
Abstract
Sexual harassment—unwanted sexual comments, advances, or behaviors—and sexual violence are still prevalent worldwide, leading to a variety of physical, cognitive, and emotional problems among those being harassed. In particular, youth in care are at risk of becoming perpetrators (and victims) of sexual harassment. However, in general, there are very few interventions targeting this at-risk group, and no such programs exist in the Netherlands. To this end, a group intervention program—Make a Move—targeting determinants of sexual harassment was developed. This program was implemented and evaluated among boys (N = 177) in Dutch residential youth care (20 institutions). A pre-test, post-test, and 6-month follow-up design including an intervention and a waiting list control group with randomized assignment of institutions (cluster randomized trial) was used to measure the effects of the intervention on determinants of sexual harassment. Multilevel (mixed) regression analysis with Bonferroni correction for multiple testing (α = .005) showed no significant effects of Make a Move on determinants of sexual harassment (ps > .03, Cohen’s ds < .44). Results are discussed in light of a three-way explanatory model focusing on intervention content, evaluation, and implementation as potential explanations for not finding any measurable intervention effects.
Introduction
Sexual harassment—in this article conceptualized as unwanted sexual comments, advances, or behaviors that cause harm to the victim—and sexual violence toward women are major problems worldwide. According to the World Health Organization, globally, 35.6% of women experience sexual violence at least once in their lifetime (World Health Organization, 2013). Although sexual harassment is more prevalent in less developed countries with higher gender inequalities (Agardh, Odberg-Pettersson, & Östergren, 2011; Devries et al., 2013; Peterman, Palermo, & Bredenkamp, 2011), Western countries also show worrisome rates. A surveillance study by the American Centers for Disease Control and Prevention (CDC), for example, showed that 10.4% of American high school students (girls but also boys) who had been out with or dated someone in the previous year had been the victim of some type of sexual harassment in the 12 months preceding the survey (CDC, 2014). In a recent British study, on average, 45% of 13- and 14-year-old girls and boys reported having been a victim of sexual harassment by someone they had ever dated or been with in a relationship. The authors reported that emotional abuse and controlling behaviors (38%), physical abuse (17%), and sexual victimization (14%) were the three most reported types of harassment (Fox, Corr, Gadd, & Butler, 2014). Moreover, Dutch studies suggest that 4% to 23% of boys and 18% to 36% of girls have experienced some form of physically violent sexual behavior (de Bruijn, Burrie, & van Wel, 2006; H. de Graaf, Meijer, Poelman, & Vanwesenbeeck, 2005; Dukers-Muijrers, Somers, de Graaf, Meijer, & Hoebe, 2015). The experience of sexual harassment can lead to a variety of physical, cognitive, and emotional problems, such as post-traumatic stress disorder (PTSD), substance abuse, depression, and anxiety (Holmes & Sher, 2013; Kilpatrick et al., 2000, 2003; Van Berlo & Mooren, 2009), and as such, there is a strong need for prevention efforts. Furthermore, adolescence is an important period in terms of developing (healthy) sexual attitudes and behaviors, a further reason why interventions targeted at this particular group may help to prevent these individuals from becoming perpetrators of sexual harassment (Foshee, Benefield, Ennett, Bauman, & Suchindran, 2004; White & Smith, 2004).
Understanding the factors that are linked to an individual becoming or being a perpetrator of sexual harassment is important for designing prevention programs (Bartholomew, Parcel, Kok, Gottlieb, & Fernández, 2011). Meta-analyses and other reports on prevalence rates show that the vast majority of perpetrators of sexual harassment are male, and a significant proportion of them are underage (Barbaree & Marshall, 2006; Fago, 2003; Hall & Barongan, 1997). Psychiatric and personality disorders have also been identified as determinants of sexual harassment behaviors (Kafka & Hennen, 2002; Zakireh, Ronis, & Knight, 2008). Furthermore, growing up in an unstable social environment with severe disturbances and having been the victim of or exposed to sexual and/or physical and emotional abuse during childhood are factors that have been associated with sexual harassers (Abbey, McAuslan, Zawacki, Clinton, & Buck, 2001; Barbaree & Marshall, 2006; Burton, Miller, & Shill, 2002; de Bruijn et al., 2006; Salter et al., 2003; Wekerle et al., 2009; Wolfe, Wekerle, Scott, Straatman, & Grasley, 2004). Other studies have shown that perpetrators of sexual harassment generally have an earlier sexual debut and a greater number of sex partners as compared with their non-offending peers (Abbey et al., 2001; Barbaree & Marshall, 2006; Wekerle et al., 2009). Wolfe et al. (2004) found that childhood maltreatment significantly contributed to trauma symptoms, attitudes justifying dating violence, and actual dating violence. Furthermore, some studies have reported a relationship between committing acts of sexual harassment and having friends who approve of forced sex (Abbey et al., 2001; de Bruijn et al., 2006).
The findings described above suggest that, in particular, youth in residential care (youth in 24-hr group living facilities that are not licensed as hospitals or youth correctional institutions and offer—mental health—care for children and adolescents with serious emotional and/or behavioral problems, including law violations) are highly vulnerable in terms of involvement in sexual harassment and violence, both as a victim and/or a perpetrator, as these adolescents often have behavioral and emotional disturbances (Connor, Doerfler, Toscano, Volungis, & Steingard, 2004; Jonson-Reid, Scott, McMillen, & Edmond, 2007). In addition, studies show that many of these individuals have grown up with emotional, sexual, and/or physical abuse or neglect, and have witnessed domestic violence or have substance abusing parents (Connor et al., 2004). Besides the behavioral and emotional problems of these boys, the atmosphere in the group homes might contribute to developing positive attitudes toward deviant sexual behavior (Murnen, 2000). Group homes, particularly male-only homes, typically have a macho culture, sometimes referred to as an atmosphere of hyper-masculinity (Colton, 2002; Gault, 2012). Sexual aggression, being related to social recognition and power struggles, often defines manhood in such group settings (Murnen, 2000). Furthermore, bullying (both with and without sexual overtones) is an everyday practice in adolescent residential care groups (Gruber & Fineran, 2008; Sekol, 2013; Sekol & Farrington, 2009; Smith, 2006). Together, the experiences boys have gone through at home and their living conditions in youth care make boys in residential youth care a specific risk group for perpetrating (as well as becoming a victim of) sexual harassment and sexual violence (Boendermaker, van Rooijen, Berg, & Bartelink, 2013; Colton, 2002).
Over the years, many sexual harassment prevention programs have been developed to empower women and men against sexual victimization and to prevent potential perpetrators from sexually harassing others (see, for example, I. de Graaf, de Haas, Zaagsma, & Wijsen, 2016; DeGue et al., 2014; De Koker, Mathews, Zuch, Bastien, & Mason-Jones, 2014; Taylor, Stein, Mumford, & Woods, 2013). However, evidence regarding the effectiveness of these programs is not straightforward, as the interventions differ along multiple dimensions such as intervention goals, methods, settings, design, and target groups, making it difficult to draw general conclusions. In addition, interventions specifically directed at young people who are at risk for sexual harassment perpetration (such as those in youth in care) are scarce (Antle, Sullivan, Dryden, Karam, & Barbee, 2011; Ball et al., 2012).
To our knowledge, only two interventions have targeted at-risk youth in care-related settings (Ball, Kerig, & Rosenbluth, 2009; Wolfe et al., 2003), and none has been implemented in the Netherlands. Ball and colleagues’ Expect Respect dating violence prevention program for pupils who have experienced domestic violence or sexual abuse in the United States showed improved communication skills as well as anger control, knowledge of healthy relationships, and awareness of abusive behaviors (Ball et al., 2009). Wolfe and colleagues (2003) evaluated a Canadian teen dating violence prevention program targeting adolescents who were recruited through Child Protection Services. Participants showed decreased emotional distress and reduced incidence of both physical and emotional abuse after participating in the program. Veerman and van Yperen (2007) pointed to the difficulties of performing a randomized controlled trial (RCT) in youth care practices. These difficulties, alongside possible ethical considerations, may contribute to the lack of intervention evaluations found in scientific literature for this target group.
In response to the need for a sexual harassment prevention program specifically targeting at-risk boys in Dutch youth care, the Dutch organization Rutgers—Center for Sexual and Reproductive Health and Rights—developed an intervention called Make a Move. This intervention was designed to be delivered in a group setting using groups of six to eight boys. In the Netherlands, youth care services include ambulant care, placement in foster care or residential care (group homes), residential care with a specific focus on mental health services or disabilities, and youth correctional institutions. Make a Move targets boys in regular residential care. Residential youth care institutions (group homes) accommodate around 12,000 boys and girls on an annual basis (Boendermaker et al., 2013). Children may be placed in residential care if their parents are unable to take care of their children and if other forms of (ambulant) youth care prove insufficient. This can be the case if the child has severe emotional or behavioral problems, or when family circumstances prevent parents from taking care of their children. Placement can be either on a voluntary basis or a juridical measure although residential care should not be mistaken for youth correctional institutes. The main purposes of a placement vary as these are very personal, but usually, the main aim is to facilitate a safe place to grow up combined with family and/or individual interventions (Boendermaker et al., 2013). In most cases, the child and staff together work toward either moving back to living with their family or other relatives or train self-reliance in preparation for (assisted) independent living. The average length of stay has in recent years decreased from 24 months to approximately 11 months (Boendermaker et al., 2013).
Make a Move was implemented by freelance trainers working for Rutgers. The main goal of Make a Move is to promote respectful (sexual) relationships and to prevent sexual harassment. Subgoals include, for example, increasing awareness of differences in relationship expectations and teaching the boys how to control their wishes and desires if they are not in line with their partners’ wishes. Make a Move intends to be a prevention program, not a treatment program. Make a Move has a cognitive-behavioral approach and addresses determinants related to sexual harassment such as attitudes and social-relational skills. As part of a trial implementation of the program, an effect and process evaluation was performed to assess the effectiveness of Make a Move in influencing determinants of sexual harassment. Outcome measures were based on the objectives of the program and taken from previous studies exploring determinants of sexual harassment. Previously identified determinants include gender attitudes (Abbey et al., 2001; McCauley et al., 2013), adverse sexual beliefs, attitudes about gender roles, acceptance of verbal pressure in obtaining sex (Abbey et al., 2001), rape myth acceptance, acceptance of interpersonal violence, adverse sexual beliefs, rape empathy, and self-efficacy (O’Donohue, Yeater, & Fanetti, 2003). This article describes the effect evaluation of a trial implementation of Make a Move in Dutch residential youth care. The process evaluation is described elsewhere (van Lieshout, Mevissen, Jonker, & Ruiter, in press).
Method
Recruitment, Randomization, and Study Design
All (n = 49) Dutch youth care institutions that offer residential care to boys aged 12 to 18 were contacted by email and telephone and were invited to participate (with one or more groups of boys) in the trial implementation of Make a Move. Twenty (40.8%) institutions agreed to participate in the pilot; the remaining 29 (59.2%) institutions had no interest in participating at that moment. Reasons mentioned for non-participation varied and ranged from already partaking in another research project, lack of time, to mainly taking care of girls at that time. To prevent large baseline differences with regard to background characteristics between the intervention and control groups, institutions were matched in pairs based on characteristics such as geographical setting, type of care offered, and number of participating groups of boys within the institutions. Within each matching pair, one institution was randomly assigned to the intervention condition (the Make a Move program) and the other was assigned to the waiting list control condition (no prevention program). In the end, each treatment condition included 10 institutions. The effectiveness of the Make a Move program in changing determinants of sexual harassment was evaluated using a baseline measure (T0), a direct post measure (T1), and a 6-month follow-up (T2). See figure 1 for the timeline.
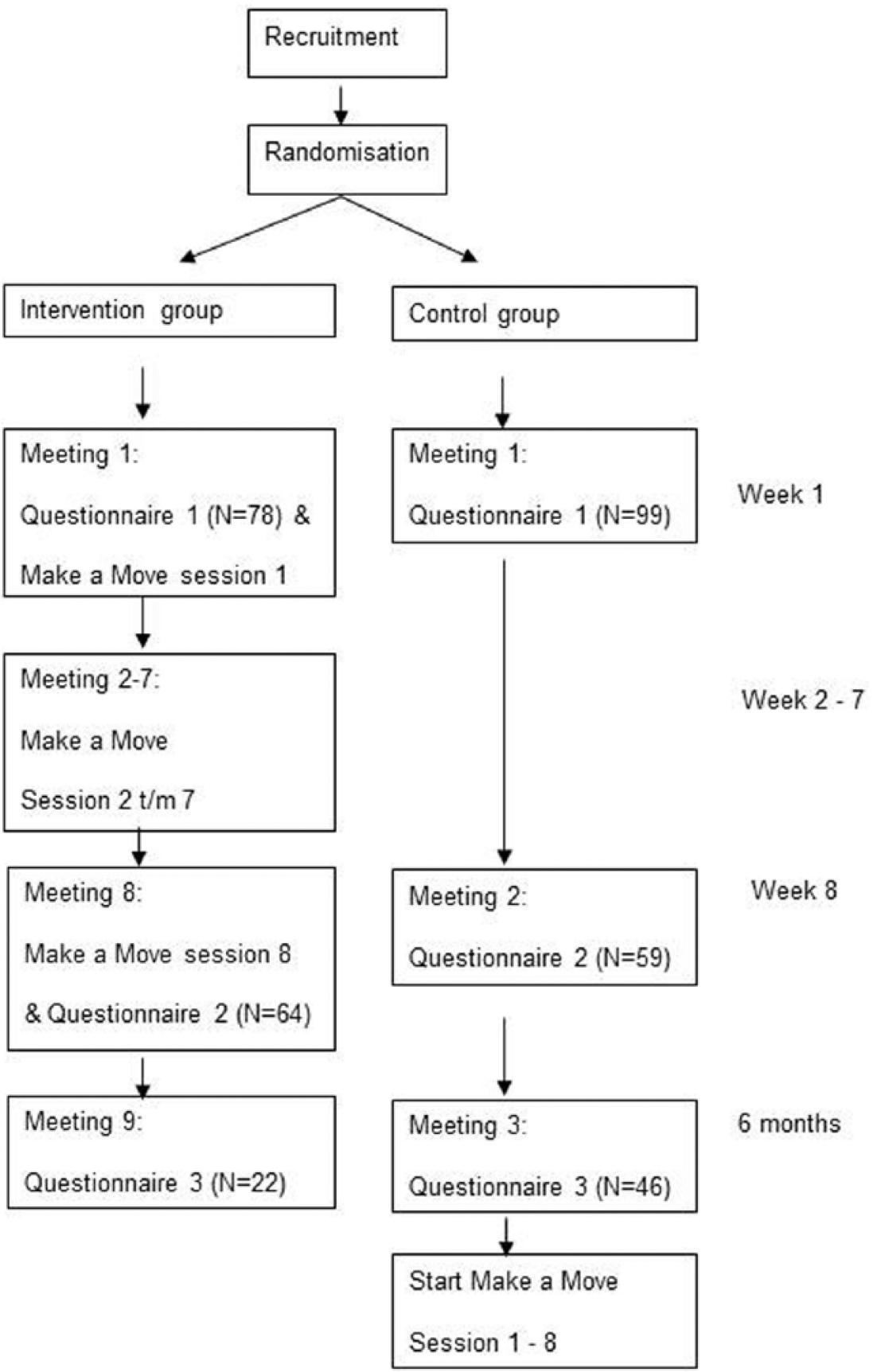
Timeline Make a Move trial implementation.
The 20 participating institutions were requested to form one to three groups of boys, each consisting of six to eight boys aged 12 to 17 years. Important exclusion criteria for participation were as follows: having severe autism spectrum disorders (ASD), being unable to function in group meetings (e.g., due to aggression regulation problems), having an IQ level below 80, and being known by the institution to suffer from post-traumatic stress due to sexual abuse or to have been convicted as a perpetrator of sexual assault. The reason for the latter exclusion criterion is that Make a Move is a preventive program, not a treatment component. In addition, at the start of the program, boys had to have a remaining stay of at least 8 months within the institution to be able to finish the full program including the follow-up survey. In the end, 29 groups were formed (14 in the intervention condition, 15 in the control condition) with number of groups per institution ranging from one to three. The number of boys per group at the start of the program ranged from three to nine.
At baseline, 177 boys (44% in the intervention group) started the pilot and filled out the first questionnaire (T0). Following baseline, 139 boys (46% in the intervention group) completed the direct post measure (T1), and 68 (32.4% in the intervention group) completed the 6-month follow-up (T2). Individual time measures were matched on date of birth and mother’s initials. Not all boys consistently filled out the matching criteria. Matching of all three questionnaires was possible for 63 boys while matching of two questionnaires was possible for 64 boys (59 for T0 and T1, one for T0 and T2, and four based on T1 and T2).
Participants
With regard to the 177 boys starting the pilot at T0, mean age 14.8 years (SD = 1.64, range = 12-18 years). The majority were of Dutch origin (61.6%). A few participants had a (partly) Antillean-Surinam (10.7%), or Turkish or Moroccan (5.1%) background, and the remaining boys (22.6%) were from a very diverse range of (non-)Western backgrounds. Most boys (53.4%) had no religious orientation. Of the remaining boys, 27.6% had a Christian orientation (Catholic, Protestant, or similar), 7.5% an Islamic, and 11.5% another sometimes unclearly defined orientation (Agnostic, God, or an “I don’t know” response). The educational level of most boys (95.5%) did not exceed lower vocational education, which is the lowest level of secondary education in the Netherlands.
Of these 177 boys, most (71%) had had sexual intercourse, and 19% reported having had sexual experience without intercourse (i.e., touching, oral sex). Age at first intercourse ranged from 6 to 17 years old (M = 13.3, SD = 1.85, median 13 years old). Reported number of sexual partners ranged from 1 to 30 (median = 5). Ninety-two percent had had a relationship in the past 2 years. Regarding reported sexual harassment behaviors, 40.9% reported to have sometimes or regularly tried to persuade somebody into having sex and 23.8% had sometimes or regularly taken advantage of another person’s drunkenness to get sex, 23.5% had sometimes or regularly used nagging to get sex, and 17.2% had sometimes or regularly lied to get sex. One in 10 (9.7%) had sometimes or regularly become angry towards a partner, 4.0% had sometimes or regularly used violence, and 4.0% had sometimes or regularly threatened their partner with violence to get sex.
Procedure
All participating institutions received an informed consent form to sign. In addition, they received a letter that they were asked to use to inform parents or legal guardians about Make a Move, which included information about the option to withdraw the child by requesting an objection form (i.e., passive consent). No requests were received for an objection form. After the institutional consent forms had been returned, all participating boys received the first questionnaire, which included information about the research, their privacy, and the fact that that they could withdraw at any time, as well as instructions on how to fill out the questionnaire. Their consent was given by ticking the box indicating that they understood and agreed with the terms of agreement. Prior to the start of the intervention groups, the contact persons of the institutions were asked to invite the potential participating boys for a brief introduction talk with the aim to inform and motivate them to participate. After the baseline measurement was completed, seven schooled trainers from Rutgers (one male, six female, aged 51-58, M = 54.6), often assisted by an employee from the youth care institution, delivered the Make a Move program to boys in the intervention group, during eight group meetings over a time period of about 8 weeks. Some trainers visited several institutions, and some institutions were visited by several trainers. Within institutions, visiting trainers were not always consistently assisted by one and the same youth care employee. No group meetings were organized for the boys in the control group during those 8 weeks. At the end of the last Make a Move meeting (intervention group) or eight weeks after T0 (control group), the boys were asked to fill out the post-test survey (T1). The T0 and T1 surveys were filled in during a group meeting under the supervision of a trainer (intervention group) or a researcher (control group) to assure a quiet and private surrounding for the boys and in case the boys needed help with the survey. For the 6-month follow-up (T2), all institutions were contacted by phone to make arrangements for administering the 6-month follow-up questionnaires to the boys. As most boys had by then left the institutes, T2 was not administered in a similar group setting as T0 and T1. Instead, institutes were requested to forward the questionnaires to the boys who had left the institute. After the T2 measurement, waiting list control group institutions were assigned a trainer and also received the intervention.
Make a Move Program
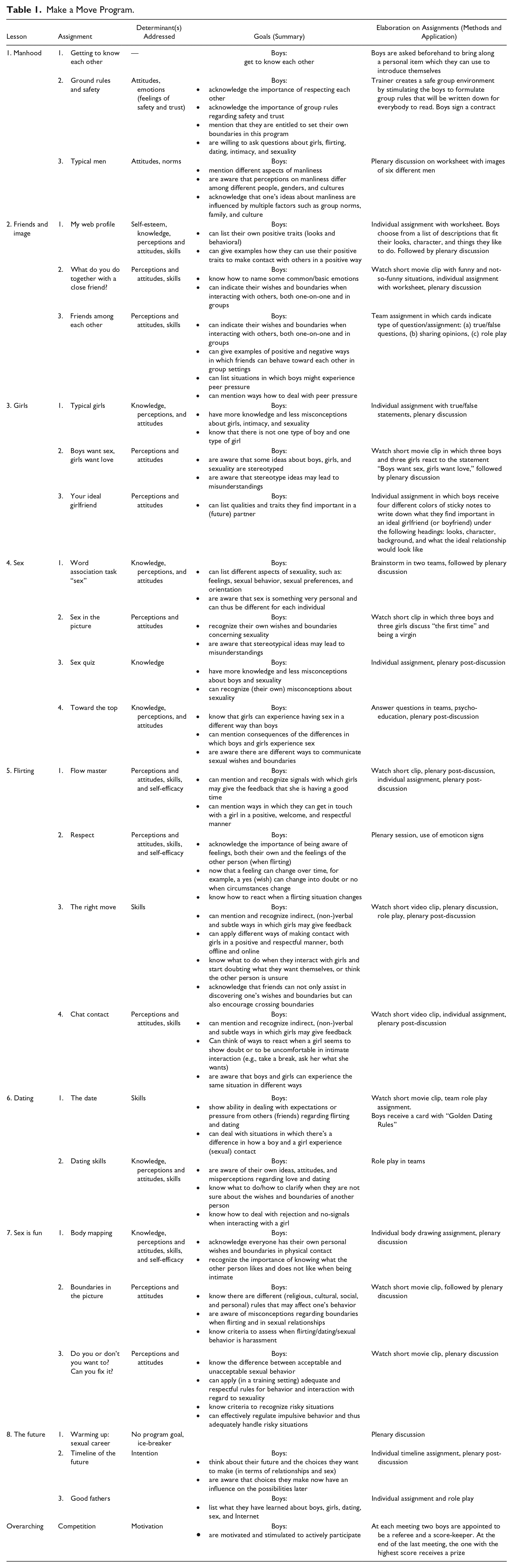
Make a Move is a group intervention for boys aged 12 to 17 years about sexuality and relationships, designed to prevent sexual harassment and dating violence. The program consists of eight weekly meetings of 90 min each. The themes covered by the eight meetings are, in order, men, image, girls, sex, flirting, dating, pleasurable sex, and the future. Each meeting includes several exercises such as role play, discussion, and watching short movie clips. See Table 1 for an overview of the content of the program. A competitive element runs through the program. Boys can earn credits for doing the exercises as well as for active participation and good manners, both individually and as a group. At each meeting, a new score-keeper is appointed among the boys, and the final winner receives an incentive. This competitive element of the intervention was added after a pre-test of the program, to increase the boys’ engagement in the tasks.
Make a Move Program.
Measures
The questionnaire included measures on background characteristics: age, ethnicity, religion, educational level (very low, low, high, unknown), sexual history (relationship experience over the past 2 years; yes vs. no), sexual experience with and without penetration (yes vs. no), age at first time sex, lifetime number of sex partners, and sexual harassment behaviors such as “have you ever tried to persuade somebody into having sex?” (never, sometimes, regularly, very often). This last response scale was recoded into three response categories: never, sometimes, and regularly/very often.
In addition, the questionnaire included six validated scales previously used in empirical research to measure antecedents of sexually offensive behavior, as well as eight measures based on elements taken from the Reasoned Action Approach (Fishbein & Ajzen, 2010) that were adapted to the outcome goals of the intervention. From the six validated scales, we selected a subset of items with the highest inter-item correlations, to keep the survey short and maximize the chance that the boys would be able to concentrate on it. All psycho-social measures used 7-point Likert-type scales. Higher scores indicate more of that attribute. We calculated mean scores for scales at each time point for a participant only if more than half of the items that made up one measure had been answered. The outcome measures and their mean scores are showed in Table 2.
Mean Scores (SD) on All 14 Outcome Measures for Each of the Three Measurements.
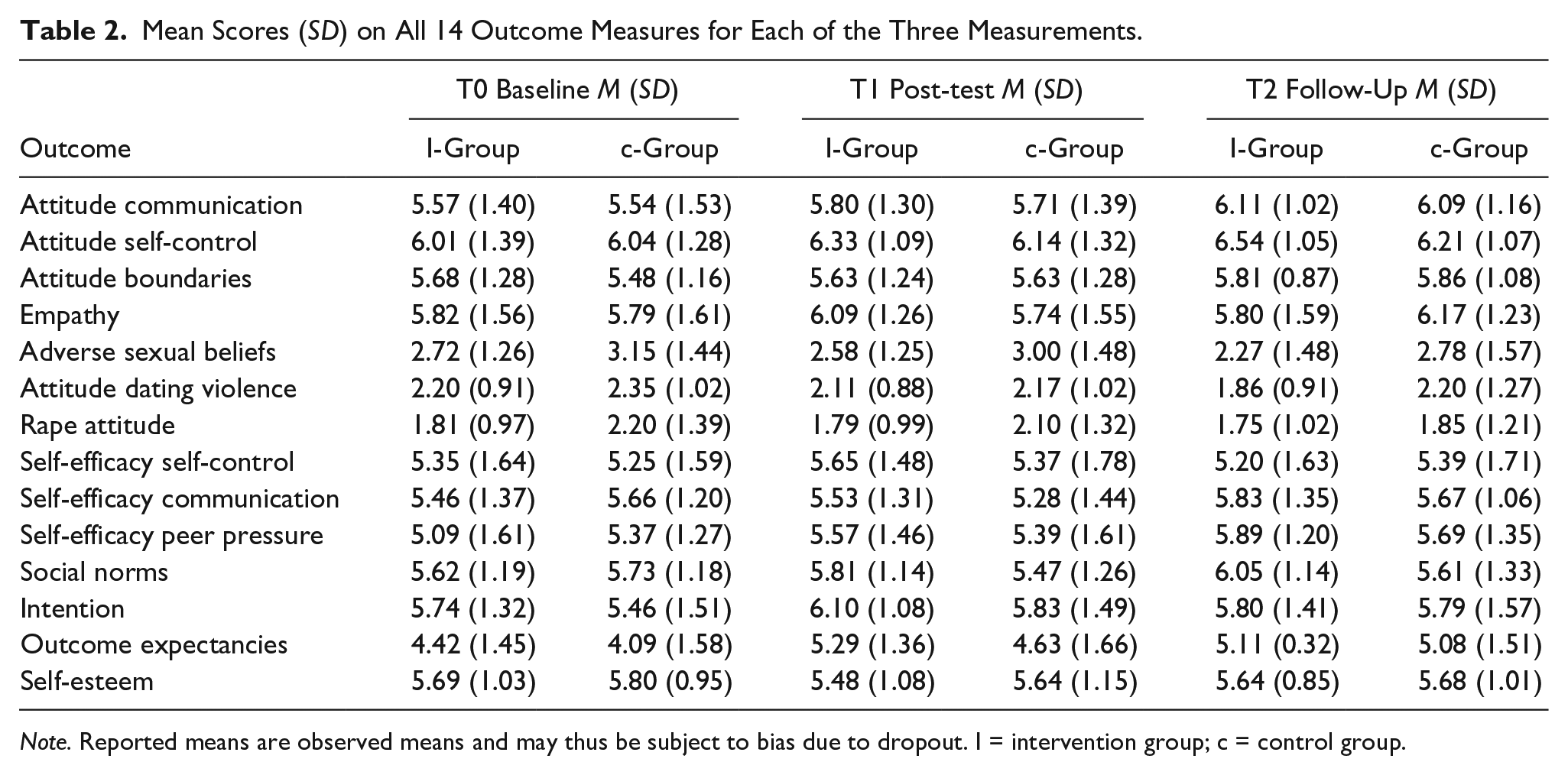
Note. Reported means are observed means and may thus be subject to bias due to dropout. I = intervention group; c = control group.
Self-esteem was measured with five items (α = .64) taken from Heatherton and Polivy (1991), for example, “I am confident about my talents” (1 = totally disagree, 7 = totally agree). Our measure of empathy was based on Bos, Dijker, and Koomen (2007) and Van Alphen, Dijker, Bos, van den Borne, and Curfs (2011). Boys were asked to read a short scenario in which a boy assaulted a girl on the street and then had to indicate by use of two items the degree to which they experienced empathy (“I feel empathy/compassion for the girl,” 1 = totally disagree, 7 = totally agree; r = .71). Adverse sexual beliefs were measured using three items (α = .68), for example, “I think women mostly date men as to make use of them” (1 = totally disagree, 7 = totally agree) and adapted from Burt (1980). Attitude toward dating violence was measured by nine items (α = .81), for example, “I think that a girl who cheats on her boyfriend deserves to be beaten” (1 = totally disagree, 7 = totally agree) and was based on Price, Byers, & the Dating Violence Research Team (1999). Rape attitude included eight items (α = .91), for example, “I think a boy is allowed to force a girl into having intercourse when she has allowed him to take off her pants” (1 = totally disagree, 7 = totally agree) and was based on Maxwell, Robinson, and Post (2014). The scale Outcome Expectancies (α = .89) was based on O’Donohue et al. (2003). The scale measured to what extent the participant would expect seven outcomes that could occur as a consequence of persuading a girlfriend who is not in the mood to have sex (e.g., I would enjoy, she would enjoy, I would feel guilty; 1 = no, definitely not, 7 = yes, absolutely).
Attitudes toward stating boundaries when with friends (“To say no to my friends when I don’t agree with them, seems to me . . .” α = .60), attitudes toward communicating with a partner (“To ask my girlfriend what she does and does not want during sex, seems to me . . .” α = .88) and attitudes toward self-control (“To only have sex with my girlfriend when she also wants it, seems to me . . .” α = .88) were each measured by one statement with three semantic differentials (very bad, very good; very unimportant, very important; very uncomfortable, very comfortable). Self-efficacy toward self-control was measured with the following statement: “Imagine you have a girlfriend. You want to have sex but she does not want to.” followed by four response questions, such as “would you manage to . . . not become angry” (1 = no, absolutely not; 7 = yes, definitely; α = .85). Self-efficacy toward communication was measured by a scale which included five items (α = .87), such as “I’m able to communicate with my sex partner about what we do and do not want regarding sex” (1 = no, absolutely not; 7 = yes, definitely). Social norms were measured with four items (α = .61), for example, “my friends believe it’s okay to force a date into having sex when you spent a lot of money on her” (1 = no, absolutely not; 7 = yes, definitely). Self-efficacy to deal with peer pressure was measured with three items (α = .60), for example, “I’m able to say no to my friends when I don’t agree with them” (1 = no, absolutely not; 7 = yes, definitely). Finally, intention was measured with three items (α = .78) and assessed to what extent subjects expect to become angry, start persuading, or start whining when they want to have sex but their girlfriend does not (1 = no, absolutely not; 7 = yes, definitely).
Data Analysis
The data were analyzed in IBM SPSS 21 using mixed (multilevel) regression because of the nested structure of the design (repeated measurements nested within boys, who are nested within institutions). The predictors were condition (0 = control, 1 = intervention) and time of measurement (with dummy-indicators for post-test and follow-up, respectively, t1 and t2, and baseline as reference category). To capture unexplained outcome differences between institutions, a random intercept was included. To capture inter-individual differences over time, an unstructured covariance matrix for the repeated measures was selected. Due to the small sample size, no distinctions have been made with regard to the different cultural backgrounds or religions. Possible outcome differences between groups within institutions could not be modeled as most institutions contributed only one group, and those with more than one group did not (always) include a group identifier in the returned data. Similarly, possible outcome differences based on trainers could not be modeled as some trainers visited several institutions, and some institutions were visited by several trainers.
Histograms were used to check for normality and possible outliers in the distribution of the random intercept, as well as of the residuals per time point. Two outcome measures (social norm and rape attitude) showed severe non-normality (e.g., a large floor or ceiling effect). The scores on these outcome measures were recoded to better approach normality or at least to reduce severe skewness and outliers. 1 The effect analyses for these outcome measures were then rerun to check the robustness of the untransformed results. Running the effect analyses on the transformed outcome measures did not change the results in any relevant way. We therefore report the original (untransformed) data. Results were considered significant at p ≤ .005 (two-tailed) to correct for multiple testing. 2 Effect sizes were calculated as β/√ var, where β is the estimated group difference at T1 or at T2, and var is the residual outcome variance at that same time point. Note that this effect size comes down to Cohen’s d per time point, except that it is not based on the student t test for two unpaired means, but on multilevel analysis taking into account the baseline T0 and the nesting of boys within institutions.
Results
Table 2 provides the mean scores (observed) on the outcome measures at T0, T1, and T2. Mixed regression with institution as a random effect was used to check for baseline differences between intervention and control group on the outcome measures. There was no significant baseline difference on any of the 14 outcome measures (ps ≥ .21), suggesting successful randomization of institutions and participants across intervention and control conditions.
The aim of this research was to investigate whether there are program effects at post-test and follow-up, as reflected by a significant condition by time interaction (represented by the product terms Condition × T1dummy and Condition × T2dummy). No significant support for a program effect was found on any of the 14 outcome measures (ps > .03; see Table 3), but some small (d < .2) and small to medium (.2 < d < .05) effect sizes, both at short-term (T1) and long-term (T2), were observed.
Significance (p values) and Effect Sizes (Cohen’s d) of the Condition × Time Interactions.
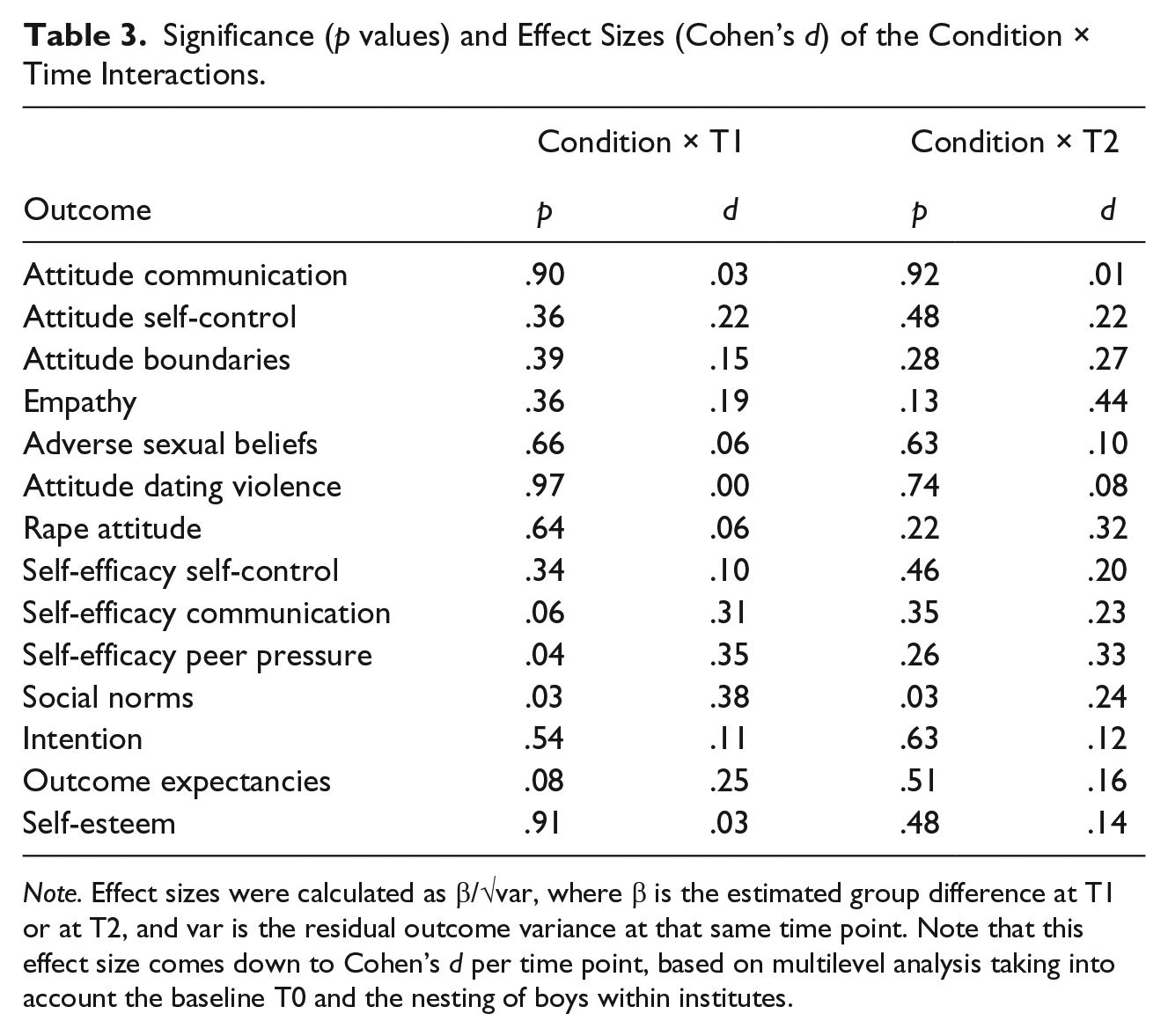
Note. Effect sizes were calculated as β/√var, where β is the estimated group difference at T1 or at T2, and var is the residual outcome variance at that same time point. Note that this effect size comes down to Cohen’s d per time point, based on multilevel analysis taking into account the baseline T0 and the nesting of boys within institutes.
To explore the possibility that program effects were dependent on whether participants had sexual experience (0 = no, 1 = yes), we reran the analyses with sexual experience and its two- and three-way interactions with condition and time in the model. When taking into account the critical values of the chi-squares, as in Johnson (1988), no statistical support was found for three-way interactions. The outcome measure rape attitude (p = .004) was the only measure that showed a significant three-way interaction effect with sex experience. However, its chi-square was below the critical value (χ2 = 9.06; df = 2; p = .004). We therefore rejected the model and thus concluded that sexual experience did not influence program effects. We also looked into age (recoded as a dichotomous variable, 0 = under 15; 1 = 15 and older) as a potential effect moderator. No significant tests of the Condition × Time × Age effects emerged (all χ2s ≤ 5.39, df = 2; all ps > .022).
Discussion
The present study describes the effect evaluation of a Dutch sexual harassment prevention program, Make a Move, which addresses determinants of sexual harassment among adolescent boys in residential youth care. The program has a cognitive-behavioral approach and includes eight group meetings guided by a trainer. Overall, results showed that after program delivery, boys in the intervention group did not differ significantly from boys in the control group, neither at direct post-test nor follow-up, on any of the 14 outcome measures.
As compared with the adolescent population in general, it seems that the boys in youth care did, on the whole, show higher rates of sexual harassment behaviors. For example, 40.9% reported having tried to persuade a partner into having sex, and 23.8% reported having taken advantage of a person’s drunkenness to get sex, as compared with 33% and 16.5%, respectively, in the report of Kuyper, de Wit, Adam, Woertman, and van Berlo (2010). These rates illustrate that boys in youth care are indeed a target group specifically at risk of being or becoming perpetrators of sexual harassment and are thus very much in need of a prevention intervention.
The main conclusion of the effect evaluation is that, even though effect sizes were small to medium, no significant changes were observed in the intervention group. It often is difficult to prove the effectiveness of interventions, even if they have a solid grounding in theory and evidence. Many different factors can play a role in this, and often there is more than one explanation for the lack of results found. Such explanations can generally be linked to the intervention itself, to its implementation, or to the evaluation.
First, the intervention itself might not be well designed, and may not address the exact needs of the target population. In the case of Make a Move, it is difficult to address the exact needs of the target population, as it is a population with a diverse range of problems and negative experiences that often result in emotional and behavioral disturbances (Connor et al., 2004; Jonson-Reid et al., 2007; Veerman & van Yperen, 2007). An extensive range of risk factors, in combination with a complex target population, made it difficult to identify which determinants may contribute most to preventing sexual harassment. In relation to juvenile sexual offenders, Seto and Lalumière (2010) did not find significant differences in terms of social skills or social competencies between adolescent sex offenders and adolescent non-sex offenders. They argue that to understand why sexual offenses are committed, and to prevent re-offending, it is important to discuss sexuality, including sexual fantasies, sexual arousal, and early exposure to sex and pornography. However, according to Seto and Lalumière (2010), interventions often focus on social skills and social competency, which would explain the lack of effects. Make a Move can be positioned somewhat in the middle. It not only includes communication skills training but also explicitly addresses aspects of sexuality. Furthermore, discussions about sexuality and sexuality-related attitudes and norms are an important part of the program. At the same time, it is difficult to assess whether the program adequately meets the needs of this particular target group, with its complex and diverse problems and experiences.
Meta-analyses on the effectiveness of youth care institutions in contributing to a positive development of youth with serious behavioral and/or emotional problems also show mixed results (De Swart et al., 2012; Knorth, Harder, Zandberg, & Kendrick, 2008; Souverein, Van der Helm, & Stams, 2013). De Swart et al.’s (2012) review on the effectiveness of institutional youth care confirms the findings of Seto and Lalumière (2010), who showed that (social) skills training had no positive effects. A review by Knorth and colleagues (2008) suggests that programs which also involve the family show the most promising results in improving the behavioral development of youth in care. All in all, these findings show that more research is needed to establish what may work best in the context of youth care.
A second factor influencing program effectiveness relates to the level of intervention implementation. When a program is not implemented as intended, but rather with lower levels of completeness and fidelity, its potential will not be reached (Brownson, Glanz, Tabak, & Stamatakis, 2015). The implementation of Make a Move appeared to be very challenging and needed to take into account several factors such as the interaction with and between the boys, time constraints, and the fact that the resources and facilities allocated were not always suitable (van Lieshout et al., in press). Differences between the trainers (styles, skills, motivation) are also likely to have played a role in the implementation of the program. Closely linked to adequate implementation (dose delivered) is the dose received by the target group; this also turned out to be very low, in large part because groups were unstable, with many boys missing meetings. Furthermore, issues such as the problematic backgrounds and social power struggles among some boys made it difficult for them to open up and actively participate in the group meetings. This explanation seems to be in line with that of Veerman and van Yperen (2007), who propose that the difficulties of performing RCTs in youth care practices can contribute to the lack of carefully controlled effect evaluations.
Finally, it is worth noting that a program might be effective, but the evaluation of it may not have been optimal. Sufficient participants are needed when using a RCT, and the measures included should match the objectives targeted by the intervention (Bartholomew et al., 2011). Although the design of our study was based on an RCT and included a baseline measure and two post-tests (direct post-treatment and 6-month follow-up), the number of participants that completed all of the questionnaires was rather low. Moreover, it is difficult to estimate how seriously the boys may have answered the questionnaires. It is possible that they might have answered some questions while anticipating what would be socially desirable. Furthermore, trainers reported back that many boys had problems concentrating long enough to answer the full questionnaire, and that some also had difficulties in fully comprehending the questions. Furthermore, the dropout rate in the intervention group was higher than in the (waiting list) control group, which could have biased our results.
Conclusions and Implications
There is a considerable lack of systematically described and evaluated programs addressing sexual harassment which focus on at-risk youth. This article is among the first to describe an effect evaluation of a program targeting sexual harassment among the specific at-risk group of adolescent boys in youth care. Even though no significant intervention effects were found, the present study contributes to the literature by providing a systematic overview of the intervention content and an in-depth example of how such a program can be evaluated in the complex setting of youth care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the Netherlands Organization for Health Research and Development (ZonMw No: 124330006).