
Abstract
The purpose of this study was to identify characteristics of investigations of sexual abuse concerning vulnerable adults residing in facility settings that were associated with case substantiation. Data on 410 reports of sexual abuse were collected prospectively from Adult Protective Services (APS) and state licensure agency staff in New Hampshire, Oregon, Tennessee, Texas, and Wisconsin over a six-month period. Specifically, we examined differences between reports that were substantiated and those that were not by comparing characteristics of alleged victims, alleged perpetrators, and aspects of investigation using logistic regression. We found that a relatively low proportion of cases (18%) were substantiated overall. Compared to cases that were not substantiated, cases that were substantiated were more likely to feature nursing home residents, older victims, female victims, and allegations of physical contact between the alleged perpetrator and victim. Despite the high proportion of alleged perpetrators who were facility staff (51%) compared to resident perpetrators (25%), cases with resident-to-resident allegations of abuse were much more likely to be substantiated, accounting for 63% of substantiated cases. In light of these findings, we believe it is important that investigators are trained to handle sexual abuse cases appropriately and that they are able to investigate the case thoroughly, promptly, and with as much information as possible. It is also critical that investigators make substantiation decisions using the appropriate standard for confirmation (e.g., preponderance of the evidence, beyond a reasonable doubt, clear and convincing evidence) as state law dictates.
Keywords
Introduction
Because of the potentially traumatic nature of sexual abuse on vulnerable adults and its potential to have a lasting negative impact on its victims, it is imperative that investigation, identification, intervention, and prevention efforts be conducted appropriately and in a timely manner. The purpose of this study was to understand the nature of sexual abuse concerning vulnerable adults residing in facility settings whose cases were investigated by Adult Protective Services (APS) and state licensure agencies. Specifically, we examined differences between reports that were substantiated (i.e., allegations that met the legally set standard of evidence, which is typically more than 50% or the “preponderance standard” for APS and regulatory agencies) and those that were not. The authors stress that unsubstantiated cases did not necessarily constitute false allegations, but rather, in the opinion of the assigned investigator and following applicable regulations and other protocols, not enough evidence existed to substantiate the allegations.
According to the National Center on Elder Abuse (NCEA), sexual abuse is defined as “non-consenting sexual contact of any kind” (NCEA, 1995). It includes, but is not limited to, unwanted touching; sexual assault or battery, such as rape, sodomy, and coerced nudity; sexually explicit photographing; and sexual contact with any person incapable of giving consent. Easily the most hidden form of mistreatment, sexual abuse constitutes less than 1% of all cases reported and substantiated by APS, which is the state agency that usually first receives such reports of mistreatment perpetrated against vulnerable adults (Acierno et al., 2010; Daly & Jogerst, 2014; Ernst & Smith, 2012; Lifespan of Greater Rochester et al., 2011; NCEA, 1995; Tatara, 1993; Teaster et al., 2006; Wangmo et al., 2014). Researchers and practitioners alike suggest that reported cases grossly underestimate actual incidence. Older and vulnerable younger adult sexual abuse cases require complex intervention efforts because of their especially intimate nature (Brozowski & Hall, 2010).
Men and women with physical, cognitive, or emotional disabilities may be at increased risk for abuse, and those living in residential or long-term care settings (e.g., nursing homes, assisted living facilities, group homes) are especially vulnerable because in addition to physical limitations, they may not only experience dementia or other cognitive impairments but also are more often dependent on others for care (Rosen, Lachs, & Pillemer, 2010). There are no prevalence and incidence studies of sexual abuse of vulnerable adults in these settings. However, in earlier studies, the National Ombudsman Reporting System (NORS) revealed that in a 2-year period there were more than 1,700 complaints of alleged sexual abuse of nursing home residents (Hawes, 2003), and a General Accounting Office (GAO) report concerning investigations of 158 allegations of physical and sexual abuse identified intolerable rates of sexual abuse of nursing home residents (U.S. GAO, 2002).
Background
Theoretical Approach
Studies on the abuse of vulnerable adults often lack a theoretical framework from which to understand precursors and outcomes of an adult’s experiences with sexual abuse. Scholars from the fields of disability (Curry, Hassouneh-Phillips, & Johnston-Silverberg, 2001) and gerontology (Kosberg & Nahmiash, 1996; Reilly & Gravdal, 2012; Schiamberg & Gans, 2000; Teaster, Roberto, & Dugar, 2006) propose a socio-ecological model for understanding abuse. The ecological model states that an individual is embedded in a series of interacting environmental systems (Bronfenbrenner, 1986; Horsford, Parra-Cardona, Post, & Schiamberg, 2011; Wangmo et al., 2014) (Figure 1). Applied to sexual abuse, the model provides a focus on characteristics of vulnerable adults and four nested systems: (a) the microsystem, or the immediate context in which the abuse takes place (e.g., resident and residential setting); (b) the mesosytem, or the relationship between the adult and the abuser (e.g., fellow resident, staff member); (c) the exosystem, or environments external to the adults (e.g., APS, state licensure, investigation issues) that may affect residents’ well-being; and (d) the macrosystem, or broad ideological values, norms, and institutional patterns of a particular culture (Roberto & Teaster, 2005; Schiamberg & Gans, 2000). This study examines the intersection of the microsystem, the mesosystem, and the exosystem.

The socio-ecological framework for elder mistreatment.
Literature Review
What is known about older and vulnerable adult sexual abuse is that it generally constitutes a small but significant proportion of total abuse cases reported in residential care settings. Studying 488 incidents of abuse in nursing homes using Medicaid Fraud Reports from 42 states over 5 years, Payne and Cikovic (1995) found that 8.8% involved cases of sexual abuse (4% were under 59 years of age). Teaster et al. (2006) reported that in 2004, APS received 565,747 domestic and institutional reports of the mistreatment of vulnerable adults, which included 5,797 (1.0%) allegations involving sexual abuse. Because APS does not have the authority to investigate alleged facility abuse in all states, this number underestimates the reported sexual abuse cases in residential care facilities.
Research indicates that sexual abuse of vulnerable adults in residential care settings primarily involves female victims and male perpetrators (Baladerian, 1991; Brown, Stein, & Turk, 1995; Payne & Cikovic, 1995; Rosen et al., 2010; Sobsey & Doe, 1991; Teaster, Roberto, Duke, & Kim, 2001), but male victims (Brown et al., 1995; Payne & Cikovic, 1995; Teaster et al., 2007; Roberto, Teaster, & Nikzad, 2007) and female perpetrators should not be discounted. Victims can experience physical injuries, sexually transmitted infections, and psycho-social trauma (Burgess, Dowdell, & Prentky, 2000). Impaired cognition and physical disability (Furey, Niesen, & Strauch, 2006) as well as advanced age (Brozowski & Hall, 2010) serve to isolate the resident victim as well as put him or her at heightened risk for sexual abuse.
Though isolated by comorbid conditions, resident victims often have a relationship with the perpetrators who abuse them (Brown et al., 1995); perpetrators may be family members, paid care providers, and fellow residents (Furey et al., 2006; Ramsey-Klawsnik et al., 2008; Rosen et al., 2010; Teaster et al., 2001). Because the perpetrators may have a relationship with the resident, facility staff members may be unprepared to deal appropriately with sexual abuse allegations, as they, too, may have a relationship with the perpetrator. For instance, Burgess et al. (2000) noted a “lack of sensitivity of nursing home staff to the gravity of the assaults on the residents” (p. 17) in their study of sexual abuse comprising 20 nursing home residents. Further, cases involving resident perpetrators are substantiated more often than non-resident accused perpetrators (Ramsey-Klawsnik et al., 2008). Consequently, perpetrators in sexual abuse cases are rarely prosecuted and convicted (Hodell et al., 2009; Ramsey-Klawsnik et al., 2008; Roberto et al., 2007; Teaster et al., 2001).
Most prior studies are limited due to their small sample sizes such that most did not have adequate statistical power. Specifically, studies have relatively low numbers of cases, limited sources of data (i.e., often involving a single state), and a paucity of studies involving adults who experience cognitive impairments. These factors limit the generalizability of the results. Also lacking are multi-state studies using prospective, systematic data collection of the sexual abuse of vulnerable adults residing in multiple types of facilities as well as of existing investigatory processes and documentations of service provision. Generalizable data emanating from more than one state are critically needed to inform prevention, reporting, investigation, and intervention measures across the country, especially because of the few studies that focus on this problem and the limitations of the resultant findings. This study, which informs both future researchers and practitioners, helps fill this research gap because it presents prospective multi-state data on sexual abuse of facility residents.
Design and Methods
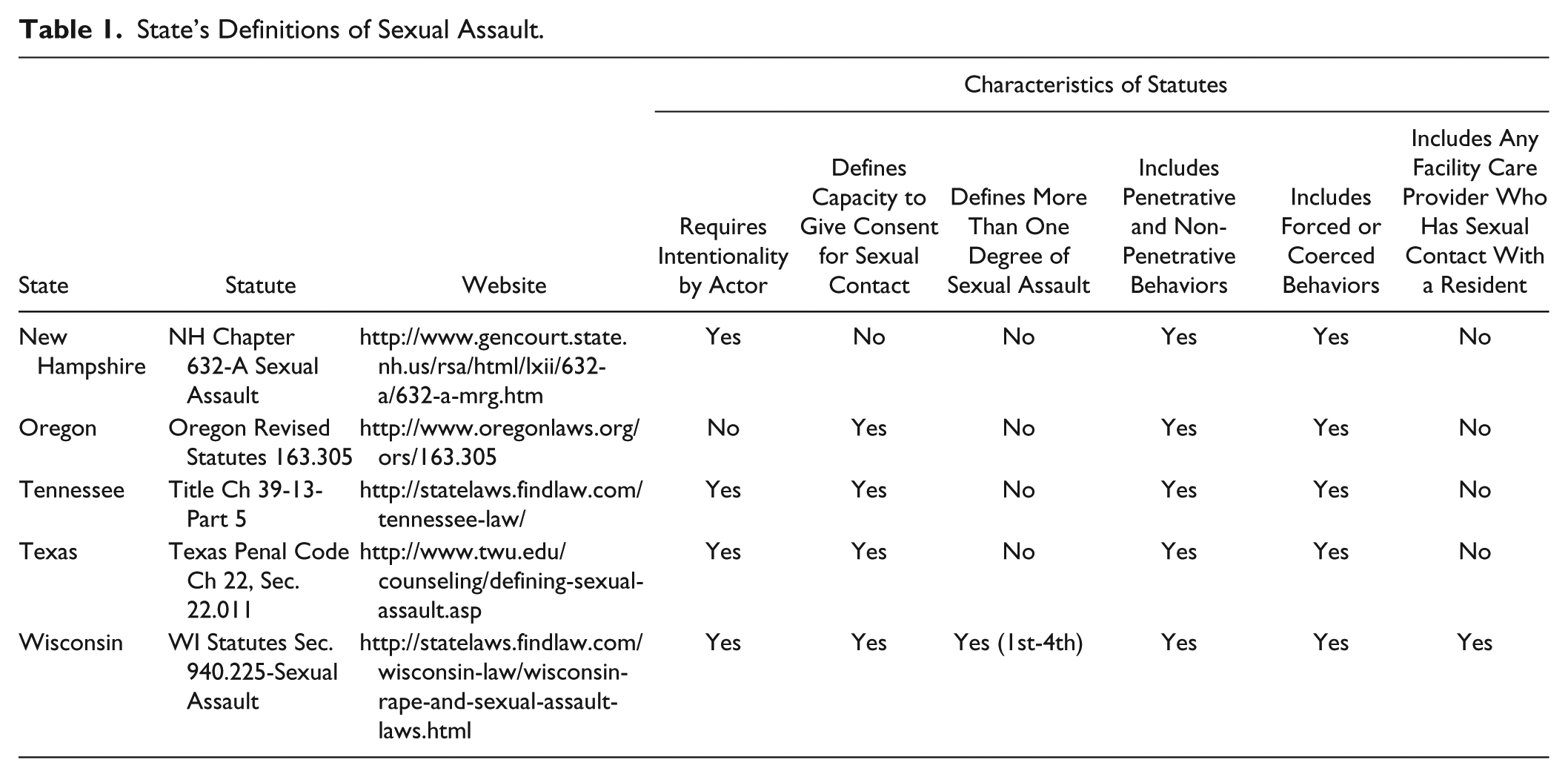
The Sexual Abuse of Vulnerable Adults in Institutions study collected prospective data on all reported sexual abuse allegations involving victims 18 years of age and older living in residential care facilities reported to APS and other long-term care investigatory agencies in New Hampshire, Oregon, Tennessee, Texas, and Wisconsin over a 6-month period in 2005. A case was classified as sexual assault and therefore appropriate for inclusion in our study if under the statutes and regulations for each state a behavior was classified as such, as detailed in Table 1. Details on study design and methods have been previously reported (Ramsey-Klawsnik et al., 2008). Case investigators or designated agency staff submitted completed study data collection instruments based on sexual abuse allegations that were reported to the state agencies between May 1 and October 31, 2005. De-identified data were collected on alleged victim characteristics (including age, ethnicity, gender, diagnoses and disabilities experienced, activity of daily living impairments, level of orientation), alleged perpetrator characteristics (including age, ethnicity, gender, relationship to the alleged victim, diagnosed disabilities experienced), facility type (such as nursing home, assisted living facility, state mental hospital, etc.), sexual and other types of abuse allegations (such as neglect, physical and/or emotional abuse), forensic markers of abuse (such as presence of bleeding, bruising, other physical injury, sexually transmitted disease), investigation procedures (including specific agencies that conducted investigations, number of hours spent in investigation, if alleged victim and alleged perpetrator(s) and witnesses were interviewed), and substantiation decisions and rationales. All research activities were approved by the University of Kentucky Institutional Review Board.
State’s Definitions of Sexual Assault.
Mentioned above, data elements collected were situated within the microsystem, mesosystem, and exosystem levels of the ecological theoretical framework. The study examined suspected sexual abuse cases of vulnerable adults residing in care facilities to determine the number and types of allegations reported as well as signs and symptoms of possible abuse that triggered case reporting. Cases did not have to originate as sexual abuse allegations; sexual abuse allegations could be discovered through the process of investigating other allegations, such as neglect. As specified above, also collected and analyzed were victim and perpetrator characteristics, abuse specifics (e.g., type of abuse alleged and substantiated and the degree of assault), impact of sexual assault on the victim, and circumstances correlated with sexual assault in residential care facilities, investigation steps taken to determine how suspected sexual abuse cases in facilities were investigated, the rate of case substantiation, and rationales for substantiation decisions.
Statistical Analysis
Alleged victim, perpetrator, facility, and investigation characteristics were examined with descriptive statistics for all reported victims and by substantiation status (yes vs. no). To facilitate analysis, the research team classified the care facilities into three categories by estimated level of supervision provided to the residents. From highest to lowest level of supervision, the categories included (highest) acute care hospital, state school, state mental hospital, community mental health/mental retardation facility, intermediate care facility for mental retardation or related condition; (moderate) skilled nursing facility, assisted living facility, rehabilitation center/enhanced care facility; and (lowest) adult family home, adult foster home, community-based residential program/facility, group home, residential care facility/apartments.
Crude (unadjusted) differences between substantiation groups were assessed with t tests and Pearson chi-square tests. Logistic regression was used to estimate the relative adjusted effect of variables (i.e., adjusted for the effect of all other variables in the model) associated with the probability of substantiation of sexual abuse. Variables that were significantly different at the 0.10 level between substantiated and unsubstantiated cases in the bivariate analysis were selected for inclusion in the regression model. Victim age was centered at the sample median, and with the exception of number of activities of daily living (ADL) impairments, all other variables were entered into the model as indicators. The initial analysis was restricted to main effects. In light of the wide range of victim ages, two-way interactions between victim age and all other variables in the model were assessed. Interactions significant at the 0.10 level were retained. Data were analyzed using SAS/STAT® 9.3 (SAS Institute, Cary, NC) statistical software.
Missing Data
A large proportion of case reports (28%) reported that the time between when the alleged sexual abuse incident occurred and the time when it was reported was unknown. Thus, the regression analysis was conducted without this variable and then repeated on the subset of cases where it was known.
Results
Participating agencies submitted reports on 438 cases of sexual abuse. Nine cases were reported to the investigating agency outside the study period and were excluded from further analysis. From the remaining 429 cases, five contained allegations that did not identify a specific victim, and an additional 14 did not report the age of the alleged victim. These cases were also excluded, leaving 410 cases of alleged victims of sexual abuse for analysis (Table 2). Of the 410 cases, sexual abuse allegations were substantiated by the investigating agency in 72 cases (17.6%). At the time of the investigation, the mean age of all alleged victims was 49.8 ± 22.5 years (median 46 years), and 61% were female (Table 2).
Victim, Perpetrator, and Investigation Characteristics by Sexual Abuse Allegation Substantiation Status.
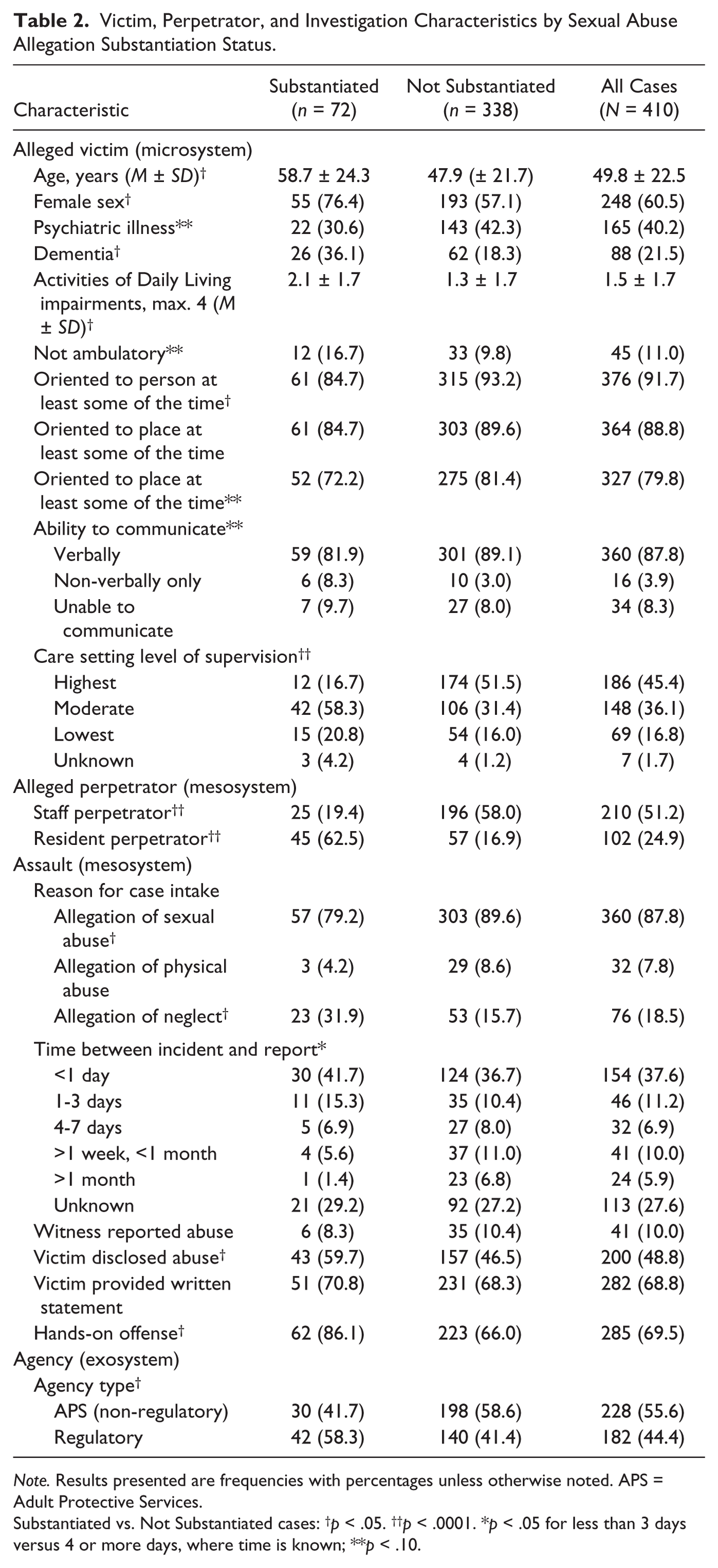
Note. Results presented are frequencies with percentages unless otherwise noted. APS = Adult Protective Services.
Substantiated vs. Not Substantiated cases: †p < .05. ††p < .0001. *p < .05 for less than 3 days versus 4 or more days, where time is known; **p < .10.
Bivariate Analyses
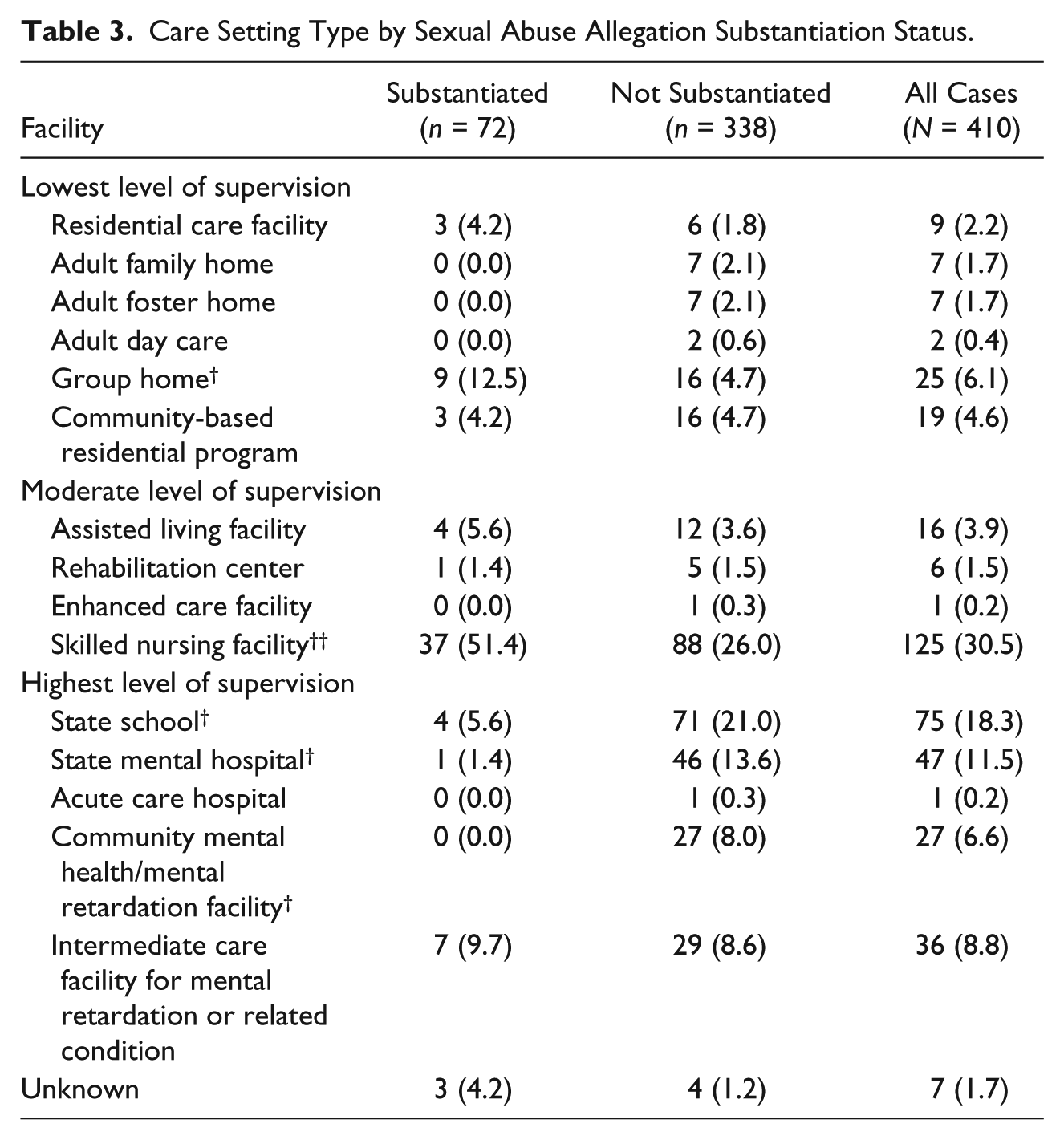
Victims in substantiated cases were older than victims in unsubstantiated cases (58.7 vs. 47.9, t408 = 3.8, p = .0002) and disproportionately female (76.4% vs. 57.1%, χ2 = 9.2, p = .0024). Victims in substantiated cases had more activities of daily living impairments (Δ = 0.8 ± 1.7, t408 = 3.4, p = .0002), were more likely to have dementia (χ2 = 11.1, p = .0009), and were less likely to be oriented to person at least some of the time (χ2 = 5.6, p = .018). Over half of victims in substantiated cases (58.3%) resided in care facilities with a moderate level of supervision as compared with less than one third (31.4%) of those not substantiated (χ2 = 20.9, p < .0001; Tables 2 and 3). No differences were observed between victims in substantiated and unsubstantiated cases in prevalence of psychiatric illness, inability to ambulate, ability to communicate verbally or non-verbally, or orientation to place or time (Table 2).
Care Setting Type by Sexual Abuse Allegation Substantiation Status.
When the alleged perpetrator was a staff member, the sexual abuse allegation was not substantiated in 80.6% of cases and was substantiated in 19.4% of cases (χ2 = 35.3, p < .0001). By contrast, when the alleged perpetrator was another resident in the same facility as the victim, the sexual abuse allegation was substantiated 62.5% of the time and was not substantiated 37.5% of the time (χ2 = 66.1, p < .0001). Cases with allegations of hands-on type offenses (e.g., rape, attempted rape, molestation, harmful genital practices, oral-genital contact, prostitution of victim, sadistic sexual activity, or sexualized kissing) were also substantiated more often (χ2 = 11.4, p = .0008) than hands-off offenses (e.g., exhibitionism, sexual jokes and comments made to or about the victim, showing victim pornography, or voyeuristic activity). While observed injuries to the victim were rare (perhaps in part due to the fact that few of the alleged victims were physically examined by a forensic health specialist), substantiated cases were more likely to include reported injuries than unsubstantiated cases (χ2 = 10.7, p = .0011).
Characteristics of allegations that were associated with increased probability of substantiation include an allegation of neglect (χ2 = 10.4, p = .0013) or sexual abuse (χ2 = 6.1, p = .014) at report intake. Agencies other than APS responsible for investigating the abuse of vulnerable adults residing in care facilities substantiated cases more often than non-regulatory (we are not considering APS a regulatory agency) agencies (χ2 = 6.9, p = .0087). When the agency received the report within 3 days of the alleged abuse incident, substantiation was more likely (χ2 = 5.3, p = .022), although the large proportion of missing data (28%) for this item necessitates cautious interpretation. The alleged victim disclosed abuse in 59.7% of the substantiated cases compared with 46.5% of unsubstantiated cases (χ2 = 4.2, p = .041). There were no statistically significant differences in proportion of cases featuring a witness or when the victim provided a written statement (Table 2).
Logistic Regression Analyses
Based on the results of the bivariate analyses, 18 variables were selected for inclusion in the initial multivariable logistic regression analysis (Table 4). Logistic regression analyses yielded good accuracy for identifying substantiated cases. However, despite the large number of variables that were statistically significantly different at the 0.05 level between substantiated and unsubstantiated cases in the bivariate analyses (n = 13), only a few variables remained so in the multivariable analyses (Tables 5-8). Indeed, the explanatory variables that were significant at the 0.05 level alone accounted for between 83% and 93% of the total information gained by including all the explanatory variables in the model, as measured by the maximum-rescaled R2 statistic (Table 4).
Logistic Regression Model Fit Statistics.

Note. AIC = Akaike’s information criteria.
Logistic Regression Main Effects Model Effect Estimates.

Note. Model is predicting probability of sex abuse allegation substantiation (n = 403). CI = confidence interval; ADL = Activities of Daily Living.
Logistic Regression Main Effects Plus Interactions Model Effect Estimates.
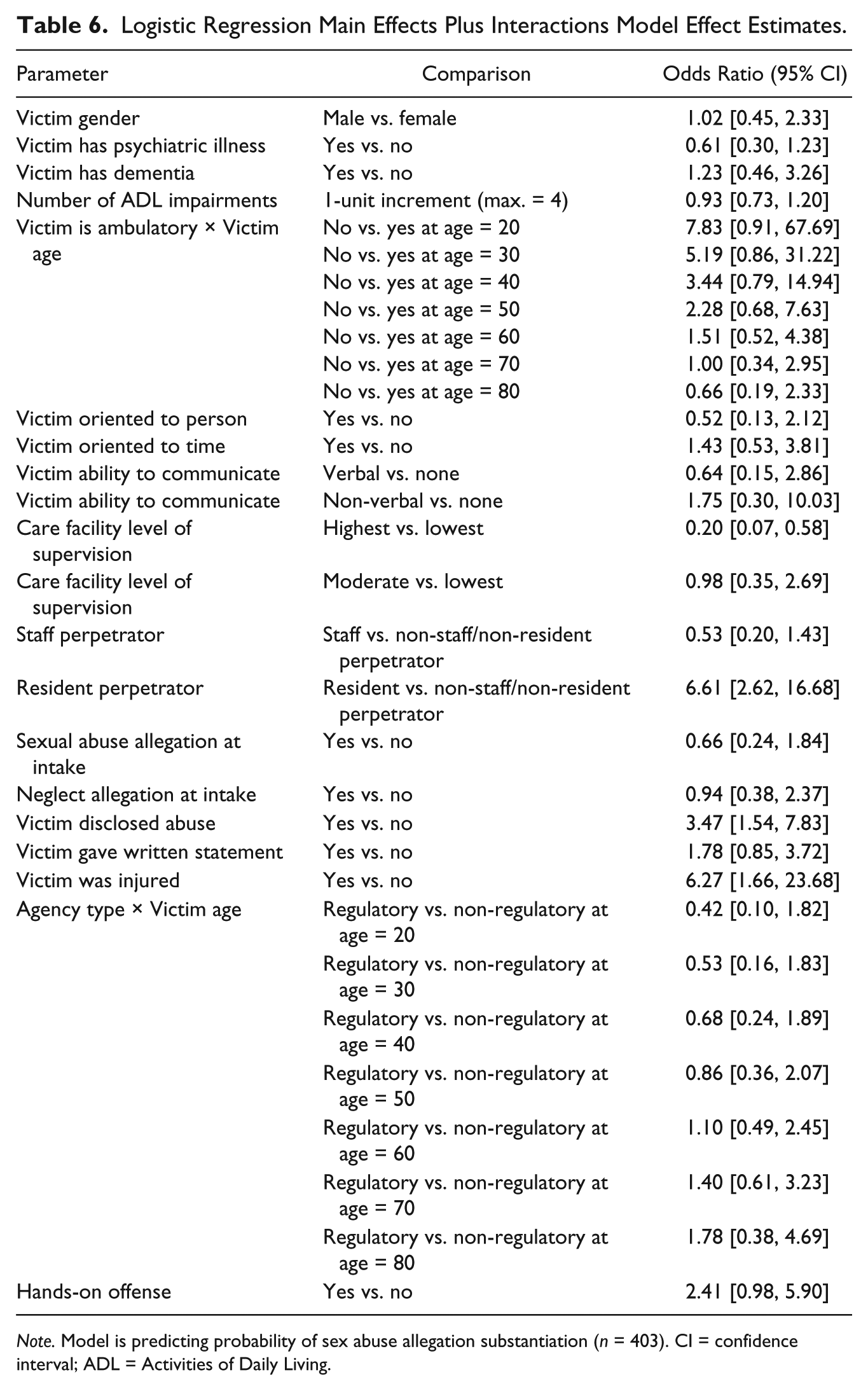
Note. Model is predicting probability of sex abuse allegation substantiation (n = 403). CI = confidence interval; ADL = Activities of Daily Living.
Logistic Regression Main Effects Model Effect Estimates.

Note. Time from incident to report to agency is included. Model is predicting probability of sex abuse allegation substantiation (n = 293). CI = confidence interval.
Logistic Regression Main Effects Plus Interactions Model Effect Estimates.
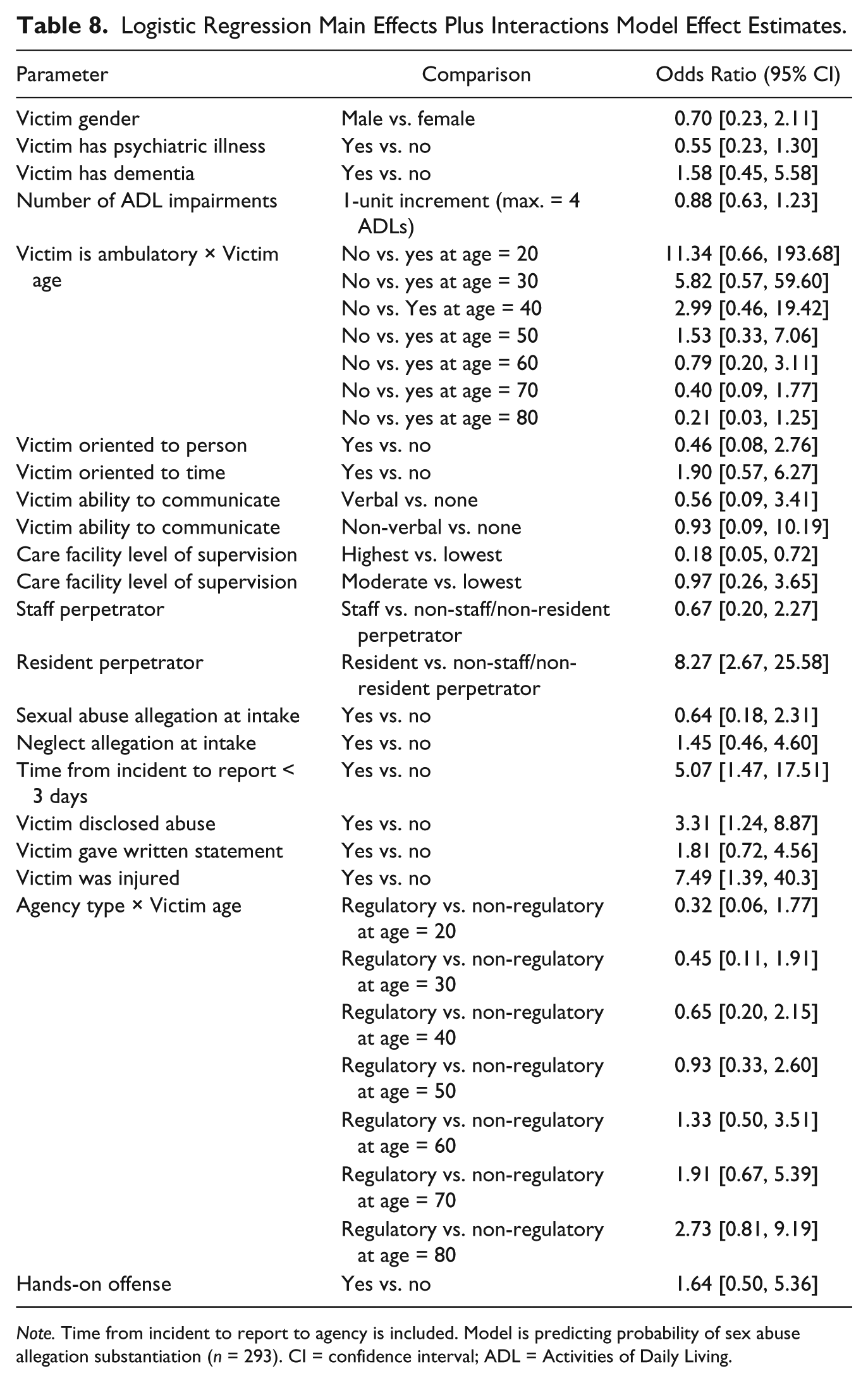
Note. Time from incident to report to agency is included. Model is predicting probability of sex abuse allegation substantiation (n = 293). CI = confidence interval; ADL = Activities of Daily Living.
Older age and female gender appeared to be strongly associated with the probability of substantiation in the bivariate analyses but had little effect in the multivariable analyses. Instead, the model results indicate that probability of substantiation is mostly explained by the type of perpetrator (facility resident, facility employee, neither facility resident nor facility employee), facility type, whether or not the victim disclosed abuse, and whether or not the victim was injured (Tables 4-7). The type of perpetrator consistently emerged as a critical factor. Specifically, if the alleged perpetrator was another resident in the facility (vs. an employee or non-resident/non-staff perpetrator), the odds of substantiation were at least two and half times greater. Level of supervision in the facility was also found to significantly predict substantiation, with cases in the lowest level of supervision (see Table 3 for listing of facilities in each category) having at least 20% greater odds of substantiation compared with cases in the highest level.
Factors that were associated with allegations being substantiated included injury to the victim, which though rarely reported (Table 5) was associated with about five-fold greater odds of substantiation. A disclosure of sexual abuse by the victim was associated with about three-fold greater odds of substantiation, compared with cases where no disclosure was made (Tables 5-8). Finally, when the indicator for time from the abuse incident to the report to the agency being less than 3 days was included in the model, it strongly predicted substantiation. Cases reported within 3 days of the alleged sexual abuse incident had at least four-fold greater odds of substantiation than those reported later (Tables 7 and 8). Cases that were missing information on time to report were more likely to include hands-off offenses (e.g., voyeurism, exhibitionism, sexual threats or unwanted comments, and “harmful genital practices”) (40.7% vs. 26.6%, χ2 = 7.7, p = .0056), less likely to have a victim disclose abuse (40.7% vs. 51.9%, χ2 = 4.1, p = .044) or provide a written statement (61.1% vs. 71.7%, χ2 = 4.4, p = .038), less likely to have a witness (3.5% vs. 12.5%, χ2 = 7.2, p = .0072), less likely to feature an allegation of neglect at intake (12.4% vs. 20.9%, χ2 = 3.9, p = .048), and the victim was more likely to live in a care setting with the lowest estimated level of supervision (25.5% vs. 14.0%, χ2 = 8.2, p = .016).
Discussion
This study examined outcomes of the investigations of the sexual abuse of vulnerable adults and utilized multivariable regression modeling to explore factors associated with the substantiation of allegations of sexual abuse. The findings are illuminating. At the microsystem level, persons who were reported as sexually abused had a mean age of slightly under 50 with the majority being female (60%). Alleged sexual abuse victims were for the most part ambulatory, and over one third were oriented to person, time, and place. Nearly half resided in restrictive care settings of some type, and approximately a third lived in nursing homes. The majority of alleged victims had reported a hands-on offense. One half of all alleged perpetrators were staff members, whereas one fourth were other residents in the facility.
Victims in the substantiated cases of sexual abuse were found to be significantly older and female (74% vs. 57%) than were alleged victims for whom cases were not substantiated. Over half lived in nursing homes. Although the overwhelming majority of substantiated cases involved hands-on offenses (e.g., rape and molestation; 86.1%), only 11.1% involved documented injuries (however, few alleged victims received a forensic sexual assault exam by a qualified specialist, hence, assault injuries may have gone undocumented). Not surprisingly, the majority of substantiated cases involved victims who disclosed that sexual abuse had occurred. Substantiated cases involved far more resident perpetrators (62.5%) than facility employee perpetrators (19.4%).
The higher proportion of female victims in substantiated cases likely reflects the population of older adults, the majority of whom are women. But, as expressed in earlier research, because 40% of the allegations concerned male victims, this finding may also reflect that women are more vulnerable to sexual abuse than men. Although this may be true in the general population, it is critical to keep in mind that sexual abuse represents an abuse carrying a tremendous stigma, one perhaps even more egregious for men than for women. Investigators may unwittingly be more likely to substantiate the alleged sexual abuse of women over that of men. It should be noted, however, that gender was not a significant factor in predicting substantiation after controlling for other variables. Also, gender may influence victim willingness to disclose. Men may be more reticent to disclose sexual abuse due to the stigma discussed above. Men in this study disclosed abuse in 37.5% of cases compared with 62.5% of women.
At the exosystem level, and because an investigation finding that substantiates sexual abuse may easily be open to litigation (both against and by the perpetrator), it is not surprising that in addition to disclosure, visible indications of hands-on offenses, such as injuries, are associated with substantiated allegations. Those who investigate reports of sexual abuse are looking for overt signs of sexual abuse and are understandably more comfortable substantiating cases when those signs are obvious.
An additional factor in our model that correlated with case substantiation was time from alleged abuse incident to report. Reports of sexual abuse in which the time is less than 3 days had a far greater chance of being substantiated than those for which time from incident to report is greater than 3 days. Presumably, abuse evidence (including memory) degrades as time elapses; consequently, degradation of abuse evidence is likely an explanation for this being a significant finding. This finding carries important implications for federal and state legislation in terms of the importance of, and research evidence supporting, requiring immediate reporting of alleged sexual abuse of vulnerable adults that occurs both in care facilities and in other locations.
Typically, abuse investigators are required to substantiate abuse cases using a “preponderance of evidence” standard (see Ramsey-Klawsnik et al., 2008), but some appeared to have applied a higher standard (i.e., beyond a reasonable doubt; reported and discussed in Ramsey-Klawsnik & Teaster, 2012) based on both our review of the surveys concerning each case as well as follow-up interviews (not discussed in this article) with randomly selected case investigators. There may be multiple potential reasons for this including failure to understand the standard of evidence set by law for civil abuse investigations, the egregious nature of sexual abuse, and the ramifications of substantiating for the perpetrator as well as the facility. The upshot is that investigators may be substantiating cases of sexual abuse (18%) at lower rates than that of other types of abuse (49%; Teaster et al., 2006), not only because of the difficulty of substantiating sexual abuse cases but also because substantiating these cases may mean that the offender is prosecuted and, consequently, that the entire investigation is thus open to public scrutiny. Additionally, investigators may question victim credibility based on such factors as age, vulnerability, intellectual disability (Hodell et al., 2009; Wasarhaley, Simcic, & Golding, 2012), or other factors and fail to substantiate a case. Among a subset of the alleged victims in this study (64 older women residing in nursing homes), 27% disclosed to investigators that they had been sexually assaulted but were not believed and their cases went unsubstantiated (Teaster, Ramsey-Klawsnik, Abner, & Kim, 2015). As noted above, the lack of training for investigators in understanding and applying appropriate standards of evidence, especially critical due to the intrusive and complex nature of these cases, may also be a factor that affects outcomes of present and future cases of sexual assault. Investigators who participated in this study and were interviewed regarding needed improvements in case-handling procedures recommended training for care facility staff in recognizing signs and symptoms of sexual assault, understanding the boundaries between staff and residents, abuse patterns, appropriate responses to suspected cases, and generational and cultural differences among residents and staff members (Ramsey-Klawsnik & Teaster, 2012).
The tendency to confirm residents as sexual abusers rather than staff members is a striking finding. Alleged perpetrators of sexual abuse were overwhelmingly staff members, but substantiated cases contained overwhelmingly resident perpetrators (Ramsey-Klawsnik et al., 2008). Although it is entirely expected that some allegations against staff members would not be substantiated upon investigation, it is surprising that so many staff members were not substantiated yet so many residents were. Facility staff members are better able than residents to plan and execute sexual assaults in ways that hide evidence and protect themselves from detection as offenders. Substantiating a staff member as a perpetrator of sexual abuse may potentially implicate him or her in losing a position, not finding another position, and if found guilty of committing a crime, going to jail. This outcome would not be true for a facility resident who may experience dementia or a psychiatric illness. A sexually abusive resident would likely be moved to a different part of a facility and placed under increased supervision or restrained in other ways.
Very few of the 410 cases of alleged sexual abuse were substantiated (18%). It is therefore critical that investigators are highly trained to handle this type of case and that they are able to investigate the case thoroughly, promptly, and with as much information as possible. It is also critical that they make substantiation decisions using the appropriate standard for confirmation (e.g., preponderance of the evidence, beyond a reasonable doubt, clear and convincing evidence) as state law dictates. Not doing so may mean that information critical to substantiate a case is inappropriately minimized or is disregarded altogether. It may also mean that cases that should have been substantiated are not, therefore dismissing important and needed forms of intervention, potentially discouraging other victims from coming forward, and allowing a perpetrator to continue assaulting vulnerable adults.
Because of the intensely traumatizing nature of this type of abuse, more resources and constant training are critical to conduct proper investigations. Realizing that relatively few alleged sexual abuse cases (as opposed to other forms of abuse allegations) are typically assigned to any one investigator in a year’s time, a suggestion is to develop a highly trained specialty group that would be ready when any allegation of sexual abuse occurs. Developing such teams is not without precedent and measured outcomes: the intensive training of Sexual Assault Nurse Examiner programs, which usually provide forensic services to younger victims, has resulted in sexual assault cases that are investigated more appropriately and prosecuted more frequently (Campbell, Patterson, & Fehler-Cabral, 2010; Campbell, Patterson, & Lichty, 2005; Wasarhaley, Simcic, & Golding, 2012). A specially trained team of sexual abuse investigators would have the advantage of having the most up-to-date knowledge regarding investigation and intervention in such cases. This team would also require continually updated training on working these cases. Part of their training could include an exploration of potential biases when working on such cases including using criteria unreasonably high to substantiate cases, substantiating cases of older versus younger victims, substantiating cases of disclosing and injured female victims more readily than their male counterparts, and substantiating resident perpetrators more readily than staff members.
This study is not without limitations. We recognize that our original data are “aging.” However, we continue to reanalyze our data and publish our findings because the study provided very rich data and because very little has changed in facility care. Indeed, President Barack Obama, in his remarks at the White House Conference on Aging (2015), opined that there has been little change in how nursing homes address residents’ safety or quality of life in nearly 25 years.
Our study prospectively explored sexual abuse cases during a 6-month period in five states, but those states may not reflect the sexual abuse investigations that occur in all states. Although the research team asked that data be provided on all reports of sexual abuse that occurred during the study period, for some reporting entities in some of the study states, not all cases were provided. Despite investigators’ efforts to provide a rich amount of data on our 12-page study instrument, they were unable to provide all information for all items requested. Additionally, it may be the case that some investigators are more likely to substantiate cases than others, as we know that educational background of the case investigator plays a role (Daly, Jogerst, Haigh, Leeney, & Dawson, 2005; Ernst & Smith, 2012). Because the instrument did not collect this information, the effect of particular investigators cannot be assessed.
Despite limitations, this study provides information important to researchers and practitioners alike concerning conditions under which allegations of sexual abuse are likely to be substantiated. Alleged sexual abuse victims in care facilities whose cases are reported quickly, those who disclose abuse, those who demonstrate visible injuries, and those who are sexually abused by a resident are far more likely to have allegations substantiated than those who do not meet such conditions. It is critical to construct more research to investigate why such propensities are so and to make sure that reports of sexual abuse are investigated and then appropriately substantiated at the appropriate index for determination. It is important to stress that the degree of violation and trauma experienced by the victim is unrelated to whether the perpetrator is a fellow resident or facility employee. More than ever, it is also critical to replicate this study in community as well as facility settings, and it is also critical to conduct this same study on other types of abuse, such as physical abuse, emotional abuse, and financial exploitation. It is abundantly clear that when it occurs, sexual abuse, regardless of the investigatory finding, constitutes an intense violation to the victim, and by extension, to each member of society who is diminished by it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Institute on Aging, R01 AG022944.