
Abstract
It is often said that intimate partner violence (IPV) happens “behind closed doors”; however, research on IPV and other crimes suggests that witnesses are sometimes present. This suggests that bystanders may be in a position to help victims or potential victims of violence. Bystander behavior has been studied primarily in school settings, and consequently, little is known about how often it occurs or what its effects may be in the broader community. This study examined IPV incidents in a rural sample to assess the presence and potential impact of bystanders on victim-reported outcomes. One thousand nine hundred seventy-seven adult participants completed a questionnaire that asked about five violent behaviors (my partner threatened to hurt me; pushed, grabbed, or shook me; hit me; beat me up; sexually assaulted me), bystander characteristics, and victim outcomes (fear; injury; disruption of daily routines; mental health). Adult or teen bystanders were present for each IPV approximately one third of the time, except in the case of sexual assault (14.3%). When a bystander was present, victims reported higher rates of injury, greater disruption in their routines, and poorer mental health. When a bystander’s safety was threatened, victims reported more physical injury and more routine disruption. A considerable number of IPV incidents do not happen behind closed doors, and the presence of a bystander was associated with worse outcomes for victims. Prevention efforts for adult IPV may need to take a more cautious or nuanced approach to encouraging bystander action, especially when confronted with more severe incidents. Bystander safety should be a priority for violence prevention.
Intimate partner violence (IPV) is a widespread public health problem with as many as one in three women (35.6%) and more than one in four men (28.5%) in the United States experience rape or physical violence by an intimate partner (Black et al., 2011; Breiding et al., 2014). A common perception is that IPV happens in private, outside of public awareness (Wright & Benson, 2011). However, findings from the National Crime Victim Survey (Planty, 2002) found that as many as one third of reported IPV incidents were witnessed by a third party. This raises the possibility that bystanders often may be in a position to help victims or potential victims of partner violence (Banyard & Moynihan, 2011; Hamby, Weber, Grych, & Banyard, 2015). Bystanders are third parties who witness dangerous or potentially dangerous interactions or receive disclosures from victims about incidents of IPV. These witnesses can choose to do nothing or can take action to try to remedy the situation by helping the victim or potentially make the situation worse by joining with the perpetrator.
IPV is the use of physical force, psychological or sexual coercion against a current or former romantic or sexual partner. With the widespread nature of IPV, many researchers have turned to how bystanders affect IPV. Most research on the nature of bystander behavior has focused on students and forms of violence such as bullying, sexual assault, or conventional crime (Banyard, 2008; Banyard, Plante, & Moynihan, 2004; Salmivalli, 2010; Swearer, Espelage, Vaillancourt, & Hymel, 2010). Frye and colleagues (2012) documented bystander actions that participants in urban areas consider to be feasible and helpful in response to IPV, which includes calling the authorities, communicating with and engaging with neighbors, and offering help. Few studies have been conducted in rural areas, which may have different bystander patterns due to lower population density or less access to services (Edwards, Mattingly, Dixon, & Banyard, 2014; Wee, Todd, Oshiro, Greene, & Frye, 2016). There remains a broader lack of research on IPV in rural communities as well (DeKeseredy & Schwartz, 2009; Edwards, 2015). The current study examined incidents of IPV in a community sample from rural Appalachia to assess rates of bystander presence and the potential impact of bystanders on victim-reported outcomes.
Bystander Intervention
Bystander intervention was originally described by Latané and Darley (1970), who identified key factors that make it more likely that individuals will step in to help someone in danger. To take action, a bystander must first notice the situation and label it as problematic. They must then feel some sense of personal responsibility to do something about it, have the skills to create a course of action for what must be done, and then choose to act. More recently, relational and community factors that may affect bystander action have been studied (Banyard, 2015; McMahon et al., 2015). For example, Edwards and colleagues (2014) found that young adults in rural communities were more likely to take action when they witness IPV if they felt a strong connection to their community. Another study focused on youth victimization by peers and adults (Hamby et al., 2015) found that higher community support scores were associated with perceiving bystanders as helpful in cases of youth violence. Support scores, especially collective efficacy, were also associated with bystander safety for some victimization types. As suggested by the foregoing, most published studies of bystander behavior have focused on college and high school samples, and there is less information available on young and middle adults (see Banyard & Moynihan, 2011; Bennett, Banyard, & Garnhart, 2013; Edwards et al., 2014; McMahon et al., 2015, for reviews).
Few studies have researched bystander action in community samples or from the viewpoint of victims (see Edwards et al., 2014; Wee et al., 2016; for exceptions). One exception (Frye et al., 2012) utilized concept mapping to determine how bystanders in urban neighborhoods prevented IPV and how effective residents perceived them to be. Neighborhood bystanders were likely to engage in behaviors such as calling the police or making known to the perpetrator that others heard the violence. Moreover, they found that intervention behaviors that focused on the victim (e.g., involving friends and family, local businesses, and residential building staff) were perceived to be the most practical, whereas formal actions, such as calling the police, were perceived to be more effective than practical.
Consequences of Bystander Actions
Existing research suggests that bystanders may have good intentions, but intervening in a potentially dangerous situation is complicated. Too little attention has been paid to the consequences of bystander presence and actions, particularly for IPV (Banyard, 2015). There are many components to consider when determining whether bystander intervention is effective and safe for the bystander and victim. Hamby et al. (2015) explored a range of childhood victimizations and found that bystander presence or absence was not significantly associated with victim outcomes. However, when victims perceived that bystanders were helpful and were not harmed, victims reported higher well-being. Bystanders can be at risk for harm when they intervene in high- or low-risk situations (Hamby et al., 2015), and bystanders report that they consider the potential consequences and often experience anxiety that interferes with their ability to act (McMahon & Dick, 2011). Questions remain about the role of bystanders in instances of IPV, the extent to which bystander safety may be compromised in these situations, and victims’ views of bystander impact.
The Effectiveness of Bystanders in Rural Versus Urban Settings
Rennison, DeKeseredy, and Dragiewicz (2012) and Edwards et al. (2015) have described how the experience of IPV may be different in rural and urban settings. Not only are rural communities generally more isolated, but victims of IPV in rural communities also report having less social support and more difficulty in reporting and seeking help than urban victims (Logan, Evans, Stevenson, & Jordan, 2005; Logan, Walker, Cole, Ratliff, & Leukefeld, 2003). Many studies suggest that rural perpetrators may perpetrate more frequent and severe IPV than urban perpetrators (Goodrum, Wiese, & Leukefeld, 2004). Moreover, Websdale (1998) and Websdale and Johnson’s (1997) data suggest that rural perpetrators may choose to live in rural locations to isolate their victims. It is likely, then, that rural bystanders may be present in fewer instances of partner violence, and when they are, they may be confronted with more severe IPV and greater risk to their own safety. On the positive side, a greater sense of community and connection in rural communities may help promote bystander safety and promote action (Banyard, 2015; Edwards et al., 2014). Because less research has been conducted on bystanders and IPV in rural and urban settings, little is known about whether bystander intervention has different outcomes for victims or bystanders (Edwards et al., 2014; Frye et al., 2008; Wright & Benson, 2011).
Bystander Intervention Training
The past decade has witnessed an explosion of bystander intervention training as one prong of sexual assault and relationship violence prevention. While the bulk of these programs exist in secondary schools and college campuses (Cares et al, 2015; Coker et al., 2011), community approaches are appearing as well (Banyard, Edwards, & Seibold, 2016). These training programs will be enhanced by continuing to answer more basic questions about bystander action—how often it occurs in different contexts like rural communities and with what impact on victims.
The Current Study
The aim of the current study was to investigate, in a rural and understudied community sample, how often victims of IPV reported that bystanders were present across several different forms of IPV, whether victims reported that bystanders helped the situation, whether bystanders were harmed, and how such factors were related to victim outcomes, such as a victims’ levels of fear, whether a victims’ routine was disrupted, and victims’ self-report of current mental health. Unlike many studies of bystander intervention that focus on self-reports by bystanders, this exploratory study examined this issue through the eyes of victims of IPV with a victim-centered, incident-specific approach to describe bystander involvement in IPV.
We hypothesized that (a) there would be a substantial level of bystander presence for IPV incidents; (b) the presence of bystanders would be associated with more positive outcomes for victims; (c) when a bystander was present, we hypothesized that helpful bystanders would be associated with more positive outcomes than bystanders whose actions made the situation worse; and (d) better victim outcomes would be associated with bystander safety than when the bystander was harmed or threatened.
Method
Participants
Participants were 1,977 individuals from rural areas in the Southern United States, who were a subsample of a larger community study (N = 2,565). For this study, we focused on participants above the age of 18 years who had at least one dating partner and answered the full set of questions on IPV (M = 33.6, SD = 12.2). The sample was 65.3% female and 34.7% male; most (76%) of the sample identified as White/European American (non-Hispanic), 12.4% as African American/Black (non-Hispanic), 6.3% as Hispanic/Latino (any race), 3.2% as more than one race, 1.1% as American Indian/Alaskan Native, 0.7% as Asian, and 0.3% as Hawaiian/Pacific Islander.
Regarding education, 3.0% of participants were currently in school, 40.7% held either a high school diploma or a General Education Degree (GED), 7.8% had dropped out of school, 24.4% had some college with no degree, and the rest (24%) had an associate’s degree or higher. Forty percent of participants reported earning US$20,000 or less per year (total household income), 34.6% reported earning US$20,000 to US$50,000, and 25.5% reported earning US$50,000 or more. Most of the sample (67.7%) lived in small towns with a population of 2,500 to 20,000 people, 20.1% of participants lived in rural areas with populations of less than 2,500 people, and the others (12.3%) lived in more populous areas.
Procedure
Participants were recruited through a range of advertising techniques in 2013 and 2014. This range was used to reach segments of the population in rural Appalachia who are not often sampled in research and participants who might have limited transportation access. Furthermore, interviewers often met participants at different locations (including the research center and participants’ homes). The majority of participants (72.9%) were recruited at local community events, such as festivals and county fairs. Word-of-mouth was the second most productive recruitment strategy, accounting for 15.6% of participants. The remaining 11.5% were recruited through other strategies, including flyers, newspaper and radio ads, and direct mail. The survey was self-administered using Snap10 survey software on laptops and iPads so that Internet connectivity was not needed. An audio option was available. Technical problems (such as iPads overheating) and time limitations prevented some individuals from completing the survey; overall, the completion rate was 85%, and the median completion time was 53 min. This is an excellent result by current survey standards, especially considering the survey length, with current completion rates often below 70% (Abt SRBI, 2012) and sometimes below 50% (Galesic & Bosnjak, 2009). All participants received a US$30 Walmart gift card and information on local resources. All procedures were conducted in accordance with American Psychological Association (APA) ethical principles and approved by the institutional review board (IRB) of the study’s home institution.
Materials
The measures included in this study were part of a larger set of questionnaires assessing a wide range of constructs. Those used in the current analyses are described below. For more details and a full list of measures, visit https://lifepathsresearch.org.
Victimization
The Partner Victimization Scale (PVS; Hamby, 2016) included five forms of direct victimization, including verbal, physical, and sexual victimization. Construct validity was demonstrated with significant, moderate correlations with other indices of victimization and adversity. Reliability showed a Cronbach’s alpha of .75. The five partner victimization items included the following: “Not including horseplay or joking around, my partner threatened to hurt me and I thought I might really get hurt,” “Not including horseplay or joking around, my partner pushed, grabbed, or shook me,” “Not including horseplay or joking around, my partner hit me,” “Not including horseplay or joking around, my partner beat me up,” and “My partner made me do sexual things when I didn’t want to.”
For each type of partner victimization, specific questions were asked first in a yes/no format to learn whether this form of victimization happened to the participant. When they answered yes to any of these questions, they were then directed to an additional series of questions that asked about other characteristics of the event. Participants who indicated that a form of victimization had happened multiple times were asked to answer follow-up questions about the most recent occurrence.
Bystander characteristics
Participants who reported they experienced a particular form of IPV on the PVS were asked three follow-up questions about bystanders (and if a participant had multiple incidents of the same type, they were asked to answer in relation to the most recent incident), which were adapted from Planty (2002). The first asked, “Did any teen or grown-up see what happened to you, besides you and the person who did this?” with response options of family, friend/acquaintance, police, stranger, or no one. The next follow-up asked, “Did anyone who saw what happened, (1) Help in any way, (2) Make things worse, (3) Both help and make things worse, or (4) Didn’t help and didn’t make it worse?” Finally, participants were asked, “Did any witness get hurt or threatened?”
Incident outcomes
For each form of partner victimization a participant experienced, they were asked the PVS follow-up questions assessing fear (“Thinking back to when it happened, how afraid did you feel?”) and disruption of daily routines (“Did you miss any days of school, work, or your normal routine because of what happened?”). For items on physical violence, a follow-up question about physical injury (“Were you physically hurt when this happened?”) was included as well. Response categories for the fear item was on a 3-point scale (not at all, a little, or very afraid), and the routine disruption and injury items were answered with “yes” or “no.”
Mental health
We selected 10 of the 28 Trauma Symptom Checklist for Children (TSCC; Briere, 1996) items used in a national survey (Finkelhor, Hamby, Ormrod, & Turner, 2009) that loaded the strongest onto the single factor revealed by a factor analysis and further validated in a pilot study for use with adults. The 10 symptoms assessed were loneliness, sadness, irritability, feeling bad, guilt, worry, dissociation, intrusive images, unpleasant memories, and intrusive memories. Reliability showed a Cronbach’s alpha of .90. The TSCC exhibited moderate correlations with the Age 16 Trauma Symptoms Checklist (Briere, 1996). We used this version because our original, larger sample (N = 2,565) included both youth and adults. All 10 questions asked how often the participant experienced a certain symptom in the past month. For example, to assess loneliness, we asked, “How often have you experienced loneliness in the past month?” Response categories ranged from 1 (often) to 4 (never), such that possible scores range from 10 to 40, and higher scores indicate better mental health.
Results
Table 1 presents descriptive information about the frequency of victimization, bystander presence, and identity of the bystander for five forms of IPV. Note that only victims of a particular form of IPV were asked questions about bystander involvement, and only victims with bystanders could be asked about the impact of the bystander (the percentage of participants who endorsed each branch of the follow-ups are in Table 1). The most common victimization was pushing or grabbing, and the least common was sexual victimization. In partial support of our first hypothesis, bystanders were present in about one in three instances for all four forms of psychological and physical IPV (30%-38%). They were less commonly reported for sexual victimization incidents but still present in about one in seven cases (14.3%). Bystanders were most commonly described as family, friends, and acquaintances. Strangers and police were seldom present, except in the case of sexual victimization, 22.7% and 13.6%, respectively.
Frequencies of Victimization, Bystander Presence, and Bystander Type Reported for Five Forms of Victimization.
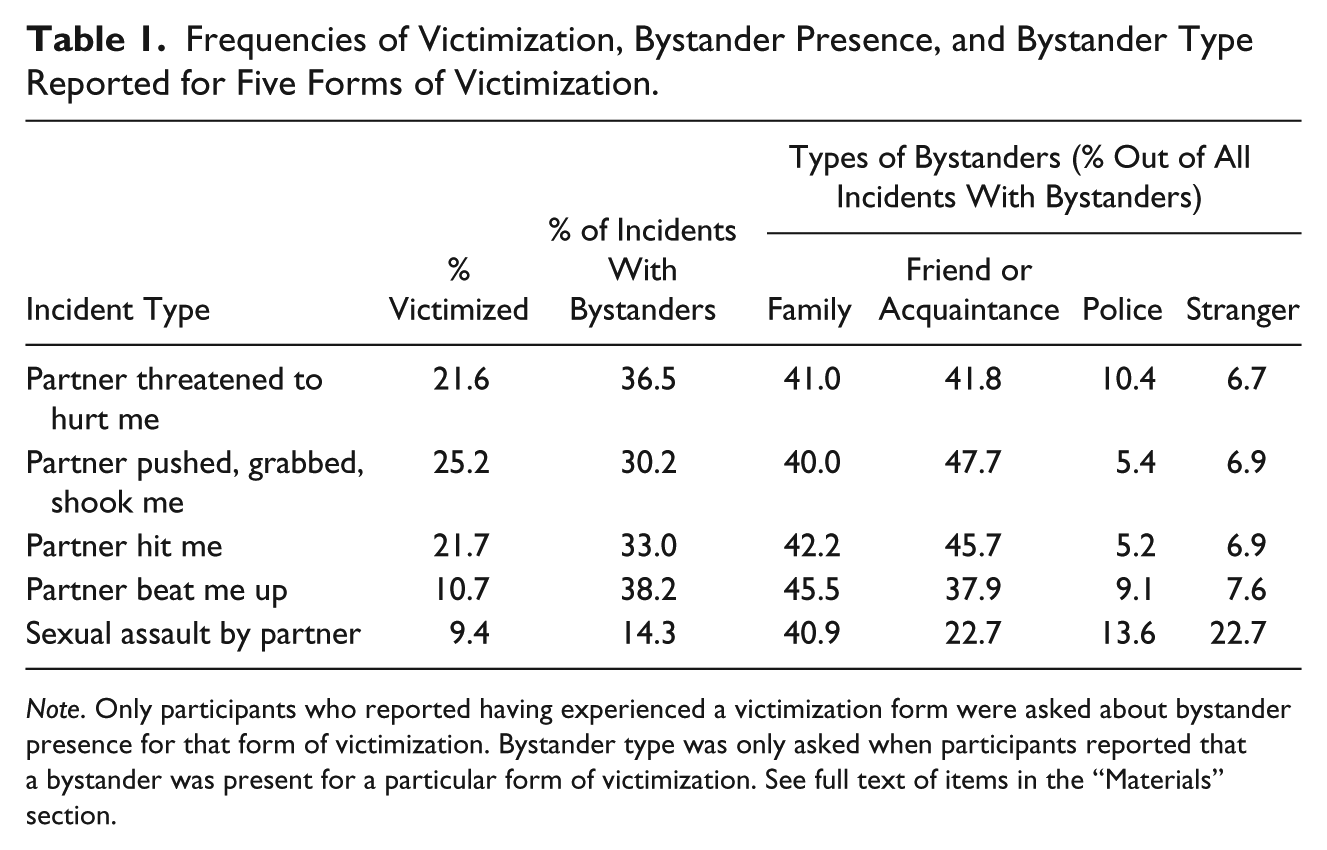
Note. Only participants who reported having experienced a victimization form were asked about bystander presence for that form of victimization. Bystander type was only asked when participants reported that a bystander was present for a particular form of victimization. See full text of items in the “Materials” section.
Table 2 presents descriptive data about the incident outcomes (fear, injury, and disruption of daily routines) related to each of the five forms of victimization. In terms of victim fear, victims reported experiencing more fear when their partner beat them up (65.5%) and when their partner threatened to hurt them (52.9%) in comparison with the other forms of IPV; however, victims reported feeling very afraid one third of the time across all victimization types (more than 40% for each). Getting beaten up also led to the highest reports of daily routine disruption (33.3%) and injury (64%) compared with other forms of IPV victimization.
Frequencies of Incident Outcomes and Victim Harm Reported for Five Forms of Victimization.
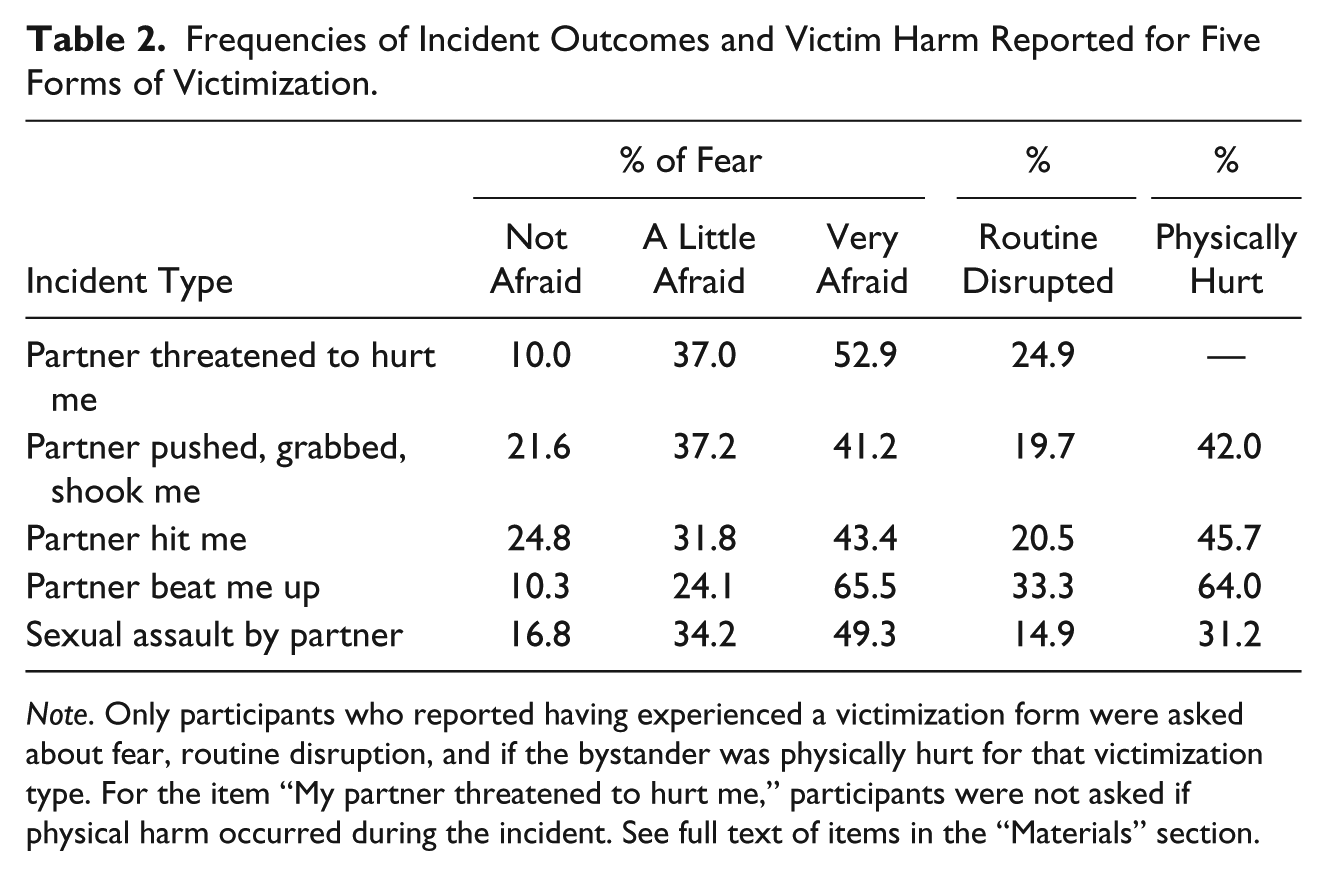
Note. Only participants who reported having experienced a victimization form were asked about fear, routine disruption, and if the bystander was physically hurt for that victimization type. For the item “My partner threatened to hurt me,” participants were not asked if physical harm occurred during the incident. See full text of items in the “Materials” section.
Table 3 presents data regarding bystander actions and whether the bystanders were themselves harmed or threatened. Across all forms of IPV victimization, bystanders who helped or had no impact were more common than bystanders who harmed the situation or both helped and harmed. The highest reports of bystander helpfulness were for being pushed, grabbed, or shoved. The majority of bystanders were unharmed, but rates of harm were still substantial, with 15.6% to 22.7% experiencing harm.
Frequencies of Bystanders’ Actions and Harm or Threat to Bystanders, Reported for Five Forms of Victimization.

Note. Participants who reported that no bystanders were present were not asked about bystander’s actions or harm/threat to bystanders. “Did nothing” indicates bystander neither helped nor harmed the situation.
Bystander Presence and Victim Outcomes
We examined whether the presence of witnesses affected the self-reported outcomes by victims of each of the five forms of partner victimization. We used four indicators of victim outcome: victim fear, victim injury, victim routine disruption, and victim current mental health. Chi-square tests were used to examine the differences in rates of injury and routine disruptions by the presence or absence of a bystander, and ANOVAs were used for fear and mental health ratings.
Our hypothesis regarding more positive victim outcomes with bystander presence was not supported. Fear ratings were not significantly related to the presence or absence of a bystander. Indeed, victims had significantly higher rates of injury when a bystander was present than absent for two forms of IPV: being pushed or grabbed (p < .01) and if the victims were hit by their partner (p < .05). In addition, for three forms of IPV, the victims’ routine was more likely to be disrupted when a bystander was present: being threatened by their partner (p < .01), if the victims were hit by their partner (p < .01), and if the victims were sexually assaulted by their partner (p < .01). In terms of mental health, victims’ current mental health was worse when a bystander was present for three forms of IPV: when their partner pushed or grabbed them (p < .05), when their partner hit them (p < .05), and when their partner beat them up (p < .05). For full results, refer to Table 4.
Bystander Presence as a Function of Four Outcomes of Victimization for Five Forms of Victimization.

Note. Values indicate M (SD) or % yes. n varies because only participants who reported having experienced a victimization type were asked about bystander presence for that victimization type. Fear ratings were on a scale from 1 (not afraid) to 3 (very afraid). Injury was only asked about physical and sexual assault.
p < .05. **p < .01. ***p < .001.
Bystander Impact and Victim Outcomes
We also examined the relationship between victims’ perceived bystander impact and victim outcomes. These analyses were only calculated for the subgroup of participants reporting that a bystander was present (n = 490). Using the same four indicators of victim outcome, we examined bystander impact across the five forms of IPV. Outcomes including victim’s physical injury and rates of victim routine disruption were analyzed with chi squares, while the outcomes of victim’s fear level and current mental health were analyzed with ANOVAs. Due to reduced sample size, bystander impact was dichotomized with one category indicating that a bystander helped the situation, and another category being a composite that included bystanders who harmed, helped and harmed, or did nothing in relation to the situation. See Table 5 for full results.
Bystanders’ Actions as a Function of Four Outcomes of Victimization for Five Forms of Victimization.

Note. Values indicate M (SD) or % yes. n varies because only participants who reported that bystanders were present were asked about bystander actions. “Did nothing” indicates bystander neither helped nor harmed the situation. Fear ratings were on a scale from 1 (not afraid) to 3 (very afraid). Injury was only asked about physical and sexual assault. Participants who reported that no bystanders were present were not asked about bystander’s actions.
p < .10. *p < .05.
Hypotheses were partially confirmed regarding bystander impact and victim outcomes. Victims reported less fear during instances of being pushed or grabbed by a partner when a bystander was helpful (p < .05) compared with when bystanders harmed, helped/harmed, or did nothing. The outcomes of physical harm and mental health were not significantly related to bystander impact. For sexual assault, victims who reported helpful bystanders also reported greater physical harm (p < .05), and routine disruption (p < .10), though caution should be used when examining these analyses as the n was quite small for victims of sexual assault who also reported the presence of a bystander.
Bystander Safety and Victim Outcomes
In addition to assessing the association of bystander impact and victim outcomes, we examined how harm or threats to the bystander were associated with the same four victim outcomes, again using chi squares to compare rates of victim physical injury and routine disruption with bystander safety and using ANOVAs to compare fear levels and current mental health scores with bystander safety.
Two outcomes, fear and mental health, were not significantly related to whether the victim perceived the bystander was harmed or threatened. Contrary to our last hypothesis, victims were more likely to report physical injury when a bystander was also harmed or threatened in three of the five forms of IPV: being pushed, grabbed, or shook (p < .05); being hit (p < .05); and getting beat up (p < .05). When a bystanders’ safety was jeopardized, victims’ routines were significantly more likely to be disrupted than when bystanders were not harmed for all five victimization forms (ranging from p < .001 to p < .10). See Table 6 for full results.
Harm or Threat to Bystander as a Function of Four Outcomes of Victimization for Five Forms of Victimization.
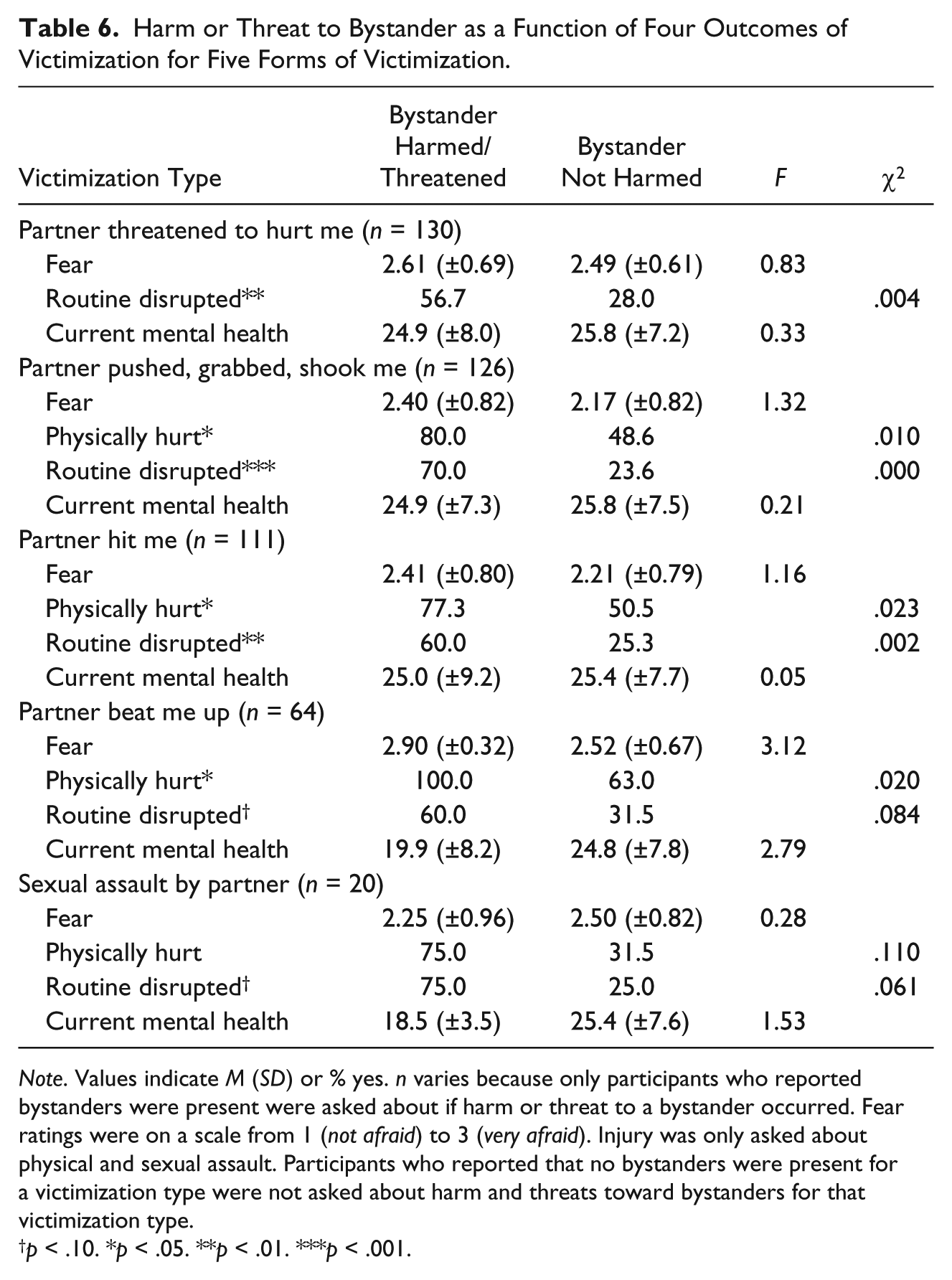
Note. Values indicate M (SD) or % yes. n varies because only participants who reported bystanders were present were asked about if harm or threat to a bystander occurred. Fear ratings were on a scale from 1 (not afraid) to 3 (very afraid). Injury was only asked about physical and sexual assault. Participants who reported that no bystanders were present for a victimization type were not asked about harm and threats toward bystanders for that victimization type.
p < .10. *p < .05. **p < .01. ***p < .001.
Discussion
To our knowledge, this is one of the first studies of bystander consequences and victim outcomes for IPV, as well as one of the first to examine an adult, rural community sample. The rates of bystander presence are consistent with the only other estimate we could find, a more than 10-year-old figure from Planty (2002), which also found that third parties were present for incidents of IPV about one third of the time. These findings contrast with earlier work suggesting that bystanders in rural locations might be present less often than in urban areas (Edwards, 2015; Websdale, 1998; Websdale & Johnson, 1997). About one third of bystanders were reported by victims to have helped the situation, greater proportions than harmed or hurt and harmed, but about the same as the percentage of bystanders who did nothing, similar to Planty’s (2002) findings. Importantly, the findings from the current study suggest that across multiple victim outcomes and forms of IPV, the presence or absence of a bystander was either not significantly related to victim outcomes or that bystander presence made the outcomes worse.
The finding that bystanders were present during interactions when victims reported more adverse outcomes was counter to our prediction. It is possible that bystanders are most likely to become aware of potential danger and to make their presence known when IPV is more serious. This explanation fits with Latané and Darley’s (1970) situational model, which states that bystanders are more likely to intervene if there is a clear need, and physical violence may be a clearer signal to draw bystanders in than other forms of IPV (which might be more subtle and ambiguous to bystanders). Alternatively, the presence of a bystander may make a violent or potentially violent situation worse by reinforcing the behavior of the perpetrator or even inadvertently promoting escalation, perhaps by increasing a perpetrator’s perceived need to act “tough” or not back down.
Even when victims reported that bystanders helped the situation, this perception was not associated with better victim outcomes. This finding contrasts with other work using data from this study examining youth victimization, which found that self-reports by victims about helpful bystanders were associated with improved victim outcomes (Hamby et al., 2015). The present data suggest that bystander intervention may not be as effective with adult IPV as it is with bullying or other youth violence. Furthermore, the current analyses showcase potential consequences for bystanders. About one in five victims of IPV who indicated the presence of third parties during IPV reported that those bystanders were harmed or threatened in some way, and harm to a bystander was clearly associated with more negative victim consequences. This finding is consistent with research suggesting that bystanders in rural locations would be intervening in more severe instances of IPV, putting their safety at higher risk (Edwards, 2015; Websdale, 1998; Websdale & Johnson, 1997).
One possible difference is that IPV as measured in the current study was adult-on-adult violence and may be easier to intervene more effectively in cases with child victims, especially in cases of adults intervening in peer-on-peer violence. Bystanders, whether peers or adults, may have more power to influence peer violence situations more effectively. More research is needed to better understand these processes. From a practice perspective, this suggests the need for bystander training to reexamine what bystanders should do in cases of adult-on-adult violence to ameliorate the impact of victim outcomes. To date, most bystander trainings are for schools or campuses rather than for community members.
Bystander intervention training also needs to place safety training for bystanders at the center of curriculum development. Safety will likely look different across different community contexts, such as a stronger focus on the higher possibility of victim isolation in rural locales or a building a stronger sense of community within urban locales. While program evaluation of bystander intervention training in the context of schools and college campuses has been promising, the current findings indicate that translating such research to community settings and to other forms of violence is complicated. Thus, further research is needed to better understand the risks for bystander intervention, the array of harms and consequences bystanders’ experience, and which specific bystander actions may be most or least helpful in different contexts. While the work of Frye et al. (2012) and others show that community members seem ready to engage as active bystanders, we still know far too little about what happens when they do—both for victims and for bystanders. One particular noteworthy strength of our study is that this is the largest social science study ever conducted in rural Appalachia, an area known for being relatively isolated and underrepresented in existing research. However, more research is needed to examine our posed questions in urban and more ethnically diverse samples.
Limitations
There are some limitations to the current study that should be acknowledged. Our data are self-report, and future studies should include multiple sources of information about the event, and alternative data sources would be valuable as well. Moreover, though more than a majority of our participants reported living in a rural area, we did not ask whether the IPV occurred in a rural setting. Future studies should include this in the questionnaire to strengthen the comparison between urban and rural settings. Because of sample size issues, we had to dichotomize the bystander action variable. Further research is needed to explore the effects of bystander action with a larger sample size. Qualitative data would also aid in determining the impact bystanders have on IPV and to determine what victims do find helpful across these IPV situations. We were also limited when asking details about more than one incident, and future research would benefit from exploring additional bystander characteristics, such as the age of the bystander, aside from whether they were adolescents or adults. Moreover, our sample was collected from a rural, southern part of the United States with less racial and ethnic diversity than other regions. It would benefit future research to examine the impact of bystanders in diverse communities. Our sample adds to the diversity of existing literature with our rural, Appalachian, low socioeconomic status (SES) sample. In addition, we were able to recruit a sample that is more ethnically and racially diverse than is typical of the region, but future research would benefit from continuing to extend this work to other underserviced and disadvantaged communities. Future research should also explore bystander behavior for IPV among couples with the full range of gender identities and sexual orientations.
Clinical and Policy Implications
Although we examined specific instances of IPV, other studies and researchers might benefit from conducting qualitative analyses to garner more detailed information about the IPV instance itself, such as what specific actions the bystander took to help or even hinder the situation and with what effect. Future research would also benefit from expanding the level of detail on bystander impact and involvement. For instance, the response option we adopted from the National Crime Victimization Survey (NCVS), “the bystander both help and harmed,” is more ambiguous than the other response categories. More measurement development could advance the research in this area. Furthermore, in the current study, we did not ask many questions about characteristics of the bystander. Future work may benefit from analyzing the impact of specific bystander behaviors. Prevention efforts should focus on educating bystanders about effective strategies that also maintain in potentially harmful situations.
Conclusion
A good deal of IPV does not take place entirely behind closed doors. When it occurs in the presence of bystanders, these data indicate that their impact in a rural adult community sample is mixed. Bystanders seem more often present in forms of IPV that involve physical injury. Bystanders are equally perceived as helpful and as doing nothing by victims, but, even when perceived as helpful, bystanders have less impact on improving victim outcomes than has been reported in similar studies on youth victimization. What is it about IPV itself that may be a unique and more challenging context for bystander intervention? How can we improve bystander safety as harm to bystanders is clearly associated with victim distress? More research to disentangle these complexities is needed. Our data suggest rethinking current bystander training with a greater emphasis on safety and more exploration of what victims want from bystanders. The current study represents a first step.
Footnotes
Authors’ Note
The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of the John Templeton Foundation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible through the support of a grant from the John Templeton Foundation.