
Abstract
This study aims to examine the prevalence of multiple types of child victimization and the effects of multiple types of victimization on children’s mental health and behavior in Taiwan. The study also examines the child-protection rate and its correlates among children experiencing various types of victimization. This study collected data with a self-report questionnaire from a national proportionately stratified sample of 6,233 fourth-grade students covering every city and county in Taiwan in 2014. After calculating the 1-year prevalence of child victimization, the study found that bullying was the most prevalent (71%), followed by physical neglect (66%), psychological violence (43%), inter-parental violence (28%), community violence (22%), physical abuse (21%), and sexual violence (9%). As the number of victimization types increased, children were more likely to report greater posttraumatic symptoms, psychiatric symptoms, suicide ideation, self-harm thoughts, and violent behaviors. Gender, neonatal status, parental marital status, and other family risks were significantly associated with elevated incidences of the victimization types. Only 20.6% of the children who had experienced all seven types of victimization had received child protective services. A child was more likely to receive child protective services if he or she had experienced sexual violence, community violence, inter-parental violence exposure, higher family risks, higher suicidal ideation, or living in a single-parent or separated family. In conclusion, this study demonstrates the cumulative effects and the harmful effects that children’s experience of multiple types of victimization can have on the children’s mental health and behavior. The present findings also raise alarms regarding the severity of under-serving in child-victimization cases. These results underscore the importance of assessing, identifying, and helping children with multiple victimization experiences.
Keywords
Introduction
Emerging studies during the past 15 years have revealed that children’s experience of multiple types of victimization across settings (i.e., family, school, community) is prevalent and a distinct threat to children’s health, mental health, and development (e.g., Ford, Elhai, Connor, & Frueh, 2010; Turner, Finkelhor, & Ormrod, 2010). A national U.S. study showed that 71% of children 2 to 17 years old had experienced at least one type of victimization during the preceding year (Finkelhor, Ormrod, Turner, & Hamby, 2005). Studies in Europe and Asia indicated a similar high prevalence of child victimization. For example, two thirds of sixth and ninth graders in Finland had experienced at least one type of victimization during the preceding year (Ellonen & Salmi, 2011). Three quarters of 10- to 12-year olds in Malaysia experienced at least one type of maltreatment over their lifetime (Ahmed et al., 2015).
Despite differences in terminology and definition across studies (e.g., “poly-victimization” versus “poly-traumatization”), research evidence demonstrates that the cumulative effects of experiencing multiple types of victimization not only place the victims at high risk of posttraumatic stress disorder (PTSD), major depressive disorder, substance abuse, suicide, delinquency, self-harm behavior, and other violent behavior during their childhood (Ford et al., 2010; Tossone et al., 2015; Turner, Finkelhor, & Ormrod, 2006), but also place the victims at high risk of deleterious physical- and mental-health outcomes in adulthood (Edwards, Holden, Felitti, & Anda, 2003; Felitti et al., 1998). Prior research has shown that children who experience multiple types of victimization tend to have risk factors related to gender (being a boy), family adversity (e.g., having a parent who suffers from substance abuse or mental illness), and family structure (e.g., living with a single parent or a step-parent; Chan, 2013; Finkelhor, Turner, Hamby, & Ormrod, 2011). Moreover, previous studies have indicated that neonatal status and congenital diseases may predispose children to victimization in a variety of contexts (Wei et al., 2017; Wu et al., 2004).
In contrast to the significant body of related emerging studies that address these issues in Western contexts, few studies have examined the combined effects of different types of victimization on children in Chinese societies. Therefore, the aim of the present study is to fully capture the burden of victimization on Taiwanese children by examining two important areas: first, the prevalence and risk factors of multiple types of child victimization in Taiwan, and second, the effects of multiple types of victimization on these children’s mental health and behavior in Taiwan.
Child Victimization in Chinese Societies
Most research examining child victimization in Chinese societies has focused on physical or sexual abuse (e.g., J. Chen, Dunne, & Han, 2004; Ji & Finkelhor, 2015). Few studies have examined and demonstrated the negative effects of dual violence (children’s experience of both their own maltreatment and inter-parental violence) on children’s and young adults’ PTSD, internalizing behaviors, and externalizing behaviors (Chan, Brownridge, Yan, Fong, & Tiwari, 2011; Shen, 2009). The scant studies examining multiple types of victimization in reference to Chinese populations have surveyed only adolescents (i.e., individuals between 12 and 18 years old; Chan, 2013; Dong, Cao, Cheng, Cui, & Li, 2013; Feng, Chang, Chang, Fetzer, & Wang, 2015). Chan (2013) surveyed 18,341 adolescents 15 to 17 years old from six cities in China using the Juvenile Victimization Questionnaire (JVQ) and found that 58.5% of the respondents had experienced preceding-year child victimization (i.e., had experienced at least one type of victimization). Moreover, Chan’s study found that poly-victims (those who had experienced four types of victimization or more) were more likely to exhibit symptoms of PTSD, depression, suicide ideation, self-harm, and poorer health than non-victims and victims of one to three forms of violence. Child victimization was positively associated with being a boy, being older, having siblings, and the location of one’s school. Another study surveyed 3,155 adolescents 12 to 18 years old from one province in China using the JVQ and found that the preceding-year prevalence of child victimization was 66.2% (Dong et al., 2013). They found that adolescents who had experienced poly-victimization (i.e., five types of victimization or more) exhibited more symptoms of depression and anxiety than their non-poly-victimization counterparts. Moreover, poly-victimization was positively associated with younger ages, one-child families, and lower socioeconomic status. One national study (Feng et al., 2015) surveyed 5,236 adolescents 12 to 18 years old in Taiwan and found that the preceding-year prevalence of child victimization was 83% (the aforementioned study used the Chinese version of the International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool: Children’s Home Version). The present study has found, to date, no previous study that examined multiple types of victimization relative to children below 11 years of age in Chinese societies. In other words, in Chinese societies, neither the extent to which younger children experience multiple types of victimization nor the effects that these experiences have on the children are well understood. To bridge this research gap, the present study examines the prevalence of multiple victimization types and their effects on children below 11 years of age in Taiwan.
Child Victimization and Child Protection
Much is known about the damage that children suffer after they experience multiple types of victimization in Western contexts; however, little is known about whether poly-victimized children receive child protective services. Previous Western studies have found that many child-maltreatment cases are not identified, reported, or responded to by professionals in various child-protection systems (Gilbert et al., 2009). Western researchers have estimated that only one out of every 30 cases of child physical maltreatment is recognized in developed countries’ official statistics (Gilbert et al., 2012). In Taiwan, professionals (e.g., social workers, educators, medical workers) are mandated by law and protocol to report child physical, sexual, or psychological abuse (occurring within or outside the family) to county or city governments (e.g., the Protection of Children and Youths Welfare and Rights Act, the Family Violence Prevention Act, Guidelines for Preventing Bullying on Campus). After government officials receive a report, a child-protection social worker will investigate the alleged case, provide services to children and families in need, or remove the child from the home if there is immediate danger to the child’s safety. A prior study in Taiwan revealed that official statistics had been significantly under-estimating child-maltreatment rates in the home (Feng et al., 2015). Moreover, no studies, so far, have examined the child-protection rate and its correlates among children experiencing multiple types of victimization in Taiwan. Hence, another aim of the present study is to examine Taiwan’s child-protection rate and its correlates among children experiencing multiple types of victimization.
Given that children who experience multiple types of victimization can suffer detrimental effects and given that there is a lack of epidemiologic research on multiple types of victimization among younger children in Chinese societies, the present study examines (a) the prevalence and risk factors of multiple types of victimization among children in Taiwan, (b) the child-protection rate and its correlates among children experiencing multiple types of victimization in Taiwan, and (c) the association between the children’s experience of multiple types of victimization and the children’s mental health and behavior outcomes. On the basis of prior research findings, we hypothesize that as the number of types of victimization increases, children will report a greater incidence of posttraumatic and psychiatric symptoms, suicide and self-harm ideation, and violent behavior.
Method
Participants
This study took place in the spring semester of 2014 with 6,233 fourth-grade students (10 to 11 years old) from 314 primary schools. Before the formal data collection got underway in 2014, a pilot study took place in the fall semester of 2013 with 726 fourth-grade students, mainly as a way to test the psychometrics of the measures. Of the sampled schools (N = 34) in the pilot study, 35.3% (n = 12) agreed to participate. Some measures were modified according to not only students’ responses but also the results of the reliability and validity analyses from the pilot study.
The formal sample was proportionately stratified according to each county and each city in Taiwan (19 counties and cities in total, excluding outlying islands). The counties and cities were first divided into urban or rural areas, and districts within each area were randomly selected. All the primary schools in each selected district were invited to participate in the study. There were 2,583 primary schools (213,226 fourth-grade students) in Taiwan in the 2013-2014 academic year (Republic of China Ministry of Education, 2015; excluding outlying islands), and the current study sampled 25% of the total primary schools in Taiwan via stratified random sampling. Of the sampled schools, 49% agreed to participate in this study. At the participating schools (n = 314), 99.9% of the consenting parents’ children agreed to participate, and we collected 6,290 questionnaires in total. Of the 6,290 questionnaires, 57 were invalid and excluded from the analyses (owing mostly to incomplete signatures of either parents or children), so that the valid sample size was 6,233. There were significant geographical differences between participating schools and non-participating schools. The average Northern Taiwanese school-participant rates were lower than the average national school-participant rates, and the average Eastern Taiwanese school-participant rates were higher than the average national school-participant rates.
Procedure
The present study received approval from the Research Ethics Committee of National Taiwan University Hospital before sampling and data collection took place. After sampling the schools for the data-collection process, research assistants contacted the school principals for their consent to the schools’ participation in the study. The schools whose principals agreed to the participation then asked the students to give their parents both a letter explaining the study and a form requesting an informed-consent signature. Children whose parents signed the informed-consent forms brought the forms back to the schoolteachers. Afterward, the research assistants consulted with the teachers to schedule a date for data collection.
Before administering the questionnaires, trained research assistants collected the informed-consent forms and explained the research purpose and procedures to students who had parental written consent, emphasizing the study’s voluntary and confidential nature. Research assistants also informed students of their right to refuse or withdraw their participation at any time. Self-report questionnaires were distributed to consenting students in group sessions, scheduled for times during or outside regular class hours (depending on each school’s preferences). For their participation, children received stationery as a gift.
Measures
Measures included in the self-reporting paper-and-pen questionnaire provided information about demographic and family background, school and violence experiences, current behaviors, PTSD, and psychiatric symptoms. The questionnaire contained other scales and data that were not analyzed in this article. The questionnaire was first sent to a group of seven experts for content-validity examination (four child development scholars, one sociologist, one clinical social worker, one statistician) before the measures were administered to pilot-study participants. Some measures were modified according to experts’ and scholars’ suggestions, as well as to the results of internal consistency and principal component analyses after the pilot study. Psychometrics of these measures were examined again after formal data were collected. It is worth noting that other researchers have used self-report questionnaires to collect data from 10- to 12-year olds regarding violence-victimization experience (e.g., Ahmed et al., 2015; Holt, Finkelhor, & Kantor, 2007).
Child Victimization
This study measured seven child-victimization types (Table 1): physical neglect (four items), psychological violence (four items for father and the same four items for mother), physical abuse (seven items for father and the same seven items for mother), sexual violence (two items), inter-parental violence (two items), bullying (seven items covering verbal, physical, and relational bullying), and community violence (two items). We adopted, modified, and simplified these self-report items from related instruments to suit the participants’ cognitive ability and level of understanding (Furlong et al., 2005; Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998; Runyan et al., 1998; Walsh, MacMillan, Trocmé, Jamieson, & Boyle, 2008; Zolotor et al., 2009). Participants used a 5-point Likert-type scale to rate the frequency at which they had experienced each item in the preceding year. The responses for all items were coded 0 = never, 1 = 1 to 2 times, 2 = 3 to 5 times, 3 = 6 to 10 times, and 4 = more than 10 times. Participants were categorized as children who had experienced a type of victimization if they scored a 1 or more on any scale item, except for the physical-abuse items. This study adopted a conservative algorithm (Definition 2, proposed by Walsh et al., 2008) for categorizing participants as children who had experienced physical abuse (please see physical-abuse items in Table 1). We constructed a summary count of total exposure to these victimization types, with the possible sums ranging from 0 (no victimization) to 7 (experienced seven types). All scales showed adequate internal-consistency reliability for the present sample (from α = .45 for sexual violence to .88 for physical abuse). Regarding the construct validity of the victimization scale, on the basis of the principal component analyses, all the sub-scale victimization items were grouped together into eight factors consistent with this study’s typology of victimization (the physical-abuse items were grouped into two factors: fathers’ and mothers’ violence toward children). All the victimization items explained 58.7% of the total variance.
Type and Percentage of Victimization Items Among Fourth Graders in Taiwan in 2014 (n = 6,233).
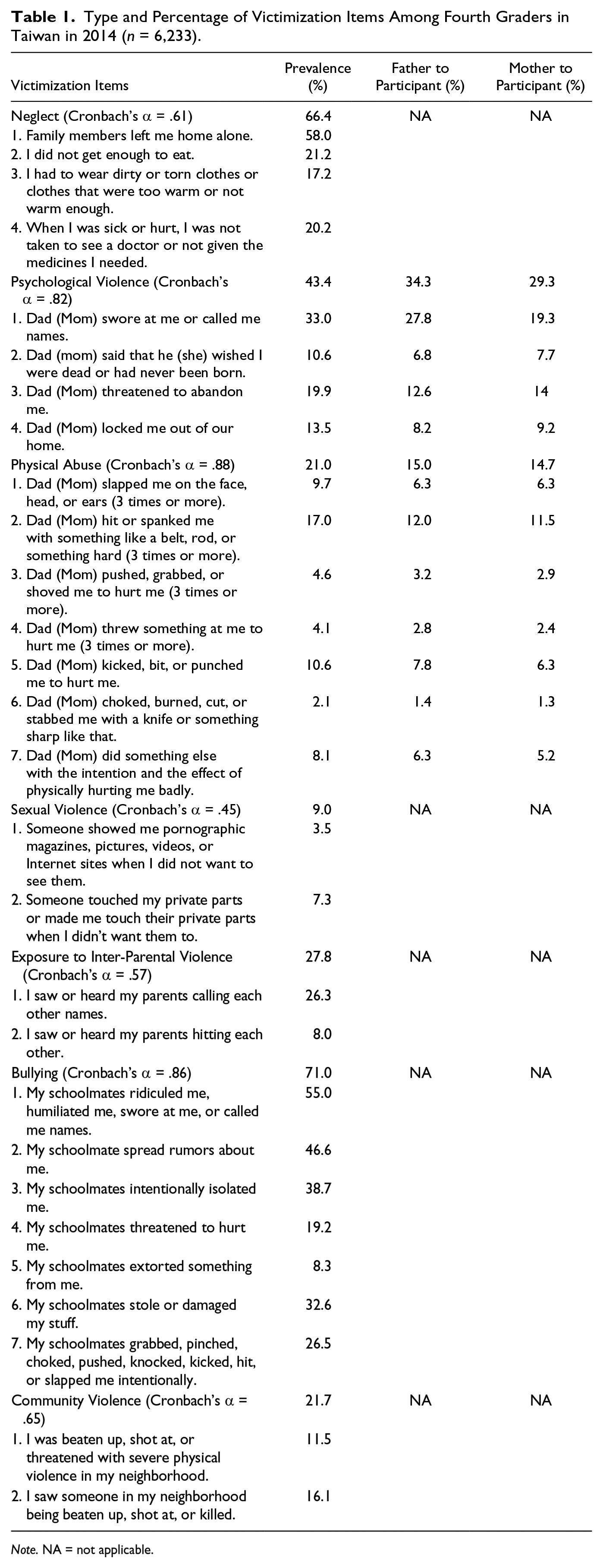
Note. NA = not applicable.
PTSD
The Chinese version of the University of California at Los Angeles Post-traumatic Stress Disorder Reaction Index (UCLA PTSD-RI) for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994; adolescent version; Part III) measures traumatic-experience symptoms to provide preliminary PTSD diagnoses using DSM-IV criteria (Chen, Lin, Tseng, & Wu, 2002; Steinberg, Brymer, Decker, & Pynoos, 2004). Participants used a 5-point Likert-type scale (from 0 = none of the time to 4 = most of the time) to rate the frequency at which they had experienced each symptom during the previous month. These items map directly onto the DSM-IV Criterion B (intrusion), Criterion C (avoidance), and Criterion D (arousal) for PTSD. The following items are sample statements for each criterion: “Upsetting thoughts, pictures, or sounds of what happened come into my mind when I do not want them to” (intrusion); “I try not to talk about, think about, or have feelings about what happened” (avoidance); “I have trouble going to sleep or I wake up often during the night” (arousal). To reduce the time that children would need to complete the questionnaires, we deleted five alternatively worded items (Items 11, 14, 20, 21, 22) from the original scale according to the pilot study’s factor-analysis results. Therefore, the current study features only 17 items. The total computed score combines all 17 responses. Higher scores reflect greater posttraumatic-symptom severity. A cutoff of 38 has a sensitivity of 0.93 and specificity of 0.87 in detecting PTSD (Rodriguez, Steinberg, Saltzman, & Pynoos, 2001). Several previous Western studies reported strong internal consistency (Cronbach’s alpha around .90) and test–retest reliability (between .84 and .93) across UCLA PTSD-RI versions (Steinberg et al., 2004). In Taiwan, the Chinese adolescent version of the UCLA PTSD-RI has been used with children and adolescents who experienced earthquakes (fourth to ninth graders; α = .91) and college students who experienced family violence (α = .94), and has exhibited strong internal consistency (Chen et al., 2002; Shen, 2009). The PTSD Scale exhibited good internal-consistency reliability for the present sample (α = .89).
Psychiatric symptoms and suicidal ideation
We used the Brief Symptom Rating Scale (BSRS-5; Lee et al., 2003), a common screening tool in Taiwan, to assess participants’ psychiatric symptoms in the previous week. The scale contains five items measuring anxiety, hostility, depression, inferiority, and insomnia. An additional sixth item asked the participants about their suicidal ideation, which was scored separately from the scale and measured as an outcome variable. The score for each item ranged from 0 to 4 (0 = not at all, 1 = a little bit, 2 = moderately, 3 = quite a bit, and 4 = constantly). Higher scores reflect greater psychiatric-symptom severity. A cutoff of 6 has a sensitivity of 0.79 and specificity of 0.74 in detecting psychiatric morbidity (Lee et al., 2003). Previous studies reported good internal consistency (between .77 and .90), test–retest reliability (.82), and concurrent validity (ranging from .87 to .95) among psychiatric patients and community samples comprising people between 15 and 60 years old (Lee et al., 2003). The BSRS-5 exhibited good internal-consistency reliability for the present sample (α = .84).
Self-harm and violent behaviors
We selected two items from the Child’s Developmental History Questionnaire (Garber, 2012) to measure children’s self-harm thoughts and violent behaviors as outcome variables (yes or no questions). Participants were categorized as having self-harm thoughts or violent behaviors if they answered yes to either item.
Child protective services
We used one item to ask children whether they had ever received child protective services from social workers (yes or no question). Participants were categorized as receiving child protective services if they answered yes to this item.
Risk factors
In the analyses, several additional measures were examined as both risk and confounding factors, covering gender, neonatal status, parental marital status, and other family risks. We used one self-report item to assess the neonatal status of children. The participating children could select any of four responses regarding neonatal status: normal birth, premature birth, low birth weight, and congenital disease. Each item response was coded 1 = yes or 0 = no. Participants were categorized as having had a normal birth status, as having been prematurely born, as having had a low birth weight, or as having had a congenital disease if the corresponding response was coded yes.
We used six items in the Family Health History & Health Appraisal Questionnaire (Centers for Disease Control and Prevention, 2005) to examine other family risks that might affect children’s mental health and behavior. Participants were asked whether or not a parent or a sibling had experienced the following stressors: alcoholism, drug abuse, gambling, a suicide attempt, mental illness, or imprisonment (yes or no questions). We calculated total exposure to these family risks. Higher scores indicate greater exposure to other family risks (scores’ possible range is 0-18).
Statistical Analyses
We conducted (a) chi-square analyses to test the association between children’s experience of multiple victimization types and related risk factors, (b) logistic-regression analyses to examine the correlates of receiving child protective services, (c) ANOVAs to examine the association between children’s experience of multiple victimization types (the independent variable) and the children’s mental health (the dependent variable), and (d) logistic-regression analyses to examine the cumulative effects of multiple victimization (the independent variable) on self-harm and violent behaviors (the dichotomous dependent variables) while adjusting for potential confounding factors. SPSS 21 was used for statistical analyses.
Results
Participant Characteristics
The participants’ gender ratio was approximately 1:1 (boys: 50.3%). Most participants had siblings (85%), while 13.3% of the participants were the only child (1.7% had missing data). Most participants’ parents were married (83.5%), 13.7% of the parents were divorced, and 1.7% were “other status,” including widowed and remarried. Finally, 74.3% of the participants’ fathers and 70.8% of the participants’ mothers were high school graduates.
Prevalence and Risk Factors
For this study, we calculated the 1-year prevalence of seven child-victimization types (Figure 1): Bullying was the most prevalent (71%), followed by physical neglect (66%), psychological violence (43%), exposure to inter-parental violence (28%), community violence (22%), physical abuse (21%), and sexual violence (9%). Correlation analyses show that all types of victimization were inter-correlated at the .01 level (two-tailed), ranging from r = .111 for physical neglect and sexual violence (p < .001) to r = .383 for psychological violence and inter-parental violence (p < .001; the correlation table is not shown in this article). With the exceptions of bullying and exposure to inter-parental violence, male participants reported a significantly higher prevalence of all types of victimization than did female participants at the .01 level.

Percentage of children experiencing each type of victimization and percentage of children receiving child protective services for each type of victimization involving fourth graders in Taiwan in 2014 (n = 6,233 for type of violence experienced).
Of the participants, 41% had experienced one or two types of victimization during the past year; 32.6% had experienced three or four types of victimization during the past year; and 15.4% had experienced five or more types of victimization during the past year. The participants had experienced a median of two types of victimization (M = 2.6). Male participants reported experiencing more types of victimization than female participants (boys’ M = 2.8; girls’ M = 2.4; t = 7.6, p < .001).
Table 2 presents the number of victimization types by demographic characteristics and associated factors. Chi-square analyses reveal that the more victimization types a child experienced, the likelier the child was to be a boy, to have been born with an abnormal status, to have divorced parents, and to face high levels of other family risks. For example, of the children with no victimization, 82.2% had been born with a normal status; by contrast, of the children who had experienced all seven types of victimization, only 58.7% had been born with a normal status. The number of victimization types a child experienced was not associated with children’s birth order. There were no gender differences in PTSD, psychiatric symptoms, suicidal ideation, and self-harm variables. Male participants reported a higher prevalence of violent behaviors than female participants did (t = 8.2, p < .001).
Percentage and Mean Scores of Participants’ Characteristics and Outcome Variables According to the Number of Victimization Types Among Children in Taiwan in 2014.
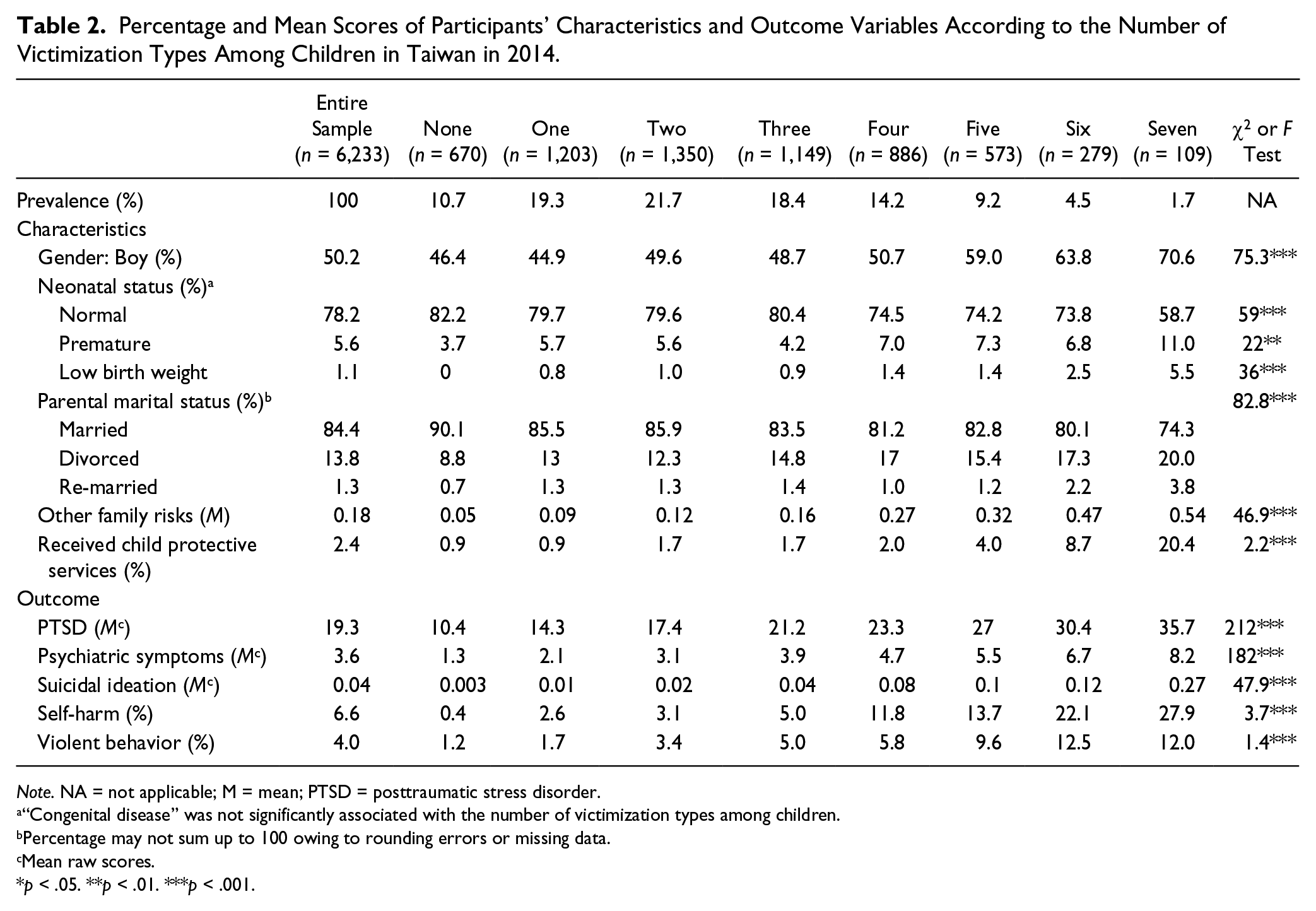
Note. NA = not applicable; M = mean; PTSD = posttraumatic stress disorder.
“Congenital disease” was not significantly associated with the number of victimization types among children.
Percentage may not sum up to 100 owing to rounding errors or missing data.
Mean raw scores.
p < .05. **p < .01. ***p < .001.
Child-Protection Rate and Correlates
Only 2.4% (n = 148) of the participants reported having received child protective services. Of the protected participants, 56.8% were boys, and 68.2% of them had been born with a normal status. Of the protected participants’ parents, 66.9% were married, and 25.7% were divorced. On average, the participants receiving child protective services had experienced four types of victimization.
Although bullying was the most prevalent type of victimization among fourth graders in Taiwan, bullying victims reported the lowest child-protection rate (2.8%) among all types of victimization victims (Figure 1). By contrast, although sexual violence was the least prevalent type of victimization among fourth graders in Taiwan, sexual-violence victims reported the highest child-protection rate (8.6%) among all types of victimization victims. Chi-square analyses (Table 2) reveal that the more victimization types a child experienced, the likelier the child was to receive child protective services. Specifically, 20.6% of the children who had experienced all seven types of victimization had received child protective services. By contrast, only 0.9% of the children who had experienced one type of victimization had received child protective services. Moreover, logistic analyses (Table 3) show that a child was more likely to receive child protective services if he or she had experienced sexual violence, community violence, inter-parental violence exposure, higher family risks, higher suicidal ideation, or living in a single-parent or separated family.
The Significant Correlates (Identified by Logistic Regression) of Children Receiving Child Protective Services in Taiwan in 2014 (n = 6,233).

Only significant correlates were presented in this table. Non-significant variables included bullying, physical abuse, psychological violence, neglect, gender, birth status, PTSD, psychiatric symptoms, self-harm thoughts, and violent behavior.
Reference group = a family headed by a married and living-together couple.
p < .05. **p < .01. ***p < .001.
Effects on Mental Health
Figures 2 through 4 clearly illustrate the cumulative effects that children’s experience of multiple types of victimization can have on the children’s mental health. With each additional type of victimization experienced, children reported a linear increase in PTSD, psychiatric symptoms, and suicidal ideation. Least significant difference (LSD) post hoc tests revealed significant mean differences across victimization types for PTSD, psychiatric symptoms, and suicidal ideation at the 0.01 level, with a few exceptions (zero vs. one, zero vs. two, one vs. two, and four vs. five types for suicide ideation). Experiencing six or more types had the group mean of more than six (cutoff) on the BSRS-5 for detecting psychiatric morbidity (Table 2). The ANOVA analyses support the cumulative-effect hypothesis that as the number of types of victimization increases, children will report higher levels of posttraumatic symptoms, psychiatric symptoms, and suicide ideation.
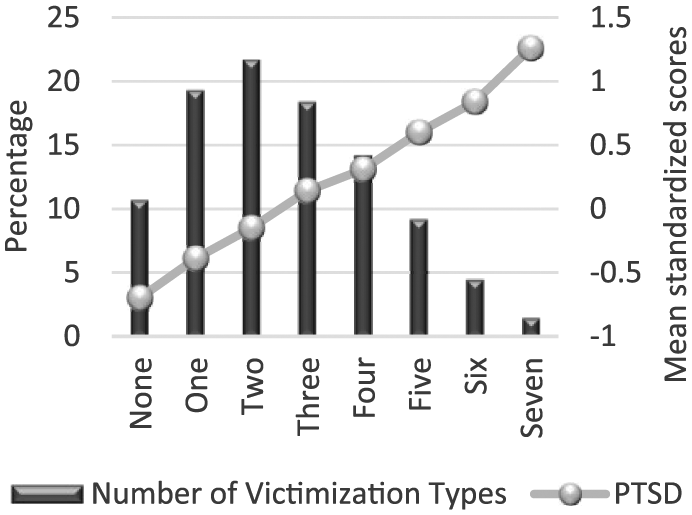
PTSD scores by total number of victimization types among fourth graders in Taiwan (n = 6,214).

Psychiatric-symptom scores by total number of victimization types among fourth graders in Taiwan (n = 6,196).

Suicidal-ideation scores by total number of victimization types among fourth graders in Taiwan (n = 6,184).
Effects on Behavior
Table 4 shows the results from the logistic-regression analyses modeling self-harm thoughts and violent behavior (with risk factors controlled for). For every additional victimization type, the odds of self-harm thoughts increased by between 5.8 and 72 times. The presence of two or more victimization types versus no victimization type significantly increased the odds that children would report violent behaviors by between 2.8 and 8.5 times. The logistic-regression analyses support the independent- and cumulative-effect hypothesis that, in general, as the number of types of victimization increases, children will report a greater incidence of self-harm and other violent behavior.
The Association (Identified by Logistic Regression) Between the Number of Victimization Types Among Children and Their Harmful Behavior in Taiwan in 2014.

Reference group = no victimization.
Adjusted for gender, parental marital status, birth status (normal or not), other family risks.
p < .05. **p < .01. ***p < .001.
Discussion
In the present study, we used a large and national population-based sample to investigate both the prevalence of child victimization and child-protection rates. We reveal that the preceding-year prevalence of victimization among fourth graders in Taiwan was 89.2%. This prevalence rate is slightly higher than a recent Taiwan-based study involving an adolescent sample (12-18 years old), showing 83% preceding-year prevalence (Feng et al., 2015). These prevalence differences probably reflect our assessment of bullying as a distinct type of victimization, which was not measured in the other Taiwan-based study. If we discount bullying as a type of victimization, the prevalence rate will drop to 79.7%. The high prevalence of self-reporting victimization among children contrasts sharply with the 0.26% official rate of substantiated child-abuse cases (0-18 years old) in Taiwan in 2014 (Republic of China Ministry of Health and Welfare, 2015). Although Taiwanese law mandates that professionals in the relevant fields should report cases of child maltreatment, the present findings are alarming because of the severity of under-reporting in child-victimization cases. Moreover, we found that only 2.4% of the participants had received child protective services. Even for children who had experienced all seven types of victimization, the majority of them (79.4%) did not receive child protective services. These findings suggest that there is a high level of unrecognized need of protection among victimized children and that neither high-risk nor low-risk children are adequately served. These findings echo those of previous Western studies showing that many child-maltreatment cases are not recognized, reported, or protected by professionals in various child-protection systems (Gilbert et al., 2009).
The present study’s findings demonstrate the detrimental and cumulative effects that children’s experience of multiple types of victimization can have on the children’s mental health and behavior. We found that, among the Taiwanese children, experiencing a high number of victimization types leads to high levels of psychiatric morbidity and high risks of harming behaviors. These findings corroborate prior research (Chan, 2013; Ford et al., 2010; Turner et al., 2010), revealing that children’s experience of multiple types of victimization can have more severe combined effects on the children than can children’s experience of either no victimization or only one form of victimization. In addition, our findings show that participating children who were boys, who had divorced parents, or who faced significant family risks were significantly more likely to be associated with a high number of victimization types than were the participating children who did not fall into one or more of these three categories. These findings corroborate prior research (Dong et al., 2013; Finkelhor et al., 2011). The strong association between child victimization and family instability or family risks (e.g., parental mental-health illness, parental substance abuse) emphasizes the need for professionals to consider the well-being of the family when dealing with child-victimization problems.
A unique finding of this study is that neonatal status was significantly associated with children’s experience of multiple victimization types: Specifically, abnormal, preterm, and low-birth-weight neonatal statuses were significantly related to elevated numbers of victimization types in children. Prior research has identified neonatal status as a risk factor for infant maltreatment (Wu et al., 2004). This noteworthy finding suggests that neonatal status may predispose infants to not only child abuse but also multiple types of victimization in middle childhood.
The current study found that bullying was the most prevalent type of victimization among fourth graders in Taiwan. The preceding-year prevalence of bullying found in this study (71%) was comparable with previous findings based on adolescent samples in the United Kingdom (75%; Glover, Gough, Johnson, & Cartwright, 2000) and in Taiwan (55% within a 3-month time period; Wei, Jonson-Reid, & Tsao, 2007). Although bullying is prevalent in Taiwan, it did not become an urgent issue until several incidents involving peer-group violence surfaced and caused public furor in 2010 (Hsu, 2011). Consequently, the government in 2012 announced a set of formal anti-bullying rules (Guidelines for Preventing Bullying on Campus). It is nevertheless the case that, in Taiwan, professionals have only just begun to learn how to identify and intervene in bullying cases.
Study Limitations
This study’s findings are limited because of its cross-sectional nature and its single-source data collection, which involved retrospective self-reporting measures. Causal relationships cannot be determined, and results cannot be generalized to children who are not in the fourth grade and who did not participate in this study. The retrospective-study method itself is subject to recall errors and memory inaccessibility for traumatic abuse. The single-source data were not verified by other informants. Moreover, there may be covariates not controlled by this study. Finally, half of the sampled schools did not participate in this study mainly because schools in Taiwan are invited to participate in various kinds of surveys rather frequently. Some schools have decided to refrain from participating in any study unless it is required by the government: The rationale behind this decision generally involves an effort to avoid overburdening teachers’ workloads. Moreover, most schools in Northern Taiwan are geared toward accelerated academic performance and tend to frown upon any school-time activity that detracts from their students’ academics: This fact heavily accounts for the significantly lower participation rate in northern cities. After identifying the schools’ reasons for refraining from participation in our pilot study, we asked the city and county governments to issue an official document encouraging the schools to participate in the formal study. The formal encouragement increased the school-participation rate from 35.3% for the pilot study to 49% for the formal study. Although not all the sampled schools participated in the present study, a quite satisfactory total of 314 schools (covering each of Taiwan’s counties and cities) participated in the present study, notably strengthening the diversity of the sample.
Research Implications
The present study offers significant evidence that children’s experience of multiple types of victimization is prevalent in Chinese society. The findings highlight the need to incorporate diverse populations into the growing literature on multiple types of child victimization. Future studies can further explore this issue from cultural perspectives, paying special attention to risk and protective factors affecting children who experience multiple types of victimization. In addition, future studies can collect data from other types of informants (e.g., parents, teachers) to verify children’s data. In this regard, a prior study conducted in Taiwan showed that children reported less family violence than did their parents (Shen, 2006).
Clinical and Policy Implications
The apparent and harmful effects that children’s exposure to multiple types of violence can have on the children underscore the need to develop effective identification, assessment, and intervention available to children confronting the perils of victimization. Prevention can start as early as a child is born with risk factors, such as non-normal birth status, single-parent families, and families with a history of crime, mental health, and drug abuse. For example, some U.S. home-visitation programs targeting prenatal months and early childhood exhibited promising long-term effects in reducing child abuse and neglect by promoting parental child–health care skills, improving parent–child interaction, strengthening home safety, and linking parents to community-based resources (Chaffin, Hecht, Bard, Silovsky, & Beasley, 2012; Olds et al., 1997). Interventions should minimize the number of victimization types that children experience, with the goal of maximizing the children’s mental-health outcomes. Moreover, children experiencing six or more types of victimization should be given priority in receiving service or intervention because they are at a higher risk of developing psychiatric morbidity, as the present findings show.
Conclusion
The present study is the first national epidemiologic study to use a large sample in comprehensively examining children’s victimization across settings in Taiwan. Hence, this study’s population survey provides the first available national estimates regarding various types of victimization. The present research findings add to the growing knowledge of poly-victimization by extending research to the understudied populations of Chinese children and by examining the extent of child protection for poly-victimized children. The present findings raise alarms regarding the severity of under-reporting and under-serving in child-victimization cases. Educators, social workers, medical workers, and other workers who are charged with looking after children must rigorously identify and assess victimized children to fully protect them from harm in families, schools, and communities.
Footnotes
Acknowledgements
The authors would like to thank all the schools, parents and students who participated in this study.
Authors’ Note
The first author is the principal investigator, who initiated and conducted this study when she served as the CEO of the National Taiwan University (NTU) Children and Family Research Center. The second author is the director of the NTU Children and Family Research Center. The other authors are the co-principal investigators of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Taiwan University (NTU) Children and Family Research Center.