lagged regression models (Gershoff, 2013), has found that parent effects on children are stronger than the effect of children’s behavior on parental behavior. That being said, we note that in this study, the randomized assignment that was part of the research design strengthens our inference that the treatment was responsible for changes in corporal punishment and minimizes the likelihood that child effects were involved.
Several studies have demonstrated a positive relationship between parenting stress and the use of corporal punishment (Khoury-Kassabri, Attar-Schwartz, & Zur, 2014; Liu & Wang, 2015), as well as a direct relationship between maternal depression and the use of corporal punishment (Eamon, 2001; Silverstein, Augustyn, Young, & Zuckerman, 2009). Although this evaluation of the MEP does not include assessments of parenting stress, the MEP has been shown to reduce mothers’ depression and posttraumatic stress (Graham-Bermann & Miller, 2013; Graham-Bermann & Miller-Graff, 2015). It is possible, therefore, that in addition to the direct effect of the program in teaching effective, non-corporal forms of child discipline, reductions in the use of corporal punishment over time may also have been promoted by decreases in maternal stress and improvement in maternal mental health. Future evaluations of this treatment paradigm should therefore consider parental stress as a mediator or moderator of treatment effects.
Limitations
This study provides valuable information on the immediate and long-term impact of intervention participation on parenting practices among women who experience IPV. There are, however, important limitations to consider when interpreting these results. First, potential issues of bias arise because mothers completed all study measures. This is especially pertinent to the research questions addressed here because women may have underreported their use of corporal punishment techniques due to social desirability concerns or fear of retribution. Furthermore, the measure of corporal punishment was fairly general and relatively short. Future studies should include a more comprehensive assessment tool, completed by multiple informants or through objective means, that offers more nuanced information about the types of physical punishment used in the home. In addition, this study only examined corporal parenting practices, without assessing other parenting techniques, parenting attitudes, or parenting efficacy.
The generalizability of study findings is also limited because participants were from a relatively small geographic region, typically low income, and solely female caregivers. In addition, all participants were treatment seeking, which may bias the sample toward women who were more open to change, thus exaggerating treatment effects.
There was some ethnic and racial diversity among study participants. The most predominant ethnic or racial groups in the study were African American and European American women. However, there were also some women who identified as Asian American, Biracial, and Latina. Due to the lower percentages of women indicating these identities, however, clearly more research is needed with women who identify as being part of one of these groups. There was some educational diversity in our sample; however, levels of education were generally low. We did not explore gender diversity among our participants as the focus of this intervention program was helping women who have been exposed to IPV. Finally, methodological concerns regarding sample retention, consistent group attendance, and the lack of a measure of treatment fidelity are relevant limitations to consider.
Clinical Implications
Results from the current study indicated that even in the context of exposure to severe violence, mothers are able to effectively learn and integrate new parenting skills and practices. Given that exposure to IPV already poses a serious risk to children’s health and development (Graham-Bermann et al., 2007, 2012, 2015; Kitzmann et al., 2003), preventing parental use of corporal punishment is an important family-level intervention to facilitate positive child development. It should be noted, however, that these interventions need to occur simultaneously with broader community and national policy change around the regulation of corporal punishment, as legal bans are strongly associated with decreases in the acceptability and use of such discipline tactics (Zolotor & Puzia, 2010).
Conclusion
Limitations notwithstanding, results of this analysis suggest that the MEP is an effective way to reduce use of corporal punishment in families with histories of exposure to IPV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Original funding for this project was received from the Blue Cross Blue Shield Foundation of Michigan.