
Abstract
Youth is a period in life when the risk of violence victimization is high and association between victimization and ill health is well established. Youth rarely reveal violence victimization to health professionals if not directly asked but favor health professionals asking about victimization. The study’s primary aim was to examine health outcomes in young women being routinely asked about violence victimization and offered subsequent support, compared with controls, at 12-month follow-up. Secondary aims were to examine to what extent routine inquiry altered the consultation and re-victimization rates during the study period. A randomized controlled intervention study was conducted at Swedish youth health centers. Participants assigned to the intervention group were asked structured questions about violence. Victimized participants received empowering strategies and were offered further counseling. Participants in the control group completed questionnaires about victimization after the visit. Both groups answered questions about sociodemographics and health, constructed from validated instruments. A questionnaire was administered to all participants 12 months after baseline. Of 1,445 eligible young women, 1,051 (73%) participated, with 54% of the participants completing the 12-month follow-up. Lifetime violence victimization was reported by 53% in the intervention group and 60% in the control group, ns. There were no significant differences in health outcomes, between baseline and 12-month follow-up, within either group or between groups. Re-victimization rates were 16% in the intervention group and 12% in the control group, ns. Of victimized young women in the intervention group, 14% wanted and received further counseling. Routine inquiry about violence victimization and empowering strategies were feasible within ordinary consultations at youth health centers but did not demonstrate improved health outcomes at 12-month follow-up compared with controls. Questions about violence led to a high degree of disclosure, and 14% of victimized young women in the intervention group received further counseling as a result.
Background
Youth is a time when the risk of violence victimization is high (Finkelhor, Turner, Shattuck, & Hamby, 2015; Palm, Danielsson, Skalkidou, Olofsson, & Hogberg, 2016). Victimized youth are at risk of a number of adverse health outcomes such as depression and post-traumatic stress disorders, as well as somatic complaints, and report more days of absence from school due to ill health (Finkelhor et al., 2015; Gini & Pozzoli, 2013; Gore et al., 2011; Kilpatrick et al., 2003; Palm et al., 2016). The processes by which violence victimization leads to ill health are less well understood. It is suggested that victimization may damage a person’s self-concept, leading to low self-esteem and a feeling of helplessness, which might be a mediator for depressive symptoms (Turner, Finkelhor, & Ormrod, 2010). Alterations in the neuroendocrine stress response have also been implicated in the development of mental and physical ill health (Anda et al., 2006; Heim, Newport, Mletzko, Miller, & Nemeroff, 2008).
Preventing victimization and ill health in youth might reduce the burden of morbidity in adulthood (Catalano et al., 2012). In response to the broad direct and indirect health impacts violence may have on young people’s lives, routine inquiry about, and intervention for, violence victimization in youth in health care settings have been advocated by organizations such as the American Academy of Pediatrics, Committee on Child Abuse and Neglect (1998) and the American Medical Association (2008), as well as the Swedish authority, the National Center for Knowledge on Men’s Violence Against Women (2011). However, despite recommended guidelines, there is no consensus on how routine inquiry and intervention in victimized youth should be performed.
Young people rarely reveal violence victimization to health professionals if not directly asked (Ashley & Foshee, 2005; Black, Tolman, Callahan, Saunders, & Weisz, 2008; Crisma, Bascelli, Paci, & Romito, 2004; Priebe & Svedin, 2008; Rickert et al., 2009). However, several studies have demonstrated that youth are in favor of health professionals routinely asking about violence victimization (Finkelhor, Vanderminden, Turner, Hamby, & Shattuck, 2014; Priebe & Svedin, 2008; Rickert et al., 2009; Zeitler et al., 2006). This finding contrasts with health care providers often being hesitant to inquire about violence victimization because of the barriers of a reported lack of training, a fear of offending the patient or even of making matters worse, and time constraints (Lo Fo Wong, Wester, Mol, & Lagro-Janssen, 2006; Ramsay, Richardson, Carter, Davidson, & Feder, 2002).
Studies suggest that routine inquiry by health care providers can be effective in increasing disclosure of intimate partner violence in adult women (Feder, Hutson, Ramsay, & Taket, 2006; Lo Fo Wong et al., 2006; Ramsay et al., 2002; Taft et al., 2013). Some studies on interventions in health care settings for adult women who have experienced intimate partner violence have demonstrated a moderate effect of the interventions on health outcomes (Garcia-Moreno et al., 2015; Hegarty et al., 2013; Resick et al., 2008; Tiwari et al., 2005). One study of pregnant abused women who were offered empowering strategies showed reduced rates of intimate partner violence and improved health outcomes at follow-up (Tiwari et al., 2005). Studies on routine inquiry and interventions for violence in health care settings in youth are few. Prior studies have mainly been conducted with victimized youth attending emergency departments because of injuries, demonstrating some effects in the form of decreased re-victimization (Cunningham et al., 2012; Zun, Downey, & Rosen, 2006). Qualitative studies of sexually abused youth in psychiatric settings have indicated that most youth who received counseling considered it helpful (Schonbucher, Maier, Mohler-Kuo, Schnyder, & Landolt, 2014). It is also increasingly known that various types of violence often co-occur and that prior victimization is the best predictor of subsequent victimization (Blom, Hogberg, Olofsson, & Danielsson, 2014; Finkelhor, Ormrod, & Turner, 2007). A recent study showed that all victims of teen dating violence also reported at least one other type of victimization, and that teen dating violence was closely associated with sexual victimization, child maltreatment, and poly-victimization (Hamby, Finkelhor, & Turner, 2012). These findings emphasize the importance of a comprehensive approach when addressing violence victimization in youth. Routine inquiry that identifies different types of victimizations and interventions that can simultaneously address multiple types of violence might prove more effective than just targeting one type of violence, such as dating violence, at a time (Foshee et al., 2014; Hamby et al., 2012). To our knowledge, no studies on routine inquiry about violence victimization and subsequent interventions in a general population of youth attending non-emergency health care settings have been conducted. The primary aim of this study was to examine health outcomes in young women receiving routine inquiry about violence victimization and offered subsequent support at youth health centers, compared with controls, at 12-month follow-up. Secondary aims were to study re-victimization during the study period, and to examine whether and to what extent routine inquiry altered the consultation.
Method
Setting
In Sweden, almost all municipalities have youth health centers. These centers are staffed by midwives, social workers, and physicians. Young people attend until the age of 23 years for counseling on sexual and reproductive health, as well as social, psychological, and physical problems. Young women account for about 90% of the visits, with the prescription of contraceptives being the predominant reason for their first visit. Youth can test for pregnancy at the youth health centers, but all pregnant women are referred to the nearest obstetrics and gynecology department. About 15% of visits consist of psychological or social problems, and those youth will be appointed a social worker.
This study was conducted at four youth health centers in two mid-size towns and two small towns in the county of Västerrnorrland, Sweden. The county has a total population of 240,000 inhabitants. The level of at least 3 years of postsecondary education is 19%, and 8% have a foreign background, compared with 23% and 15%, respectively, in the whole of Sweden (Statistics Sweden, 2012, 2014).
Study Design
The design was a randomized parallel controlled intervention study. All 15- to 22-year-olds coming for their first visit to one of the four youth health centers during the period January 1, 2012, to December 31, 2012, were consecutively asked to participate in the study. In one of the youth health centers, participants were included until June 10, 2013, owing to a lack of staff at the beginning of the study period.
In Sweden, the general position of the Central Ethical Review Board is that consent from parents/guardians is not needed for a youth above the age of 15 years to participate in a study, provided that the youth is considered to be able to fully comprehend the information in the study. Hence, exclusion criteria were severe mental disease, intellectual mental impairment, and inability to understand written Swedish.
Possible participants were informed about the study orally and in writing by a midwife or social worker in a private room. Oral informed consent was obtained. The participants received no incentives for inclusion in the study. The youth who agreed to participate were randomized into the intervention group or the control group. A random allocation sequence was generated by a statistician not otherwise involved in the study. The randomization, which was stratified by sex and youth health center, occurred in blocks of eight, with sealed envelopes being used.
One thousand fifty-one young women (73% of eligible women) and 86 young men (65% of eligible men) consented to randomization and were enrolled in the study. Due to the small number of young men participating in this study, only the young women’s results are reported on.
Intervention
The participants assigned to the intervention group were asked structured questions about violence victimization by the midwife/social worker during their regular visit. For the participants in the intervention group who had been violence victimized, the midwife/social worker employed empowerment strategies (Chang et al., 2005; Feder et al., 2006; Tiwari et al., 2005). Empowerment strategies include listening to the participant’s story, taking in and accepting the participant’s perceptions and feelings in a non-judgmental way, and emphasizing that violence is never the victim’s fault (Tiwari et al., 2005). We found it paramount to use an intervention that was feasible to include within the ordinary consultation, and the time frame of empowerment strategies was considered an advantage. Furthermore, earlier studies have used empowerment strategies as an intervention for adult women victims of intimate partner violence (Parker, McFarlane, Soeken, Silva, & Reel, 1999; Tiwari et al., 2005). The intervention protocol was based on similar studies but was adapted to the current setting.
The midwife/social worker also addressed safety issues and contacted social authorities when considered necessary. All participants with experience of victimization were offered further counseling. Prior to the start of the study, all personnel had participated in several education sessions on violence against youth and women. Action plans for personnel on how to handle victimized youth were well established at all four youth health centers. Two of the researchers (AP and ID) visited all included youth health centers every second month to ensure that the interventions were consistently carried out during the study period.
For every young woman answering routine questions about violence victimization, the midwife/social worker documented whether the questions led to any form of further intervention or whether they altered the consultation in any way. An assessment of to what degree the questions about violence changed the total management of the patient was performed using a four-grad scale: not at all, a little, quite a lot, and a lot. This documentation did not contain data on the identity of either the participant or the midwife/social worker.
The participants in the control group had a regular visit with a midwife/social worker who attended to the specific reason for the visit. Violence victimization was not generally addressed, but these participants answered the same questions about violence victimization in a questionnaire after the visit. Both groups answered questions about health and sociodemographics in a sealed questionnaire after their visits.
A questionnaire with the same questions, including questions on violence victimization, was then administered to the participants in both groups by mail, email, or cell-phone text message, at 3 months and then at 12 months after the baseline. Non-responders received two reminders and were considered non-responders if they failed to answer after the second reminder.
All staff at the participating youth health centers was carefully informed about the ethical implications of the study, and all participants were informed about the possibility of prompt counseling if needed. The study was approved by the Regional Ethical Review Board in Umeå (Dnr 2011-110-31Ö).
Measures
Violence victimization
Five structured questions on lifetime violence victimization were used in the health dialogue interview for the intervention group and in the questionnaire for the control group. Four questions were modeled on but shortened from the NorVold Abuse Questionnaire (Swahnberg & Wijma, 2003), and were worded as follows: (a) “Have you ever experienced being repressed, humiliated, or threatened?” (b) “Have you ever experienced physical abuse (e.g., been slapped in the face, hit with fists or kicked, or had a weapon used against you)?” (c) “Have you ever experienced being touched against your will on your body or genitals, or been forced to touch someone else’s body or genitals, or has anybody used your body to satisfy himself or herself?” and (d) “Have you ever experienced someone, against your will, putting or trying to put his penis, or something else, into your (vagina), mouth, or rectum?” A final question was added about witnessing family violence: (e) “Have you ever seen or heard an adult in your family hurting someone in your family?” After each question, the participant, if victimized, was asked to mark on a Visual Analogue Scale (VAS) to what extent they were still adversely affected by the violence. The VAS ranged from 0 to 10, where 0 was not at all and 10 was very much. This method has been validated in a prior study on physically and sexually abused gynecological patients and has also been used in a prior study addressing violence victimization in youth (Wijma et al., 2003; Danielsson, Blom, Nilses, Heimer, & Hogberg, 2009).
In the 3-month and 12-month follow-ups, a question about the perpetrator was added for each of the five questions on violence, worded as “By whom, mark all answers that apply to you” with the following alternatives: (a) “parent, sibling, or other relative”; (b) “stepparent or mother’s or father’s partner”; (c) “partner or ex-partner”; (d) “friend, school mate, or acquaintance”; and (e) “unknown.” For the question about witnessing family violence, three alternatives were used: (a) “parent,” (b) “stepparent or mother’s or father’s partner,” and (c) “another adult in the family.”
Health
Questions about self-perceived health were worded from the Swedish National Survey of Public Health (Boström & Nyqvist, 2010). They included perception of general health, days of feeling mentally or physically unwell, and number of days of absence from school or work due to ill health in the previous month. General health was dichotomized into very good/excellent or less than very good/excellent. Four questions about pain in the neck/shoulders, the limbs, and the bowel, and headache/migraine were measured as no symptoms, mild symptoms, and severe symptoms. No symptoms equaled a score of 0, mild symptoms a score of 1, and severe symptoms a score of 2 for each question. In the analysis, the answers to the four questions were merged using a score from 0 to 8
Sociodemography
Questions on demographics and sexual orientation were worded from the Swedish National Survey of Public Health (Boström & Nyqvist, 2010). Education was dichotomized into attending a vocational or an academic program in upper secondary school. The participants’ inability to access 1,600 euros (approximately US$1,825) within a week was used as an indicator of lower economic resources. Foreign background was defined as being foreign born and/or having two foreign-born parents, and Swedish background as being Swedish born, with one or two Swedish-born parents. Finally, sexual orientation was dichotomized into homo/bi/unsure about sexual orientation or heterosexual.
The internal dropout rates for the different question items in the baseline, 3-month, and 12-month questionnaires varied between 0.3% and 1.9%. No imputation for missing data was made.
Statistical Analysis
Descriptive statistics were computed for the total sample of the assigned conditions and outcomes. Categorical outcomes were analyzed using a chi-square test and McNemar’s test for binary data, and continuous outcomes using an independent t test. To detect differences within each group (intervention and control) throughout the study period, paired t tests were performed. In addition, to determine possible differences in outcomes between the intervention group and the control group, generalized estimating equations (GEEs) were performed. In the GEE analyses, a significant group-by-time interaction effect would indicate that the intervention condition significantly differed from the control condition over time (12 months) in the outcomes examined (Zeger & Liang, 1986). The level of significance was set at p < .05. The data were analyzed using SPSS 20.0 for Windows (IBM, New York, USA) for all analyses.
Results
Figure 1 depicts the research process for the participants, shown as a flow diagram. The follow-up rate among the young women at 12 months was 54%. A 3-month follow-up (65% response rate) was done mainly to ensure there were no short-term negative effects after routine inquiry about violence, or other short-term effects that would have disappeared by the time of the 12-month follow-up. There were no significant differences in outcomes between the 3-month and the 12-month follow-up; hence, only the 12-month follow-up results are presented.

Flow diagram of the young women participating in the study.
The distribution of study participants by sociodemographic and sexual orientation parameters, and by intervention/control group status, is presented in Table 1. Of the young women in the intervention group, 53% reported any lifetime violence victimization at baseline versus 60% in the control group, ns (Table 1). Re-victimization of young women victimized at baseline during the study period was reported by 16% of the intervention group and 12% of the control group at the 12-month follow-up, ns (data not shown).
Distribution of Completers a at Baseline by Sociodemographic, Sexual Orientation, and Violence Victimization Parameters, and by Control/Intervention Group Status.
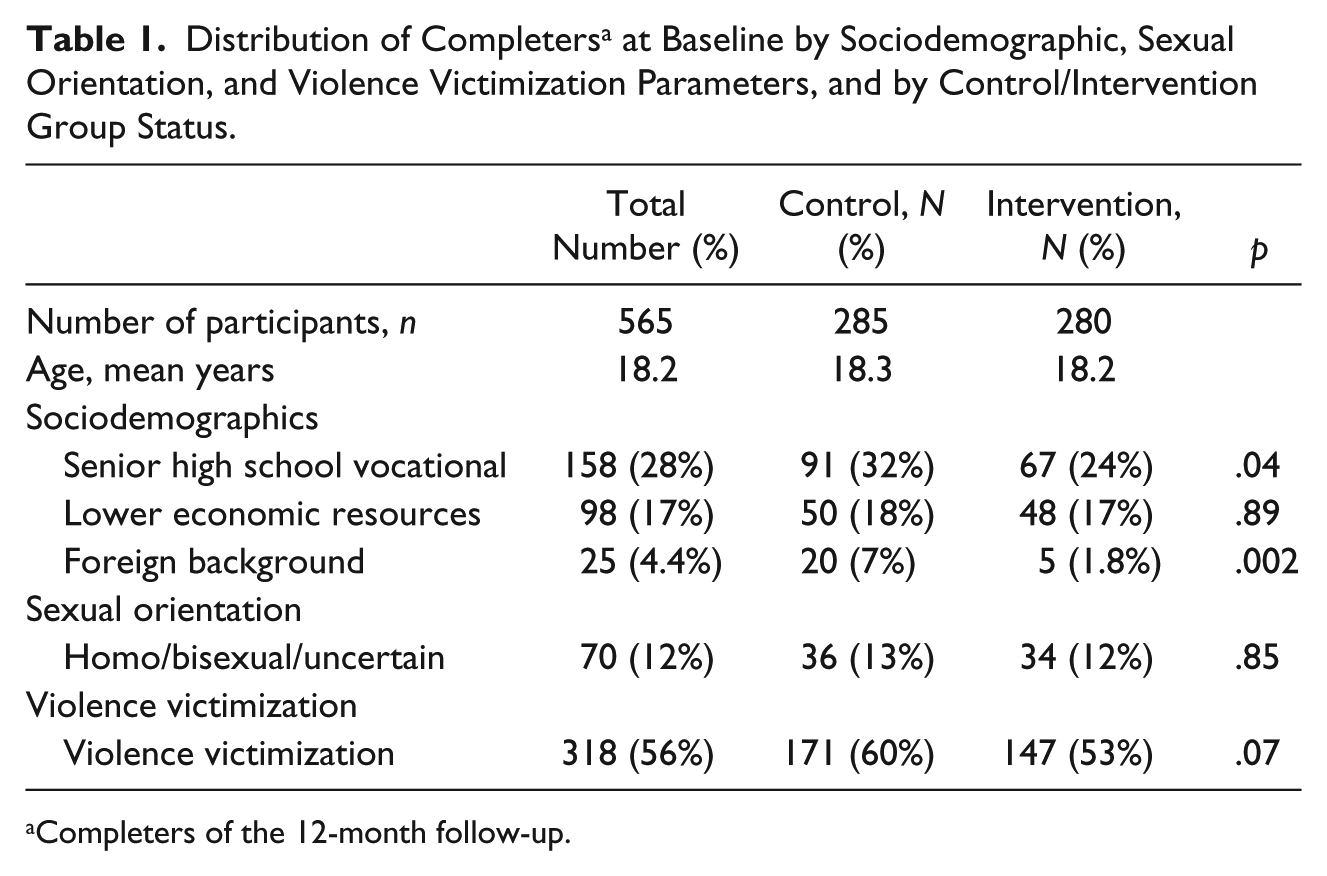
Completers of the 12-month follow-up.
Table 2 demonstrates the distribution by type of victimization and perpetrator in the young women who were victimized at baseline, and by intervention and control group status. No significant differences were seen between the groups (Table 2).
Distribution of Completers a Who Were Victimized at Baseline by Type of Violence and Perpetrator Parameters, According to Intervention/Control Group Status.
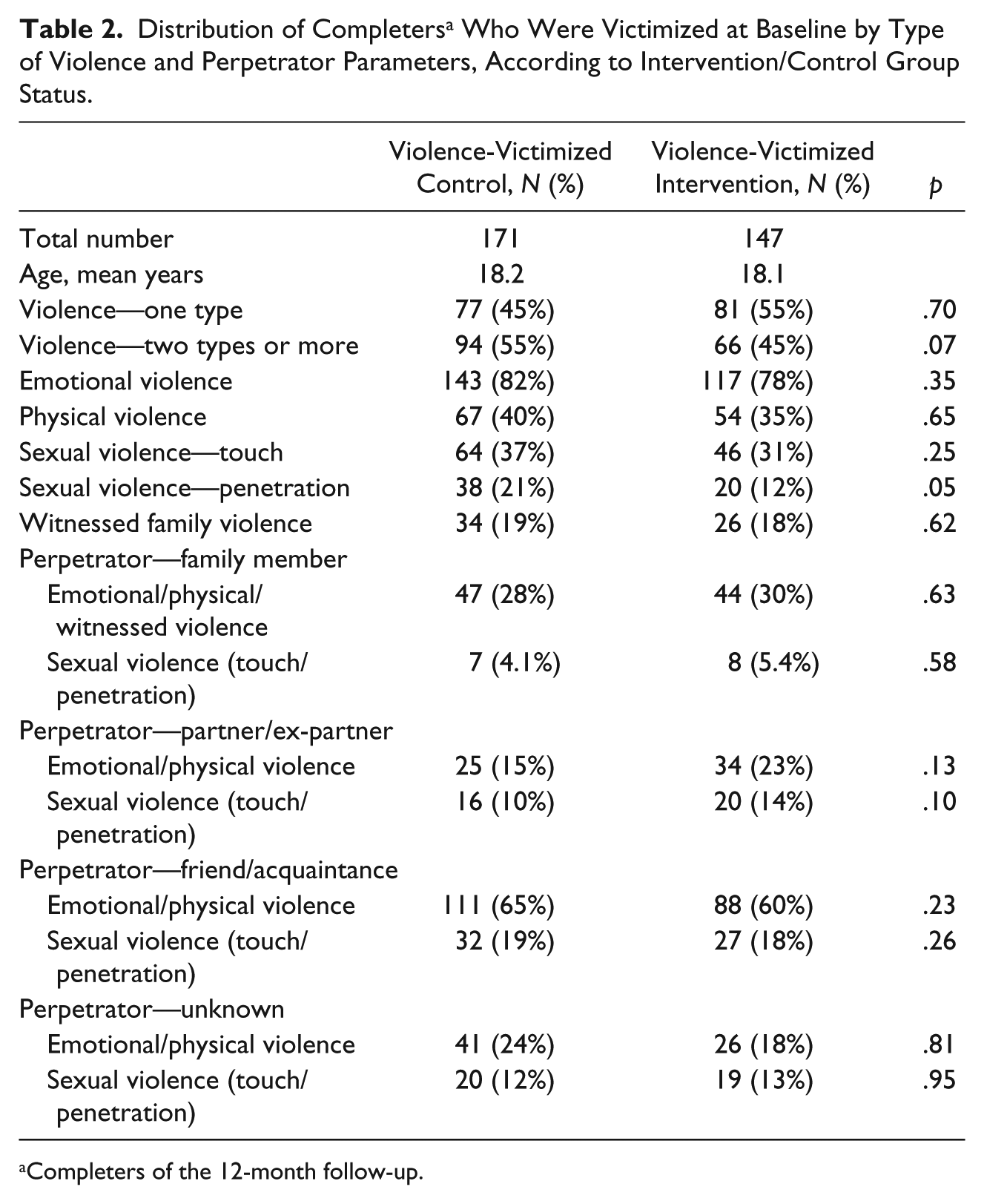
Completers of the 12-month follow-up.
There were no significant differences in health outcomes between the baseline and the 12-month follow-up within either the control group or the intervention group (Table 3).
Health Outcomes and VAS Values for the Influence of Prior Violence Victimization at Baseline and at 12-Month Follow-Up, for Young Women Who Reported Victimization at Baseline in the Intervention Group (N = 147) and in the Control Group (N = 171).
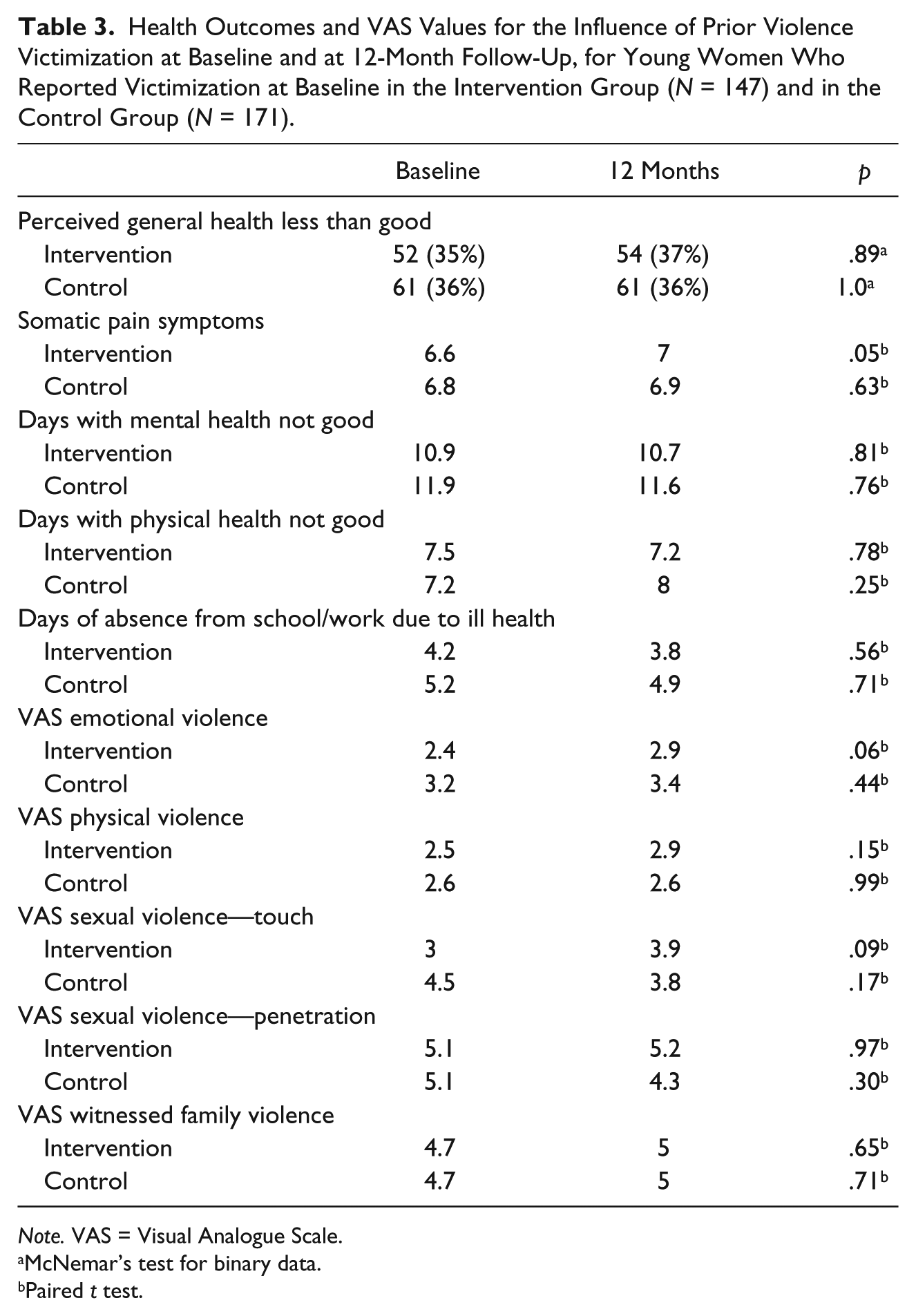
Note. VAS = Visual Analogue Scale.
McNemar’s test for binary data.
Paired t test.
A GEE analysis of the health outcomes mentioned above demonstrated no significant differences between the intervention group and the control group. The results did not change when adjusted for age, educational level, foreign/Swedish background, sexual identity, or perceived health at the baseline (Table 4).
Results From GEE Models Examining Health Outcomes at 12-Month Follow-Up for Violence-Victimized Young Women by Routine Inquiry About Violence Victimization.

Note. GEE = generalized estimating equation; CI = confidence interval; VAS = Visual Analogue Scale.
There were neither significant differences in outcomes between the intervention and control groups for the different youth health centers nor any differences in outcomes when young women were stratified by whether they had visited a midwife or a social worker (not shown).
Table 5 shows the consequences, in terms of extra visits, contact with authorities/guardians, and alteration of the consultation at the youth health center, after routine inquiry about violence victimization. In this table, all participants, both completers and non-completers of the 12-month follow-up, randomized to the intervention group at their first visit—537 participants of the total 1,051 participants enrolled in the study—are accounted for. Including routine questions about violence victimization altered the consultation quite a lot/a lot in 9% of the cases (Table 5). Of those in the intervention group who had suffered violence victimization, 14% wanted and received further counseling. The social authorities were contacted about two of these young women (Table 5).
Consequences of Routine Inquiry About Violence Victimization in Terms of Extra Visits, Contact With Authorities/Guardians, and Altered Consultation for All Young Women in the Intervention Group (N = 537; Both Completers and Non-Completers) and for the Subgroup of Violence-Victimized Young Women (N = 282), at Baseline.

Attrition Analysis
An attrition analysis was made of non-completers at the 12-month follow-up. Significantly more sexual minority young women and more young women attending academic programs in upper secondary school were among the completers than among the non-completers. At baseline, sexual minority young women were significantly more victimized than heterosexual women, whereas there were no significant differences in violence victimization between young women who attended academic programs and young women in vocational programs. Apart from these differences, non-completers did not differ from responders in sociodemographics, health outcomes, or violence victimization.
Discussion
Due to violence victimization among youth being common and its association with ill health well established, routine inquiry and intervention for violence victimization in youth in health care settings have been advocated by several health organizations. However, to this date, very few studies including routine inquiry for victimization as well as subsequent intervention for youth in health care settings have been conducted. To our knowledge, this is the first study examining routine inquiry, and subsequently offered intervention, for violence victimization in youth in a non-psychiatric or emergency setting. The current study showed that routine inquiry and brief intervention in the form of empowering strategies were feasible within an ordinary consultation. However, they did not improve health outcomes or reduce re-victimization in victimized young women compared with controls at the 12-month follow-up. Of the young women who reported any lifetime victimization in the intervention group, 14% wanted and received further counseling.
Assessing the effect of interventions is often difficult, and outcome measures may sometimes be too blunt to detect feelings and experiences that may still be beneficial for a participant. In a recent study, screening for violence victimization and subsequent intervention for adult women who were victims of intimate partner violence showed some reduction in depressive symptoms, but no improvement in their quality of life. However, 40% of the women in the study reported that the survey had made them more open to dealing with possible relationship problems (Hegarty et al., 2013). Several qualitative studies on adult women have also indicated that concern expressed by and support from health care providers have changed how victimized women viewed themselves and might even represent a turning point, leading to later change and healing (Chang et al., 2005; Chang et al., 2010; Zink, Elder, Jacobson, & Klostermann, 2004). The same studies reported that the actual change—for example, ending an abusive relationship—might have occurred years after the disclosure to health personnel, even when the women considered the disclosure to have been a turning point. Hence, it may be that the follow-up time of 12 months in this study was in fact too short.
Studies have shown that youth often do not know where to turn when victimized and also may doubt whether their experience actually was violence victimization (Crisma et al., 2004; Martin, Houston, Mmari, & Decker, 2012). Routine inquiry about violence victimization gives youth a chance to disclose victimization, and even if they may not want or need counseling at the time, they will know where to turn, should they need support later on (Black et al., 2008; Crisma et al., 2004; National Board of Health and Welfare, 2001). Routine inquiry is also an opportunity for health personnel to acknowledge the youth’s experience and affirm that violence is never acceptable (Crisma et al., 2004).
When asked, only 14% of the victimized young women in this study wanted further counseling. This finding is in line with an earlier Swedish study examining routine inquiry in pregnant women visiting antenatal clinics, where 13% of victimized women wanted further counseling (National Board of Health and Welfare, 2001).
Contrary to the present study, earlier studies with adult women suffering from intimate partner violence have demonstrated improved health outcomes after empowerment strategies. In this study, we addressed lifetime victimization, and it may be that empowerment strategies are not suited to address the effects of past victimization or other types of victimization apart from intimate partner violence. It could also be that empowerment strategies are not adaptable in young women, or need to be further developed to target the needs of victimized young women. A qualitative study with victimized participants from the current study is planned and may add more understanding to what interventions are considered helpful.
Even though no direct improvement in health outcomes after routine inquiry about violence victimization was seen in this study, identifying victimization in youth who present with medical problems in health care settings is important. This is, in part, not only for the reasons discussed above but also to direct adequate treatment. If violence victimization has contributed to mental and physical ill health, interventions in these problems will probably not succeed without addressing the victimization.
One of the arguments against routine inquiry about violence victimization is the fear it may upset the patient or even contribute to ill health (Ramsay et al., 2002; Taft et al., 2013). Hence, an important finding in this study was that no adverse effects in health outcomes in those asked about violence victimization were seen compared with controls at both the 3-month and the 12-month follow-up. Another consideration often expressed concerning routine inquiry about victimization is the lack of time, both for asking the questions and for handling the answers (Lo Fo Wong et al., 2006; Ramsay et al., 2002). However, routine inquiry about violence victimization in this study only altered the consultation “quite a lot” or “a lot” in 9% of consultations, contradicting the fear of routine inquiry being very time consuming.
In adult women, studies have demonstrated that routine inquiry about victimization can be effective in increasing the disclosure of intimate partner violence (Feder et al., 2006; Lo Fo Wong et al., 2006; Ramsay et al., 2002). In this study, there were no significant differences between the intervention group and the control group in the rate of disclosure of various types of victimization. The indication in this setting is that when asked, young women to a large extent revealed victimization. The extent of the disclosure in this study was somewhat higher than in earlier studies (Rickert et al., 2009; Zeitler et al., 2006).
Methodological Considerations
To date, the field of violence prevention and intervention research has primarily focused on one type of violence at a time (Hamby & Grych, 2013). In light of the increasing evidence of co-occurrence of violence being more the norm than the exception (Finkelhor et al., 2015; Hamby & Grych, 2013; Palm et al., 2016), the current study entailed a comprehensive approach, assessing lifetime emotional, physical, sexual, and family violence victimization in young women, which is one of the strengths of the study. Other strengths are the study having a fairly long follow-up time of 12 months and the questions on violence victimization and the intervention outcomes being based on validated questionnaires.
Prior research has mainly screened for violence in victims of youth violence attending emergency departments because of injuries (Cunningham et al., 2012; Zun et al., 2006). This study has extended the prior research, studying routine inquiry and subsequent support in a different group of youth, namely those visiting youth health centers mainly for other reasons such as prescription of contraceptives, health problems, or testing for sexually transmitted infections.
It is common for young women in Sweden to attend youth health centers; 25% of all 16- to 25-year-old women in Sweden reported having visited a youth health center in the previous 3 months (Danielsson et al., 2012). When comparing the young women in this study with young women of the same age answering the Swedish National Public Health Survey, the study participants reported similar rates of ill health (Lager, Berlin, Heimerson, & Danielsson, 2012). The prevalence of violence victimization in this study was also in line with earlier population-based studies (Andersson, Heimer, & Lucas, 2015). This is an indication that as a group, young women visiting youth health centers do not present with more ill health or a higher degree of victimization than do young women in the general population.
This study represents a large sample of young women attending youth health centers in Sweden. Of all eligible young women, 72% agreed to participate in the study. The young women who declined participation mostly stated a lack of time as the reason, but the results may be biased by not having further information about them. The relatively high level of attrition between the baseline and the 12-month follow-up may have caused selection bias. The attrition analysis demonstrated no differences at baseline between completers and non-completers other than a higher number of young women with a higher educational level and a higher number of sexual minority young woman among the completers. At baseline, sexual minority women reported more victimization than heterosexual women did, which might have influenced the results. Attrition rates did not significantly differ between the intervention and control groups.
Another reason for the relatively high attrition level is that for two periods during the 12-month follow-up, there were severe problems with the server handling the digital questionnaires. A number of questionnaires, approximately 50 to 70, were not received.
Another limitation was that the assessment of violence victimization was based on self-reporting, which may have introduced some risk of under-reporting because of shame, guilt, or unwillingness to disclose. Unmeasured confounders and external variables such as the timing of victimization may also have biased the results.
The present study took place in a part of Sweden with mid-size and small towns including rural areas. The people in the area have a lower level of postsecondary education and fewer people with foreign background than in the whole of Sweden. Hence, the results in this study may not be generalizable to young women from urban and more ethnically mixed backgrounds.
Conclusion
The current study showed that routine inquiry for violence victimization and brief intervention in the form of empowering strategies were feasible within ordinary consultations at youth health centers. During the period of this study, no differences were found in violence victimization rates or health outcomes between the intervention and the control group. Questions about violence led to a high degree of disclosure, and 14% of the young women in the intervention group wanted and received further counseling as a result.
Even though no effect on health outcomes could be measured in this study, routine inquiry about violence victimization, as well as disclosure and subsequent support, may still play an important role, specifically to address possible health problems in victimized youth. More research is needed to better understand how young people experience being asked about violence victimization and what interventions they consider may be helpful.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the Swedish Crime Victim Compensation and Support Authority and the Research and Development Department, Västernorrland County Council, Sweden.