
Abstract
Mental health correlates of intimate partner violence (IPV) victimization including negative physical and mental health outcomes are well documented. However, certain subgroups of African American women, such as those living in impoverished, urban communities, are underrepresented in most studies and may experience IPV at higher rates. Furthermore, the circumstances of this women including poverty makes them at risk to IPV and its consequences. The present study estimated the prevalence of IPV victimization and its association with depression in a sample of low-income African American women participating in the Mobile Youth and Poverty Study. Participants in this study were caregivers of adolescents living in extremely impoverished conditions and were part of the Mobile Youth Survey, a community-based, longitudinal, multiple cohort survey conducted between the years 1998 and 2011. Data for the current study were collected between the years 2001 and 2010. The dependent variable was depressive symptoms as measured by the Center for Epidemiological Studies–Depression Scale (CES-D). The independent variable was IPV measured using a subsample of items from the Conflict Tactics Scale. Nearly three quarters (73.6%, n = 489) of the sample experienced some form of IPV and 49.1% (n = 326) had a CES-D depression score of 16 or greater indicating mild to severe depression symptoms. The highest proportion of women who met the CES-D criteria for depression were those experiencing the most severe IPV irrespective of category (i.e., physical, psychological, or combined). Logistic regression analyses showed that women reporting the most severe abuse, irrespective of category, were significantly more likely to meet the CES-D criteria for depression. In addition, low education and receipt of economic assistance were significantly associated with depressive symptoms. The combination of poor economic conditions and IPV may predispose African American women living in impoverished, urban communities to mental health outcomes such as depression.
Keywords
Introduction
Intimate partner violence (IPV) is a serious public health concern in the United States. According to the latest report from the National Intimate Partner and Sexual Violence Survey (NISVS), over a third (or 35.6%) of women in the United States have experienced rape, physical violence, and/or stalking by an intimate partner in their lifetime (Black et al., 2011). IPV prevalence rates among African American women have generally been shown to be higher than among European American women (Black et al., 2011; Golden, Perreira, & Durrance, 2013; Lacey, McPherson, Samuel, Sears, & Head, 2013). Given the poor mental health outcomes associated with IPV victimization (Coker et al., 2012), low-income African American women experiencing IPV are a particularly vulnerable population because of the possible additive stress from various economic, racial, and social factors (Lacey et al., 2013). The purpose of this study is to investigate the prevalence of IPV and its association with depression in a unique sample of low-income African American women living in impoverished communities in the southeastern United States.
IPV Prevalence Among African American Women
According to the 2010 NISVS, the lifetime prevalence rate for IPV among non-Hispanic Blacks was 43.7% compared with 37.1% among non-Hispanic Whites (Black et al., 2011). Similar rates are consistently reported in other national surveys (Cho, 2012; Halpern, Spriggs, Martin, & Kupper, 2009). However, measurement and data collection methods used in national surveys (e.g., randomly generated lists of home phone numbers or random digit dialing) may lead to an underrepresentation of African American women living in impoverished communities. Researchers have tried to combat this issue by recruiting participants from unique settings, such as clinics and emergency rooms, where access to this population is greater. For example, Anderson, Stockman, Sabri, Campbell, and Campbell (2015) approached African American and African Caribbean women visiting family planning, prenatal, and primary care clinics and completed interviews using an audio computer-assisted self-interview (ACASI) system. Forty-two percent (n = 380) of the respondents who consented and completed the study survey reported having experienced recent IPV (Anderson et al., 2015). Similarly, Houry, Kemball, Rhodes, and Kaslow (2006) approached African American women in an emergency room setting to complete a computerized screening for IPV and various mental health correlates. Of the 569 self-identified African American females who agreed and completed the survey, 461 (or 81%) had been in an intimate relationship in the past year, and 167 (36%) disclosed IPV (Houry et al., 2006). In another study, Fincher and colleagues (2015) used two forms of assessment—face-to-face interview and computerized interview—to assess IPV prevalence in a sample of African American women receiving Special Supplemental Nutrition Program (SSNP) services at Women, Infants, and Children (WIC) clinics. Between 34% and 48% of women reported IPV lifetime rates, with higher rates found in the face-to-face interviews where the personal connection helped foster a trusting relationship (Fincher et al., 2015). The present study builds on this culturally tailored, personalized assessment by employing face-to-face interviews during home visitations.
IPV and Mental Health Outcomes
Research consistently shows that IPV is associated with several adverse outcomes including injuries (Anderson et al., 2015) and poor mental health functioning (Plichta, 2004). Mental health correlates of IPV victimization, in particular, are well documented among female victims. For example, IPV substantially increases the risk for mental health problems such as eating disorders (Bundock et al., 2013), depression (Lacey et al., 2013), posttraumatic stress disorder (Dutton, Bermudez, Matas, Majid, & Myers, 2013), and suicidal ideation (Alhusen, Frohman, & Purcell, 2015) among women. The strength of the relation between depression and IPV has been particularly robust (Lilly & Graham-Berman, 2009; Prosman, Jansen, Lo Fo Wong, & Lagro-Janssen, 2011; Rhodes, Lauderdale, He, Howes, & Levinson, 2002; Teitelman, Ratcliffe, McDonald, Brawner, & Sullivan, 2011). In a meta-analysis, Stith, Smith, Penn, Ward, and Tritt (2004) found a moderate effect size for the association between depression and IPV among victims and perpetrators of IPV. Rhodes and colleagues (2002) found that female patients who reported IPV victimization were over 2 times more likely to report depressive symptoms and almost 5 times more likely to have attempted suicide compared with female patients not reporting IPV victimization. Thompson, Kaslow, and Kingree (2002) found that women reporting prior year IPV victimization were more likely to attempt suicide if they had elevated symptoms of depression. Results from studies also indicate that some women who experience IPV have chronic depression, which can be exacerbated by not only the stress of the violent relationship (J. C. Campbell, 2002) but also social and ecological factors (Lacey et al., 2013, Lacey et al., 2015).
Particularly for low-income African American women, IPV has been shown to be associated with depression, posttraumatic stress symptoms, and suicidal ideation (Fincher et al., 2015; Houry, Kaslow, & Thompson, 2005; Houry, Kemball, Rhodes, & Kaslow, 2006; Lacey et al., 2013; Leiner, Compton, Houry, & Kaslow, 2008). In a sample of African American women, who screened positive for past-year IPV during an emergency room visit, one fourth reported moderate to severe levels of depressive symptoms and 6% reported suicidal ideation (Houry et al., 2006). Similarly, in a study of predominantly African American (93%) pregnant women, depressive symptomatology (odds ratio [OR] = 17.04; 95% confidence interval [CI] = [2.10, 38.27]) and experiencing IPV (OR = 9.37; 95% CI = [3.41, 25.75]) were significantly associated with an increased risk of suicidal ideation (Alhusen et al., 2015). Low-income, African American women are more likely to experience issues of racism, gender-based and race-based discrimination, oppression, and poor living conditions compared with their White American peers (Pager & Shepherd, 2008). African American women may also have fewer economic resources, human support networks, and greater stress exposure than White American women. These factors and experiences may exacerbate the effects of IPV (Lacey et al., 2013).
Despite these findings, Ramos (2008) and others (see R. Campbell, Raja, & Grining, 1999; Stover & Lent, 2014) suggest that many mental health professionals have little training in identifying or treating individuals with IPV. In addition, Taft, Bryant-Davis, Woodward, Tilman, and Torres (2009) suggest that these mental health professionals have even less knowledge and skills on how to tailor assessment and treatment of IPV that are culturally appropriate for minority for racial and ethnic populations. More research is needed on the relationship between IPV victimization and depression in low-income African American women to promote tailored treatment protocols that can be maximally effective and culturally responsive. Thus, the present study takes a step toward addressing this limitation by investigating the prevalence and mental health correlates of IPV in a unique sample of low-income African American women living in impoverished communities in the southeastern United States. As mentioned above, the present study uses face-to-face interviews during home visitation to query participants about IPV victimization experiences and depressive symptoms.
Method
Participants and Recruitment Procedures
The present study uses face-to-face interviews during home visitation to query participants about IPV victimization experiences and depressive symptoms. The data utilized in the current study is derived from the Mobile Youth Study (MYS), a multiple cohort, longitudinal study of poverty and adolescent risk. The MYS study was conducted in the most impoverished neighborhoods in the Mobile, Alabama Metropolitan Statistical Area (MSA) between 1998 and 2011. In 1998, MYS researchers identified the 13 poorest neighborhoods in the MSA and surveyed adolescents within those neighborhoods. The census data at the beginning of the study (i.e., 1990 census) showed that these neighborhoods had a median household income of US$5,190 and a 73% poverty rate (U.S. Census Bureau, 2012) The researchers followed participants as they moved throughout the study thus adding new neighborhoods. By 2011 the MYS was conducted in 50 neighborhoods (see A. C. Bolland, 2012; K. A. Bolland et al., 2016, for a discussion of MYS procedures and the MYS sample).
The survey for the present study was administered cross-sectionally between the years 2001 and 2010 to a sample of adults (1,043: 180 men and 863 women) to caregivers of the original MYS participants. This secondary study was referred to as the Adult and Family Dynamics Questionnaire (AFDQ). Because of length, the AFDQ was separated into two sections and several subsections that could be completed at different times; not all participants completed all sections. The complete survey took approximately 3 hr to complete. Participants were compensated for their time between US$12 and US$50 (depending on the number of sections completed). The University of Alabama’s Institutional Review Board approved the study.
Given that the objective of the current study is to examine IPV victimization among African American women, out of the 1,043 respondents who were administered the AFDQ, men (n = 180) were excluded. Also excluded were women who did not self-identify as African American (n = 73) and those without information on interpersonal violence (n = 126). The final sample thus contained 664 adult African American women.
The mean age of participants was 38.9 years (SD = 12.9). Many participants were unmarried, but currently dating (38.6%, n = 256); some participants had never married and were not dating (29.2%, n = 194); 15.2% were separated or divorced and not currently dating (n = 101); a few were currently married (6.0%, n = 40) or widowed (6.9%, n = 46); and marital status could not be ascertained on 4.1% (n = 27) of the participants. A majority of the participants (88.1%, n = 585) received economic assistance and 11.9% (n = 79) did not report receiving economic assistance. In this sample, 60.1% (n = 397) had completed high school or received GED and 39.9% (n = 264) had not completed high school or received a GED.
Measures
Dependent variable
Depressive risk, as measured by the Center for Epidemiological Studies–Depression Scale (CES-D; Radloff, 1977), served as the dependent variable in this study. The CES-D is a 20-item measure where participants indicate how often, over the past week, they experienced symptoms associated with depression, such as restless sleep, poor appetite, and feeling lonely. Participants rate the extent to which they have experienced each of these symptoms none of the time (=0), rarely (=1), some or little of the time (=2), or most or all of the time (=3). For this scale, total scores range from 0 to 60, with higher scores indicating greater depressive symptoms. The CES-D was designed to measure depressive experiences in the general population and includes items reflecting major dimensions of depression including depressed affect, positive affect, somatic symptoms/retarded activity, and interpersonal (Radloff, 1977). The CES-D has been validated in a general population and clinical patient samples (e.g., Chung et al., 2015; Foley, Reed, Mutran, & DeVellis, 2002) and has been utilized in ascertaining depressive symptoms among individuals both current and lifetime IPV (Bonomi et al., 2006; Zlotnick, Johnson, & Kohn, 2006).
Internal consistency for the scale in general and clinical populations is very good (α = .85 and .90, respectively; see Radloff, 1977). The internal reliability of the CES-D for the present study was α = .83). A cutoff score of 16 or greater has been shown to be an indicator of individuals at risk for clinical depression, with good sensitivity and specificity as well as high internal consistency (Lewinsohn, Seeley, Roberts, & Allen, 1997). Thus, depressive symptoms were dichotomized into less than 16 (=0) and equal or greater than 16 (=1) to distinguish those at risk for clinical depression. The CES-D mean score for the current sample was 17.0 (SD = 10.5), and 49.1% (n = 326) of the sample had CES-D scores equal or greater than 16.
Independent variables
IPV served as the independent variable and was measured using select items from the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). The CTS2 measures 39 self-rated behaviors (or acts) coded into five categories: (a) negotiation (six items), (b) physical assault (12 items), (c) sexual coercion (seven items), (d) psychological aggression (eight items), and (e) injury (six items). Each category is composed of items that represent a range of severity. A strength of the CTS2 is that it allows items to be classified into categories and classified by severity level (e.g., minor and severe; Strauss et al., 1996). The CTS2 has been used in many studies involving both married and dating partners with evidence of reliability and validity (e.g., Archer, 1999; Straus, 2004). For instance, Straus and colleagues reported internal consistency reliability of .86 for the Physical Assault subscale and .79 for the Psychological Aggression subscale.
To accommodate the various questions asked, the researchers limited questions in the AFDQ to only two subscales of the CTS2 (i.e., Psychological Aggression and Physical Assault; see Table 1). These two scales provided information that was deemed sufficient to answer the current study’s research questions. The individual items in each subscale were weighted according to their severity, with the act associated with questionnaire item being categorized as minor or severe (Straus et al., 1996). Scoring was conducted using the prevalence method, which indicates whether one or more of the acts in the scale occurs and does not differentiate on the basis of how many of the acts occurred or how often each act was used (Straus, 2004).
Proportion of Women Reporting Interpersonal Violence Acts Committed by Current, Previous, or Any Partner.
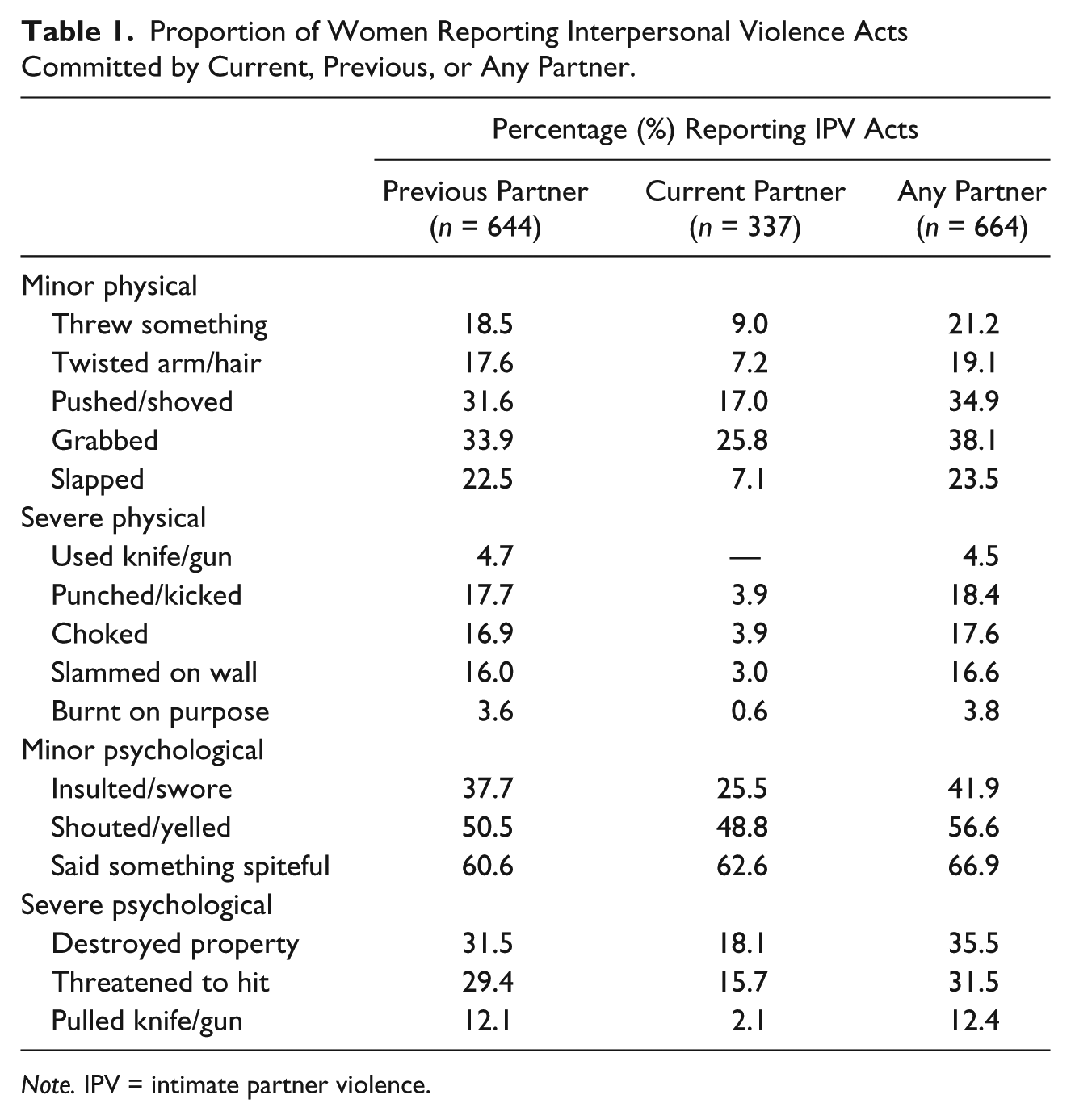
Note. IPV = intimate partner violence.
The Physical Assault subscale (PhA) was categorized and coded as follows: respondents indicating that they had experienced any severe form of IPV from either a current and/or past relationship were categorized as (a) having experienced severe IPV (coded as 2), (b) those who experienced minor IPV and no severe IPV either from a current and/or past relationship were categorized as minor (coded as 1), and (c) those who had never experienced any IPV either in their current and/or past relationship were categorized as none (coded as 0). Thus, the Physical Assault subscale (PhA) was coded as 0 = none, 1 = minor, and 2 = severe. The Psychological Aggression severity subscale (PsA) was categorized and coded in the same way. The internal consistency coefficients for the Physical Assault scale and Psychological Aggression scale were very good (α = .85 and .80 respectively). The participant distribution on the Physical Assault subscale was as follows: none (52.8%, n = 351); minor (21.5%, n = 143); severe (25.6%, n = 170). While for psychological aggression, the distribution was none (27.3%, n = 181); minor (28.3%, n = 188); severe (44.4%, n = 295).
Cognizant that violence does not occur in isolation (i.e., a woman experiencing physical violence is also likely to experience psychological violence) and that the effect of experiencing both severe psychological and severe physical violence on depression is likely to be higher than experiencing either type on its own, a four-category composite IPV severity scale (CoS) was used. Previous studies have evaluated the effect of co-occurrence of physical and psychological violence (Barreira, Lima, & Avanci, 2013; Graham, Bernards, Flynn, Tremblay, & Wells, 2012; Jun, Rich-Edwards, Boynton-Jarrett, & Wright, 2008). The CoS was created as follows:
CoS
i
(none) = 0 if PhA
i
= 0 CoS
i
(minor only) = 1 if (PhA
i
= 1 CoS
i
(severe; i.e., severe on one) = 2 if (PhA
i
= 2 CoS
i
(very severe; i.e., severe on both) = 3 if PhA
i
= 2
The participant distribution on the composite IPV severity scale (CoS) was none (26.4%, n = 175); minor (27.1%, n = 180); severe (23.0%, n = 153); very severe (23.5%, n = 156).
Demographic and other covariates
Previous research indicates that various demographic and socioeconomic factors influence the relationship between experiencing IPV and depressive symptoms (e.g., Chuang et al., 2012; González-Guarda, Peragallo, Vasquez, Urrutia, & Mitrani, 2009; Tjaden & Thoennes, 2000). For instance, Chuang and colleagues in a population-based longitudinal survey of women aged 18 to 45 found that in addition to IPV, older age, lower educational attainment, and lower household income were all significant predictors of depression. Thus, additional variables collected as part of the AFDQ were included in the analyses to control for possible confounding. As a measure of poverty, respondents were asked whether they received public support, including unemployment insurance benefits, Supplemental Nutrition Assistance Program (SNAP), Temporary Assistance for Needy Families (TANF), and supplemental security income (SSI). If they indicated that they received benefits from any of these programs, public support was coded as 1; otherwise it was coded as 0. Participants were also asked to report their age and marital status. Age in years was categorized and coded as follows: 19 to 24 (=1); 25 to 34; (=2); 35 to 44 (=3); 45 to 54 (=4); 5 = 55 plus (=4), while for marital status the coding was never married (=1); not dating, dating/engaged (=2); currently married (=3); separated/divorced and not currently dating (=4); unknown (=1). Finally, participants were asked to indicate their education level, which was dichotomized and coded as did not complete high school (=0); high school completion, GED, or more (=1).
Analysis Plan
All the analyses were conducted in STATA12 (StataCorp, 2015). Descriptive analyses were first conducted. Next, the proportion of women reporting various acts of IPV committed by the previous, current partner, and any partner(s) was obtained. Chi-square tests were conducted to establish the relationship between meeting CES-D criteria for depression and the various predictor variables. This was followed by t tests with corrections on the significant relationships to ascertain the specific proportions that were significant. Finally, logistic regression analyses were conducted to examine the associations between meeting the CES-D criteria for depressive symptoms and IPV. Given preliminary bivariate analyses between the various IPV measures (i.e., physical assault, psychological aggression, and composite IPV severity scale), showing that there was high correlation between the variables coefficients (Cramér’s V values ranged from 0.51 to 0.77), three separate logistic regression analyses for each type of IPV (i.e., physical assault, psychological aggression, and composite IPV severity scale) were conducted.
Results
Descriptive Statistics
In general, nearly three quarters of the women in the sample (73.6%, n = 489) reported experiencing some form of IPV. The proportion of participants reporting various acts of IPV committed by previous, current, and any intimate partner are presented in Table 1. Minor psychological aggressions were the most prevalent acts of IPV committed by current or previous intimate partners with “saying something that is spiteful” being the most reported form of abuse by both current (62.6%) and previous (60.6%) partners. Conversely, severe forms of physical assault were the least reported acts of IPV, with a partner using a knife or gun (i.e., current partner 0.0%; previous partner 4.7%) and burning/scalding a partner on purpose (i.e., current partner 0.6%; previous partner 3.5%) being the least reported acts of IPV.
Chi-square tests indicated that age group, receipt of economic assistance, and reporting any type of IPV (i.e., physical assault [PhA]; psychological aggression [PsA], or composite IPV [CoS]) were significantly related to meeting CES-D criteria for depressive symptoms (Table 2). Post hoc t test analyses with corrections showed significant difference in meeting CES-D criteria among participants aged 55 years plus and those not receiving economic support. In terms of IPV, a significantly higher percentage of those reporting severe PhA, severe PsA, and severe CoS met the CES-D criteria for depression. Similarly, a significantly higher percentage of participants reporting very severe CoS met the CES-D criteria for depression.
Relationship Between Meeting the CES-D Criteria for Depression and Predictor Variables.

Note. Bold indicates statistically proportional differences on follow-up t tests after corrections. CES-D = Center for Epidemiological Studies–Depression Scale.
Severe in either physical assault or psychological assault.
Severe in both physical assault and psychological assault.
Logistic Regression
Prior to analyzing the effects of IPV on depression, demographic covariates were evaluated in each of the three logistic regression models. Results are presented in Table 3. Results indicate that all covariates (age, marital status, education, and economic assistance) were significantly associated with meeting the CES-D criteria for risk of depression in all three models for PsA, PhA, and CoS. Women with low education and those receiving economic assistance were significantly more likely to meet the CES-D criteria for risk of depression. Conversely, participants who were older (i.e., 55 years plus) were less likely to meet the CES-D criteria for depression when compared with those 19 to 24 years. In addition, women who indicated that they were married and those who were dating/engaged were less likely to meet the CES-D criteria for depression when compared with those who had never been married and were not currently dating, in all the three models.
Logistic Regression Analysis of the Association Between Depression and Reporting Physical, Psychological, and Combined Interpersonal Violence.

Note. N = 664. PsA = psychological aggression; PhA = physical assault; CoS = composite IPV.
p < .05. **p < .01.
After adjusting for the demographic covariates, each of the three IPV variables (PsA, PhA, and CoS) were found to significantly increase the likelihood of depressive symptoms. Results of the adjusted logistic regression model are presented in Table 3. Women reporting severe PsA (OR = 2.25, 95% CI = [1.49, 3.40]), severe PhA (OR = 2.92 95% CI = [1.94, 4.40]), and severe CoS (OR = 2.02, 95% CI = [1.26, 3.24]) were all significantly more likely to meet the CES-D criteria for depression risk than those who had not experienced instances of IPV after controlling for sociodemographic factors. In addition, compared with women who did not experience PhA, those experiencing minor PhA were significantly more likely to meet the CES-D criteria for depression (OR = 1.69, 95% CI = [1.12, 2.55]. Last, women reporting severe CoS (OR = 2.02, 95% CI = [1.26, 3.24]) and very severe CoS (OR = 2.84, 95% CI = [1.75, 4.62]) were significantly more likely to meet the CES-D criteria for depression.
Discussion
The purposes of the current study were twofold: (a) to examine the prevalence of IPV in a sample of predominantly African American women living in highly impoverished neighborhoods and (b) to examine the relation between IPV and comorbid depressive symptoms. Results indicate that nearly three quarters of the study participants had experienced some form of IPV. Furthermore, more than half of women in current study reporting IPV met the criteria for comorbid depressive symptoms as measured by the CES-D. In addition, severe IPV (irrespective of type) was significantly associated with increased likelihood of depressive symptoms. The prevalence of IPV in the current study are much higher than the 43.7% national prevalence among African Americans as reported by the latest NISVS (Black et al., 2011) and the levels reported by other researchers (Fincher et al., 2015; Houry et al., 2006). Fincher and colleagues (2015) in a study of low-income African American women receiving WIC reported lifetime and past-year IPV prevalence rates of 50% and 36% respectively, while in Houry and colleagues (2006) study, 36% of African American women in an emergency room reported past-year IPV (Houry et al., 2006). Differences in these rates could be due to differences in assessment methods. The MYS was a community-based study that relied on face-to-face interviews to gather sensitive information about IPV rates. Participants may have been more willing to share information considered confidential such as IPV history in this setting.
In terms of specific forms of IPV, our findings indicate that minor psychological forms of IPV (i.e., swearing, shouting/yelling, and saying something spiteful) were the most prevalent in both current and previous partner relationships. These rates of psychological aggression are consistent with the literature. Fortin, Guay, Lavoie, Boisvert, and Beaudry (2012), in a study of young couples, found that 80% of the participants had experienced at least one act of the minor psychological aggression. Even minor psychological aggression in partner relationships may be meaningful as they can escalate to severe violence. In the current study, out of the 295 women who had experienced severe psychological aggression, 97.3% (n = 287) of them had also experienced minor psychological abuse. Some researchers have found that the effects of psychological abuse are just as detrimental, if not more detrimental, than physical abuse (Sackett & Saunders, 1999; Street & Arias, 2001). Tolman and Bhosley (1991) found that psychological abuse was more strongly associated with psychosocial problems when compared with threats of or actual physical abuse. In the current study, the women who experienced severe psychological aggression, a majority of whom had also experienced minor psychological aggression, were 2.25 times likely to meet the CES-D criteria for depression.
Nearly half of the participants in this study reported experiencing physical abuse, with those experiencing even minor physical violence being significantly more likely to meet the CES-D criteria for depression. This finding is consistent with several studies that demonstrate a link between physical abuse and depression (e.g., Houry, Reddy, & Parramore, 2006; McCauley et al., 1995; Stith et al., 2004). It is noteworthy that in addition to mental health problems, physical abuse has been linked to an increased risk of injuries or other chronic illnesses including chronic pain, headaches, and osteoarthritis (J. C. Campbell & Soeken, 1999; Coker, Smith, Bethea, King, & McKeown, 2000).
About half of the women in our study experienced both physical assault and psychological aggression, which is consistent with other research that has found that women typically experience more than one form of abuse (Lacey et al., 2013; Outlaw, 2009; Wyatt, Axelrod, Chin, Carmona, & Loeb, 2000). Wyatt and colleagues (2000) studied African American women with mixed HIV serostatus and found that about half of the women had experienced a combination of both physical and verbal conflict in addition to moderate to severe physical abuse. Similarly, Outlaw’s (2009) analysis of the National Violence Against Women Survey (NVAWS) data revealed that women who had experienced physical abuse were twice (sometimes 3 or 4 times) more likely to experience nonphysical abuse. In the current study, women reporting the severe abuse in either physical assault or psychological assault and those reporting severe abuse in both physical assault and psychological assault were more than 2 times likely to meet the CES-D criteria for depressive symptoms. This concurs with Jun et al.’s (2008) findings that co-occurrence of psychological abuse with physical or sexual abuse magnifies the risk of smoking among abused women, whereby smoking, especially among women, has previously been shown to be a means of reducing stress (Kassel, Stroud, & Paronis, 2003).
It is worth noting that reporting severe IPV, irrespective of type of IPV, was significantly associated with increased likelihood of depressive symptoms. This finding concurs with previous studies of African American women (e.g., Houry et al., 2005; Leiner et al., 2008) and the general population (Cascardi, Langhinrichsen, & Vivian, 1992; Coker et al., 2002; Graham et al., 2012; Johnson & Leone, 2005), showing that severity of IPV is associated with depressive symptoms. Women experiencing IPV, especially when the IPV is continuous, have the potential of developing poor coping mechanisms such as learned helplessness and feelings of powerlessness (Renner & Slack, 2006; Walker, 1978, 2000), and even accepting IPV as part of marital life (Mugoya, Witte, & Ernst, 2015) all of which can lead to depression. Graham et al. (2012) noted that “if depression is a consequence of IPV, it may operate through feelings of powerlessness and the emotional impact of victimization for women” (p. 769). The consequences of learned helplessness, including low self-esteem, apathy, passivity, and difficulties with problem solving, are characteristics common among IPV victims (J. C. Campbell, Kub, & Rose, 1996; Clements & Sawhney, 2000), which also can lead to depression. Another explanation that may be relevant to the findings is the extent to which individuals in the current study experienced unmeasured factors commonly reported among low-income, African American women (e.g., racism, discrimination, oppression, and poor living conditions). As previously mentioned, these race- and cultural-specific factors and experiences may impact levels of and outcomes associated with IPV (Lacey et al., 2013; Taft et al., 2009).
All the covariates evaluated (i.e., age, marital status, education, and economic assistance) were significantly associated with depressive symptoms. A majority of the participants (88.1%) reported receiving economic assistance. Furthermore, those receiving economic assistance were significantly more likely to meet the CES-D criteria for depressive symptoms irrespective of the type of IPV reported (see Table 3). Similarly, women with low education (i.e., no high school diploma or GED) were significantly more likely to experience all forms of IPV. This finding is consistent with previous studies showing a relationship between low social economic status and experiencing IPV (Chuang et al., 2012; Hernandez, Marshall, & Mineo, 2014; Mitchell et al., 2006). Hernandez et al. (2014) found that women experiencing economic hardship were at a significantly increased risk of experiencing depression. Mitchell et al. (2006) in a sample that included low-income African American women found that women acknowledging abuse also reported more symptoms of depression. While participants in the current study were recruited from low-income neighborhoods, implying that a majority were from low socioeconomic status, women receiving economic support and with low levels of education are likely to be representative of those who have even fewer tangible resources available to them. Such women may feel as though they do not have control over certain aspects of their life including economic support and thus may be more fearful of consequences that often follow the use of active coping strategies like leaving an abusive spouse. Indeed previous research has shown that economic insecurity increases the risk for depressive symptoms among low-income women, especially those receiving economic assistance such as welfare (Horwitz & Kerker, 2001). Older women (55 years plus) were less likely to meet the CES-D criteria for depression when compared with their younger colleagues (19-24 years) after adjustment for all variables. Additional research utilizing larger sample size needs to be undertaken to clarify this finding. This result is consistent with findings by González-Guarda et al. (2009) but contradicts Chuang et al.’s (2012) findings. Last, women who were currently married and those dating/engaged were significantly less likely to report IPV when compared with those who were never married and were not currently dating. It is thus possible that being in a relationship acted as a protective factor for depressive symptoms.
Study Limitations
The findings of this study should be considered with the following limitations in mind. First, the cross-sectional design does not allow for establishing a temporal relationship between IPV and depression. Thus, while it is not possible to establish a temporal relationship between IPV and depression, our results are consistent with results from other studies that demonstrate a significant positive relationship between IPV and depression (e.g., Dienemann et al., 2000; Resnick, Acierno, & Kilpatrick, 1997). Furthermore, longitudinal studies have shown that depression decreases with a reduction in IPV (J. C. Campbell & Soeken, 1999; Silva, McFarlane, Soeken, Parker, & Reel, 1997).
Second, the analysis is based on participants with complete data, leaving a possibility of nonrepresentativeness of those with incomplete data to the entire AFDQ sample. Participants were instructed that they did not have to answer questions and the response options of “no answer” or “don’t know” were available for all questions regarding IPV. Missing values were relatively infrequent, and therefore eliminating cases with missing values (i.e., =126 or 14% of women surveyed) should introduce little bias into the results.
Third, while participants in the AFDQ were recruited randomly, as is the case in many social science research studies, resources were not available to recruit all caregivers of the original MYS. Thus, it is possible that those who participated in the AFDQ are not representative of the population of MYS caregivers or of the population of caregivers living in the highly impoverished neighborhoods identified in the MYS. The generalizability of the results to populations beyond highly impoverished adult female African American caregivers of adolescents is also quite limited.
Fourth, the measures utilized in the current study are based on self-report and may therefore be biased. Of particular concern is the possibility that women who are depressed may believe that IPV is a “cause” of the depression and therefore exaggerate its incidence.
Finally, decisions about combining variables may have biased interpretations in one direction or another. For example, the decision to combine current and previous reports of abuse makes interpretation of current depressive risk more difficult; however, the incidence of abuse during any single romantic relationship may be small and very dependent on the length of the relationship. Moreover, over half of the women in the sample reported that they were not currently in a romantic relationship. Thus, lifetime or cumulative incidence is a better measure than either current or past incidence alone. As another example, abuse was considered severe if even a single severe type of abuse (e.g., burning) was experienced. Thus, the assumption is made that the effects of abuse are a function of the most severe experience rather than the number of different types of abuse experienced. Finally, we used receipt of public assistance benefits as a measure of poverty. While actual income is a better measure of poverty, measuring income is fraught with methodological challenges. Indeed, we attempted to measure income, but because of inconsistencies, missing data, and other problems with the measure we chose the simpler measure of public support.
Conclusion and Implication for Practice and Research
Overall, our findings show that IPV is prevalent among African American women living in impoverished communities. In addition, IPV is significantly associated with depressive symptoms among African American women, especially those experiencing the most severe forms of IPV. These findings have both clinical and research implications for professionals, including psychologists and counselors, working with IPV victims, especially African American women.
Given the results showing that nearly half of the sample (49.1%, n = 326) met criteria for probable depressive symptoms (i.e., had CES-D score of 16 and above), counselors and other mental health providers working with African American IPV victims should be encouraged to screen for depressive symptoms in this population. Furthermore, given previous research showing that a majority of IPV victims seeks help from mental health professionals, rather than other service providers such as the police (e.g., R. Campbell, Raja, & Grining, 1999; Fanslow & Robinson, 2010), there is need for increased training among mental health professionals on how to identify and counsel IPV victims. Unfortunately, many mental health professionals have little or no training in identifying or treating IPV victims (R. Campbell et al., 1999; Ramos, 2008; Stover & Lent, 2014). In addition, professionals should be more aware of services available for IPV victims in their communities and how those services may need to be culturally tailored (Gillum, 2008; Hien & Ruglass, 2009; Lacey et al., 2015).
In addition to being competent to provide services to individuals who present with a history of IPV and comorbid mental health conditions, providers should be aware of other barriers that often exist for individuals in general and African American in particular engaging in help seeking behaviors (see Hien & Ruglass, 2009; Taft et al., 2009). Toward this end, a recent study involving predominantly African American women in Baltimore found that a majority of women who had experienced IPV did not utilize available resources evidenced in the community, with only 18% of the women accessing domestic violence–specific resources and 13% of the women using health care resources such as primary care providers or emergency room personnel (Lucea et al., 2013). A majority of the women in Lucea and colleagues’ study who did not utilize domestic violence–specific resources indicated that they were unaware of resources available to them. Lucea and colleague’s results are not unique. Postmus, Severson, Berry, and Yoo (2009) previously found that women experiencing IPV reported a lack of knowledge about available resources as a barrier to seeking them.
The consideration of providers’ level of competency in working with individuals who experience IPV and individuals access to and awareness about resources are not the only implications we highlight. In addition to depression, the increased risk of IPV among racial minority women may be a contributing factor to health disparities observed in this population. Pearlin, Schieman, Fazio, and Meersman (2005) noted that exposure to trauma (e.g., through IPV) increases the risk for later experience of stress, which in turn contributes to health disparities observed in these populations. Thus, there is need for more research, especially longitudinal studies, to elucidate the effect of IPV including its direct relationship to mental health effects and its contribution to health disparities among minorities. Last, the association between economic support, IPV, and depression warrants further research. Future researchers should consider employing larger samples and utilize additional measures of social economic status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.