
Abstract
Intimate partner violence (IPV) is a serious public health problem with known negative physical and mental health outcomes for women exposed. Studies have shown that with increased violence exposure, there are increased risks of negative outcomes for women. Likewise, chronicity of IPV across multiple partners is linked to more profound psychological suffering than acute exposure. However, little is known about the social- and individual-level characteristics of women that are correlated with engagement with multiple abusive partners. The current study (N = 164) identifies the characteristics of women that are associated with the number of violent partners with which they have been involved, with 35% of the sample reporting multiple IPV relationships. Participants reported on the number of violent partners, demographic characteristics, trauma history, current trauma and depressive symptoms, and exposure to IPV, including physical, sexual, and psychological violence. Results of multiple regression analysis indicate that trauma history (childhood sexual abuse, being held hostage, and torture) and current psychological violence were associated with women’s engagement with multiple violent partners. Additional findings reveal that identification as African American and White was associated with greater re-engagement compared with identification as Latina. Finally, current exposure to sexual violence was associated with fewer violent partners. The clinical implications of these findings for treatment for women at risk for engagement with multiple partners in IPV relationships are discussed.
Keywords
Recent estimates suggest that approximately one in three women have experienced intimate partner violence (IPV) in their lifetime (Breiding, Chen, & Black, 2014). Rates of IPV are even higher among Black and Latino communities (Nowotny & Graves, 2013), as well as populations with compromised economic resources and low levels of educational attainment (Golden, Perreira, & Durrance, 2013). IPV has been shown to lead to serious negative physical and mental health outcomes including depression, posttraumatic stress disorder (PTSD), and other associated trauma symptoms (Lacey, McPherson, Samuel, Powell Sears, & Head, 2013; Lilly & Graham-Bermann, 2010; Ouellet-Morin et al., 2015). The cost of direct medical and mental health care services resulting from IPV is estimated at nearly US$4.1 billion per year in the United States (National Center for Injury Prevention and Control, 2003), thus making IPV an issue of vast social and financial concern. Research has also long established a dosage effect of exposure to IPV, such that the severity and amount of exposure are linked to an increased risk of negative outcomes for women (Bonomi et al., 2006; Golding, 1999). Likewise, chronicity of IPV across multiple partners and time periods is linked to more profound psychological suffering than acute exposures to this type of violence (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012; Bogat, Levendosky, Theran, Von Eye, & Davidson, 2003; Bonomi et al., 2006; Coolidge & Anderson, 2002; Golding, 1999). Thus, a woman’s involvement with multiple violent partners (re-engagement in violent relationships) is an issue of paramount importance. However, little is known about the characteristics of women who have had multiple violent partners (Cattaneo & Goodman, 2005). In this study, we address what factors are associated with the number of women’s violent partners, using demographic characteristics (including ethno-racial variation), trauma history, current trauma and depressive symptoms, and IPV exposure.
IPV Exposure in the United States
IPV is physical violence, sexual violence, threats of physical or sexual violence, stalking, and psychological aggression (including coercive tactics) by a current or former intimate partner (Black et al., 2011). Exposure to IPV is associated with increases in annual health care costs lasting up to 15 years after the cessation of the violence (Rivara et al., 2007). Although measurement concerns make exact prevalence rates difficult to ascertain, Ouellet-Morin et al. (2015) found that 33% of women from England and Wales had experienced violence by a partner over a 10-year period. This supports previous findings that established the pervasiveness of IPV over time, estimating a lifetime prevalence of any type of IPV at 44%, physical/sexual violence at 34.1%, and non-physical violence at 35.1% for women (Thompson et al., 2006). Furthermore, these authors found that the proportion of women rating exposure to violence as moderately to extremely violent was significant: 61% for physical violence, 45% for forced sexual intercourse, 36% for forced sexual contact, 63% for fear due to a partner’s threats/anger, and 31% for controlling behavior (Thompson et al., 2006).
Ethno-Racial Variation in IPV Exposure
Research on ethno-racial variation in IPV exposure has consistently shown that African American and Latina women are 3 times more likely to experience IPV than their White counterparts, even after controlling for demographic factors, alcohol consumption, and psychosocial variables (Caetano, Field, Ramisetty-Mikler, & McGrath, 2005). It is especially important to control for socioeconomic status due to the lower income and greater proportion of racial and ethnic minority women who live in poverty, thus ruling out findings that confound violence with poverty. Results from several studies have indicated that after controlling for socioeconomic status, Latinas still experience disproportionate levels of IPV as compared with both African American and White women (Clark, Galano, Grogan-Kaylor, Montalvo-Liendo, & Graham-Bermann, 2014; Nowotny & Graves, 2013) and that the rate of reoccurrence of severe IPV in Black and Latina women is 6 and 4 times higher, respectively, than the rate for Whites (Caetano et al., 2005). Finally, researchers have shown that both African American women and Latinas are more likely to be murdered by an intimate partner than their White counterparts (Azziz-Baumgartner, McKeown, Melvin, Dang, & Reed, 2011), although a limitation of this study is that the socioeconomic status of the sample was not included as a control variable. Ethno-racial considerations are of the utmost importance when assessing women’s exposure to IPV given that initial findings have shown both the amount and severity of exposure vastly differ among these populations. The present study represents an improvement over some previous studies in the literature that were limited by not controlling for socioeconomic status.
Effects of IPV on Women
The harmful effects of IPV on women’s physical and mental health have been well established irrespective of the ethno-racial group with which they identify (Clark et al., 2014; Edelson, Hokoda, & Ramos-Lira, 2007; Flicker, Cerulli, Swogger, & Talbot, 2012; Lacey et al., 2013). Research clearly shows that IPV leads to pervasive and long-term physical health concerns (Campbell et al., 2002; Coker, Davis, & Arias, 2002; Dillon, Hussain, Loxton, & Rahman, 2013), including increased risk of injury and death (Devries et al., 2011; Sheridan & Nash, 2007). IPV is also strongly linked to profound and debilitating negative mental health outcomes, such as depression, traumatic stress, and PTSD (Lacey et al., 2013; Lilly & Graham-Bermann, 2010; Nathanson, Shorey, Tirone, & Rhatigan, 2012). Furthermore, the extent of the violence is shown to lead to worse outcomes, which supports a dose–response relationship with IPV (Beydoun et al., 2012; Bogat et al., 2003; Bonomi et al., 2006; Golding, 1999). Thus, studying women’s exposure to IPV is complex and should include the examination of chronic engagement with multiple violent partners.
Women’s Engagement With Multiple Violent Partners
Women who have been in one violent relationship often tend to report involvement with other violent partners, although this is not the case for all IPV-exposed women (Alexander, 2009; Bogat et al., 2003; Coolidge & Anderson, 2002). Thompson et al. (2006) conducted a retrospective cohort study using a telephone survey (n = 3,568) of women aged 18 to 64 years enrolled in a U.S. health maintenance program for three or more years, and found that 10%-21% of IPV-exposed women reported abuse by two or more partners in their lifetimes. Likewise, Kemp, Rawlings, and Green (1991), using a sample of women whom they identified as “battered” and “non-battered” (n = 277) from shelters, counseling centers, and the community, revealed that 41% of women currently exposed to IPV reported a history of abuse with a previous (different) partner. Further research on IPV showed that among a sample of 93 women, 44% were exposed to a single violent relationship and 56% had multiple abusive partners in adulthood (Alexander, 2009).
Studies suggest that the majority of negative mental health outcomes are seen in IPV-exposed women with multiple violent partners, as compared with those who have only had one violent partner (Bogat et al., 2003). There is evidence that the past extent and severity of IPV in a woman’s life reliably predicts more negative mental health outcomes in women (Beydoun et al., 2012; Bogat et al., 2003; Bonomi et al., 2006; Golding, 1999). For example, Coolidge and Anderson (2002) found that women with multiple partners had significantly more depression than women with a single abusive partner, although this study did not control for duration of violent relationship exposure. In addition, these authors established that women with only one abusive relationship did not significantly differ in psychopathology from the control group that was matched for relationship status.
Defining Re-Engagement
Despite the significance of this issue, Cattaneo and Goodman (2005) identified important gaps in the current literature through a systematic review of 64 studies of what they termed re-abuse. The findings highlight discrepancies in how the concepts of re-abuse, re-victimization, and recidivism are defined (e.g., distinguishing between continued abuse within the same relationship or abuse in a new relationship). This inconsistency across studies makes the body of evidence inconclusive (Cattaneo & Goodman, 2005) and calls for further research with more clearly defined categories of abuse exposure. In the present study, we use the term re-engagement, meaning a woman’s involvement with multiple violent partners (including physical, sexual, and psychological abuse). In addition, Cattaneo and Goodman (2005) revealed that the majority of the research conducted on re-abuse has been perpetrator focused (i.e., the recidivism of the aggressor) and not on the characteristics associated with the women who have been abused. As such, the present study addresses a central gap in the literature, exploring the factors associated with women who have had multiple abusive partners.
The need for this research is clear from the evidence showing that abuse is a dyadic process, such that both partners’ (men’s and women’s) individual-level characteristics may increase IPV risk (Kuijpers, Van der Knaap, & Winkel, 2012; Moffitt, Robins, & Caspi, 2001). The present study challenges the prevailing conceptualization of women in some of the literature—for example, some feminist literature on domestic violence—as solely victims, which places them in a passive role with no subjectivity in their relationships. This is a limited and dangerous perspective, as it supports the notion of women as helpless objects with no agency in decision making. As such, in the present study, we address the issue of women’s involvement in IPV relationships from a strengths perspective, considering that women do have agency in partner selection, while also understanding that there are social- and individual-level factors that affect this agency. We are thus interested in exploring the social- and individual-level characteristics associated with women with multiple violent partners. Far from a “person-centered” blaming approach to understanding women who have been involved in IPV relationships, the exploration of the underlying mechanisms associated with women’s engagement with different abusive partners would allow for the development of interventions that could target women at increased risk, to address the social- and individual-level factors that those exposed could potentially influence (Dutton, 2009). This conceptualization is supported by previous work noting that IPV-exposed women may benefit from identifying factors that they can influence to decrease their vulnerability to abuse (Kuijpers et al., 2012).
Elements That May Predict Re-Engagement
As previously stated, little research has been conducted on the social- and individual-level characteristics of women that may predict their engagement multiple violent partners. While women’s overall IPV exposure (extent and severity) is not the same as engagement with multiple violent partners, it is plausible that the factors associated with overall exposure would likewise be connected to re-engagement. Due to the limited research with a focus on women with multiple IPV relationships, this study relies heavily on the literature on general exposure when necessary.
Findings have consistently shown an important connection between certain social-level factors and a woman’s increased risk of any exposure to IPV. In addition to the increased risk of IPV exposure in certain ethno-racial groups, as previously discussed, economic hardship has regularly been associated with women’s IPV exposure (Golden et al., 2013; Gonzalez-Guarda, Vasquez, Urrutia, Villarruel, & Peragallo, 2011; Rennison & Planty, 2003). Research has made clear that families living in impoverished conditions are more likely to have higher levels of stress, experience greater unemployment, be more socially isolated, and have an exacerbated sense of hopelessness, which may then lead to increased rates of IPV (as reviewed in Cummings, Gonzalez-Guarda, & Sandoval, 2013; Martin, Tsui, Maitra, & Marinshaw, 1999). Furthermore, studies have long revealed an association between lower education attainment and greater IPV exposure risk (Thompson et al., 2006). However, the few studies that have considered the issue of re-engagement have not found ethno-racial identification, income, or education to significantly predict involvement with multiple abusive partners (Alexander, 2009; Coolidge & Anderson, 2002). The persuasive evidence that these demographic characteristics are associated with greater IPV exposure challenges the more limited body of evidence that has not found these connections with IPV re-engagement. Further research is therefore needed to empirically explore this plausible connection.
Alexander (2009) is one of the few researchers to explore the characteristics of women who have been involved with multiple violent partners. Utilizing a sample of 93 women seeking IPV services, this study noted that a younger age of study participants predicted multiple victimizations. However, given the counterintuitive nature of this finding (a younger age providing a shorter amount of time to be in relationships), Alexander concluded that this result could be attributable to a cohort effect or the higher level of candidness of the younger women in the sample. Further research is therefore needed to better understand the relationship between a woman’s age and engagement with multiple violent intimate partners.
In this study, Alexander compared childhood trauma and attachment in women with a single violent partner with those with multiple violent partners. Findings established that women with multiple victimizations in adulthood were significantly more likely to have experienced multiple types of childhood trauma. This research adds to an ample body of literature that established a link between childhood abuse and increased IPV risk for women in adulthood (Briere & Jordan, 2004; Campbell, Greeson, Bybee, & Raja, 2008; Lilly, London, & Bridgett, 2014; Pico-Alfonso, Echeburúa, & Martinez, 2008; Thompson et al., 2006). Specifically, Whitfield, Anda, Dube, and Felitti (2003) demonstrated the way in which women’s childhood physical abuse increased their risk of IPV victimization in adulthood twofold and that childhood sexual abuse increased risk 1.8-fold. Furthermore, a study on childhood abuse and IPV in women (n = 1,521) during early pregnancy revealed that women with a history of childhood physical and sexual abuse had a 7.14-fold increase in lifetime odds of physical and sexual IPV (Barrios et al., 2015). The wealth of research on the connection between childhood abuse and adulthood IPV exposure highlights the importance of assessing trauma history when exploring the characteristics of women associated with engagement with multiple abusive partners.
While little research exists on the relation between women’s mental health and engagement with multiple violent partners, the strong associations between IPV exposure and women’s traumatic stress and depressive symptoms suggest that engagement with multiple violent partners may also be linked to women’s mental health symptoms. Among help-seeking samples, PTSD symptomatology has been found to be predictive of women’s repeated exposure to IPV (Krause, Kaltman, Goodman, & Dutton, 2006; Perez & Johnson, 2008). Furthermore, women’s depressive symptoms have been linked to their involvement in multiple violent relationships, and women with more than one violent partner have been found to be nearly 3 times as likely as women with a single partner to meet diagnostic criteria for depression, and more than twice as likely to meet criteria for a diagnosis of PTSD (Coolidge & Anderson, 2002). As the predictive effects of socio-demographic characteristics and prior trauma exposure on women’s engagement with multiple violent partners may be, in part, attributable to an increased risk for trauma and depressive symptoms, research that elucidates the relative contributions of each of these variables in predicting engagement with multiple violent partners is of great importance.
Alexander (2009) further established that women’s involvement in multiple abusive relationships was unrelated to their current IPV exposure. However, current exposure to sexual violence was not reported, which limits the extent of this evidence. Despite these important findings, this study used a help-seeking sample and therefore the results may not generalize to a community sample. Thus, research using a community sample may be needed to more comprehensively explore the individual and social-level factors associated with women’s engagement with multiple abusive partners.
Aims
Given that very little is known about the characteristics associated with women who engage with multiple abusive partners, the present study aims to identify a set of social- and individual-level factors correlated with women’s engagement in multiple IPV relationships. The present study seeks to inform the development and refinement of treatment and prevention interventions for IPV-exposed women, by identifying the social and individual mechanisms that may increase risk for further exposure to IPV in the future with a subsequent abusive partners. While not every risk factor can be included, such as substance use or abuse or characteristics of the abusive partner, in the present study, we assessed the most common variables found to be significant in prior studies of women exposed to IPV, for example, ethno-racial variation, demographic factors, trauma history, current trauma and depressive symptoms, and IPV exposure. Early identification and treatment of women with these vulnerabilities may reduce severity and chronicity of exposure to IPV and the serious mental health consequences that can result.
Hypotheses
Following the review of the literature on women’s engagement in IPV relationships with multiple partners, it is expected that specific social factors will be associated with involvement with more violent partners. Given the state of the current literature (only one study of age and number of violent partners to date) we pose an exploratory research question: is there a significant association between women’s age and their engagement with multiple violent partners? Furthermore, we hypothesize that ethno-racial identity will be significantly correlated with multiple violent partners such that African American and Latina women will have a greater number of violent partners compared with their White counterparts. Furthermore, as demographic factors associated with greater stress like low-income and low-education attainment have been previously linked to IPV exposure, we hypothesize that these will likewise be associated with greater re-engagement.
We also expect a number of individual-level variables from a woman’s past and current life to be linked to greater number of violent partners. As findings have consistently shown a connection between past physical and sexual abuse and current IPV exposure, we hypothesize that trauma history (physical and sexual violence and exposure to significant stressors) will be correlated with a woman’s greater engagement with multiple violent partners. Further, women’s current traumatic stress and depressive symptoms are expected to be positively associated with engagement with multiple violent partners, given the established associations between women’s IPV exposure and negative mental health outcomes. Finally, due to the chronic nature of this type of re-engagement, we hypothesize that women with more violent partners will also be exposed to more current IPV, including physical, sexual, and psychological violence.
Method
Participants (N = 164) were women with children who had been exposed to IPV within the previous 2 years who spanned ages 21 to 54 years (M = 33.39 years, SD = 7.47; Table 1). Participants were recruited to participate in a community-based clinical evaluation trial for women in Michigan, Ohio, Texas, and Ontario. Baseline data are used in the present study. This was a multiethnic sample with 21.18% of the women identifying as African American, 5.91% as Biracial, 44.83% as Latina, and finally 28.08% as White. Unemployment was high (58.57%) and monthly household income for the women ranged from US$0 to US$9,700 (M = US$1,067, SD = US$1,167) with wide variation between the different ethno-racial groups. The maximum education level attained was relatively low, as 11.11% of the sample had completed grade school or less, and 26.26% had completed some of high school. The majority of women were single, divorced, or separated (70.34%) at the time of the interview, 43.27% had ever visited a domestic violence shelter, and many had experienced a fair amount of housing instability over the past 4 years, with the number of times moved ranging from 0 to 15 (M = 2.82, SD = 2.59).
Demographic Characteristics of Women With One or More Than One Violent Partner.
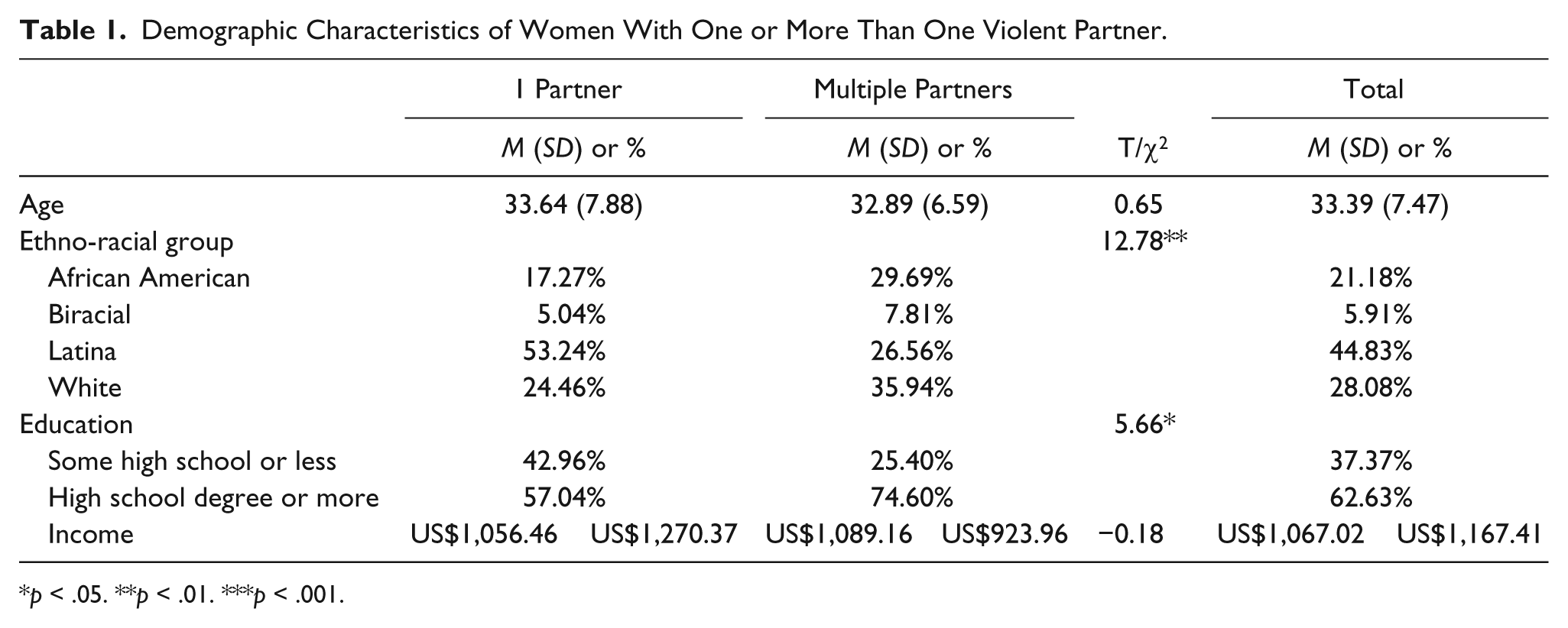
p < .05. **p < .01. ***p < .001.
Procedure
Following study approval from the university institutional review board, women were recruited through referrals from agencies providing services for IPV-exposed women and through postings in local businesses, school campuses, and social service agencies. Participants were enrolled in the study if they met the criteria of IPV exposure within the past 2 years. After providing written informed consent, women participated in a structured clinical interview in the language of their choice (English or Spanish). Female research assistants and graduate students in clinical psychology and social work, trained in clinical interviewing techniques and research ethics, administered the interviews. All interviewers received training from a supervising licensed psychologist. Interviews were held at the participating service agencies, the research facilities of the university, participants’ homes, or at local community businesses. During the interviews, participants were asked about current mental health, IPV exposure, trauma history, and demographic information. Interviews lasted approximately 1 to 2 hours, and participants were compensated in the amount of US$40 for their time. All rights of the participants were protected.
All measures that were given in the Spanish language were translated from the original version in the English language by a translation team. Translators were fluent in the Spanish language and had ample experience doing translation work. The questionnaires were then back-translated to ensure the accuracy of the translation. All Spanish-language interviewers were assessed by the members of the translation team to certify the quality and sensitivity of the interviewing process.
Measures
Demographic information
Demographic information was gathered during the interviews to capture the following information for each participant: age, ethno-racial identification, monthly household income, and education level.
IPV exposure
Women’s exposure to IPV was evaluated using the Revised Conflict Tactics Scale (CTS-2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). This measure is composed of five subscales that categorize the type of violence exposure: physical assault, psychological aggression, injury, sexual coercion, and negotiation with your intimate partner over the last year. The CTS-2 is a 78-item questionnaire in which the respondent indicates how often each incidence of violence has occurred with an intimate partner in the last year, ranging from zero (never) to seven (20 times or more). The measure includes items such as, “My partner punched or hit me with something that could hurt” or “You had a broken bone from a fight with your partner.” Although both violence victimization and perpetration of women is measured in the full CTS-2, only the 39 items associated with violence victimization were included due to the scope and aims of this study. Previous studies have established the good reliability and validity across the measure and subscales (Straus et al., 1996). Reliability for the present study was (α) .93. Reliability (α) for the subscales was .92 for physical assault, .85 for psychological aggression, .70 for injury, .70 for negotiation, and .87 for sexual coercion.
Information regarding women’s re-engagement in violent relationships over her lifetime was assessed by asking, “How many violent partners have you had in your lifetime?”
Traumatic stress symptoms and trauma history
Women’s current traumatic stress symptoms and trauma history were collected using the Posttraumatic Diagnostic Scale (PDS; Foa, Cashman, Jaycox, & Perry, 1997). The PDS is a 49-item self-report questionnaire that assesses the lifetime history of exposure to particular traumatic events and the frequency of posttraumatic stress symptoms over the past month. The first 12 items ask about a history of stressful events, such as non-sexual and sexual assault, childhood sexual abuse, torture, and having been held hostage. The PDS defines non-sexual assault as being mugged, physically attacked, shot, stabbed, or held at gunpoint; a sexual-assault includes rape or attempted rape (Foa et al., 1997). In its original form, the measure distinguishes between exposure to non-sexual and sexual assault by a family member or someone you know and by a stranger. A collapse of this distinction was conducted to reduce the number of predictor variables in the model. The new variables measured non-sexual assault (by a family member/someone you know or stranger) and sexual assault (by a family member/someone you know or stranger).
Items 22 through 38 of the PDS assess frequency of traumatic stress symptoms over the past month, using a scale from zero (not at all or only 1 time) to three (5 or more times a week/almost always). Sample items include “trying not think about, talk about, or have feelings about the traumatic event” and “reliving the traumatic event, acting or feeling as if it was happening again.” A total score is calculated using Items 22 through 38. Reliability for the present study was (α) .88.
Depressed mood
Depressed mood was measured using the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). This is a 20-item self-report scale that was developed to measure depressive symptomology. Women reported frequency of symptoms over the prior week on a 4-point Likert-type scale ranging from 0 = less than 1 day per week to 3 = most or all of the time (5-7 days). A summary score was tabulated by reverse coding the positive items (Items 4, 8, 12, and 16) and tallying the responses across all items. The CES-D has been examined in a variety of populations and has consistently shown excellent reliability (Miller, Anton, & Townson, 2008). Reliability for the present study was (α) .90.
Data Analysis Strategy
Ordinary least squares linear regression was conducted to determine the association between women’s engagement with multiple different abusive partners and their trauma history, current mental health symptoms, and type of current violence exposure. Demographic factors that have previously been linked to exposure to IPV were included in the analysis to control for any differences accounted for by these variables. Data were analyzed using Stata 14.
Results
Women’s current exposure to the three different types of IPV was high (Table 2). On average, the women reported experiencing 4.92 (SD = 5.61) acts of physical violence, 4.05 (SD = 5.91) acts of sexual abuse, and 12.25 (SD = 7.09) acts of psychological abuse over the last year. Psychological abuse emerged as the most frequent type of violence in this sample. Thirty-five percent of women had multiple violent partners. There was no significant difference in exposure to acts of physical violence between women with one violent partner and those who reported engagement with multiple violent partners. In addition, there were no significant differences between women who reported engagement with multiple violent partners and those with one violent partner in exposure to sexual and psychological abuse (Table 2).
Trauma History, Current Mental Health Symptoms, and Current IPV Exposure for Women With One or More Than One Violent Partner.

Note. IPV = intimate partner violence.
p < .05. **p < .01. ***p < .001.
Forty-nine percent of the sample reported having experienced at least one episode of non-sexual assault throughout their lifetime, with women with more than one violent partner being significantly more likely to have had a history of non-sexual assault than those with only one reported violent partner. Childhood sexual abuse was also prevalent in this sample, with 43.63% of the women reporting exposure to this history of trauma. Furthermore, there were significant differences in childhood sexual abuse between women with one violent partner and those who reported engagement with multiple partners, such that those with more than one violent partner were significantly more likely to have a history of childhood sexual abuse than those with only one violent partner. There were also significant differences in the history of having been held hostage. Here, women with a history of being held hostage were most likely to have multiple violent partners and those with only one violent partner were least likely to have been held hostage. Finally, women reported high levels of posttraumatic stress symptoms (M = 21.51, SD = 11.91) and depressive symptoms (M = 26.85, SD = 12.52). However, as shown in Table 2, there were no significant differences in terms of depressive symptoms and posttraumatic stress symptoms and whether the woman had one or more than one violent intimate partner.
Ordinary least squares linear regression modeling was used to examine the associations between re-engagement in violent relationships and the women’s age, ethno-racial identification, education level, income, trauma history, and current mental health symptoms (traumatic stress and depressive symptoms) and current IPV exposure (as shown in Table 3). The data collection site was not included as an independent variable in this model as it was too highly correlated with ethno-racial group to include both as predictors. The correlations between all predictors were examined using a correlation matrix, with no correlation between independent variables high enough to warrant concerns about multicollinearity. This was confirmed through inspection of the variance inflation factors and tolerance statistics (StataCorp, 2015).
Regression Results for Number of Violent Partners.
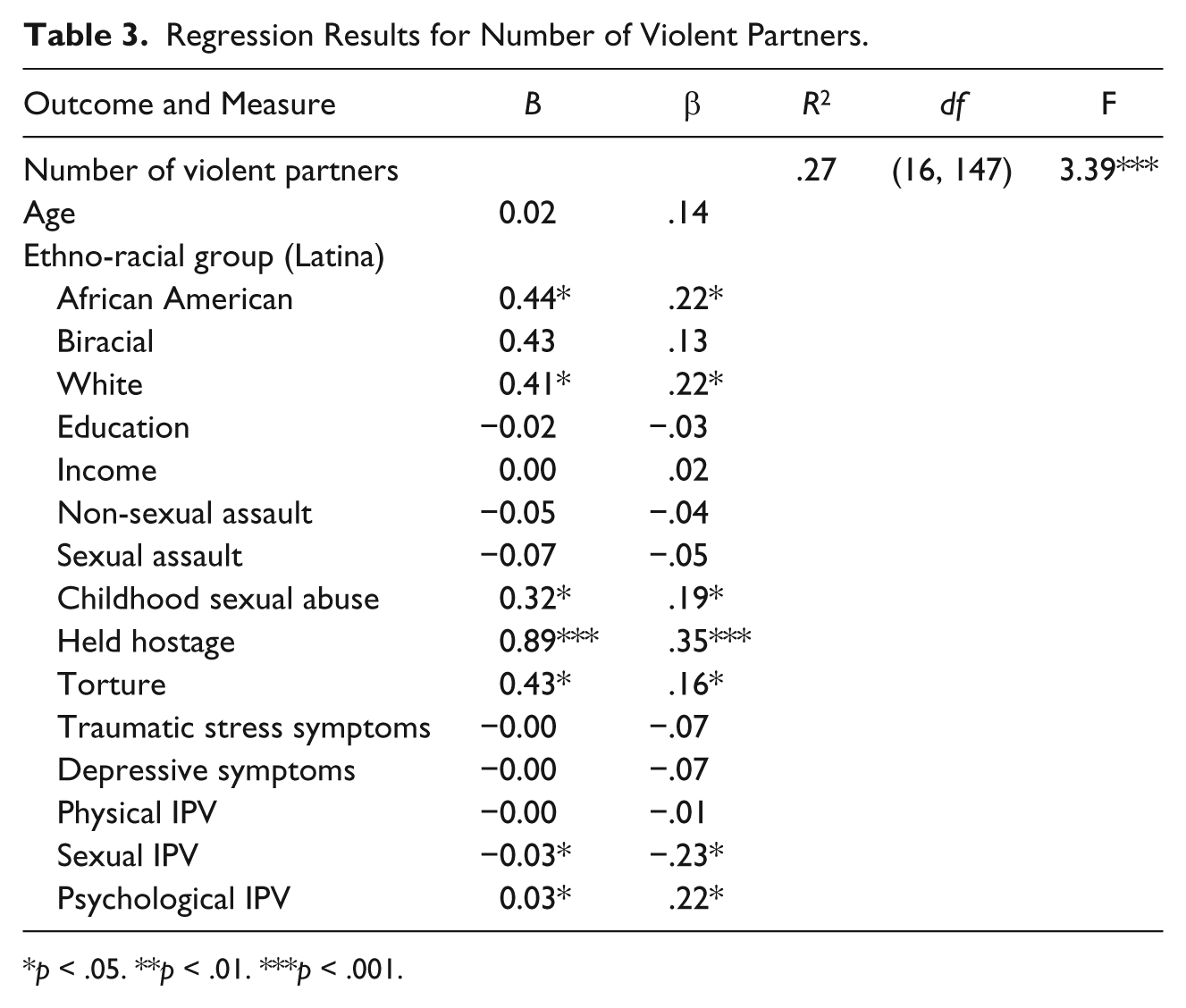
p < .05. **p < .01. ***p < .001.
The model accounted for 27% of the variance in women’s reported number of violent partners, F(16, 147) = 3.39, p < .001. Women’s ethno-racial group—being African American rather than Latina, (β = .22, p < .01) and White, (β = .22, p < .01), a history of childhood sexual abuse (β = .19, p < .01), a history of having been held hostage (β = .35, p < .001), a history of torture (β = .16, p < .01), current sexual violence by an intimate partner (β = −.23, p < .01), and current psychological violence by an intimate partner (β = .22, p < .01), uniquely were associated with the number of violent partners. F tests were conducted to compare all categories of the indicator variables for ethno-racial group identification. Results indicated that there were no significant differences between African American and biracial women, African American and White women, and biracial and White women for number of violent partners.
To summarize, a history of childhood sexual abuse, torture and being held hostage, and current psychological violence predicted the engagement with more violent partners. Furthermore, African American and White women had significantly more violent partners than their Latina counterparts. However, women with exposure to current sexual violence had a lower number of violent partners. Finally, women’s age, education level, income, history of non-sexual and sexual assault, current mental health symptoms, or even current physical violence were not found to be associated with the number of violent partners.
Discussion
Results partially supported the first hypothesis that the demographic factors of ethno-racial categorization, monthly income, and employment would significantly predict women’s greater number of violent partners. Findings revealed no significant relationship between women’s age and re-engagement. This is in contrast with previous results that noted that age does significantly predict re-engagement, such that a younger age predicted multiple victimizations (Alexander, 2009). One possible explanation for this discrepancy is the wider age range of the sample in the Alexander study (M = 37.4, SD = 11.2), which may have given that study greater ability to detect differences. In contrast, the present study sample had a mean age of 33.39 years (SD = 7.47 years). This difference in age variation might have contributed to the lack of findings in this area. Clearly, more work is needed to better understand the relationship between age and violence exposure by multiple partners.
Our results partially confirmed the hypothesis that ethno-racial classification was significantly associated with re-engagement, but in the opposite direction than predicted; Latina women had significantly fewer violent partners than their White and African American counterparts in this sample. This finding partially contradicts previous results showing significant differences in number of violent partners based on a woman’s ethnicity (Alexander, 2009; Coolidge & Anderson, 2002). This outcome is also interesting in relation to previous studies that have highlighted the way in which Latinas and African American women tend to be at risk for greater and more severe exposure to IPV than White women (Caetano et al., 2005; Clark et al., 2016; Field & Caetano, 2003). Taken together, these findings might indicate that Latinas’ severity of violence exposure occurs in the context of one relationship rather than over multiple relationships, potentially suggesting a different process of IPV. One potential explanation is that the Latinas in our sample were primarily Spanish-speaking immigrants living in the United States, meaning their freedom and capacity to leave a violent partner may have been more limited due to the many social barriers that immigrants face, such as difficulty accessing welfare and gaining employment. In addition, it would be important to consider the ways in which cultural factors like religious views and country of origin norms around relationships and marriage might influence the rate of re-engagement by Latina women.
Findings regarding the association between number of violent partners and income and educational attainment were not significant and did not support our initial hypothesis that women living with greater financial stress and with lower educational attainment would engage with more violent partners. These results support the conclusions from the small body of literature on re-engagement, which found that neither income nor education significantly predicted involvement with multiple abusive partners (Alexander, 2009; Coolidge & Anderson, 2002). However, these findings stand in contrast to previous literature that shows a consistent association between financial stress, education, and IPV exposure (Golden et al., 2013; Gonzalez-Guarda et al., 2011). Due to the overall low income and low educational attainment of this sample, perhaps what our results show is that being at the extremes of these groups does not significantly predict a higher number of violent partners. Additional research that includes a sample with greater range of level of income and educational attainment is needed to adequately explore the relationship between these social factors and engagement with multiple violent intimate partners.
The hypothesis that a woman’s past exposure to physical and sexual violence and her exposure to significant traumatic stressors would predict exposure to a greater number of violent partners was partially supported. The results indicate that childhood sexual abuse, history of being held hostage, and having been tortured significantly predicted to more violent partners. These findings support previous research showing that childhood sexual abuse increases risk for IPV exposure in adulthood (Alexander, 2009; Briere & Jordan, 2004; Campbell et al., 2008; Lilly et al., 2014; Pico-Alfonso et al., 2008; Thompson et al., 2006) in addition to studies that confirm the relationship between childhood sexual abuse and IPV re-engagement (Alexander, 2009). The findings that a history of having been held hostage and tortured were associated with increased re-engagement also support the literature that significant life stressors may contribute to increased risk of IPV exposure, in this case, to multiple violent partners (Bogat et al., 2003).
Still, other elements of trauma history including non-sexual and sexual assault were not significantly associated with a greater number of violent partners. This contradicts previous findings that have suggested that all childhood physical and sexual abuse increases risk for adulthood IPV (Golding, 1999; Whitfield et al., 2003). One plausible explanation for these disparate findings is the measurement of non-sexual and sexual assault in this study. Participants were asked if they had ever been exposed to non-sexual or sexual assault, thus not confining the time of exposure to childhood. Further studies that specify time of the assault would help to clarify these findings. Perhaps adulthood non-sexual and sexual assault is not correlated with increased risk of engagement with multiple partners, while it is in childhood.
Surprisingly, the hypothesis that women’s involvement with multiple violent intimate partners would be associated with greater concurrent traumatic stress and depressive symptoms was not supported by the present study. This finding is inconsistent with prior literature indicating such linkages; however, previous research has not studied these associations while controlling for demographic variables, IPV exposure, and history of exposure to other types of trauma. While it is clear from the literature that IPV is associated with greater mental health problems (Lacey et al., 2013; Lilly et al., 2010; Ouellet-Morin et al., 2015), interestingly, in this study, the presence of specific types of traumatic experiences rather than mental health sequelae of traumatic stress symptoms and depressive symptoms best predicted re-engagement.
Finally, we hypothesized that women who have had more violent partners would be exposed to more current IPV, including physical, sexual, and psychological violence. Again, our findings only partially supported this hypothesis: Physical violence did not significantly predict to a greater number of violent partners. Yet, women with a greater number of violent partners had significantly less current exposure to sexual violence and significantly more exposure to psychological violence. This adds to previous research that suggests current exposure to physical violence is not related to women’s IPV re-engagement (Alexander, 2009). The finding that exposure to less sexual violence is related to partner re-engagement is interesting and warrants further exploration. Given that this is a fairly new area of study, there is not sufficient evidence to explain this finding. Furthermore, the relationship between psychological violence and engagement remains unexplored. Perhaps the negative impacts associated with exposure to psychological violence increase risk for engagement with multiple violent partners.
Limitations
While this study provides strong evidence for the associations between ethno-racial identity, trauma history experiences, current IPV exposure, and number of violent partners, the study is not without limitations. All participants were women with children who self-disclosed exposure to IPV and who were enrolled in a community-based intervention trial for women and children exposed to IPV. These results may therefore not generalize to women who do not have children and women who are not ready to disclose exposure to IPV. Future studies could benefit from using a sample with greater diversity of participants including women without children and women who have not disclosed IPV exposure and collecting information regarding the timeline of significant life events, such as the timing of the birth of children and the onset of abusive relationships.
Information on trauma history and detailed data on women’s previous partners was limited. For example, women were free to interpret the meaning of the words being “held hostage,” a trauma history item, given their own experiences. Future studies could possibly benefit from more refined language for some of the trauma history items for greater specificity, in addition to collecting information regarding the extent and severity of women’s childhood trauma and exposure to parental IPV, as this data could provide further evidence for factors that may increase risk of engagement in IPV relationships with multiple partners in adulthood. Furthermore, a more comprehensive assessment of the duration and timeline of IPV exposure in current and all previous relationships could inform the understanding of chronicity and severity of violence and its relationship to continued cycles of violence with different partners. This appears to be a limitation of the extant literature exploring re-engagement (Cattaneo & Goodman, 2005) and is seen in Coolidge and Anderson (2002), who also did not specifically control for the duration of relationships of the women in their study. Thus, future research would benefit from collecting detailed information regarding the length and timing of all violent relationships, which may help to differentiate, for example, whether Latinas are actually more likely to have fewer violent partners or whether they are less likely to leave a violent relationship. Furthermore, data on women’s availability of options for leaving a violent relationship, substance use, social support, and interpersonal patterns of communication would be future lines of study that might help to further explain the mechanisms underlying engagement with multiple violent partners.
Finally, given the cross-sectional nature of this study, the types of conclusions that can be drawn are limited to associations among individual- and social-level factors and women’s number of violent partners. Future studies would benefit from a longitudinal design to allow for the exploration of characteristics that predict women’s involvement with a greater number of violent partners. Furthermore, a prospective longitudinal study would permit the reliable consideration of the role of mental health in engagement with multiple IPV partners.
Clinical Implications
Reliable evidence for factors that increase a woman’s risk for engagement with multiple abusive partners in adulthood remains limited, and thus, it is still too early in this research to make definitive and concrete suggestions for treatment interventions. Even so, this study’s reformulation of re-victimization as re-engagement moves women away from the domain of being passive victims in the repeated cycle of violence with different abusers. Understanding the social- and individual-level factors that may increase a woman’s risk for being involved with multiple violent partners in adulthood allows for a treatment perspective where women may reclaim a sense of agency and personhood. Focusing on the factors that increase their risk for this type of re-engagement potentially offers women the opportunity to address the social- and individual-level factors that they could potentially influence. At the same time, women’s ability to reduce their re-engagement in violence will substantially benefit from increased availability of social services and mental health services for women who have experienced IPV.
This research preliminarily suggests that a focus of interventions should be on factors that those exposed could influence to reduce their risk for IPV re-engagement. Specifically, interventions should address trauma history as it is highly correlated with a greater number of violent partners, including women’s childhood sexual abuse, a history of being held hostage, and of torture. However, further research is needed to understand the etiology of the connection between these trauma experiences and risk for re-engagement. One plausible explanation for this connection is the psychological processing (the way in which an individual processes and make sense of her experiences) of past traumatic events, which is amenable to intervention. In this case, treatment that focuses on processing and providing support around these traumatic experiences could potentially serve as a preventive function for future engagement with additional violent partners.
Attention to Diversity
The research reported here focused on a diverse population. Women who participated in this study were from a diverse set of racial and ethnic backgrounds. There was some income diversity in this sample; however, due to the nature of this community-based study, income for most of the women in the study tended to be low. Future research would benefit from attention to use of samples that afford a greater diversity of economic status, though IPV is often associated with lower income. Because of the nature of the social problem being studied, the focus of this study was on women, rather than on both men and women.
Conclusion
To contribute to the creation of effective treatment intervention tools, it is necessary to develop a more complex understanding of what is influencing women’s engagement with multiple abusive partners. Identifying the underlying mechanisms that are contributing to a woman’s risk for re-engagement can inform treatment and can eventually be used to develop preventive interventions for at-risk women. As little is known about these underlying mechanisms, current interventions targeted at stemming women’s future engagement in violent relationships may have limited effectiveness. Thus, developing a greater understanding of what affects a women’s agency in partner selection is both an important and timely contribution to the field. This evidence can be used to inform ways in which to tailor both treatment and prevention programs to the needs of women in the community.
Footnotes
Authors’ Note
The views expressed in this article do not necessarily reflect those of the granting agencies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Blue Cross and Blue Shield of Michigan Foundation and the Office of the Provost, University of Michigan, Global Challenges for a Third Century grant.