
Abstract
Violence is a common phenomenon both in regular and forensic psychiatric settings, and has a profound impact on staff and other patients. Insight into the individual risk factors associated with violence in forensic psychiatric settings is rare and is therefore the subject of this research. A retrospective file study in three medium security units in Flanders was conducted to compare non-violent inpatients with inpatients who engaged in (verbal and physical) violent behavior. Binary logistic regression analyses were used to examine which variables contributed independently to the risk of violence. The results showed that absconding during treatment was independently associated with physical violence. A personality disorder diagnosis and general non-compliance with treatment were associated with verbal violence. Both types of violence predicted early termination of treatment. Contrary to previous research, the results from the risk assessment tools were not associated with inpatient violence. Clinical implications are discussed and include, among others, that clinicians should remain vigilant for early warning signs of non-compliance during treatment.
Violence is a common phenomenon in regular and forensic psychiatric settings, although the risk of very serious physical violence with serious injuries is limited (Cornaggia, Beghi, Pavone, & Barale, 2011; Kelly, Subica, Fulginiti, Brekke, & Novaco, 2015; Woods & Ashley, 2007). In a forensic psychiatric setting, nearly all staff reported verbal violence, 70% reported being physically assaulted during the past year, and 12% of the staff was injured so badly they had to take time off from work (Kelly et al., 2015). Besides affecting staff, patients perpetrating violence are adversely affected as well because seclusion and restraints are often used to manage aggressive behavior, and inpatient violence can result in prolonged involuntary confinement (Quanbeck, 2006). Furthermore, disruptive or violent behavior can result in discharge from treatment, although to the best of our knowledge, this has not been examined yet in forensic psychiatric settings. Research addressing inpatient violence in forensic psychiatric settings is relatively scarce versus the amount of research conducted in civil psychiatric settings, prisons, and among professionals working in the domain of security (Bogaerts, Daalder, Van der Knaap, Kunst, & Buschman, 2008; Chan & Chow, 2014; Hogan & Ennis, 2010; Kunst, Bogaerts, & Winkel, 2009). Studying inpatient violence and victimization in forensic settings is important because one of the primary objectives of forensic psychiatric treatment is to learn violent patients how to de-escalate as well as to teach vulnerable patients, such as psychotic forensic patients, how to prevent (re)victimization. Furthermore, inpatient violence predicts violent recidivism after treatment (Spreen, Brand, Ter Horst, & Bogaerts, 2014).
Several models can explain the occurrence of inpatient violence. The internal model suggests that individual factors such as antisocial personality characteristics or impulsivity contribute to violence. The external model emphasizes the role of environmental factors such as ward design and the approach to treating staff. The situational or interactional model focuses on interactions between patients and staff members (Dickens, Piccirillo, & Alderman, 2012). Relatively few studies compared individual characteristics of violent and non-violent (forensic) patients (Bowers et al., 2011). However, knowledge about these individual inpatient risk factors is very important and can inform risk management policies and strategies, and enables staff to recognize risk situations, thus limiting both inpatient as well as future aggressive incidents (Bowers et al., 2011).
Individual Factors Associated With Inpatient Violence in Forensic Psychiatric Settings
First, we note that a uniform overall accepted definition of aggressive or violent behavior is lacking, which can result in different operationalizations (Klerx-Van Mierlo & Bogaerts, 2011). Some studies focused exclusively on physical violence toward others, that is, one type of interpersonal violence (Linhorst & Scott, 2004). Other studies included verbal violence in their definition of interpersonal violence and/or included other forms of violence such as self-directed violence (e.g., suicidal behavior) or violence toward objects (e.g., Chan & Chow, 2014). Here, violence refers to a specific form of interpersonal aggression that results in or threatens physical harm to another person (further interpersonal violence [IPV]). Aggression refers to a broader definition including other forms of violence such as self-directed violence or violence against property (further aggression in general [AIG]).
Two meta-analyses of the risk factors associated with inpatient AIG in forensic settings found that aggressive patients were significantly younger and—contrary to the findings in acute general psychiatric settings—more likely to be male (Dack, Ross, Papadopoulos, Stewart, & Bowers, 2013; Hogan & Ennis, 2010). However, some other single studies found no gender-aggression association (Ball, Young, Dotson, Brothers, & Robbins, 1994; Nicholls, Brink, Greaves, Lussier, & Verdun-Jones, 2009; Rogers, Watt, Gray, MacCulloch, & Gournay, 2002). Criminal history variables such as previous violent offenses or having a violent index offense were not associated with IPV in most single studies (Doyle, Dolan, & McGovern, 2002; Hoptman, Yates, Patalinjug, Wack, & Convit, 1999; Linhorst & Scott, 2004; Rasmussen & Levander, 1996; Rogers et al., 2002). One study stressed a history of violence as a predictor of AIG in general and IPV in particular (Ball et al., 1994). The number of previous psychiatric admissions was associated with IPV (Ball et al., 1994; Linhorst & Scott, 2004) and with seclusion after an AIG incident (Thomas et al., 2009).
From a clinical perspective, intellectual disability was not associated with IPV (Ball et al., 1994), but some studies found an association between low education and IPV (Harris & Varney, 1986; Hoptman et al., 1999). Personality disorders were typically associated with IPV and AIG (Chan & Chow, 2014; Gow, Choo, Darjee, Gould, & Steele, 2010), but one study failed to find an association (Ball et al., 1994). In contrast, a history of substance misuse (including alcohol misuse) at admission was not associated with IPV (Ball et al., 1994; Hoptman et al., 1999; Rogers et al., 2002; van der Kraan et al., 2014). However, a current substance-related disorder and a dual diagnosis of schizophrenia and substance misuse were associated with IPV (Chan & Chow, 2014; Hoptman et al., 1999). Psychosis or schizophrenia alone was not associated with IPV in forensic psychiatric settings (Douglas, Guy, & Hart, 2009; Hoptman et al., 1999). In general, the presence of a psychiatric diagnosis per se does not seem to be a sufficiently sensitive or reliable measure for IPV (Doyle et al., 2002), but the stage of the illness or active symptomatology might be a more valuable predictor (Gudjonsson, Rabe-Hesketh, & Wilson, 1999). For example, several studies found that positive psychotic symptoms were significantly higher in IPV and AIG (Daffern, Howell, Ogloff, & Lee, 2005; Rasmussen & Levander, 1996; Vitacco et al., 2009). Doyle and Dolan (2006) found that anger emotion regulation problems were associated with IPV, and Wang and Diamond (1999) addressed anger as a stronger predictor of IPV than previous violence. Furthermore, patients exhibiting chronic suicidal and self-injuring behaviors showed the highest levels of IPV (Hillbrand, 1995). Finally, more objective markers, such as cognitive tests or serum cholesterol may be potentially valuable predictors for IPV and AIG. However, research in this field is still in its infancy (O’Reilly et al., 2015; Sedgwick, Young, Das, & Kumari, 2016).
Other potential risk factors for violence in forensic settings relate to general misconduct during treatment. First, persistent substance misuse during treatment was associated with violent recidivism during absconding (Hildebrand, Schönberger, & Spreen, 2007). Second, low treatment engagement (defined as both attendance and active participation at core program sessions) was significantly more common in aggressive female forensic patients (Long, Dolley, & Hollin, 2012). The items unresponsive to treatment and non-compliance with remediation attempts of the Historical Clinical Risk Management-20 (HCR-20; Webster, Douglas, Eaves, & Hart, 1997) were both related to IPV (Abidin et al., 2013; Mudde, Nijman, van der Hulst, & van den Bout, 2011). Third, absconding was associated with AIG (Brook, Dolan, & Coorey, 1999) and with verbal but not with physical IPV (Cullen et al., 2015). Ball et al. (1994) stressed the current risk of escape as a potential indicator for IPV.
Risk Assessment Instruments Predicting Inpatient Violence in Forensic Psychiatric Settings
Besides these individual risk factors for inpatient IPV and AIG, the value of risk assessment instruments to predict inpatient violence has been studied. For example, the HCR-20 (especially the clinical scale) was useful in assessing risk for inpatient IPV and AIG in forensic psychiatric settings (Hogan & Ennis, 2010; McDermott, Edens, Quanbeck, Busse, & Scott, 2008; Mudde et al., 2011; Wilson, Desmarais, Nicholls, Hart, & Brink, 2013). Contrary to these findings, the predictive validity of the HCR-20 for IPV in forensic units was poor in field validity studies (Jeandarme, Pouls, De Laender, Oei, & Bogaerts, 2016; Neal, Miller, & Shealy, 2015; Pedersen, Ramussen, & Elsass, 2012; Vojt, Thomson, & Marshall, 2013). Along with the HCR-20, Hogan and Ennis (2010) found that the Hare psychopathy scales were predictive of AIG. Other meta-analyses investigated the association between the Hare psychopathy scales and institutional violence in different settings among which forensic psychiatric settings. They found a more robust association with general inpatient misconduct compared with physical violence and with Psychopathy Checklist–Revised (PCL-R) Factor 2 compared with PCL-R Factor 1 (Guy, Edens, Anthony, & Douglas, 2005; Walters, 2003). Furthermore, psychopathy was a stronger predictor for proactive or instrumental IPV than for reactive IPV in a forensic psychiatric hospital (Vitacco et al., 2009). The Violence Risk Appraisal Guide (VRAG; Quinsey, Harris, Rice, & Cormier, 2006) is another risk-assessment instrument designed to predict violence. Some studies found that the VRAG was predictive of inpatient IPV and AIG (Doyle et al., 2002; McDermott, Dualan, & Scott, 2011; Snowden, Gray, Taylor, & Fitzgerald, 2009), although others found no effect (Chu, Thomas, Ogloff, & Daffern, 2013; McDermott, Quanbeck, Busse, Yastro, & Scott, 2008). In Flanders, the VRAG predicted institutional IPV only marginally in forensic psychiatric offenders with an intellectual disability (Pouls, Jeandarme, & Habets, 2014). Unlike these previous studies, other schemes such as the Brøset Violence Checklist (BVC; Almvik, Woods, & Rasmussen, 2000) or the Dynamic Appraisal of Situational Aggression (DASA; Chan & Chow, 2014; Ogloff & Daffern, 2006) have been developed specifically to assess the risk for inpatient violence, but these are used infrequently in forensic settings (for example, see, Woods, Olver, & Muller, 2015).
Methodological Problems Associated With Studies on Inpatient Violence
The comparison of studies investigating inpatient violence and aggression is hampered by several methodological problems. First, as mentioned earlier, different definitions and operationalizations of violent or aggressive behavior are used and may contribute to some of the contradictory findings. A literature review on psychiatric inpatient aggression identified the most common operationalizations: (a) interpersonal physical violence, (b) a combination of interpersonal physical and verbal violence and aggression toward objects, and (c) a combination of interpersonal physical and verbal violence, aggression toward objects, and self-directed violence (Bowers et al., 2011).
Second, the review of Dack et al. (2013) shows that the studies differ in their method of data collection. The majority of studies used patient notes or standard incident reports, while some used standardized and validated scales designed to measure aggression, such as the Staff Observation Aggression Scale–Revised (SOAS-R; Nijman et al., 1999). In addition, it is likely that the terms inpatient and institutional are used interchangeably. Inpatient violence can occur on different occasions: in the unit, in the hospital premises, or during (un)supervised leave outside of the hospital premises. Institutional violence only refers to violence on the ward. These specifications are rarely reported.
Third, studies use different follow-up periods, whereby higher base rates for interpersonal violence can be expected with longer follow-up periods. In addition, different statistical analyses that do or do not control or adjust for potential confounding factors may result in different interpretations.
Present Study
This study contributes to the research on IPV within a forensic psychiatric setting by examining risk factors for IPV during medium security treatment. Prior research rarely evaluates separate forms of violence. Therefore, we will analyze several types of IPV (verbal, physical, and a combination of both). This study also analyzes whether IPV predicts treatment dropout. The following research questions are addressed:
Material and Method
Setting
The study was conducted at the three forensic medium security units (MSUs) in Flanders (the Dutch-speaking part of Belgium). These units are part of the general psychiatric hospitals and are located in the communities of Bierbeek, Rekem, and Zelzate. All patients were found not guilty by reason of insanity (NGRI, in Belgium referred to as internees) after having committed an offense. They were submitted to an internment measure to protect society from further offenses. Conditional release from an internment measure is linked to mandatory treatment under the supervision of a regional court—the Commission for the Protection of Society (CPS). Violent (and other) incidents occurring during the treatment are reported to the CPS on a regular basis by the MSUs and/or the probation officer. In the case of incidents, the CPS may interrupt treatment due to revocation of conditional release. This would typically be the case when either the MSU or the internee (less common) decide to stop the treatment. In case of very serious incidents, i.e. when the safety of the public can no longer be guaranteed by the MSU, the treatment can be stopped. Because no high security units were established at the time of the study, revocation of conditional release resulted in incarceration either for a time-out period or for a longer confinement.
The MSUs were implemented in Flanders in 2001 with the goal of providing a treatment setting for NGRI patients who do not require very secure hospital care, but who are deemed too dangerous or unsuitable for a general psychiatric ward or outpatient care. MSUs typically admit psychotic as well as personality-disordered internees. Internees with a primary diagnosis of substance use disorder, intellectual disability, or paraphilia are excluded from treatment, although all these conditions can be present as co-morbid disorders (see Boers, Vandevelde, Soyez, De Smet, & Ting to, 2011, for a description of treatment programs).
Study Population
The population (N = 531) was predominantly male (94.9%, n = 504) with a Belgian nationality (90.1%, n = 475). The mean age at first admission to a MSU was 36.5 years (SD = 10.82 years, range = 18.8-73.4 years). The average length of stay in these units was 676.4 days (SD = 505.90 days, range = 8-2,729 days). About 10% of the internees (n = 65) were still in treatment at the end of the study. Of the remaining group (n = 461), a third (31.7%, n = 146) dropped out prematurely from treatment.
Participants were found NGRI for a variety of offenses, where the most serious offense consisted of violence (77.2%, n = 410), property crimes (18.6%, n = 99), drug-related crimes (2.3%, n = 12), sexual non-violent crimes (0.8%, n = 4), and other offenses such as destruction of property (1.1%, n = 6). Prior contact with the criminal justice system was common; only a minority (15.6%, n = 83) were registered as first offender. On average, patients had been sentenced on 6.3 occasions (SD = 5.73, range = 1-40) for a general offense and on 2.4 occasions (SD = 1.91, range = 0-11) for a violent offense.
The most common diagnoses according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) were personality disorders (70.6%, n = 375), substance use disorders (56.7%, n = 301), psychotic disorders (43.9%, n = 233), and intellectual disability (12.8%, n = 68). The mean total score on the PCL-R (Hare, 2003; n = 224) was 21.1 (SD = 6.58, range = 6-36.8). The mean HCR-20 score (n = 235) was 24.5 (SD = 5.34, range = 10.5-36), and the mean VRAG score (n = 230) was 8 (SD = 10.94, range = −26 to +38).
Procedure and Outcome Measures
Data were collected for all patients treated between 2001 and 2010. All patients were asked for passive consent. Eleven patients refused, leaving a total study population of 531 patients. This comprised approximately the whole Flemish medium security population over a 10-year study period.
Violent incidents were registered based on the incident reports found in CPS files. Person-based information was gathered through CPS as well as through hospital files. Information on treatment variables was limited to information that was reported to the CPS. This study focused on IPV, which referred to the intentional use of physical force or power—threatened, attempted, or actual—against another person. Verbal IPV referred to threatened violence; physical IPV referred to attempted or actual IPV. Four groups were constructed with increasing severity of violence: (a) patients with no violent incidents, (b) patients with only verbally violent incidents, (c) patients with only physically violent incidents, and (d) patients with both verbally and physically violent incidents.
Non-compliance referred to not adhering to treatment rules, for example, not engaging in treatment plans, refusing prescribed medication, or drinking alcohol during treatment, whereas non-compliance alcohol was limited to drinking alcohol. Drug use referred to the use of illegal substances or non-prescription medication as well as to dealing of illicit substances. Absconding referred to absconding from (un)supervised leave or absconding without permission to leave the unit or premises. Dropout referred to treatment dropout. As explained earlier, internees whose treatment was stopped were incarcerated again.
The VRAG was scored on a convenience sample of 230 patients; other risk assessment scores were field validity scores. In case of multiple scores, the first assessment was selected.
The study was approved by the Medical Ethical Commission of the University Hospital of Antwerp.
Data Analysis
SPSS Version 22 was used for the statistical analyses. Patient base rates (violent patients/sample × 100) and event base rates (incidents/sample × 100) were calculated (based on Bowers et al., 2011). Differences between the four patient groups were tested using the chi-square or Fisher exact test in case of categorical variables. The means between the patient groups were compared with between-group one-way ANOVAs if needed after root square log transformation. Post hoc comparisons used Tukey HSD or Dunnett T3 in case of unequal variances. Effect sizes were measured using Cramer’s V for categorical variables and partial eta squared and r for continuous variables. McNemar’s test was used on paired nominal data. Significant bivariate associations were entered in multiple logistic regression analyses. An additional regression analysis investigated whether IPV would predict dropout. The correlation between length of stay and the occurrence of (physically and verbally) violent incidents was analyzed using point-biserial correlations to determine whether this effect needed to be controlled for in subsequent analyses.
Some analyses were based on smaller samples because the data sources were characterized by some missing data; this is noted throughout the article and in Table 2.
Results
Prevalence of Violence
Between 2001 and 2010, IPV incidents were recorded for 21.7% of the admitted patients (n = 115). In total, 189 IPV incidents were reported (event base rate = 35.6%). The patient base rate was 13.7% (n = 73) for verbal IPV and 13% (n = 69) for physical IPV. The event base rate for verbal IPV was 17.5% and 18.1% for physical IPV. Table 1 shows the nature of the incidents in more detail. Twenty-seven patients exhibited both verbal and physical IPV. Neither type of IPV were associated (McNemar, p = .75).
Nature of IPV (Event and Person Related).

Note. IPV = interpersonal violence.
Most patients involved in incidents were violent in the unit or hospital premises (82.6%, n = 95); a minority were violent only during (un)supervised leave (7%, n = 8) or on both occasions (10.4%, n = 12).
The relationship between patients’ length of stay and the occurrence of violent incidents (r = .02, p = .59), physically violent incidents (r = .07, p = .12), and verbally violent incidents (r = −.02, p = .72), was not significant.
Variables Contributing to the Risk of Violence
Four groups of patients were compared in Table 2: (a) patients with no IPV incidents (n = 416), (b) patients with only verbal IPV incidents (n = 46), (c) patients with only physical IPV incidents (n = 42), and (d) patients with both verbal and physical IPV incidents (n = 27).
Person-Related Characteristics of (Verbal and Physical) IPV.
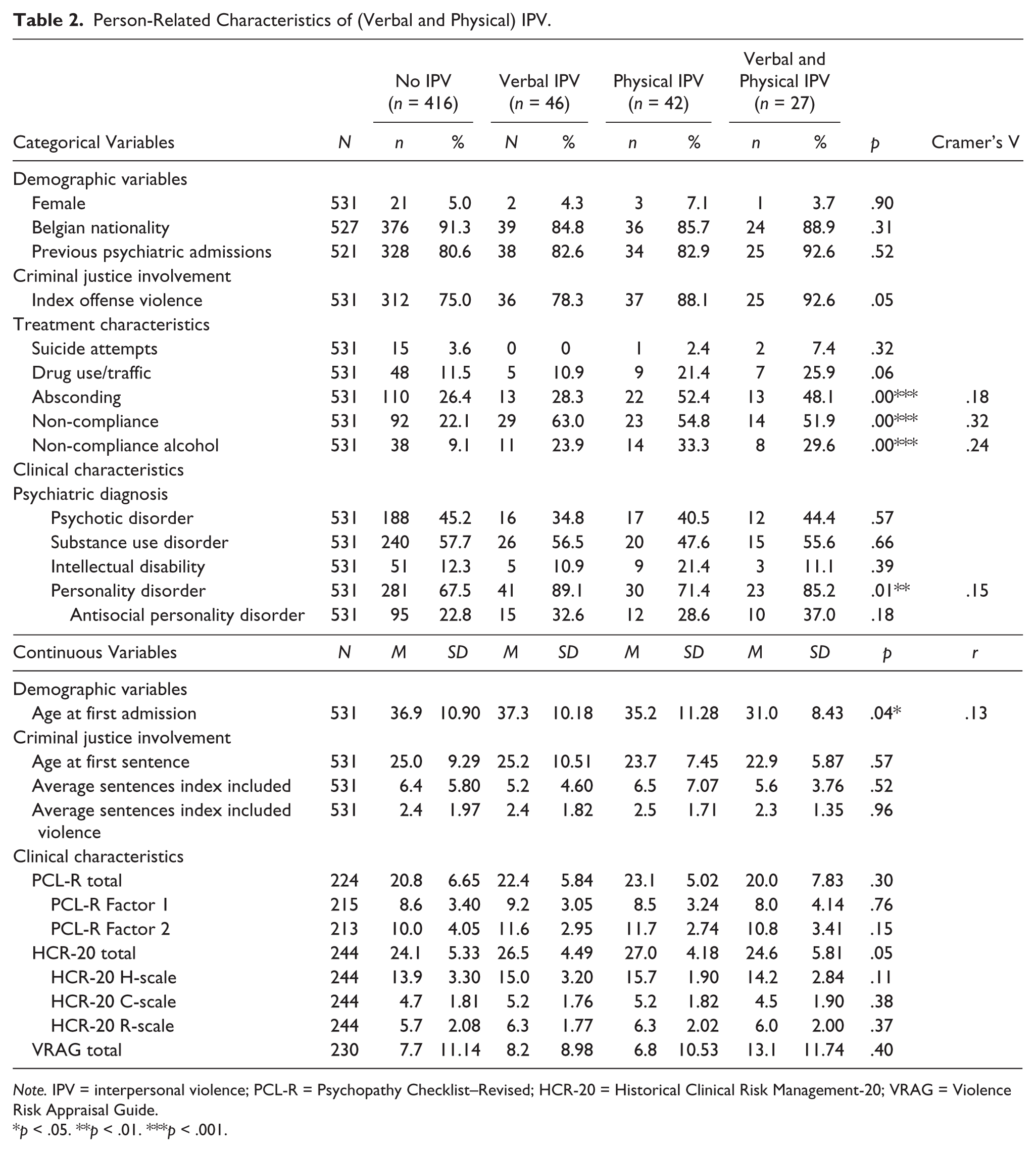
Note. IPV = interpersonal violence; PCL-R = Psychopathy Checklist–Revised; HCR-20 = Historical Clinical Risk Management-20; VRAG = Violence Risk Appraisal Guide.
p < .05. **p < .01. ***p < .001.
Demographic, criminal history, and clinical variables
There was a marginal significant negative effect of age on severity of IPV, F(3, 527) = 2.85, p = .04. There was also a significant linear trend indicating that as the age at admission decreased, the severity of IPV increased proportionally, F(1, 527) = 8.52 p = .00. The magnitude in the differences of the means and effect size was small (partial eta squared = .02). Post hoc comparisons to evaluate pairwise differences among group means were conducted with the Tukey HSD test because equal variances were tenable. Tests revealed significant pairwise differences between the mean age of the group with no IPV (M = 36.9, SD = 10.90, CI = [35.81, 37.91]) compared with the combined verbally and physically IPV group (M = 31.0, SD = 8.43, CI = [27.62, 34.29]), p = .03. The verbal and physical IPV groups did not significantly differ from the other two groups.
No significant differences were found among the groups regarding criminal justice involvement.
In general, personality disorders were associated with the severity of IPV. There was a significant difference between the percentage of patients with a personality disorder in the group with no IPV (67.5%), verbal IPV (89.1%), physical IPV (71.4%), and the combined IPV group (85.2%), χ2(3) = 12.26, p = .01, Cramer’s V = .15.
Treatment characteristics
Several treatment characteristics were associated with the occurrence and severity of IPV. There was a significant difference between the percentage of absconders in the group with no IPV (26.4%), verbal IPV (28.3%), physical IPV (52.4%), and combined IPV group (48.1%), χ2(3) = 16.89, p = .00, Cramer’s V = .18. There was also a significant difference between the percentage of non-compliers in the group with no IPV (22.1%), verbal IPV (63.0%), physical IPV (54.8%), and the combined IPV group (51.9%), χ2(3) = 54.88, p = .00, Cramer’s V = .32.
Violating the alcohol prohibition was associated with the severity of IPV. There was a significant difference between the percentage of patients using alcohol in the group with no IPV (9.1%), verbal IPV (23.9%), physical IPV (33.3%), and the combined IPV group (29.6%), Fisher exact, p = .00, Cramer’s V = .24. Finally, dropout was associated with the severity of IPV. There was a significant difference between the percentage of patients who dropped out from treatment in the group with no IPV (22.3%), verbal IPV (60.0%), physical IPV (66.7%), and the combined IPV group (66.7%), χ2(3) = 64.87, p = .00, Cramer’s V = .38.
Logistic Regression Analyses
Variables that showed a significant difference on the bivariate level (absconding, non-compliance, non-compliance alcohol, personality disorder, and age at first admission) for severity level of IPV were entered in the logistic regression models to examine which variables contributed independently to the risk of inpatient verbal, physical, and combined verbal/physical IPV. In these analyses, the dependent variables were (a) verbal IPV (n = 46), (b) physical IPV (n = 42), and (c) verbal in combination with physical IPV (n = 27). The enter option was used for all analyses, and the results can be found in Table 3.
Logistic Regression Analyses Explaining Verbal Violence, Physical Violence, and Combined Violence.
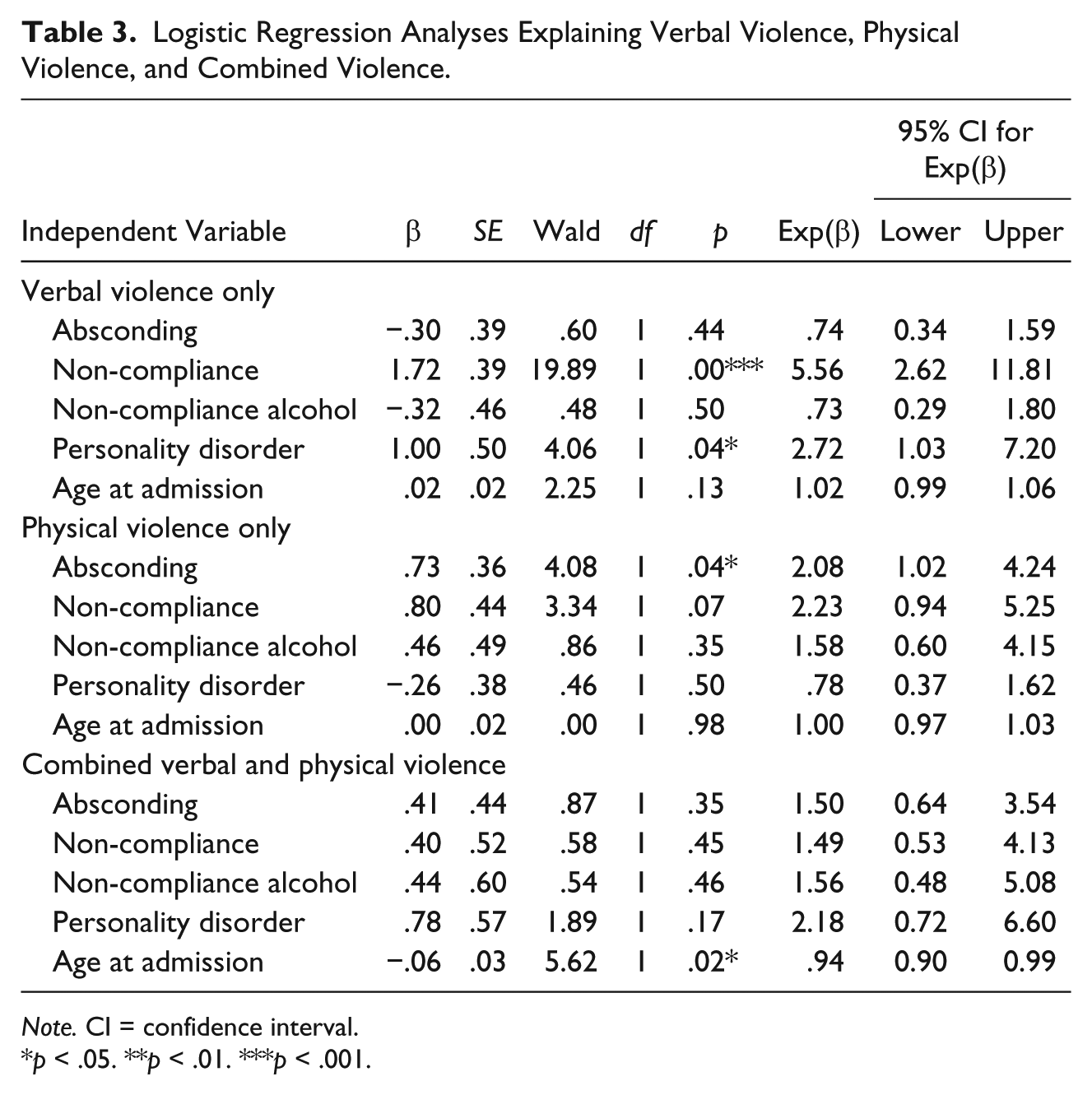
Note. CI = confidence interval.
p < .05. **p < .01. ***p < .001.
The first binary logistic regression analysis examined the association with verbal IPV and included 531 of the 531 internees. The model was statistically significant, χ2(5) = 33.14, p = .00, and correctly classified 91.3% of the cases. A Nagelkerke R2 of .14 showed that the global model explained 14% of the variation in the dependent variable. Internees who did not comply were six times more likely to be verbally violent and internees with a personality disorder were three times more likely to be verbally violent.
The second binary logistic regression analysis, which examined the association with physical IPV, included 531 of the 531 internees. The model was statistically significant, χ2(5) = 19.87, p = .00, and correctly classified 92.1% of the cases. A Nagelkerke R2 of .09 showed that the global model explained 9% of the variation in the dependent variable. Internees who absconded were twice as likely to be physically violent.
The third binary logistic regression analysis, which examined the association with combined verbal and physical IPV, included 531 of the 531 internees. The model was statistically significant, χ2(5) = 17.16, p = .00, and correctly classified 94.9% of the cases. A Nagelkerke R2 of .10 showed that the global model explained 10% of the variation in the dependent variable. Younger internees were more likely to be both verbally and physically violent.
Prediction of Treatment Dropout
Finally, we studied whether IPV would predict treatment dropout. For these analyses, the dependent variable was dropout from treatment and the independent variables were verbal IPV, physical IPV, and combined verbal and physical IPV. The enter option was used for all analyses. The binary logistic regression analysis included 461 of the 531 internees. The model was statistically significant, χ2(5) = 61.24, p = .00, and correctly classified 74.6% of the cases. A Nagelkerke R2 of .17 showed that the global model explained 17% of the variation in the dependent variable. Verbal violence predicted dropout from treatment (β = 1.65, Wald = 22.67, df = 1, p < .00, Exp(β) = 5.21, CI = [2.64, 10.29]), as well as physical violence (β = 1.94, Wald = 28.59, df = 1, p < .00, Exp(β) = 6.95, CI = [3.42, 14.15]) and combined verbal and physical violence (β = 1.94, Wald = 18.46, df = 1, p < .00, Exp(β) = 6.95, CI = [2.87, 16.83]).
Discussion
The aim of the present study was to shed light on the prevalence of inpatient IPV in the three medium security settings in Flanders. Verbal, physical, and both verbal and physical IPV patients were compared with patients with no IPV via several sociodemographic, clinical, and criminogenic factors. This study contributes to the limited research in the area of inpatient violence in forensic psychiatry (Dack et al., 2013). The study retrospectively investigated violent behavior through the analysis of incidents reported in judicial files. The study also analyzed whether IPV would predict dropout from treatment. The person and event base rate for physical IPV was low versus the base rates found in a meta-analysis of studies in forensic psychiatric settings (Bowers et al., 2011). When controlling for other variables, distinct associations were found for different forms of IPV. Overall, few risk factors for inpatient IPV were found. This is not surprising because the study mainly focused on static individual patient factors (Dack et al., 2013). More surprisingly, common risk assessment instruments such as the HCR-20, PCL-R, and VRAG were not associated with inpatient IPV. All degrees of IPV predicted dropout from treatment.
Only one demographic factor differentiated between the severity of violence. In line with the meta-analysis of Dack et al. (2013), IPV patients were significantly younger than non-violent patients. Also, the severity of violence increased as the age of admission decreased. After controlling for other variables, age was only associated with the combination of both verbal and physical violence. Previous research found that in forensic settings, women show significantly more violent behavior than men (Dack et al., 2013), although other studies did not (Daffern et al., 2005; Nicholls et al., 2009). We found no gender differences similar to Daffern et al. (2005); this might be due to the limited number of female patients.
With respect to criminal justice involvement, having a violent index offense or a violent history was not associated with IPV. This was in line with other research (Doyle et al., 2002; Linhorst & Scott, 2004). These studies showed that past violence is a poor predictor of inpatient IPV in samples with high numbers of previous violence.
More associations were found between treatment variables and violence. However, suicide attempts while in treatment were not associated with the severity of violence, which is in line with Hillbrand (1995). He found that having a history of suicide attempts alone was not associated with violence, although severe and chronic self-injurious and suicidal behavior did predict violence. Other variables associated with the severity of IPV related to treatment-interfering factors more generally (non-compliance, non-compliance alcohol, and absconding). After controlling for other variables, non-compliance was only associated with verbal IPV. Our definition of non-compliance (a combination of non-engagement in treatment and not adhering to treatment rules) was broader than the definitions found in other forensic studies, but added to the research and stated that non-cooperative and non-engaged patients were more likely to be violent (Long et al., 2012; Mudde et al., 2011). In line with Ball et al. (1994), absconding was associated with the severity of IPV, but this effect disappeared after controlling for other variables for verbal violence and the combined outcome measure; it remained significant for physical violence. This study somewhat contradicts Cullen et al. (2015), who found an association with verbal but not with physical IPV.
Alcohol use was associated with the severity of IPV, while illicit drug use was not. After controlling for other variables, alcohol use was no longer associated with IPV. A few studies investigated the influence of ongoing substance use during treatment, but the relationship between substance use and crime is still poorly understood. Several factors can mediate or moderate this relationship such as the severity of the substance-related disorder; individual psychological, social, and neurobiological characteristics; situational factors; and the expectations regarding the psychopharmacological effects of a particular substance (Lammers et al., 2014). As van der Kraan et al. (2014) mentioned, it is relevant to identify whether substance misuse is a primary or a secondary criminogenic need.
The severity of IPV also showed associations with one clinical variable—a diagnosis of personality disorder. This was consistent with other research (Chan & Chow, 2014). After controlling for other variables, a personality disorder diagnosis was only associated with verbal violence. Whittington and Richter (2006) argued that the practical relevance of psychopathological and personality factors for dealing with aggressive patients remains unproven. In the present study, psychopathology was not associated with the severity of violence. More specifically, a diagnosis of psychosis was not associated with the severity of violence, thereby confirming the meta-analytic work by Douglas et al. (2009). A possible explanation for these findings is that the stage of the illness or the presence of active symptoms might be a more valuable predictor of violence than diagnosis as such (Daffern et al., 2005).
More surprisingly, this study found no association between the PCL-R, HCR-20, and VRAG and severity of inpatient IPV. Although previous studies found mixed results (Chu et al., 2013; Doyle et al., 2002; Endrass, Rossegger, Frischknecht, Noll, & Urbaniok, 2008; Snowden et al., 2009), the VRAG was not associated with severity of violence here. Also, in contrast to other research (McDermott, Edens, et al., 2008; Mudde et al., 2011), the HCR total and subscales were not associated with the severity of IPV. One of the explanations for this finding could be that the HCR-20 scores in this study were field validity scores, which are poor to even non-significant predictors of inpatient violence (Jeandarme et al., 2016; Neal et al., 2015; Pedersen et al., 2012; Vojt et al., 2013). In the literature, the association of psychopathy with institutional violence is well established, although some studies found no association (e.g., Rasmussen & Levander, 1996) or showed a more nuanced picture. In this study, psychopathy was not associated with the severity of violence. It may well be that in forensic psychiatric settings, the predictive accuracy of risk assessment schemes was reduced due to risk management strategies. These are implemented when a high risk patient was identified.
All forms of violence (verbal, physical, and a combination of both) predicted dropout from treatment. Two thirds of the patients with physical violence also dropped out from treatment. The present study did not investigate whether the violent incidents actually caused the expulsion from treatment, but it did highlight that inpatient IPV was not only associated with prolonged confinement as stated by Quanbeck (2006) but also associated with early treatment termination. The association of violence with a high risk of treatment dropout raises concern because a meta-analysis investigating cognitive–behavioral offender treatment programs has shown that offenders who do not complete treatment have higher recidivism rates than offenders who complete the treatment program. Furthermore, non-completers had higher recidivism rates than those who were not offered treatment (d = −.16; McMurran & Theodosi, 2007). While this study did not investigate this, it is plausible that being violent was a reason for treatment expulsion (Long et al., 2012).
Limitations
Some limitations of the current study must be understood to interpret the results appropriately. First, the outcome measure of the study was limited to violence against others or IPV whereas other studies examined a much wider range of violent or aggressive behavior including aggression to property or self-directed violence. As such, methodological issues hamper the comparability of the current results with other studies.
Second, violent incidents were selected from incident reports recorded in judicial files, which tend to underestimate the number of assaults. Because there is neither a formal obligation nor standardized reporting protocol in Flemish forensic institutions to the CPS court, the dark number of violent incidents remains unknown. Some studies used a standardized instrument such as the SOAS-R (Nijman et al., 1999; Palmstierna & Wistedt, 1987), while other studies used a range of approaches. This also contributes to methodological problems in comparing study results.
Third, severity was defined according to whether the IPV was verbal or physical (or combined). This may be somewhat arbitrary if, for example, a death threat (verbal) is compared with a push (physical).
Fourth, data of the three forensic units were not presented separately, and thus, possible differences in treatment and reporting approaches could not be differentiated.
Fifth, with respect to the bivariate analyses, the hypotheses were based on the unadjusted p values with a probability that some of the true null hypotheses were rejected.
Finally, the study was retrospective, which limits its utility. We focused on individual risk factors for interpersonal violence and did not analyze protective factors. Also, it was, for example, not possible to gain insight into how these incidents influenced the therapeutic relationship between patients and hospital staff and what the role of patient–staff interactions might have been on the occurrence of violence (Cornaggia et al., 2011). In this respect, this study is only the first step toward the management and prevention of violent incidents. It would be very interesting to study de-escalation techniques applied by staff in different settings, and to examine whether the application of different techniques can impact the prevalence and severity of violent incidents (Hallett & Dickens, 2015).
Clinical Implications and Conclusion
The most surprising finding regarding IPV was perhaps that in MSUs where the vast majority of the patients had a history of violence, most patients did not behave violently during their stay. This low figure possibly reflects adequate risk management of staff but may also be explained by underreporting. Accurate reporting is important both to enhance risk management and to limit liability issues. This study showed that IPV patients misbehaved more generally during treatment, that is, more violent patients absconded, did not comply with hospital rules, and kept on drinking alcohol during treatment even though this was prohibited. In fact, after controlling for other variables, treatment characteristics were the only characteristics that predicted IPV. The commonly used risk assessment instruments and other well-established risk factors for community violence such as previous violence were not useful predictors. Patients who are not actively collaborating with staff or who do not comply with hospital rules are more prone to become engaged in coercive interactions that may escalate into IPV. Two thirds of the patients with physical IPV dropped out from treatment versus one in five patients without IPV. This increased risk for dropout was not exclusively related to physical violence—60% of the patients with verbal IPV dropped out from treatment. Thus, it is important to be vigilant for verbal violence and to investigate this form of violence further. Although not studied here, threats may precede physical violence and may be a powerful predictor of violent acts in forensic patients as already noted by Ball et al. (1994) and Woods et al. (2015).
In sum, these results suggest that dynamic treatment variables can act as warning signals for IPV. As was noted in a review on patients’ perspectives on violence, patients stated that they had often given staff warnings about potential violence or showed clear signals of distress over a long period, without receiving adequate intervention. This causes misunderstanding, and feelings of being ignored (Gudde, Olso, Whittington, & Vatne, 2015). Treatment staff should carefully monitor incidents, for instance, by using an instrument to monitor treatment progress and incidents such as the Dutch Instrument for Forensic Treatment Evaluation (Schuringa, Spreen, & Bogaerts, 2014).
Furthermore, the need for a more dynamic and contextual approach in investigating predictors of inpatient IPV was highlighted by the few individual static risk factors showing different associations with verbal and physical IPV. Indeed, triggers for violence are multifactorial and involve interplay between individual, situational, and structural factors (Dickens et al., 2012). Cornaggia et al. (2011) noted in this respect that there is a particular need for an appropriate number of nurses, a non-overcrowded setting, nurses’ training, and a “good warm climate” in dealing with violence (p. 18). In other words, a narrow focus on individual patients is only part of the solution to reduce inpatient violence. As stated by Bader and Evans (2015), we cannot expect severely ill patients to recover “in polluted, toxic environments” (p. 181).
Footnotes
Acknowledgements
We wish to thank the forensic units, clinicians, and clients who participated in the study, namely Sint-Kamillus (Bierbeek), OPZC Rekem, and Sint-Jan-Baptist (Zelzate). Furthermore, we would like to thank the CPS Chairmen for help with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Limburg Sterk Merk (LSM) and the Public Psychiatric Care Center Rekem (OPZC Rekem).