
Abstract
Rape is considered a stressful trauma and often has long-lasting health consequences. Compared with adult females, limited data exist on the psychological impact of rape in adolescents. The aim of this study was to assess the prevalence and associated factors of emotional distress in a cohort of adolescent rape survivors in Cape Town. Participants in this prospective longitudinal study were 31 adolescent female rape survivors recruited from a rape clinic in Cape Town and assessed within 2 weeks of the assault. Assessment measures included a sociodemographic questionnaire and initial screening with the Child and Adolescent Trauma Survey (CATS), the patient-rated Children’s Depression Inventory (CDI), and the Multidimensional Anxiety Scale for Children (MASC). The CATS, CDI, and MASC were repeated at 1, 3, 6, 9, and 12 months post enrollment. Psychiatric diagnoses were made with the clinician-administered Mini International Neuropsychiatric Interview–Child and Adolescent version (MINI-Kid). At baseline, on the MINI-Kid, a definitive diagnosis of major depressive episode was endorsed in 22.6% of the participants. Stress-related disorders were found in 12.9%, whereas 16.1% had anxiety disorders. There was no diminution of symptoms on self-reported psychopathology measures at follow-up assessment over the five follow-up time points, suggesting persistent psychopathology over a 1-year period despite repeated clinical assessments and supportive counseling. Symptoms of anxiety, depression, and posttraumatic stress disorder in this sample of adolescent female rape survivors were high at enrollment and found to be persistent, underlining the need for long-term support, screening, and evidence-based follow-up care.
Background
Sexual violence against women and children is rampant globally, such that one in three women will be sexually assaulted in their lifetime, with about 30% to 40% of reported incidents involving minors (García-Moreno, 2013; World Health Organization, 2004). Although the number of reported rape cases in South Africa has been fairly stable with a modest decrease of 3% in the last decade (South African Police Service, 2016), the prevalence of sexual offences in this country remains among the highest in the world (Dartnall & Jewkes, 2013; Kaminer, du Plessis, Hardy, & Benjamin, 2013). The Western Cape Province has one of the highest prevalence of rape in the country (South African Police Service, 2016). Up to 40% of rape and attempted rape cases reported in South Africa in the late 1990s involved minors (Jewkes & Abrahams, 2002). In a study that examined exposure to violence among adolescents across multiple sites in South Africa, 8% of more than 600 adolescent participants reported that they had been sexually abused (Kaminer et al., 2013).
Adolescent rape survivors may experience a wide range of immediate and long-term emotional and mental health consequences following assault. These include depression, posttraumatic stress disorder (PTSD), anxiety, and feelings of guilt and shame (Ackard, Neumark-Sztainer, Hannan, French, & Story, 2001; Kendall-Tackett, Williams, & Finkelhor, 1993). PTSD is diagnosed as acute when symptoms are present in the first 3 months after the index trauma and as chronic when symptoms persist beyond 3 months. The presence of PTSD symptoms in 1 month after the index trauma is referred to as an acute stress disorder. Rape survivors are more likely to experience avoidance symptoms (e.g., not wanting to think or talk or have feelings about the trauma) and less likely to complete stress-targeting therapies (Murphy et al., 2014). Rape can also result in other psychological sequelae including sexual dysphoria, eating disorders, sleeping disturbances, substance abuse, suicide, or suicidal ideation (Johnson, 2004; Raj, Silverman, & Amaro, 2000; Silverman, Raj, Mucci, & Hathaway, 2001). The risk of experiencing negative mental health sequelae post rape may be more pronounced in adolescents given their developmental stage, their relatively limited coping skills compared with adults, and the fewer available resources to assist with recovery.
South Africa’s Western Cape Department of Health (2001) has instituted policy within its Comprehensive Primary Health Care Services that aims to provide health managers and health workers with a clear framework on the management of female and male survivors of rape and sexual assault (14 years and older). The policy is further supported by the “National Standardized guidelines for the management of rape survivors in South Africa” (South African National Management Guidelines for Sexual Assault, 2003). Current guidelines emphasize legal and biological interventions and counseling options of care immediately post rape. There is, however, no structured long-term support beyond 3 months or long-term interventions contained in the management guidelines for rape survivors in this region.
Although much research has addressed the health impact of rape among female survivors in general, there are limited data on its impact specifically in adolescent female rape survivors in South Africa and other developing countries. An understanding of the long-term psychiatric outcomes and the predictors of outcome in this vulnerable population is vital to discerning the most appropriate intervention. In this study, we examined the immediate and long-term mental health outcomes in a cohort of adolescent rape survivors in Cape Town.
Method
Study Design and Procedure
The study design was a longitudinal naturalistic cohort study and it evaluated the immediate and long-term mental health outcomes (anxiety, depression, and PTSD) and emotional distress in adolescent females exposed to rape. This study was nested within a larger study conducted between 2004 and 2014. The parent study aimed to compare the effectiveness of an early trauma-focused group cognitive-behavioral therapy (CBT) intervention with repeated clinical assessments in reducing PTSD and depressive symptoms over a 1-year follow-up period in adolescents recently exposed to rape. Adolescents included in the current study received repeated weekly clinical assessments (comprising a brief mental status examination, completion of self-report questionnaires, and supportive counseling).
Study Participants
Study participants were adolescent female rape survivors aged 14 to 18 years old, recruited from a dedicated rape crises clinic in Cape Town that provides a multi-disciplinary service for rape survivors. Participants were recruited within a 2-week period post rape. Participants were included in the study if they had a recent history of rape, were currently in school, conversant in English or Afrikaans, not living with the perpetrator, and willing to provide informed consent. They were excluded if they were suicidal, had a known past history of a major psychiatric disorder, were using psychotropic medications, or had received any formal psychotherapy in the preceding 3 months.
All survivors of rape presenting to the Thuthuzela Rape Crisis Clinic were managed by staff at the clinic in accordance with the policy and standardized management guidelines as set out by the Western Cape Department of Health. The routine treatment provided at these centers to date includes medical screening forensic/legal support and counseling-related interventions. As standard care, the rape survivors are given the option of being referred for counseling to a social worker, trained counselor (regional specific), private therapist (e.g., psychologist), rape crisis, or other local services. In addition, a follow-up at 6 weeks and at 3 months post rape is recommended, with the aim of screening for PTSD and other emotional disorders.
Screening and Enrollment
Eligible adolescents were referred by clinic nurses to the research assistant and provided with a brief description of the study. Consenting eligible adolescents returned for an initial screening interview. A total of 31 participants were enrolled and all were screened prior to commencing repeated clinical assessments (RCA). Assessment measures comprised a Demographic Questionnaire (devised by the investigators) to collect personal and family information; the MINI-Kid (Mini International Neuropsychiatric Interview–Child and Adolescent version); the Child and Adolescent Trauma Survey (CATS; March, 1999; patient-rated), the Children’s Depression Inventory (CDI; Kovacs, 1985; patient-rated), and the Multidimensional Anxiety Scale for Children (MASC; March, Parker, Sullivan, Stallings & Connors, 1997; patient-rated). All participants were required to complete the MINI-Kid as baseline at enrollment and the other listed measures (CATS, CDI, MASC) at enrollment and at 1, 3, 6, 9, and 12 months follow-up.
Assessment Measures
Sociodemographic Questionnaire
This captured information on age, ethnicity, language, and education and also included questions about family and current living circumstances.
MINI-Kid
This was used to make a definitive psychiatric diagnosis. The MINI-KID is a structured clinical diagnostic interview designed to identify current psychiatric disorders in children and adolescents aged 6 to 17 years in a comprehensive and concise manner. It is modelled from the adult version of the interview (MINI), which has been validated against the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders revised 3th edition (DSM-III-R, 1987; Sheehan et al., 1998) and against the World Health Organization–designed Composite International Diagnostic Interview (Lecrubier et al., 1997).
The CATS
The CATS was used to assess the severity of posttraumatic stress symptoms. The CATS is a self-report screening tool that includes both a PTSD inventory derived from the MASC (March et al., 1997) and the DSM-IV criteria for PTSD (APA, 1994). The trauma exposure list includes both direct (happened to me) and vicarious (happened to someone I know well) lifetime exposure. The 12 items address the core symptom categories of PTSD (re-experiencing, avoidance, and hyperarousal) and are rated on a 4-point Likert-type scale (scored as 0, 1, 2, and 3), summed to yield a CATS score. The CATS score correlates well with other measures of PTSD and a score of 27 or more suggests a probable diagnosis of PTSD. However, a score of 15 or more was used here as it has been found to be a more sensitive cutoff in South African adolescents (Suliman, Kaminer, Seedat, & Stein, 2005).
The CDI
Developed in 1979, the CDI is one of the most widely used self-report scales for depression in youth (Kovacs, 1992) . It is a brief self-report test for children and adolescents 7 to 17 years of age to screen for the presence and severity of depressive symptoms. The CDI evaluates cognitive, affective, and behavioral symptoms of depression as they relate to children, their functioning at school and with peers. Each item has three possible responses with 0 indicating the absence of symptoms, 1 mild symptom, and 2 definite symptoms. The total score ranges from 0 to 54 and the tool has an excellent reliability of .87, as measured by Cronbach’s alpha (Sitarenios & Stein, 2004).
The MASC
The MASC is a nine-item, 4-point Likert-type self-report scale for children and adolescents that assesses anxiety symptoms. The MASC measures a cross section of anxiety problems in children and adolescents. It consists of 39 items across four basic scales (Physical Symptoms, Harm Avoidance, Social Anxiety, and Separation/Panic), a scale measuring total anxiety, and two major indexes (anxiety disorder and inconsistency). It has been shown to have good internal consistency (α = .60-.85) and high test-retest reliability (r = .79-.93), as well as good convergent validity, as evidenced from its significant correlation with other measures of anxiety (March et al., 1997).
Ethical Considerations
This study was nested within a larger study and was approved by the Health Research Ethics Committee of Stellenbosch University (Ethics Reference Numbers: N04/05/093 and IRB0005239). Informed consent was obtained from participants who were 18 years of age. Participants who were younger than 18 years provided assent, while informed consent was obtained from their parents or legal guardians.
Data Analysis
Data were presented as means (standard deviation) for continuous variables or medians and 25th to 75th percentiles for skewed data and as counts and percentages for categorical variables. We used Statistical Package for Social Sciences version 22 (IBM Corp., 2013) and Statistica version 12 (StatSoft, 2013) for analysis. Using the baseline measurement as reference, paired-sample t tests and Fischer’s least significant difference (LSD) testing were used to compare mean differences at the various time points. Variables were log-transformed to approximate normality prior to analysis where necessary, and the level of statistical significance was set at p < .05.
Results
Sociodemographic Characteristics
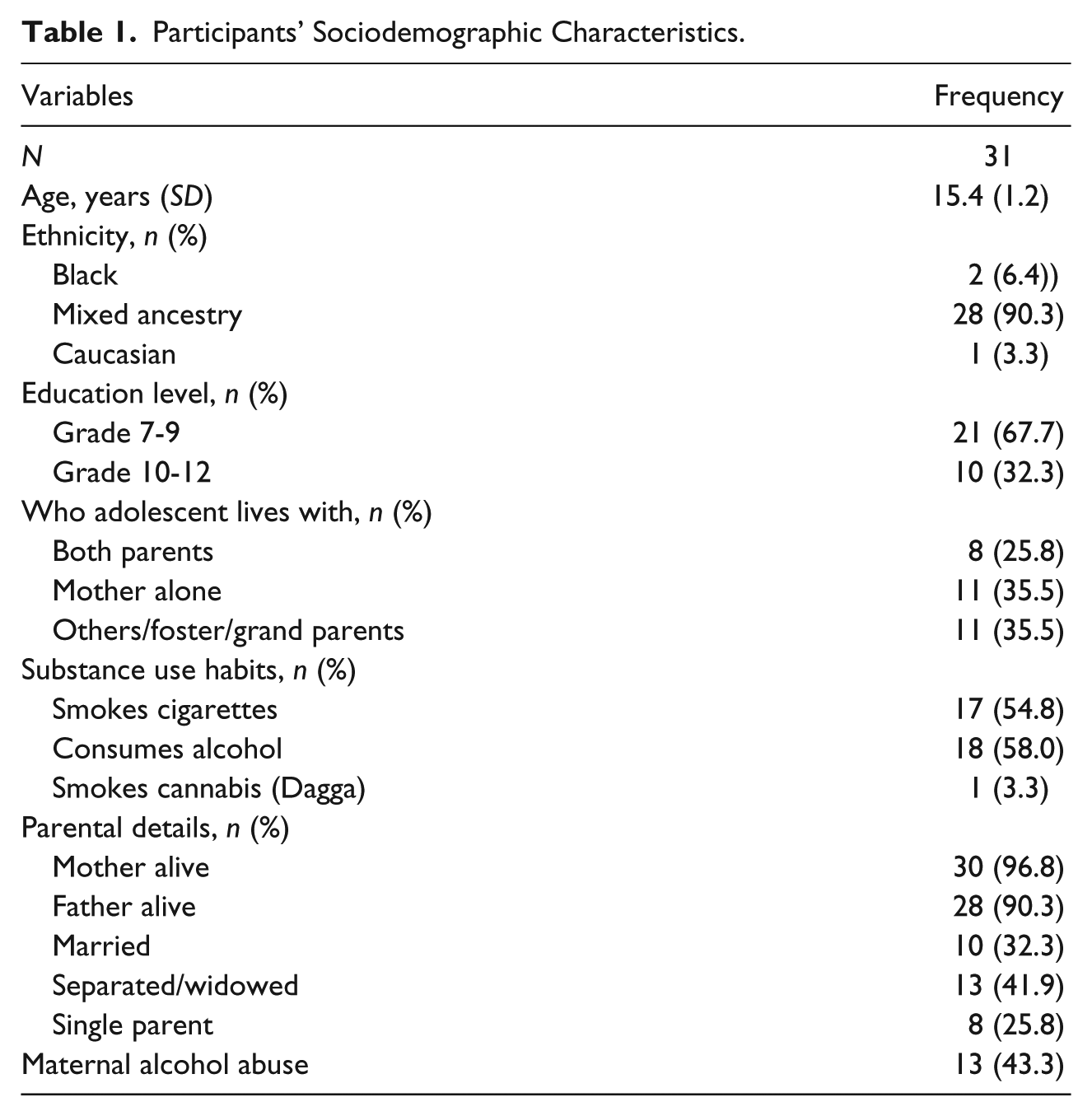
Sociodemographic characteristics are presented in Table 1. Participants (N = 31) ranged in age from 14 to 18 years, with a mean age of 15.4 ± 1.2. The majority, 28 (90.3%), was of mixed ancestry, and almost all (99%) were in Grade 7. A small proportion lived with both parents (25.8%) but most lived with one parent who was often the mother (35.5%). There was also a history of substance use in participants with 17 (54.8%) smoking cigarettes, 18 (58%) regularly taking alcohol, and one participant (3.3%) admitted to using cannabis. About a third (43.3%) of the mothers of participants also used alcohol. The average age of initiation of smoking and alcohol use was 7.9 ± 6.9 and 9.4 ± 7.18 years, respectively.
Participants’ Sociodemographic Characteristics.
Participants’ Mental Health Profile
At enrollment, based on the MINI-Kid, almost a quarter (22.6%) of the sample fulfilled criteria for a current major depressive episode, 12.9% had stress-related symptoms associated with the rape (although diagnosis of PTSD not met) and 16.1% had a pre-existing anxiety disorder. Disordered eating (45.2%) and risk for suicide (54.8%) were also disproportionately high in the group (Table 2). A range of other general emotional disturbances was noted including feelings of terror (90.3%), danger (93.5%), and helplessness (96.8%).
Participants Mental Health Profile.

Note. MINI-Kid = Mini International Neuropsychiatric Interview–Child and Adolescent version; PTSD = posttraumatic stress disorder.
Diagnosis of PTSD cannot be made as duration criterion of 1 month not met.
Course of Probable Psychopathology (Anxiety, Depressive, and Stress Disorder Diagnoses) on Repeat CDI, CATS, and MASC Assessments
Following the initial enrollment of 31 participants, the number of participants seen at the follow-up visits at Months 1, 3, 6, 9, and 12 were 31, 26, 28, 24, and 24, respectively. Retention was, therefore, good and ranged from 77.4% to 100% over the entire 12 months of follow-up.
There was a persistence of probable psychopathology observed in participants based on their performance on the screening instruments over time. Scores on the screening instruments were suggestive of depression, PTSD, and anxiety disorders, and seemed to generally persist with minimal fluctuations as assessed on repeat screening over the year-long evaluation period (Table 3). The high CATS (and low CDI) scores at baseline stabilized by the first re-assessment and remained largely unchanged throughout the year. Likewise, the four-domain index of anxiety (MASC) generally stabilized by the second re-assessment (Month 3), with a gradual reduction in the harm avoidance score, resulting in a significant difference between Months 3 and 12 (10.5 vs. 8.0, p = .003). A significant difference (p = .028) was also noted in separation anxiety scores between Months 1 and 6 (10.8 vs. 9.0) and also between 6 and 9 (9.0 vs. 11.6) on an otherwise flat trend.
Course of Probable Psychopathology (Anxiety, Depressive, and Stress Disorders Diagnoses) on Repeat Assessments.

Note. Mean scores in column followed by the same letter do not differ significantly, whereas if superscript letters differ then observed difference is statistically significant p ≤ .05. CDI = Children’s Depression Inventory; CATS = Child and Adolescent Trauma Survey.
Discussion
We assessed early and long-term mental health outcomes in adolescent girls who had been raped. A number exhibited pre-rape psychopathology in the form of major depression (22.6%) and anxiety (16.1%), and manifested rape-related posttraumatic stress symptoms in the first 2 weeks of the event (12.9%). In addition, despite weekly monitoring and support provided over a 6-week period, symptoms in the main persisted over the 12-month evaluation period, with minimal fluctuations. Possibly on account of the timing of initial assessment (i.e., within 2 weeks of the rape event), we found rates of psychopathology that were lower than the 2-week prevalence for depression (36.1%) and 1-month rate for PTSD (18.7%) reported in a larger cohort from which the present study derives (Nöthling, Lammers, Martin, & Seedat, 2015). Response to rape trauma is complex with considerable inter-individual variation (Briere & Jordan, 2004), such that some may experience severe symptoms or long-term distress whereas others do not (Kendall-Tackett et al., 1993).
Victims of sexual assault are known to have a significantly higher risk for suicide, partly because of the sequelae of increased fear, stress, and anxiety (Downer & Trestman, 2016). In our highly distressed sample, where an overwhelming majority admitted to feeling helpless and in danger, the risk for suicide was similarly high (57%). This rate was almost twice that reported in a sample of rape victims attending a genitourinary clinic in the United Kingdom with 30.4% (Petrak, Doyle, Williams, Buchan, & Forster, 1997), although the difference may partly be accounted for by the adult composition of the sample who may have acquired better coping skills. In addition to the aforementioned mental health outcomes, we also noted high rates of bingeing, smoking, and alcohol consumption in our sample, which is in line with previous trauma-related studies (Ackard et al., 2001; Amstadter et al., 2009; Vlahov, Galea, Ahern, Resnick, & Kilpatrick, 2004). Although eating and substance disorders have complex etiologies, they can also be triggered by sexual assault as part of the mechanisms to cope with the trauma (Springer, 2009). Alcohol consumption is a risk factor for rape and the majority of sexual assaults occur when the perpetrator, the victim, or both have consumed alcohol (Abbey, Zawacki, Buck, Clinton, & McAuslan, 2004; Turner, Finkelhor, & Ormrod, 2006).
Although we did not assess the role of alcohol use/abuse in the rape exposure in the sample, the high rate of alcohol use is noteworthy given the links between alcohol use and increased vulnerability to sexual assault. This study reports a history of substance abuse in these survivors, and 9.7% of the respondents met criteria for alcohol dependence problems at baseline. Most of their parents also used substances, alcohol, and cigarettes. Researchers have shown that parental substance abuse is linked to adolescent substance abuse (Schinke, Fang, & Cole, 2008). In addition, poor parental monitoring and an unstructured home environment are strongly correlated with substance use especially among girls; parents’ failure to monitor their children’s activities can put girls at risk of substance use and other attendant risks (Li, Feigelman, & Stanton, 2000; Schinke et al., 2008). Similarly, a study by Abbey et al., (2004) found that sexual assaults in adolescents were frequently associated with alcohol consumption, as were some drugs (Grisso et al., 1999).
In the context of rape trauma, social support is an important posttrauma factor. We found that only about a quarter of adolescent survivors lived with both parents at the time of the assault; thus, an overwhelming majority (74%) may have missed the protective influence of a two-parent family. It has been noted that adolescents living with two biological or adoptive parents are significantly less likely to experience sexual assault, maltreatment, and non-victimization type of adversity, compared with peers living in single-parent and stepfamilies (Frazier, 2003).
Post-baseline over five time points, mood, anxiety, and stress-related symptom scores stabilized slightly from scores obtained at initial assessment, remaining relatively unchanged and exceeding the clinical cutoffs for psychopathology. Thus, in this sample negative psychological effects mainly persisted for at least a year post-rape. Previous studies suggest that a reduction in psychopathological symptoms is common in the first few months in many victims, but in others symptoms remain elevated even at 2 years post assault (Frazier, 2003; Koss & Figueredo, 2004), suggesting inter-individual variation.
There is evidence to show that early sexual abuse (Arata, 2000, 2002; Desai, Arias, Thompson, & Basile, 2002) and childhood physical abuse (Classen, Palesh, & Aggarwal, 2005; Desai et al., 2002) are significant predictors of adult sexual abuse and revictimization, thus, highlighting the need to flag these vulnerable individuals who may require additional support following early sexual abuse. The Standard Practice Parameter Guidelines for Trauma in Children and Adolescents include trauma-focused interventions (Cohen, the Work Group on Quality Issues, & AACAP Work Group on Quality Issues, 2010). Interventions such as trauma-focused therapies and treatment planning to include treatment for comorbidities are recommended. Individual variations in response to trauma must also be accommodated in treatment planning and follow-up scheduling. The current practice of counseling in our study location, although sufficient for more resilient survivors may be inadequate for others who go on to later develop more complicated emotional outcomes following the rape incident. This is particularly relevant in a society where exposure to complex repeated trauma is common and attendant long-term consequences and risks are well (Gregorowski & Seedat, 2013).
The risks of chronic PTSD, possible neurobiological changes, and potential long-term mental health consequences in adulthood highlight the need for interventions that could reduce the negative consequences of rape trauma. Long-term follow-up for adolescent rape survivors is critical for early identification of those with more persistent symptoms (suggestive of a higher risk for psychopathology) that may require require expert intervention. The high prevalence of trauma and sexual violence in South Africa may require a more intensive approach to rape management with regard to the emotional health impact for inclusion into existing policy.
This study has several limitations. First, several participants had pre-existing psychopathology (i.e., mood and anxiety disorders) that predated the rape. Adolescents with a past history of psychiatric morbidity prior to enrollment were, therefore, included in the study. In addition, rape-related acute stress disorder was not assessed for as it is not a module contained within the MINI-Kid. Posttraumatic stress symptoms were assessed for and, based on clinical enquiry, were deemed to be a consequence of rape exposure. Second, psychopathological status at follow-up was solely based on self-report measures, which may be less precise than clinical interviews, leaving open the possibility that participants may have been misclassified. It should be noted, however, that the CATS scale has previously been validated and an appropriate cutoff recommended for South African youth (Suliman et al., 2005). Third, in view of our focus on longitudinal course of emotional problems, no appropriate comparison group was available and it is, therefore, unclear how these rates compare with unexposed adolescents. Finally, the sample was small thus limiting the generalizability of these findings to all rape exposed adolescents.
Importantly, this study suggests that there are a range of negative immediate and persistent psychiatric symptoms present in adolescents after rape and it underscores the need for early intervention in the form of scheduled screening, follow-up, and long-term monitoring and care. This is particularly crucial given that recent work suggests that, among rape survivors, having a current mental illness is associated with a significantly reduced odds (odds ratio [OR] = 0.25) of attending follow-up services thus underlining the importance of linking post-rape medical care with appropriate mental health services (Darnell et al., 2015).
Footnotes
Acknowledgements
The authors thank Lindi Martin (doctoral student at the department of psychiatry, Stellenbosch University) for coordinating the project and involvement in procuring the data. We also acknowledge Professor Martin Kidd, of the Centre for Statistical Consultation at Stellenbosch University for help with the statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Council Unit on Anxiety Disorders, the South African Research Chair in PTSD supported by the Department of Science and Technology and the National Research Foundation, and by a grant from the Harry Crossley Foundation.