
Abstract
Although many studies have assessed gender differences in posttraumatic stress disorder (PTSD) prevalence, few examine individual PTSD symptoms (PTSSs). Hypothesizing that trauma differences explain many gender differences in symptomatology, this is the first known study to adjust PTSSs for trauma type, and to compare gender differences in those with sexual traumas. Using a cross-sectional survey methodology in a sample of adult outpatients (n = 775), we examined gender, trauma type, PTSSs, suicide, alcohol, and tobacco. Among those with trauma (n = 483), women generally had more severe symptoms than men, but after adjusting for trauma type, only physical reactivity (p = .0002), excessive startle (p = .0005), external avoidance (p = .0007), internal avoidance (p = .0008), psychological reactivity (p = .0009), and suicide attempts (p = .001) remained significantly worse among women, whereas men more commonly reported alcohol problems (p = .007). Among those with PTSD (n = 164), there were no significant PTSS gender differences. Those with sexual trauma had worse symptoms (particularly amnesia) compared with non-sexual trauma (p < .0001 for PTSD diagnosis and total severity), including within each gender. Among those with sexual trauma (n = 157), men had worse recklessness (p = .004) and more commonly reported tobacco (p = .02), whereas women more commonly attempted suicide (p = .02) and had worse avoidance (p = .04). However, when isolating the effects of sexual trauma beyond other traumas, there were no significant symptom difference-in-differences between genders. Our findings suggest that, while women have higher PTSD rates, men with PTSD present similarly. In addition, while women have higher sexual trauma rates, men may have similarly severe responses. Most gender differences in PTSD presentation appear to be explained by trauma type, particularly women having higher rates of sexual trauma. We discuss potential biopsychosocial explanations.
Introduction
Despite a plethora of research examining differences between men and women in posttraumatic stress disorder (PTSD) prevalence and total symptom severity (Christiansen & Elklit, 2012; Ditlevsen & Elklit, 2012), gender differences in individual PTSD symptoms (PTSSs) are understudied. Analyzing these differences may improve our understanding of etiology, gender differences in stress responses and prevalence, and PTSD screening and treatment. Of the few PTSS gender difference studies, most focus on specific trauma types, such as motor vehicle collisions (Fullerton et al., 2001), assault (Galovski, Mott, Young-Xu, & Resick, 2011), or combat (King, Street, Gradus, Vogt, & Resick, 2013). Carmassi et al. (2014) is the only study to examine gender differences using Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5; American Psychiatric Association [APA], 2013) criteria, but was specific to an earthquake in Italy. Some studies include all trauma types (Green, 2003; Kobayashi & Delahanty, 2013), but, like those above, the samples were either trauma or PTSD patients. To our knowledge, ours shall be the first study to
assess gender differences using DSM-5 criteria among all trauma types,
adjust for trauma types, and
analyze PTSSs in trauma patients that came from a large clinical sample without a known trauma history.
The second novelty is important because, though researchers have hypothesized that many PTSD gender differences are due to trauma type differences (Tolin & Foa, 2006), our PubMed and PsycINFO searches did not yield any studies adjusting for trauma type. The third novelty is important because it (a) decreases selection bias risk by not only including those presenting specifically for trauma or PTSD, (b) allows for comparing all those with trauma with the subset who have PTSD, and (c) reflects the progression of how providers screen patients (i.e., all patients are screened for trauma, and all those who screen positive are screened for PTSD).
Because women have higher rates of PTSD and of sexual trauma than men (Christiansen & Elklit, 2012), we elected to pay particular attention to this trauma type. If trauma type does explain most gender differences in PTSSs, we suspect sexual trauma is the main culprit. We examined four groups: men with sexual trauma, women with sexual trauma, men with non-sexual trauma, and women with non-sexual trauma. Although some have examined total PTSS severity in men (Schry et al., 2015), to our knowledge, this is the first study to
analyze individual PTSSs in men with sexual trauma,
compare individual symptoms between the genders among those with sexual trauma, and
compare individual symptoms in those with sexual and non-sexual trauma.
Sexual trauma in men remains an understudied realm of the trauma literature. Most research about sexual trauma focuses on women, and what little exists about men is generally relegated to quantifying prevalence (Department of Defense [DoD], 2014; Kimerling, Gima, Smith, Street, & Frayne, 2007). Gender differences in the effects of sexual trauma are poorly understood. Understanding these differences could be important for screening, especially because research suggests sexually traumatized men face several hurdles in receiving care: fewer resources, less advocacy, and less public/provider understanding of sexual trauma that is not man to woman (Draucker & Martsolf, 2010; Turchik & Edwards, 2012).
With few exceptions (Chung & Breslau, 2008; Freedman et al., 2002), most previous research demonstrates gender differences in PTSSs. The most consistent findings (i.e., in at least two studies from PubMed and/or PsycINFO) are men having worse irritability/aggression than women (Galovski et al., 2011; Green, 2003; Olff, Langeland, Draijer, & Gersons, 2007), and women having worse insomnia (Carmassi et al., 2014; Fullerton et al., 2001; Kobayashi & Delahanty, 2013), intrusive memories (Carmassi et al., 2014; Kobayashi & Delahanty, 2013), anhedonia (Carmassi et al., 2014; Fullerton et al., 2001), physical reactivity (Fullerton et al., 2001; Kobayashi & Delahanty, 2013), psychological reactivity, and inattention than men (Fullerton et al., 2001; King et al., 2013). Based on previous research and clinical experience, we hypothesized the following:
Method
Participants
This study was reviewed by the Wright-Patterson Air Force Base Institutional Review Board (IRB), which exempted it as a cross-sectional study with anonymous surveys (Exempt Category 2) and allowed for consent to be implied by survey completion rather than documented. Participants were recruited from October 2014 to February 2015. Participants were non-emergent outpatients at a military medical center treating active duty and retired service members, and families. During clinic hours, investigators approached consecutive incoming patients. Potential participants were excluded if less than 18 years old, or in apparent physical/psychological distress. Each participant was asked to complete an anonymous survey, then place it into a sealed envelope in a collection box in the lobby. Consent was implied by survey completion as explained on the survey cover page, which participants were encouraged to keep as it contained the nature, purpose, and risks of the study, and IRB contact information.
Of the 1,000 surveys distributed to eligible participants, 775 (77.5%) were returned. Of these, 46.7% were women and the mean age was 38.6 years. Regarding military status, 48.8% were active duty, 23.5% were dependents, 19.0% were retired, 6.5% marked “other” (e.g., non-active reserves, non-retired separated), and 2.3% did not respond. Of the total sample, 483 (62.3%) reported experiencing trauma and, of those with trauma, 164 (21.2% of the total sample) met DSM-5 PTSD criteria based on the PTSD Checklist for DSM-5 (PCL-5). Participants were considered to meet DSM-5 PTSD criteria if they reported a trauma history along with at least moderate severity (2-4 on the 0-4 PCL-5 scale) of the following: at least one intrusion symptom, at least one avoidance symptom, at least two mood/cognitive symptoms, and at least two hyperarousal symptoms. To be conservative, less than moderate symptoms were not considered sufficient for diagnosis.
Table 1 summarizes participant characteristics. There were no significant gender differences in age or race among all participants (p = .9004 and .0757, respectively), those with trauma (p = .3497 and .3386, respectively), or PTSD (p = .8572 and .3575, respectively). Among all participants, there was no significant gender difference in number of traumas (p = .9211), but women more commonly reported sexual assault (p < .0001), child sexual abuse (p < .0001), child physical abuse (p = .0003), and physical assault (p = .0115). Men more commonly reported combat (p < .0001), terrorism (p < .0001), motor vehicle collisions (p < .0001), and natural disasters (p = .0207). Among those with sexual trauma (n = 157), 19.7% were men and the mean age was 38.8 years. The sexual trauma group included those with sexual assault or sexual abuse (± other trauma types) and the non-sexual trauma group included those with only non-sexual trauma types. Three participants did not respond to at least one of the questions about suicide or alcohol/tobacco, for which the sample sizes were 480 and 481, respectively.
Participant Characteristics, Including for Subsets With Any Trauma and DSM-5 Criteria for PTSD.

Note. The bolded values represent statistically significant greater levels than other gender. DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.); PTSD = posttraumatic stress disorder.
Measures
The survey assessed PTSSs using the PCL-5, the latest version of the PCL and a 20-item self-report measure based on DSM-5 criteria (Weathers et al., 2014). The PCL is commonly used, and has strong internal consistency, reliability, and validity (Blevins, Weathers, Davis, Witte, & Domino, 2015). The rest of the survey contained questions based on DSM-5 (APA, 2013) and surveys previously used by Sansone, Watts, and Wiederman (2013). These inquired about demographics; any trauma as defined by the DSM-5; 12 specific trauma types (child neglect, child physical abuse, child sexual abuse, combat, motor vehicle collision, life-threatening injury or illness, natural disaster, physical assault, terrorism, sexual assault, violent death of a loved one, witnessed violence) and a write-in section for other types; difficulty in controlling use of, or social, occupational, legal, or medical problems due to the use of, alcohol and tobacco; and history of suicide attempts. We omitted illicit drug-related problems in favor of only legal substances (i.e., alcohol and tobacco) because active duty participants (who were more commonly men) are beholden to strict anti-drug policies, which would likely skew comparisons.
Data Analysis
Demographic characteristics (Table 1) were compared between genders using t tests for continuous variables and Fisher’s exact test for categorical variables. Ordinal logistic regression was used to test for group differences in PTSS severity, both unadjusted and adjusted for trauma type. However, because means are more straightforward to present and interpret than the multiple odds ratios resulting from ordinal logistic regression, we present means of PTSS severity (with statistical significance still based on ordinal logistic regression). Differences in means between groups are presented such that positive differences indicate that those with sexual trauma (vs. those with only non-sexual trauma) or men (vs. women) had the larger mean. Binary logistic regression was used to test for group differences in DSM-5 PTSD, suicide attempts, alcohol- and tobacco-related problems, with results presented as odds ratios (>1 indicates men [vs. women] or those with sexual trauma [vs. those with only non-sexual trauma] had the greater proportion).
In the following, M = men, W = women, ST = those with sexual trauma, non-ST = those with only non-sexual trauma. For each outcome, we conducted the following comparisons, with the corresponding hypothesis in parentheses:
M versus W, unadjusted (H1), adjusted for non-sexual trauma types only, and adjusted for both non-sexual and sexual trauma types (H2, H3);
ST versus non-ST, unadjusted and adjusted for trauma type (H4);
M-ST versus M-non-ST, unadjusted and adjusted for non-sexual trauma types (H4);
W-ST versus W-non-ST, unadjusted and adjusted for non-sexual trauma types (H4);
M-ST versus W-ST, unadjusted, adjusted for non-sexual trauma types only, and adjusted for both non-sexual and sexual trauma types (H5); and
(M-ST vs. M-non-ST) versus (W-ST vs. W-non-ST), unadjusted and adjusted for non-sexual trauma types (H6).
Analyses were conducted separately for each comparison for trauma type adjustments to be distinct for each analysis. Each of the 12 specific trauma type variables was binary (yes/no) indicating whether or not a patient had experienced that particular trauma. Adjustments for trauma type were conducted via stepwise selection, starting with the 10 non-sexual trauma types or all 12 trauma types, depending on the analysis, and allowing variables to leave and enter the model if doing so resulted in a reduction in Akaike information criterion (AIC; Akaike, 1974). Multi-collinearity was checked using variance inflation factors and was found to be low (<1.9). Each set of comparisons of the 20 PTSSs was adjusted for multiple testing using the Hommel procedure (Hommel, 1988) with a family-wise Type I error (α) rate of .05.
For H6, significance of the difference-in-differences was determined using a z test assuming normality of the difference in effects (on the logit scale for outcomes tested using ordinal or logistic regression), with variance computed as the sum of the variances of the independent (M-ST vs. M-non-ST) and (F-ST vs. F-non-ST) differences.
Results
Figure 1 displays gender differences in PTSS severity, among those with trauma, those with PTSD, and between those with sexual trauma and those with only non-sexual trauma.

Gender differences in PTSD symptom severity, among those with trauma, those with PTSD, and between those with ST and those with only non-sexual trauma.
Men Versus Women
Table 2 summarizes gender differences in PTSD-related outcomes (H1), unadjusted and adjusted for trauma type (H2 and H3). Among those with trauma, women (39.0%) had significantly higher PTSD rates than men (29.4%) when unadjusted (p = .0265) and adjusted for non-sexual trauma types only (p = .0050), but the difference was not significant when also adjusting for sexual trauma (p = .0822). Women had worse total PTSS severity than men when unadjusted (p = .0013), adjusted for non-sexual trauma types (p < .0001), and adjusted for sexual trauma (p = .0115), although the difference decreased in magnitude when adjusting for sexual trauma. Women had greater severity than men in most PTSSs when unadjusted or adjusting for non-sexual trauma types only, but most differences decreased in magnitude and many were no longer significantly different after also adjusting for sexual trauma. The only PTSSs remaining statistically significant after adjusting for all trauma types and multiple testing (all worse among women than men) were physical reactivity (p = .0002), excessive startle (p = .0005), external avoidance (p = .0007), internal avoidance (p = .0008), and psychological reactivity (p = .0009). Unadjusted and adjusted, women were significantly more likely to report suicide attempts than men (p = .0001 and p = .0013, respectively), and men were significantly more likely to report alcohol-related problems than women (p = .0086 and p = .0071, respectively). Men more commonly reported tobacco-related problems than women (p = .0548), significantly so after adjusting for trauma type (p = .0024).
Gender Differences in PTSD Outcomes, UN, and ADJ for NST Only and All Trauma Types.

Note. Effect sizes (Δ) for mean comparisons are differences in means, and for prevalence comparisons (%) are ORs. The bolded values represent significantly greater levels than other trauma group (for the 20 PTSD symptoms, only if significant after adjusting for multiple testing). PTSD = posttraumatic stress disorder; UN = UNadjusted; ADJ = ADJusted; NST = non-sexual trauma; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.); OR = odds ratio.
p < .05. **p < .01. ***p < .001.
Among those with PTSD, there were no significant gender differences in PTSSs after adjusting for multiple testing. After adjusting for all trauma types, three were significantly different prior to adjusting for multiple testing (all worse among men): hypervigilance (p = .0030), nightmares (p = .0103), and recklessness (p = .0236). Men had significantly worse arousal cluster severity (p = .0242), but not after adjusting for all trauma types. Unadjusted and adjusted, women were significantly more likely to report suicide attempts than men (p = .0006 and p = .0012, respectively), and men were significantly more likely to report alcohol-related problems than women (p = .0122 and p = .0039, respectively). Men more commonly reported tobacco-related problems than women, significantly so after adjusting for trauma type (p = .0105).
Sexual Trauma Versus Only Non-Sexual Trauma
Table 3 summarizes the differences between those with sexual trauma and non-sexual trauma, both among all those with trauma and by gender (H4). Those with sexual trauma had significantly greater total PTSS severity than those with only non-sexual trauma among the total sample (p < .0001), men (p = .0005) and women (p < .0001). Among all participants, those with sexual trauma had significantly higher (p < .0001) PTSD prevalence (49.7%) than those with non-sexual trauma (26.4%), with similar rates among men (p = .0049) and women (p = .0006). Almost all outcomes were significantly different in the total sample, except recklessness and tobacco-related problems. Those with sexual trauma had significantly worse irritability/aggression unadjusted (p = .0047) and adjusted for non-sexual trauma types (p = .0134). Those with sexual trauma were significantly more likely to report suicide attempts but only unadjusted (p = .0006), and those with only non-sexual trauma were significantly more likely to report alcohol problems but only after adjusting for non-sexual trauma (p = .0483).
PTSD Outcomes in Those With ST Versus Only NST, UN, and ADJ for NSTs.

Note. Effect sizes (Δ) for mean comparisons are differences in means, and for prevalence comparisons (%) are ORs. The bolded values represent significantly greater levels than other trauma group (for the 20 PTSD symptoms, only if significant after adjusting for multiple testing). PTSD = posttraumatic stress disorder; ST = sexual trauma; NST = non-sexual trauma; UN = UNadjusted; ADJ = ADJusted; OR = odds ratio.
p < .05. **p < .01. ***p < .001.
When comparing men with sexual trauma with men with only non-sexual trauma, all outcomes except suicide attempts were more common among the former. After adjusting for non-sexual trauma types (and multiple testing in PTSSs), the differences remaining significant (all greater among men with sexual trauma) were amnesia (p < .0001), negative feelings (p = .0007), nightmares (p = .0021), irritability (p = .0046), and tobacco problems (p = .0421). The total PTSS and cluster severities all remained significantly greater among men with sexual trauma after adjusting for non-sexual trauma.
Most outcomes were significantly worse among women with sexual trauma than women with only non-sexual trauma. After adjusting for non-sexual trauma types (and multiple testing for PTSSs), the differences remaining significant (all greater among women with sexual trauma) were excessive startle (p = .0009), external avoidance (p = .0003), blame (p = .0008), amnesia (p = .0016), and detachment (p = .0039). In addition, the total and cluster severities, and PTSD prevalence, all remained significantly greater among women with sexual trauma.
Men With Sexual Trauma Versus Women With Sexual Trauma
Table 4 summarizes the gender differences among those with sexual trauma (H5) and the gender differences in sexual trauma differences (H6). Among those with sexual trauma, most outcomes were not significantly different between men and women. After adjusting for all trauma types (and multiple testing for PTSSs), only a few differences were significantly greater: tobacco-related problems among men (p = .0160) and suicide attempts (p = .0151) and total avoidance severity among women (p = .0354). The largest difference in PTSS severity was men having worse recklessness, but this was not significant after adjusting for multiple testing. The difference-in-differences analysis (H6) demonstrated that outcomes were generally worse for those with sexual trauma than for those with only non-sexual trauma, but the magnitudes of these differences were generally greater in men than women. Differences in recklessness, irritability/aggression, nightmares, and negative feelings were noticeably greater in men than women, but not significantly so. No differences were statistically significant, whether unadjusted or adjusted for trauma type (and after adjusting PTSSs for multiple testing).
Gender Differences in PTSD Outcomes in Those With ST, and Gender Differences in Gender-Specific Differences in Outcomes Between Those With ST and NST, UN and ADJ for All Trauma Types and NST Only, Respectively.
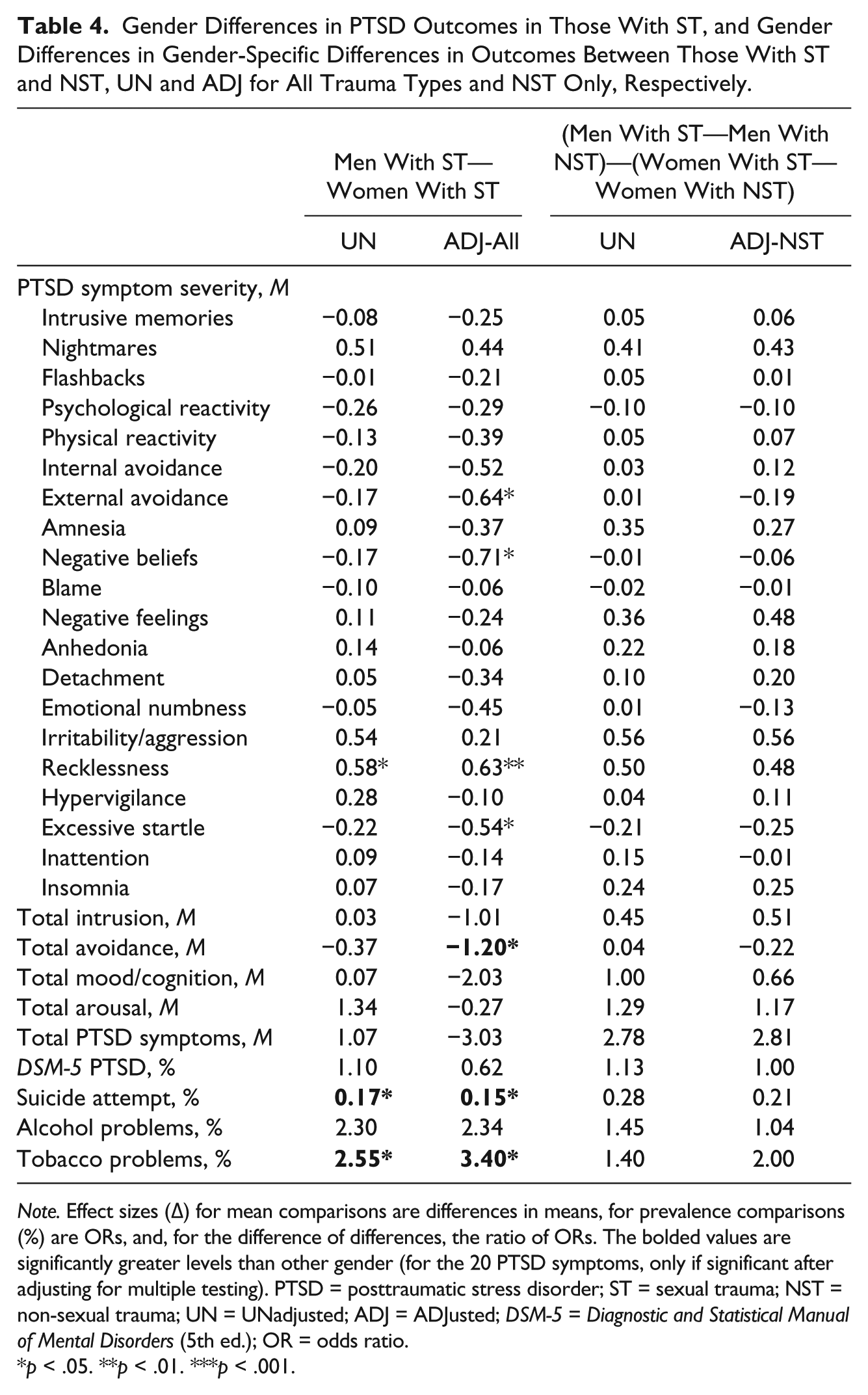
Note. Effect sizes (Δ) for mean comparisons are differences in means, for prevalence comparisons (%) are ORs, and, for the difference of differences, the ratio of ORs. The bolded values are significantly greater levels than other gender (for the 20 PTSD symptoms, only if significant after adjusting for multiple testing). PTSD = posttraumatic stress disorder; ST = sexual trauma; NST = non-sexual trauma; UN = UNadjusted; ADJ = ADJusted; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders (5th ed.); OR = odds ratio.
p < .05. **p < .01. ***p < .001.
Discussion
As expected, both gender (H1) and trauma type (H2 and H3) affect PTSD symptomatology, and most gender differences are in part explained by sexual trauma (H3). Those significantly different outcomes (all worse among women) that were largely explained by trauma type (i.e., large reductions in magnitude of difference) were amnesia, negative beliefs, blame, and negative feelings. The significantly different outcomes not explained by trauma type were physical and psychological reactivity, internal and external avoidance, and excessive startle being worse, and suicide attempts being more common among women, and alcohol and tobacco problems being more common among men.
Sexual trauma was associated with worse outcomes (e.g., PTSD prevalence and symptom severity, particularly amnesia) than non-sexual traumas among the total sample, men, and women (H4). Taken together with our other findings, suicide attempts, avoidance, physical reactivity, and excessive startle seem particularly associated with women (H1 and H5); alcohol with men (H1); mood/cognitive symptoms with sexual trauma (H4); and recklessness, tobacco, and irritability with sexual trauma in men (H5). Consistent with our predictions, there were few gender differences among those with sexual trauma. In fact, the difference-in-differences analysis demonstrated very small effect sizes and no significant gender disparities, suggesting that sexual trauma affects men and women to a similar degree beyond other traumas (H6).
Because of the paucity of studies on this topic, we are left to speculate about potential biopsychosocial explanations for our results, which we hope will stimulate further research to better understand PTSD symptomatology, neurobiology, and clinical application.
Women Generally Have Worse Trauma-Related Outcomes
This study finds more severe stress responses and higher PTSD rates among women than men, consistent with previous research (Christiansen & Elklit, 2012; Kessler, Chiu, Demler, Merikangas, & Walters, 2005; Olff et al., 2007; Tolin & Foa, 2006). Like past studies, we find that traumatized women have worse intrusive memories (Carmassi, 2014; Kobayashi & Delahanty, 2013), psychological reactivity (Fullerton et al., 2001; King et al., 2013), physical reactivity (Fullerton et al., 2001; Kobayashi & Delahanty, 2013), avoidance (Carmassi, 2014; Fullerton et al., 2001), excessive startle (Carmassi, 2014; Fullerton, 2001), and negative feelings (Carmassi, 2014). To our surprise, men did not have any significantly worse individual PTSSs. The only PTSS outcomes significantly worse among men were the arousal cluster among those with PTSD. Alcohol- and tobacco-related problems were more common among traumatized men, consistent with previous studies (Green, 2003; Solomon, Smith, Robins, & Fischbach, 1987; Zlotnick, Zimmerman, Wolfsdorf, & Mattia, 2001) and possibly explained by evidence that alcohol has greater anxiety-reducing effects on men than women (Tolin & Foa, 2006).
A potential explanation for women having worse trauma-related outcomes is intrinsic biological and psychological gender differences in stress response. For example, females have more cortisol dysregulation (implicated in PTSD; Yehuda, 1999), hypothalamic-pituitary-adrenal axis activation (Ogilvie & Rivier, 1997), and fear-induced sympathetic activation than males (Tolin & Foa, 2006). Taken together with our finding that physical reactivity and excessive startle are the only symptoms for which the magnitude of the differences becomes larger (both worse among traumatized women) when adjusting for trauma type, these particular symptoms may be explained by biological factors inherent in women. Psychologically, traumatized women are more likely to exhibit internalizing defenses (e.g., anxiety, depression) and men are more likely to externalize (e.g., impulsivity, aggression; Kessler et al., 2005; Miller & Resick, 2007; Rosenfeld, 2000; Tolin & Foa, 2006). These differences may explain why suicide attempts were more common and avoidance worse among women, and alcohol problems were more common and arousal worse among men. Another potential psychological explanation is that women are more likely to self-blame, which has been theorized to contribute to increased PTSD prevalence among women (Christiansen & Elklit, 2012). Introduced in DSM-5, blame was not assessed in studies using previous criteria, but our study did find that women tend to have greater levels than men (although the gender difference was largely explained by sexual trauma). Finally, research has suggested that avoidant coping skills interfere with natural recovery—especially among women who also have high reactivity to trauma-related cues (APA, 2013; Pineles et al., 2012). Therefore, the combination of higher levels of avoidance and physical/psychological reactivity that we found in women compared with men may partially explain (i.e., the coefficients are smaller) the higher PTSD prevalence among women.
When Men Get PTSD, It Is Just as Severe as in Women
The lack of PTSS gender differences within the PTSD subset suggests that, whereas PTSD is more prevalent among women, when men do develop PTSD, they present similarly. Our findings of no significant PTSS gender differences among PTSD patients is consistent with some past research (Chung & Breslau, 2008; Freedman et al., 2002)—although both studies were of trauma patients but not specific to those meeting criteria for PTSD. Considering the greatest differences (even if not significant) were worse among men, our results suggest that, short of PTSD, women generally have worse trauma-related outcomes, but when men also meet criteria for PTSD, their symptoms are usually just as severe, if not worse.
Although conclusions cannot be made based on failure to reject the null hypothesis, the lack of large PTSS gender differences among those with PTSD suggests that men and women meeting DSM-5 criteria may reliably have the same, distinct disorder. Observing the changes between the trauma and PTSD groups (realizing they are subsets of each other), one sees that PTSSs become more homogenized between the genders. This creates a potential for relatively severe responses to negative experiences to go unrecognized for those not meeting the strict, categorical DSM-5 criteria. For example, 36 participants (15 men, 21 women) met symptomatic criteria for PTSD but not full criteria due to a lack of a trauma (the PCL-5 instructs symptom reports to be based on a “very stressful experience” rather than specifically a trauma). This suggests a need to reconsider when a stressful experience may be considered a trauma. Furthermore, many participants met DSM-5 criteria for trauma and some clusters without meeting full criteria (e.g., 80 participants with a trauma history met mood/cognitive criteria but not the other three clusters). Although DSM-5 has created other stressor-related disorder categories in which subthreshold PTSD patients may fit, these are not well understood or accounted for in non-clinical settings. For example, in the military, not meeting strict PTSD criteria can have negative occupational/financial consequences (Guina, Welton, Broderick, Correll, & Peirson, 2016), which can miss the multi-finality of trauma (i.e., some will develop PTSD, some will develop other disorders, and some will demonstrate resilience; Bonanno et al., 2012). Although policy changes to the military disability system may be more appropriate to address these specific concerns, changes in diagnostic criteria can also help ensure all those with trauma-related distress/dysfunction are adequately recognized.
Sexual Trauma Is Associated With Worse Outcomes
Our findings are consistent with previous research demonstrating that sexual traumas are associated with higher rates of PTSD (Kimerling, Ouimette, & Wolfe, 2002), suicide attempts (Darves-Bornoz, Choquet, Ledoux, Gasquet, & Manfredi, 1998), and internalizing symptoms (Miller & Resick, 2007) than other trauma types. However, our study is unique in its comparisons of both gender and trauma type, which allows us to conjecture that both factors do not necessarily affect outcomes additively. For example, suicide attempts were most common in women with sexual trauma (28.6%) followed by women with only non-sexual trauma (15.4%), men with only non-sexual trauma (10.0%), and—unexpectedly, last—men with sexual trauma (6.5%). Without separating gender and trauma type, one would expect sexual trauma to correlate with more suicide attempts in both genders rather than just women. Based on our results, both gender and trauma type may influence suicide attempts and other outcomes to varying degrees.
Amnesia was the only symptom that was significantly greater in those with sexual trauma in both genders (combined or separate), and when adjusting for trauma type and multiple testing. Dissociative memory loss has been associated with sexual traumas and child abuse (APA, 2013; Wechsler-Zimring & Kearney, 2011), both of which are more common in women. Regardless of gender, child traumas can result in memory problems and dissociative amnesia via cortisol-induced hippocampal degeneration (Bremner & Narayan, 1998; Joseph, 1999; Weniger, Lange, Sachssee, & Irle, 2008).
Although most outcomes were worse among men with sexual trauma than men with only non-sexual trauma, some stand out as distinctly worse in the former. Tobacco problems and recklessness were the only outcomes consistently much greater among men with sexual trauma when compared with both women with sexual trauma and men with only non-sexual trauma. This suggests that these outcomes are the most uniquely associated to men with sexual trauma. In fact, when adjusting for secondary trauma types, their magnitudes of man–woman differences both increased. Tobacco has previously been associated with sexual trauma in men (Al Mamun et al., 2007). Recklessness (which is distinctly different from the other PTSSs in the sexual trauma spiderweb chart in Figure 1) has been separately correlated with sexual trauma (Carballo-Dieguez & Dolezal, 1995) and men, in general (Carmassi, 2014), but never before has been demonstrated to be so uniquely severe among men with sexual trauma.
Sexual Trauma Largely Explains Many Gender Differences
Women generally having worse trauma-related outcomes than men is not related to women having more trauma as our sample had no significant gender difference in either trauma prevalence or number of traumas (in fact, a post hoc analysis demonstrated that adjusting for number of traumas rather than trauma type was, when different, generally more similar to unadjusted analyses). Furthermore, past research demonstrates that while women have higher PTSD rates, men have higher trauma rates, and, even among those with trauma, women have higher PTSD rates and worse total PTSS severity than men (Tolin & Foa, 2006). Therefore, rather than more trauma, differences are more likely due to different types of trauma. One previous study (Ditlevsen & Elklit, 2012) determined higher rates of PTSD among women were not explained by trauma type, but it should be noted that the study did not differentiate sexual traumas as one of the specified trauma types and did not assess individual PTSSs. Many have hypothesized trauma type influences gender differences in PTSSs (Tolin & Foa, 2006), and ours is the first known study to demonstrate it.
Consistent with our hypothesis, although women generally had more severe responses to trauma than men, many of these differences became much smaller after adjusting for sexual trauma. In particular, a large part of the gender differences in mood/cognitive symptoms seems to be explained by sexual trauma. Although trauma patients present differently depending on gender and trauma type, we find that when attempting to isolate the effects of sexual trauma, PTSD prevalence and most symptom severities are not statistically different between the sexes.
Although our study suggests that men and women have similar reactions to sexual trauma, we are left to speculate about the few symptoms that stand out. Self-harm—which arguably includes suicidality, recklessness, and even tobacco use—has previously been linked to both self-treating numbness and punishing one’s self (Briere & Gil, 1998). Perhaps these behaviors are different approaches for self-treating emotional numbness (e.g., women hurt themselves and men engage in high-risk activities to escape the numbing), for which the genders had similar magnitudes among those with sexual trauma. Perhaps sexual trauma increases self-blame in both genders, but men and women express different versions of self-damaging impulsivity. Differences in avoidance may be explained by more cultural attention to sexual trauma in women making it more difficult for women to avoid trauma reminders (e.g., in news, films, social media). Although our data do not specify belief types, it is possible that increased cultural attention—a “double-edged sword”—also leads to more over-accommodated beliefs in women (e.g., “the world is completely dangerous,” “no man can be trusted”), which could contribute to worse avoidance among women. Another possibility is that avoidance manifests as recklessness in men, consistent with theories that thrill-seeking behaviors provide a reward of achieving safety (Pynoos & Briggs, 2009). Men may also seek avoidance through the numbing, sedating, and euphoric effects of substances such as alcohol (Guina, Rossetter, DeRhodes, Nahhas, & Welton, 2015). Avoidance may also manifest in men as nightmares (one of our few outcomes significantly worse in men with sexual trauma than men with non-sexual trauma), consistent with the Threat Simulation Theory, in which dreams are theorized to simulate threats to improve avoidance when awake and with men being more likely to identify negative events as triggers for nightmares (Robert & Zadra, 2014). Nightmares have been associated with traumatized men (King et al., 2013) but never specifically sexual trauma in men. Although beyond the scope of this article, our findings lead us to theorize that sexual trauma can cause similar underlying psychopathology in most survivors, but the genders often manifest pathology differently. Further research is needed to confirm and understand these differences and their causes.
Limitations, Strengths, and Suggestions for Future Research
Potential limitations of this study are generalizability (our sample is military, clinical, and predominantly White) and self-report reliability, which render these findings preliminary. Our overall PTSD rate (21.2%) is more than twice that of the general population (APA, 2013). This is likely due to our sample being a military and clinical population, both of which are more likely to have past trauma. Nevertheless, these populations are often the most accessible for large studies to obtain sufficient prevalence of PTSSs. In addition, this more severe sample is likely similar to the typical population that presents for mental health care. Another issue with our population is gender differences in military status (e.g., 59.5% of men were active duty, whereas a plurality of women at 47.6% were dependent family members) and military experience (e.g., men are more likely to serve in combat, women may have unique experiences in a hyper-masculine military culture), though we attempted to decrease selection bias by adjusting for trauma type. Larger studies in the future may be able to decrease military status as a confounder with gender. Although we had a good survey return response, another limitation is that we cannot determine the implications of approximately 22% of the sample not returning completed surveys. Time constraints are a likely reason, but lack of interest in the topic of trauma or avoidance of trauma-related material may have affected the study results. In addition, our relatively small sample size of men with sexual trauma (n = 31) may limit our results. With respect to validity, we sought to deter minimizations for fears of negative repercussions on military careers with anonymous surveys, and to mitigate exaggeration with a method for diagnosing PTSD that assures consistency with DSM-5 criteria (APA, 2013) rather than using cutoff scores. Because others have expressed concerns about how researchers and participants determine what constitutes a trauma (Tolin & Foa, 2006), we provided the DSM-5 definition of trauma in the survey. Nevertheless, participants may have over- or under-reported traumatic events (particularly for sexual assault; Koss et al., 2007), and, though we accounted for trauma type, we did not assess severity, quantity, duration, or sequelae (e.g., traumatic brain injuries) of traumas. Finally, when adjusting for trauma type, stepwise selection of a subset of trauma types was used. This method performs an automatic and fast directed search among the possible combinations of trauma types. This method-facilitated model selection, however, has the potential of not finding the model with the lowest AIC. Despite these limitations, there is a relative paucity of PTSS gender studies—none of which have specifically compared gender differences in sexual trauma—and our work may contribute to a better characterization of PTSD.
Strengths of this study include use of current diagnostic criteria, large total sample size, adjusting for trauma type, and separate comparisons within trauma patients and PTSD patients. Based on our literature search, this study was larger than all but one previous PTSS gender difference study of 2,341 participants with only combat trauma (King et al., 2013). Although previous researchers have hypothesized that gender differences are explained by trauma type, we were the first to adjust for trauma type and demonstrate its impact. Future studies may consider other potentially useful ways for adjusting (e.g., latent class variable). Finally, different findings between those with trauma and those with PTSD demonstrate the importance of how researchers define subject groups because those with trauma and those with PTSD only partially overlap. For example, if gender and trauma were not both accounted for, it would be easy to mistake the factors contributing to PTSD prevalence (higher in women than men, but greatly explained by sexual trauma), suicide attempts (higher in women with sexual trauma than women with non-sexual trauma, but lower in men with sexual trauma than men with non-sexual trauma), and recklessness (highest in men with sexual trauma, but women with sexual trauma and men with non-sexual trauma had similar levels to each other). All previous studies of PTSS gender differences have examined one of these two overlapping groups, and this is the first to examine both. We recommend our method of examining both subsets simultaneously for future studies, to avoid generalizing about the unstudied subset, and in the hopes of advancing knowledge of the progression from trauma to PTSD and what makes those labeled with “PTSD” unique.
Although our findings are preliminary, we believe our study warrants further research for confirmation and generalizability to other populations. We recommend using more validated measures (e.g., for trauma types and substance-related problems). We also recommend future studies analyze both trauma and PTSD groups, and both gender and specific trauma types (and hopefully determine other important factors). Although beyond the scope of this article, future studies may assess possible neurobiological markers, and attempt to discover clinical utility for understanding gender differences in trauma patients (e.g., targeted and diversity-sensitive screening questions, treatment targets). Understanding gender differences is important, but it is also important to not overgeneralize, to recognize that each individual has unique experiences, and that there are often more differences within groups of people than between them.
Conclusion
Although biological and psychological gender differences (e.g., endocrinology, internalizing vs. externalizing defenses) may affect some PTSD symptomatology, differences in trauma type prevalence likely explain many PTSS gender differences. With few exceptions, gender differences generally decrease or disappear when accounting for trauma type or when only considering those meeting PTSD criteria. Major exceptions include suicide attempts and avoidance (consistently worse among women), alcohol-related problems (consistently more common among men), mood/cognitive symptoms such as amnesia (associated with sexual trauma), and recklessness and tobacco (associated with sexual trauma in men). Sexual trauma may cause worse outcomes than other trauma types, regardless of gender, but gender likely influences symptomatology. Although sexual trauma is rarer among men, it appears that men and women generally respond to these terrible events in similar ways.
Footnotes
Acknowledgements
The authors gratefully appreciate Wright-Patterson Air Force Base and Wright State University Boonshoft School of Medicine Department of Psychiatry for institutional support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.