
Abstract
This study focuses on sexual violence experiences suffered by Spanish transgender individuals throughout the life span. Using a cross-sectional design, 33 face-to-face semi-structured interviews were conducted which included questions regarding the presence and/or absence of sexual violence, the nature of said sexual violence, by whom sexual violences were committed, coping mechanisms used, and certain mental health indicators. Results found a high percentage of transgender individuals to have been victims of sexual violence during childhood, to use avoidance as a coping mechanism for said experiences, as well as the frequent recurrence of experiences of sexual violence, showing victimization processes. In addition, the relationship between said experiences and mental health indicators were observed. This study highlights the importance of and need for addressing sexual violence among this population, and discusses and analyzes possible components of future educative and clinical intervention strategies.
Child Sexual Abuse and Sexual Assault in Adolescence and Adulthood
Sexual violence has been defined as any sexual act, any attempts to obtain a sexual act, or any acts to traffic for sexual purposes, directed against a person using coercion, harassment, or advances made by someone regardless of their relationship to the victim, in any setting, including but not limited to home and work (Jewkes, Sen, & Garcia-Moreno, 2002). In the area of sexual violence, there are a variety of studies on sexual abuse in childhood (Cantón & Justicia, 2008; Hornor, 2010; López, 1994; Priebe & Svedin, 2008), as well as on sexual coercion during adolescence and youth (Fernández-Fuertes, Orgaz, & Fuertes, 2011; Hernández & González, 2009; Krahé et al., 2015; Ortega, Ortega-Rivera, & Sánchez, 2008) and sexual assault in adulthood, principally in the sphere of intimate partner relationships (Cáceres, 2004; Cáceres & Cáceres, 2006). However, thus far, these studies have focused primarily on the general population; few studies that focus on specific communities have been conducted, such as the occurrence of this problem among individuals with no heteronormative identities (Bontempo & D’Augelli, 2002; Edwards et al., 2015; Han et al., 2013) and, more specifically, transgender individuals (Courvant & Cooks-Daniels, n.d.).
Child sexual abuse is defined as any sexual activity that the child cannot understand nor consent to or that violates the law (Modelli, Fonseca, & Pratesi, 2012), and includes occurrences such as forcing a child to observe exposed genitals or to witness sexual activity, genital touching, or intercourse (López, 1994). Although the data are inconclusive due to mixed results and differences in the methodology used in previous studies, it seems that child sexual abuse occurs in approximately 8% to 12% of boys and between 15% and 20% of girls (De Paúl, Milner, & Múgica, 1995; López, 1994; Pereda, Guilera, Forns, & Gómez-Benito, 2009; Stoltenborgh, van Ijzendoorn, Euser, & Bakermans-Kranenburg, 2011; White & Smith, 2011). We also know that it is more common for women to be victims than men. Women have a two or threefold greater risk than males to be sexually abused during childhood and about one out of 10 women experiences this (Barth, Bermetz, Heim, Trelle, & Tonia, 2013), particularly when sexual violence occurs in the domestic sphere, the most typical setting of sexual abuse (Echeburúa & Corral, 2006; Vázquez-Mezquita, 1995).
Figures about prevalence of sexual abuse are diverse, probably due to the different kinds of data sources used (interview vs. questionnaire), the size of the samples used, the moment at which the data are taken, or even what is understood by the term sexual abuse. In any case, studies have highlighted that sexual abuse is underreported and that women are at a greater risk to become victims, especially during childhood. Undoubtedly, suffering childhood sexual abuse can negatively affect mental health of victims, triggering symptoms such as depression, low self-esteem, and suicidal ideation among others (Hornor, 2010).
Those children who do not report their first instance of sexual abuse are at a higher risk of sexual re-victimization. In addition, those abused children who also lack familial affection are prone to feel guilty (Madansky, 1996; Milner & Crouch, 2004). The fear of not being believed, of being the cause of breaking familial bonds and/or of retaliation from the aggressor increases the probability that the child’s response will be to remain silent (Horno, Santos, & Molino, 2001).
Keeping child sexual abuse a secret prevents children from understanding or identifying themselves as victims of abuse. This cultivates a “dark spot” in awareness, caused by the idea that “what we do not talk about does not exist,” which then strengthens the relationship with the perpetrator (Malacrea, 2000). This type of childhood sexual abuse makes it difficult for children to distinguish between acceptable and inappropriate behavior, in addition to other more devastating effects. In this sense, victims could suffer physical problems, such as sleep disorders or psychosomatic symptoms and stress; interpersonal problems (e.g., loss of self-confidence or confusion about sexuality, distrust of others, and avoidance of intimacy); psychological problems, such as guilt, shame, lack of self-identity, or even mental health problems (Garbarino & Eckenrode, 1997).
Alternatively, one of the most accepted findings in scientific literature on sexual violence is the correlation between suffering sexual violence in childhood and subsequently experiencing repeated instances of sexual violence in adolescence or adulthood (Balsam, Lehavot, & Beadnell, 2011; Fuertes, Ramos, & Fernández-Fuertes, 2007; Pereda, 2010; Testa & Dermen, 1999). In addition, the difficulty of reporting child sexual abuse cases or of asking for help increases the likelihood of facing difficulties in future interpersonal and sexual relationships (Garbarino & Eckenrode, 1997).
However, there are certain differences between sexual assault in adolescence and in adulthood. However, during adolescence, sexual violence is more common in casual relationships than in stable partnerships, whereas in adult relationships, instances of sexual violence seem to occur more frequently in stable or seemingly stable relationships (Jewkes, 2002; Ortega et al., 2008). However, it seems that in both life stages the social framework of dominance-submission is present, that is, a model in which relationships are understood as the dominance of one party and submission of the other (Meras, 2003). As was the case of child sexual abuse, both in adolescence and adulthood it is women who most frequently suffer these types of experiences (J. C. Campbell & Soeken, 1999), especially women who have not adjusted to heteronormativity (Walters, Chen, & Breiding, 2013). In addition, as with child sexual assault, sexual violence suffered later in life is also associated with a variety of mental health issues such as post-traumatic stress disorder (PTSD), depression and high levels of psychological distress, failed suicide attempts, self-harming behaviors, behavioral problems, and difficulties in interpersonal relationships (Balsam et al., 2011; Walsh, Galea, & Koenen, 2012).
Sexual Violence Among Transgender Individuals
Knowledge about sexual violence suffered by transgender 1 people (National Center for Transgender Equality, 2014) is limited mainly because, as stated by Todahl, Linville, Bustin, Wheeler, and Gau (2009), in research and data on sexual assault, it is rare to find any gender identification categories used besides the typical male/female dichotomy.
The few studies that have taken transgender identities into consideration show that this population suffers frequent instances of physical and verbal violence in different contexts throughout the life span, especially transgender women. 2 These studies also show that the transgender population suffers sexual violence at disproportionately high rates in comparison with the general population (Duke & Davidson, 2009; Grant et al., 2011; Lombardi, Wilchins, Priesing, & Malouf, 2001).
The social construction of sexuality and gender, developed under the influence of heteronormativity processes, generates an ideological narrative, which is also accepted by many people who are close to transgender people in different contexts (Rich, 2003). Because of this situation, transgender individuals who are aware of the conflict between experienced and assigned gender experiment a significant level of psychological distress related to the difficulty of freely being themselves amid the pressures of demanding social and family dynamics. This situation makes this group of transgender people more vulnerable (Coates, 1990; Kenagy, 2005; Meyer & Dupkin, 1985; Scourfield, Roen, & McDermott, 2008). In addition, it is known that the most vulnerable children are more likely to suffer situations of sexual abuse (Milner & Crouch, 2004). The most proximal contexts, especially the family, must help the children by meeting their needs, promoting healthy development and preventing them from being abused, including sexual abuse (López, 2008). When the need to be valued and/or recognized is not adequately addressed, this serious lack of support results in the child’s increased vulnerability and marginalization (Conron, Scott, Stowell, & Landers, 2012; Riley, Sitharthan, Clemson, & Diamond, 2011). The likelihood of children’s vulnerability and marginalization increases when their family does not provide the child with these needs. Due to this, transgender children are more susceptible to higher rates of abuse (Fernández-Rouco, Carcedo, López, & Orgaz, 2007; Grant et al., 2010).
Alternatively, there are some studies on experiences of physical and emotional violence in transgender adults, frequently among victims of hate crimes (Federal Bureau of Investigations, 2014). The findings on the presence of repeat victimization shows higher incidences among transgender women than transgender men (Clements, Katz, & Marx, 1999; Thomas, 2004), similar to the results found among other populations (López, Carpintero, Hernández, Martín, & Fuertes, 1995), especially in regard to partner relationships (Dank, Lachman, Zweig, & Yahner, 2014) as well as to results found with respect to other types of violence within this population, in which women again are the most frequent victims of abuse (Lombardi et al., 2001). We also know that violence generates significant distress and that repeated episodes of victimization diminish welfare and health status and can even trigger failed suicide attempts (Kenagy, 2005).
Regardless of the aforementioned studies, there remains a need for research that sheds light on the occurrence and prevalence of sexual violence suffered by the transgender population, and identifies general and specific factors associated with these problems. A deeper understanding is essential in developing effective interventions to reduce the social exclusion of transgender people, and to facilitate prevention by distancing those at-risk individuals from this highly vulnerable situation.
Thus, in this article, we have tried to answer the following unanswered questions: (a) What situations of sexual violence have transgender people suffered during childhood and later on in life, and how did they deal with it? (b) Is there a clear risk of re-victimization? (c) To what extent do these instances of sexual violence impact the psychological health support of this population? In addition, we attempt to answer these questions to explore the situations of sexual violence and the consequences thereof in the lives of these individuals.
Method
An exploratory and descriptive study was designed to examine the experiences of sexual violence suffered by transgender people. Data collection was performed with a cross-sectional design.
Participants
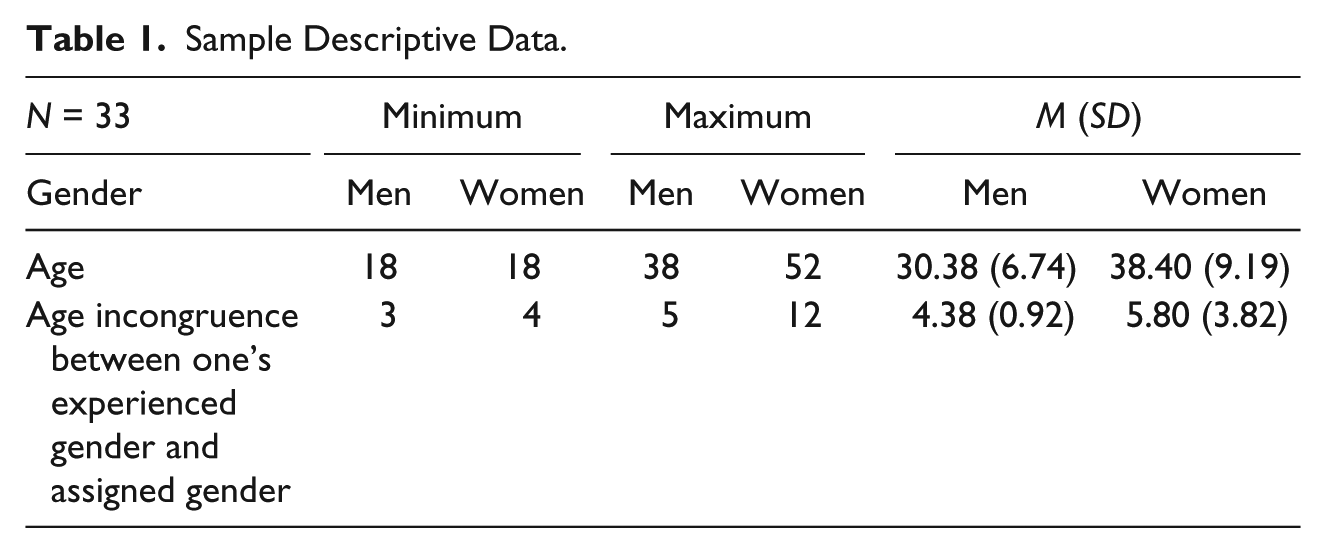
Although 120 Spanish transgender individuals were interviewed (60 men and 60 women), only those who had experienced some form of sexual violence in their life span were included in this study (N = 33). Thus, the final sample of this study comprises 33 participants, eight transgender men, and 25 transgender women, whose ages vary from 18 to 52 years (M = 36; SD = 10.19). Other descriptive data of the sample are shown in Table 1.
Sample Descriptive Data.
After informed consent was obtained, all individuals took part in the study voluntarily and they did not receive any incentive for their participation. Contact with the participants took place in different parts of the country, initiating contact by phone through different entities including associations, such as hospitals or health centers, Internet forums and by word of mouth. Participants were informed of the nature of the study and eligibility to participate was evaluated. All participants answered all the questions openly and without objection.
Procedure
As agreed upon in the initial contact, a meeting was arranged with participants in the most convenient location for them, always in a private room. Face-to-face semi-structured interviews were carried out with each person during a mean of 1 hr approximately, in which the interviewer recorded the information in writing. We introduced ourselves as university staff interested in their life story and situation in relation to experiences of sexual violence and its relationship with psychological health and support. The first part of the interview was used to establish rapport with the participant and note the possibility to end the interview at any time regardless of the fact that the interview was anonymous and the data were confidential. In this regard, no disclosure was made regarding the identity of the participants. These ethical principles set the foundation for collecting high-quality data.
Variables and Measures
Experiences of sexual violence and their consequences in childhood, adolescence, and adulthood were assessed via the following questions included in the semi-structured interview.
Sexual Violence Experiences
Child abuse
To describe the experiences of child abuse, the following questions were asked:
Have you had any unwanted or non-consensual sexual experiences prior to the age of 14? This question was dichotomized (1 = yes, 2 = no).
Which of the following unwanted or non-consensual sexual experiences have you have suffered prior to 14 years of age? The response categories were defined by taking into account the categorization proposed by López (1994; 1 = someone showed me their genitals, 2 = I touched or stroked the genitals of another person, 3 = intercourse, 4 = I performed a sexual activity while being watched).
With whom did it occur? This question was coded (1 = parents, 2 = other family relative, 3 = partner/significant other, 4 = friend, 5 = acquaintance, 6 = stranger).
How often did it occur? This question also had multiple response options (1 = once, 2 = a few times, 3 = occasionally, 4 = often 5 = very often).
How did you deal with the situation? This question was formulated openly, to analyze the response of the participants.
Sexual Assault in Adolescence and Adulthood
To describe the experience of sexual assault suffered, the following questions were asked:
Has anyone ever forced or pressured you to have unwanted/non-consensual sexual contact after 14 years of age? Answer choice was dichotomous (1 = yes, 2 = no).
What type of contact? This question was coded according to the categories of sexual behavior formulated by Schofield (1968; 1 = kissing, hugging and fondling, 2 = genital fondling, 3 = vaginal intercourse, 4 = anal intercourse, 5 = oral sex).
With whom did it occur? This question was also categorized (1 = parents, 2 = other relatives, 3 = partner/significant other, 4 = friend, 5 = acquaintance, 6 = stranger).
How often did it happen? This issue was also raised with response options (1 = once, 2 = a few times, 3 = occasionally, 4 = often 5 = very often).
How did you deal with this situation? This question was formulated openly, to become familiar with the communication style of the participants.
Consequences of violence
To explore possible consequences of sexual violence, the following question was asked: What impact has suffering sexual violence had on your life?
Violence situations presence
To consider the possible occurrence of other types of violence, it was asked whether the participant had suffered any other type of violence throughout their life. This question was categorized (1 = never, 2 = A few times, 3 = occasionally, 4 = often 5 = very often).
Psychological health support
To determine how the well-being of participants had been affected, the following questions were asked:
Have you ever sought mental health support? This issue was previously dichotomized (1 = yes, 2 = no).
Have you ever been in a mental health center? This issue was also dichotomized (1 = yes, 2 = no).
Have you ever tried to hurt yourself? This question was coded (1 = yes, 2 = no).
Have you ever tried to commit suicide? This question was also coded (1 = yes, 2 = no).
Data Analysis
First, regarding structured questions, the interviews were completed in full and correctly-answered, meaning that those with errors or questions were left blank because they were recorded in writing by the interviewer. The data codification and quantitative analyzes were performed with SPSS 20.0. First, the descriptive data (see Tables 2 and 3), frequencies, and percentages, and, second, the bivariate correlations were shown (Table 4).
Frequencies and Percentages of the Sexual Violence Experiences by Gender and for all the Participants.

Descriptive Results of Well-Being Problems.

Bivariate Correlational Analysis Between Studied Variables.

Correlation is significant at .05 (bilateral). **Correlation is significant at .01 (bilateral).
Related to open questions, because our analysis is based on a social constructionist perspective, we paid special attention to the ways in which the participants described their experiences of sexual violence and the extent to which it affected their psychological health and support. Qualitative questions (“How did you deal with the situation?” for child abuse and for sexual assault in adolescence and adulthood, and “What impact has having suffered from sexual violence had on your life?” for consequences of violence
Results
The findings of this study will be organized around two topics: first, the description of experiences of violence, exploring victimization and re-victimization, and, second, the relationship among children who have suffered from sexual abuse and sexual violence in adolescence and adulthood, and their general well-being.
Experiences of Sexual Violence: Victimization and Re-Victimization
This study is based on 33 transgender victims of sexual violence who were found in a total sample of 120 transgender individuals (used for another study). This represents a prevalence rate of sexual violence of 27.5%.
The descriptive data of these situations of sexual violence are shown, both in childhood (0-13 years old) and later (14 or more years old). As we can see, the majority of experiences of sexual violence suffered by the sample occurred during childhood (see Table 2).
In both cases, sexual abuse during childhood and sexual violence later in life, transgender women have suffered from sexual violence in higher proportions.
Alternatively, child sexual abuse has been experienced by nearly the entire sample population. The most frequent child abuse behavior suffered was being forced to touch someone’s genitals, followed by someone touching their genitals. Child abuse was committed by a family member in more than a half of the population (51.7%), 6.9% by strangers and 41.4% by acquaintances.
Furthermore, 44.8% of participants experienced one-time abuse, while more than a half of the sample experienced repeated or multiple instances of sexual violence (55.2%).
After discussing situations of sexual violence suffered, participants were asked about how they coped with these experiences as children. Responses reported primarily two response types. For the majority of those interviewed (87.5% of abused people), the main response to their experience of abuse was keeping it a secret, hiding it from their families and remaining silent for many years. Below, one of the testimonies is shown: Nothing, I couldn’t do anything, they would not have believed me, with all the problems I gave trying to present as a girl, they have not listened to me . . . I didn’t think about it, I forgot and did not talk about it for years . . .
On the contrary, some of sample population reported it to someone they trusted (12.5% of abused people). This information was collected through their interview. Below, an example is shown: At first I kept quiet, but I could not stand being around my cousin, so it had to tell my mother . . . after that it was better because she wouldn’t let me near him.
Regarding sexual violence experienced after childhood, of the 10 sexual assault victims, 60% were assaulted by the person with whom they had an intimate relationship (dating partner or sexual partner), while 30% were assaulted by an acquaintance and 10% were victims of a family member. The most frequent abuses suffered were general touching, followed by kisses and hugs and non-genital fondling.
In these cases, instances of sexual violence always happened more than once (100%).
Victims were also asked about coping techniques. The results were similar to those in the child abuse situations. In this case, of the 10 people who suffered sexual violence, 80% remained silence, while 20% asked for help. Below is the testimony of one of the participants: I had not started to transition yet and I was so embarrassed to tell anyone that the man forced who forced himself on me did it because lesbians turned him on . . . I recently told this story to my psychologist for the first time, and I still feel nervous when retelling it . . .
Another important finding was related to re-victimization, that is, people who were sexually abused as children experiencing sexual abuse again later in life. Of the 29 people who suffered child sexual abuse, 20.7% experienced some form of sexual assault later in life. This percentage increased to 69% of child sexual abuse survivors experiencing some other form of violence later in life.
Finally, in regard to the questions about the consequences of experiences of sexual violence, responses divided into two types, problems in intimate relationships and problems related to well-being.
In this sense, intimate partner relationships were affected to the extent that participants became more fearful of possible violent situations, more distrusting of people with whom they shared intimate relationships and more fearful that arguments would involve aggressive behavior from their partners.
Look, you can never know who to sleep with, because if your own partner does that it’s impossible to trust anyone . . . I do not want to have relationships anymore, friends sure, but nothing more . . .
In addition, for those whose well-being was affected by situations of violence, it often resulted in feelings of guilt, shame, anxiety, and anger. These emotions are present in their relationships and their daily lives, as shown below: This situation affected me, it changed my life. Between this experience and feeling as though I was in a body that was not mine and that others didn’t accept, I’ve always been very insecure, very afraid to have sex and afraid that they would hurt me. I know I am vulnerable, but I’ve had a really bad time of it . . .
Effects on Psychological Health
In addition to describing their experiences of sexual violence, we were interested to learn the extent to which the well-being of the transgender participants had been affected. In this regard, the results show that all participants have at one point solicited psychological or psychiatric support. In addition, the impact on well-being is clearly noted as more than half of the participants have performed self-harming behaviors at one point and/or have made failed suicide attempts (see Table 3).
From these findings, the negative impact on well-being within this community has become clear. As we move forward, we will indicate the possible relationship between sexual violence and the aforementioned problems.
Sexual Violence and Psychological Health
The bivariate correlation analysis shows significant correlations between some of the variables evaluated. It demonstrates the correlation between child abuse and instances of sexual assault after 14 years of age. Also, experiences of sexual violence were correlated with suffering other types of violence as well.
With regard to the effects of sexual violence on psychological health, the findings highlight the correlations between suffering child abuse and having spent time in a mental health unit, performing self-harming behaviors and having a failed attempted suicide. In addition, there are significant correlations between self-harm and having a failed attempted suicide among those participants who had experienced sexual assault after 14 years of age. Finally, we also found a correlation among failed suicide attempts, self-harm, and being admitted to a psych unit (see Table 4).
As we can see, experiences of sexual violence were clearly related not only among themselves and with experiences of other types of violence but also to the damaging effects on the psychological health of participants.
Discussion
This work was initially focused on compiling in-depth descriptions of experiences of sexual violence suffered throughout the life span among transgender individuals. As has already been mentioned, this work is part of a larger study of 120 participants, of whom 33 (27.5%) have experienced some form of sexual violence. Regarding the question of “what situations of sexual violence have transgender people suffered in childhood and later on in life?” the data collected shows that transgender people in this population have experienced a high level of sexual violence. Moreover, in more than half of the cases, the acts of sexual violence were cases of child abuse perpetrated by a relative, as a participant noted, “I don’t like remember it. I was a child and he was my mother’s partner. It happened a few times, until my mother split up with him.” This finding is similar to other transgender studies results (Kenagy, 2005). In addition, the testimonies about how they dealt with the sexual abuse have one aspect in common, silence. There can be three reasons for this. On one hand, due to the difficulties they experienced with their gender identity within the family, they felt they would not be deemed credible. On the other hand, considering that the aggressor is a relative, the child does not trust the family to sufficiently protect him or herself. Finally, expressions of gender that are not consistent with biology tend to be stigmatized: Most transgender people are rejected and judged since childhood. Some interviewed participants pointed out this problem as it was shown in the “Results” section: Nothing, I couldn’t do anything, they would not have believed me, with all the problems I gave trying to present myself as a girl, they wouldn’t have listened to me . . . I didn’t think about it, I forgot about it and didn’t talk about it for years . . .
Other studies showed the importance of the role of relatives and the way in which they influence a family’s functioning. When abuse occurs within the home, far from fulfilling the care and protection children need, the situation becomes increasingly grave as transgender children are in a particularly vulnerable situation, generated by the conflict around their gender identity (Scourfield et al., 2008). In addition, abused children with non-supportive families reported higher levels of anxious attachment and psychological health problems, as opposed to abused children with supportive families, who expressed good psychological and intimate relationships (Godbout, Briere, Sabourin, & Lussier, 2014). Thus, the damage and negative effects on these children may be even greater.
However, in subsequent instances of sexual assault later in life, the perpetrator is most frequently the intimate partner of the participant. This is consistent with other studies that have found sexual violence to primarily occur in intimate partner relationships (Fernández-Fuertes et al., 2011; Ortega et al., 2008). Furthermore, the victims are mainly transgender women, as previously noted (J. C. Campbell & Soeken, 1999; Fuertes et al., 2007; White & Smith, 2011).
Another finding reflected by the study tries to answer the following question: “Is there a clear risk of re-victimization?” Results showed that 33% of those who suffered childhood sexual abuse were subsequently abused and that the recurrence of abuse was probably due to the child’s vulnerability, inadequate coping skills, poor family ties, or guilty feelings. Related testimonies emphasize the secrecy and silence as coping mechanisms, which contribute directly to their experience of loneliness, lack of protection, and vulnerability (Milner & Crouch, 2004). Transgender survivors of sexual abuse (during childhood and/or later in life) found it difficult to talk about or report the “secret.” As noted, silence around abuse and assault forms an integral part of the destructive social and personal dynamic, preventing the child from understanding their own victimization. This further complicates development, as children may confuse acceptable behaviors with abusive ones, causing greater harm and relational and mental health problems (Garbarino & Eckenrode, 1997). This is remarkable for transgender people: The social construction of a specific kind of sexuality and gender identity makes this population highly susceptible to rejection and discrimination; moreover, this is related to the incidence of sexual abuse, the probability of hiding the violence they suffer, and its novice effects. One of our testimonies showed the relational problems that occurred as a result of sexual abuse experiences: Look, you can never know who to sleep with, because if your own partner does that it’s impossible to trust anyone . . . I don’t want to have relationships anymore, friendship of course, but nothing more . . .
In addition, feelings of guilt and shame are also characteristic of those adolescent and adult survivors of sexual violence: “I spent a lot of years rejecting my own body and sexual contacts: it was disgusting to me.” Previous research also found similar results (Echeburúa & Corral, 2006).
Our last interest was to answer “To what extent do these instances of sexual violence impact the psychological health support of this population?” Most of the sample demonstrated emotional and psychological distress and the need for psychological health support (e.g., “I was so hard going ahead with all of the problems. It was really difficult and I looked for a professional”), pointing out that as was shown in other studies on transgender people (Ellis & Eriksen, 2002) as well as other studies focused on the effects of sexual violence on well-being (Balsam et al., 2011). However, at present there is no data linking these two situations. Probably, in spite of the relationship between suffering sexual abuse and being transgender, gender identity takes a prominent place among the concerns of transgender people due to its influence on all areas of their lives throughout their entire life span. In any case, although the transgender experience would assumedly be a more important concern for transgender people, the consequences of being victims of sexual abuse or assault to their mental health would probably be extraordinary as well.
Thus, we have attempted to identify a possible connection between the experience of unwanted sexual encounters and psychological harm or mental health support. This relationship was confirmed in our data. In survivors of child abuse, the relationships to time in mental health units, self-harming behaviors, and suicide attempts was demonstrated; and for adolescent and adult sexual assaults, the association with self-harming behaviors and suicide attempts was demonstrated as well. The relationship between having suffered sexual violence and negative impact on mental health and well-being has been reflected in previous studies as well, particularly in relation to suicide attempts (Wathen & MacMillan, 2003).
Our testimonies showed how silence would be maintained until they received psychological health support. However, it is worth noting that in our data the instances of sexual violence showed no relationship to instances of seeking mental health support. From our perspective, this is related to the specifics of the transition process required for transgender people to medically and legally transition. The medical transition process is marked by gatekeeping, as a psychological assessment and referral is mandatory to begin the legal process of living in accordance with their true gender identity.
Furthermore, it can be noted that not only living a transgender experience but also having survived experience of sexual violence both have implications on well-being among this population. To further our depth of understanding, it would be of value to focus the subsequent debate on identifying whether being self-identified transgender from childhood increases vulnerability both in childhood and later in life, or if both situations need to be interpreted separately. However, this is particularly complex because nearly all of the people in the sample identified with a gender different from their assigned sex at birth from a very early age, forming a significant part of the construction of their identity.
It is important to mention that all these findings advance previous knowledge. First, no previous study exists regarding sexual violence in the transgender population in Spain. Second, this work analyses the retrospective history of sexual violence of transgender people, including experiences of re-victimization. Finally, the consequences of sexual violence and the strategies used to cope with it are studied from the discourse of the participants.
Some limitations were revealed in this work, despite having presented new and interesting results for the scientific, professional, and social community. For instance, the sample is not large enough to be able to perform other statistical analyses and inadequate access to this population further complicates large-scale sample sizes. Regardless, there are no historical studies related to sexual violence in trans* people, thus this article provides important findings about this historical perspective. Furthermore, the dichotomous response items would have been richer with another response format, although the larger study to which this pertains did not allow us to further deepen our exploration. Moreover, this article did not analyze cultural or racial implications concerning an issue which crosses ethnic, social, racial, national, economic, and many other boundaries, which must be included in future research. In addition, this retrospective study is subjective as it is dependent upon the participants’ memories and their biographic interpretations.
Although this study provides new, current, and interesting data in our country in regard to the transgender population, it would be valuable to continue exploring these questions. In this regard, it would be ideal to realize further studies, both cross-sectional and longitudinal, on victimization and repeat victimization in the transgender population to determine specific implications of sexual violence for these individuals. Furthermore, it would be ideal to design intervention actions for victims of sexual violence, specifically in this community. Prevention programs should help transgender people to learn the skill of saying “no” in coercive situations. It is also important for transgender people to discuss the occurrence of sexual violence and psychological consequences in their relationships. The need for intimacy and affection may reduce their assertive skills and also their perception of sexual risk, so it is essential to work on communication and emotional management skills. Although the responsibility for sexual violence is on the perpetrator, helping transgender people to prevent future sexual violence may be the best solution for avoiding re-victimization, especially until the violence against transgender people is no longer considered acceptable by society.
Finally, the challenge remains, not only to intervene in extreme cases but also to deepen our understanding of the difficulties relating to sexual violence as well as adequate intervention strategies for the transgender population. These are issues that should be addressed in future studies.
Conclusion
Transgender people are usually victims of violence, including sexual, throughout their lives. Nevertheless being transgender becomes a capital focus throughout the life span, so suffering from sexual violence experiences and its consequences, in spite of their adverse implications, are not taken into account equally.
At this moment, no study has presented this problem biographically, including both sexual abuse and sexual assaults after adolescence, especially in transgender people, whose sample access is not easy.
On the contrary, traditionally studies on sexual abuse and/or sexual assault have used only quantitative methods; trauma, victimization, and feelings have not been examined well. As research in the field of sexual abuse and assault moves forward, the use of quantitative and qualitative method approaches may be able to address difficult questions regarding this topic. Such collaborative research may help uncover answers to today’s most elusive questions (R. Campbell & Wasco, 2005).
The present study makes an important contribution to this effort using both closed and open-ended questions to explore the history of sexual violence and the consequences in has on transgender people.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.