
Abstract
The division of batterers into subtypes is hardly ever used, neither to describe the type of perpetrator nor to indicate in the clinical decision-making process what treatment should be offered. In this study, a sample of male perpetrators of intimate partner violence (IPV) who had been advised to seek treatment at a community-based Dutch forensic psychiatric facility (N = 110), either voluntarily or mandatorily, have been divided into four subtypes based on a model reported by Holtzworth-Munroe and Stuart (1994). The four subtypes are Family-Only (FO), Borderline-Dysphoric (BD), Generally Violent Antisocial (GVA), and Low-Level Antisocial (LLA). The aim of the study was to identify the subtypes and to compare the different groups on descriptive dimensions and treatment allocation. In the first part of the study, aside from identifying the batterer subtypes, important differences between the subtypes were encountered in the nature of the violence (structural vs. incidental). The characteristics of the BD subtype were found to be similar to the model except for the psychopathological dimension. Differences in allocation of treatment types between batterer subtypes were not substantial raising questions about the correspondence between typological subtypes and the judgment of clinicians. These results do suggest that more attention should be paid to the heterogeneity of the batterer population, which could improve treatment and advance our understanding of IPV.
Intimate partner violence (IPV) refers to violence committed by a partner in a romantic relationship (Saunders, 2004). This is a common problem that affects 30% of women worldwide (World Health Organization [WHO], 2013). Even in a highly developed country such as the Netherlands, 5.8% of the population has indicated to have been a victim of IPV in the previous 5 years (Van der Veen & Bogaerts, 2010). Violence in IPV is “the actual, attempted, or threatened physical harm of a current or former intimate partner” (Kropp, Hart, & Belfrage, 2005, p. 1), and it is therefore comprised of both physical and psychological violence. Victims of IPV experience lasting consequences such as physical injury, substance abuse, and chronic mental illness (Coker et al., 2002). The majority of IPV suspects are male (83% in the Netherlands), and men are also more likely to engage in more severe and structural forms of violence (Römkens, 2010; Van der Veen & Bogaerts, 2010). However, an increasing body of literature suggests that violence between partners is often bidirectional: In violent relationships, women are found to also regularly commit IPV (see, for example, Anderson, 2002; Langhinrichsen-Rohling, Misra, Selwyn, & Rohling, 2012; Straus, 2011; Van der Veen & Bogaerts, 2010; Whitaker, Haileyesus, Swahn, & Saltzman, 2007). Nevertheless, this study has focused only on men because the majority of patients in community-based forensic psychiatric treatment after committing IPV in the Netherlands are men (see, for example, Thijssen & De Ruiter, 2010; Van der Veen & Bogaerts, 2010).
Researchers have increasingly emphasized the importance of considering the heterogeneity in the batterer population, and one common approach is by using typologies (Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000; Huss & Ralston, 2008; Thijssen & De Ruiter, 2010). More knowledge on batterer typologies in forensic outpatient treatment might result in an improved and timely identification of risk factors, and could also allow men who are violent toward their partner to receive more effective treatment which could reduce instances of IPV. This study aimed to identify batterer subtypes and investigated to what extent the typology originally reported by Holtzworth-Munroe and Stuart (1994) could be replicated. First, to create a more rigorous and complete typology, both actual (physical) violence and threatened violence have been included; the latter being conceptualized as a form of psychological violence. Second, our typology has been created based on both past and present data on IPV. This made it possible to distinguish incidental batterers (i.e., men who commit IPV very sparsely) and structural batterers (men who have longer histories of IPV). This could be of considerable interest because structural violence is predictive of future violence (Cattaneo & Goodman, 2005). Third, the personality disorders (PDs) of the men in the sample, as diagnosed by the clinicians, were included. In previous typology studies, it has been found that the PDs of the batterers do not always correspond to those theorized by Holtzworth-Munroe and Stuart (1994; see, for example, Cunha & Goncalves, 2013; Fowler & Westen, 2011). Thus, it is interesting to investigate how far the theorized personality differences resemble the judgment of the clinicians. Finally, because the men in the sample could be enrolled in different types of treatments, the differences between the batterer types concerning the type of treatment that they were allocated to by the clinicians were studied.
Replication of Batterer Typology and Descriptive Dimensions
Delsol, Margolin, and John (2003) have pointed out that the first generation of research on IPV focused on comparing violent and nonviolent men. However, the results of these studies were often inconclusive (Chiffriller & Hennessy, 2006; Dixon & Browne, 2003; Holtzworth-Munroe & Stuart, 1994) with one explanation being that IPV perpetrators are a group which is too heterogeneous to generalize. To address this heterogeneity, the next generation of researchers focused on creating typologies of IPV perpetrators. As stated by Holtzworth-Munroe, Meehan, Herron, Rehman, and Stuart (2000), the understanding of IPV is more likely to advance by looking at differences between perpetrators rather than studying them as a single group. In addition, Andrews, Bonta, and Wormith (2006) and Saunders (2001) argued that treatment types that are matched to perpetrator characteristics are much more effective in reducing the propensity to reoffend than one-size-fits-all models. This shows that typology research also has important clinical implications because it opens up the possibility to match treatment to the type of batterer.
The batterer typology that has been replicated was originally reported by Holtzworth-Munroe and Stuart (1994) who deduced a model based on the most common findings in the batterer typology literature. This model differentiated types of batterers based on three dimensions: (a) severity of IPV, (b) generality of violence, and (c) psychopathology. They predicted the existence of three types of batterers. The first batterer group is the Family-Only (FO) subtype, which was predicted to commit the least violence, both domestically and publicly, and whose members have few if any psychopathological problems; in their case, violence erupts due to a combination of low-level risk factors and major stressors. The second group, Borderline-Dysphoric (BD), engages in severe partner violence but low to moderate general violence. Due to high levels of psychological distress and an inability to maintain stable relationships resulting from their borderline PD characteristics, they engage in severe violence against their partner. Finally, the last group was called the Generally Violent Antisocial (GVA) subtype who commit both severe partner violence and severe general violence. For them, violence at home is part of a larger general pattern of violence. When Holtzworth-Munroe et al. (2000) empirically tested their theoretical model, they identified not only the three subtypes as they predicted but also observed a fourth type, which they called Low-Level Antisocial (LLA); it fell between the FO and GVA subtypes on most measures. In a longitudinal follow-up study (1.5 and 3 years), Holtzworth-Munroe, Meehan, Herron, Rehman, and Stuart (2003) found that the typologies continued to differ from each other on most risk factors. The only exception was that the BD and GVA groups showed some overlap on measures related to antisociality, but the nonsignificant differences could possibly have been the result of their small sample size. They also discovered that FO batterers were most likely to desist from further violence, while GVA batterers were most likely to continue being violent to their partners; this could suggest that violence does not necessarily escalate or that all batterers engage in structural forms of violence.
In the current study, Holtzworth-Munroe and Stuart’s (1994) model has been replicated on a clinical sample of men who were in outpatient treatment for IPV and aggression regulation. Clinical samples are more likely to contain larger numbers of antisocial batterers because of court-ordered treatment; many nonantisocial batterers stay unnoticed by the law (Holtzworth-Munroe et al., 2000). However, this sample did contain batterers who were in treatment either voluntarily or mandatorily, which is why the other types could likely be discerned as well. As in previous studies, the typology has been based on the three dimensions found in the original model.
Structural and Incidental Violence
Previous batterer typologies have either based their subtypes on IPV data from the 12 months before the study, or have not made clear distinctions between violence in the recent and distant past (e.g., Delsol et al., 2003; Holtzworth-Munroe et al., 2000; Huss & Ralston, 2008). In the present study, a distinction has been made between violence in the recent past (last 12 months) and the distant past (years before the last 12 months). This could not only provide a more complete picture of a batterer’s violent tendencies, but it also opens up the possibility to distinguish structural from incidental batterers, which could aid the process of identifying important risk factors that predict IPV. Incidentally violent batterers have been conceptualized as men who commit IPV occasionally but who otherwise have generally peaceful relationships, while structural batterers were conceptualized as men who have a long history of IPV. Notably, chronically violent offenders (structural batterers) are more likely to reoffend and less likely to respond to intervention (Buzawa & Buzawa, 2013) which is why it is important to make this distinction. Furthermore, Holtzworth-Munroe et al. (2003) uncovered that batterers who did not have a history of IPV (incidental batterers) were more likely to stop being violent. This implies that greater emphasis should be placed on identifying and supervising batterers who commit structural IPV. Because previous studies have found that FO batterers were the least likely to have a history of IPV, and because FO batterers have the fewest psychological problems (Holtzworth-Munroe et al., 2003; Thijssen & De Ruiter, 2010), we expected to find that FO batterers followed a pattern of incidental violence. In their case, the violence could be the result of major life stressors such as very unhealthy relationships or the sudden loss of employment. At the same time, we expected that the high-risk patients (BD and GVA batterers) would follow structural patterns of violence as these subtypes are known to have a longer history of IPV and a greater likelihood of reoffending, which could be explained by their severe psychological problems (Holtzworth-Munroe et al., 2003; Thijssen & De Ruiter, 2010).
Variations in PDs
The PDs of the batterer subtypes were compared to investigate whether they differed in the predicted directions. This is especially salient as PDs other than Antisocial and Borderline have been found to occur in the batterers’ population. For example, Johnson et al. (2006) encountered a group of batterers mostly exhibiting traits of narcissistic PD. Furthermore, several studies have been unable to distinguish a group of batterers with clear indications of borderline PD (e.g., Cunha & Goncalves, 2013; Fowler & Westen, 2011; Thijssen & De Ruiter, 2010). However, they did distinguish a group who resembled the BD subtype on the other descriptive dimensions. This study has used clinical diagnoses for borderline, antisocial, and narcissistic PDs according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000), similarly to Waltz, Babcock, Jacobson, and Gottman (2000). We also included other PDs such as PD–Not Otherwise Specified (PD-NOS). This allowed for the possibility to include indications of severe problems in the personality structure that cannot be clearly categorized in one of the other PDs.
Allocation to Treatment
Effectively treating batterers has been found to be notoriously difficult. For example, Babcock, Green, and Robic (2004) discovered only a 5% difference in recidivism rates between treated and nontreated batterers. Furthermore, it has not been confirmed that one treatment model performs better than other models (Babcock et al., 2004; Sartin, Hansen, & Huss, 2006). However, significant individual differences concerning treatment effectiveness have been found. For instance, Saunders (1996) discovered that men with dependent personalities performed better in process-psychodynamic groups, while antisocial batterers had better outcomes when assigned to cognitive-behavioral therapy.
Increasingly, clinicians have become aware of the importance of taking into account individual differences between offenders. One emerging approach is the use of the risk, need, and responsivity (RNR) principles, which have been found to be effective in reducing recidivism (Andrews et al., 2006). This approach states that treatment intensity should be based on the risk levels of the patient (Risk), treatment should be focused on the most problematic criminogenic factors (Need), and the treatment method should be matched to the characteristics of the patient (Responsivity). Batterer typologies could assist in identifying the risk and need factors of batterers to properly match treatment to the individual. Two studies (Eckhardt, Holtzworth-Munroe, Norlander, Sibley, & Cahill, 2008; Huss & Ralston, 2008) have looked at treatment effectiveness for batterer subtypes undergoing the same intervention, and both reported that the GVA and BD batterers were more likely to drop out early or to reoffend after treatment. Holtzworth-Munroe and Meehan (2004) examined the batterer treatment literature and proposed that FO and LLA batterers were probably most likely to benefit from existing batterer interventions. GVA batterers, however, might be more receptive to structured cognitive-behavioral therapy or rehabilitation supervision, while BD batterers could possibly mostly benefit from cognitive-behavioral therapy focused on emotional regulation. Because the batterer subtypes were not explicitly used by the clinicians in this study, it is of interest to investigate whether the clinicians nonetheless allocated the most appropriate type of the treatment to the different types of IPV perpetrators. This is especially important because there is some debate about the extent to which batterer types can be qualitatively recognized by clinicians (Langhinrichsen-Rohling, Huss, & Ramsey, 2000; Sartin et al., 2006).
In summary, the aim of this study was to replicate Holtzworth-Munroe andStuart’s (1994) model using a Dutch clinical sample. Unlike previous replications, this study made an explicit distinction between violence committed in the distant past versus the recent past. As a result, we were able to distinguish incidental batterers (those with limited history of IPV) from structural batterers (men with a longer history of IPV). Specifically, it was expected that low-risk patients (FO and LLA batterers) would be more likely to display incidental IPV, while high-risk patients (GVA and BD batters) commit more structural IPV. Aside from the characteristics of the patients, we studied differences in treatment allocation between the batterer subtypes to see whether clinicians placed the batterer subtypes in different treatment types without prior awareness of batterer subtypes.
Method
Design
This study is part of an ongoing longitudinal multisite research into the Dutch version of the Level of Service/Case Management Inventory (LS/CMI; Andrews, Bonta, & Wormith, 2004) and its use in forensic psychiatric outpatient treatment in the Netherlands. In this study, patients from three different sites participated, and only male patients who were treated for IPV or other forms of aggression were included. During the admission interview at the facility, patients were asked by the clinician if they consented to their clinical and judicial information being used for the study. If they agreed, they signed an informed consent form. Data for this study were gathered between 2012 and 2015.
Setting
The study was conducted at three forensic psychiatric outpatient facilities located in Arnhem, Den Bosch, and Nijmegen, the Netherlands. These cities are relatively large (>150,000 inhabitants) for Dutch standards. All three facilities offer a range of therapies, including a group-based batterer intervention program and other types of treatments for batterers (Ministerie van Volksgezondheid, Welzijn en Sport [MVWS], 2013).
Participants
A total of 110 patients were included in this study, all of whom had committed at least one act of physical IPV, either recently or in the past, and who were in treatment for problems related to IPV or other forms of violent delinquent behavior. Patients could be assigned to forensic outpatient treatment either due to a judicial measure, after being convicted of an offense (mandatory), or by general or psychiatric health care, when there is a risk of the patient becoming violent or when the patient has been violent but has not been accused legally (voluntary). Thirty-four patients (30.9%) were in treatment mandatorily, while 76 (69.1%) patients went voluntarily into treatment.
Instruments
The first instrument that was used in this study was the LS/CMI (Andrews et al., 2004). Based on the RNR principles (Andrews et al., 2006), Section 1 of the LS/CMI assesses eight important domains (“The Central Eight”), which have empirical support concerning their predictive power regarding offending. The eight domains consist of Criminal History, Education/Employment, Family/Relationships, Leisure Time, Companions, Alcohol/Drugs Problems, Procriminal Attitude, and Antisocial Pattern. Some of the items represent dynamic risk factors (e.g., current substance abuse problems), while others relate to static risk factors (e.g., being arrested before the age of 16). This allows for the possibility to calculate a score which measures a patient’s total risk level (range = 0-43) or their risk level on each of the eight domains. The interrater reliability of the Dutch version of the LSI-r (Andrews & Bonta, 1995; the predecessor of and largely comparable to Section 1 of the LS/CMI) was found to be good (intraclass correlation [ICC] = .87; De Rooy, 2004).
The second instrument that was used is the Brief Spousal Assault Form for the Evaluation of Risk (B-SAFER; Kropp et al., 2005), which has also been used to identify Holtzworth-Munroe and Stuart’s (1994) typology before (Thijssen & De Ruiter, 2010). The B-SAFER is a structured risk assessment guide intended to estimate the risk levels of IPV perpetrators (Thijssen & De Ruiter, 2010). Each of the 15 items was scored using information in the patient files, such as indications of severely violent acts, severely violent thoughts/threats, escalation of violence, or the presence of mental health problems. Each item is coded as “N” for not present, “?” for partially or possibly present, and “Y” for clearly present. Furthermore, all items have been coded twice: once for the last 12 months and once for all the years preceding the last 12 months. When scoring parts of the B-SAFER on a different Dutch sample, Thijssen and De Ruiter (2010) found the interrater reliability to be satisfactory.
Procedure
The LS/CMI forms were completed by professional clinicians who partook in a 2-day training in the administration of this instrument. The LS/CMI was coded based on semistructured interviews and information in the patient’s files. The clinicians filled in the LS/CMI during different moments of time, once during the admission interview, and one or more times during or at the end of the treatment. The B-SAFER data were scored for all patients by the first author using all the relevant documents in the patient files, which included admission interview reports, official police reports, interviews with partners or family members, and psychological assessments.
Prior to data analyses, the data were checked for missing values and other inconsistencies. The B-SAFER items severity of physical violence and severity of psychological violence contained a total of three missing values that could not be scored due to missing or unreliable information. To maintain statistical power, these values were replaced by estimates using multiple imputations, with the variables used to create the dimensions and other variables (such as criminal attitude and association with deviant peers) as the reference points by which the missing values were estimated.
Operationalization
Descriptive dimensions used to create the typology
To create the typology, the three descriptive dimensions outlined by Holtzworth-Munroe et al. (2000) were measured. The first dimension, severity of violence, was operationalized using the first two items of the B-SAFER. These items measured whether there were indications of severe physical violence (defined as violence which caused actual injury; Item 1) and whether there were indications of severely violent thoughts or threats (not including impulsive expressions; Item 2). Both items were scored twice; once for the past 12 months (recent past) and once for all the years preceding the past 12 months (distant past). The second dimension, generality of violence, was constructed using the Criminal History section of the LS/CMI, which contains eight static and dynamic items measuring several aspects of delinquency. Finally, the third dimension, psychopathology, was measured twice using the Alcohol/Drugs problems and the Antisocial Pattern domains of the LS/CMI.
Extra-familial violence and PDs
A second measurement of Generality of Violence was included by using an item on the LS/CMI that dichotomously measures whether the patient committed violence to an adult nonfamily member or not. This item was not used to create the typology because the cluster analyses we used are not equipped to handle dichotomous variables. PDs were also coded as binary variables which indicated whether the patient received a diagnosis for the relevant disorder or not. This information was taken from the patient files. These diagnoses have been made by eligible clinicians, in accordance with DSM-IV-TR criteria.
Treatment types
The information concerning (suggested) allocation to a treatment type was extracted from the patient files. Based on the admission interview forms, the suggestions of the clinicians regarding the treatment could be collected. These suggestions were coded as binary variables, with (1) indicating that they were assigned the treatment type and (0) indicating that they were not. The first two treatment types were domestic violence treatment “Stop Huiselijk Geweld” (SHG) and aggression replacement training (ART), both of which are based on cognitive-behavioral therapy and mostly take place in group settings although it is also possible to receive individualized therapy. The difference between these two treatment types is that SHG is focused specifically on preventing further domestic violence, while ART focuses on general aggression. The third treatment type was psycho-motor therapy, which is a type of expressive therapy. Fourth, psychosocial supervision (PSS) was included where patients receive individualized treatment to help them cope with major life problems. Fifth was mentalization-based therapy (MBT), which is a type of psychodynamic psychotherapy stemming from attachment theory. Finally, couple’s therapy in which both partners are invited to take part in systematic therapy (a type of psychotherapy) was examined. There were also some other therapies that were included, such as psychiatric treatment and drama therapy, although only very few patients were allocated to these treatments.
Patients could be assigned to several treatment types at the same time. For two patients, no information was found regarding their assigned treatment, and they were therefore removed from the analyses where treatment types were compared. We also measured whether the patients entered treatment mandatorily or voluntarily. Finally, we measured some demographic characteristics, including age and ethnicity.
Analyses
To create the typology, cluster analysis was used, which is a statistical technique where individuals are classified into relatively homogeneous groups (Holtzworth-Munroe et al., 2000). Ward’s (1963) hierarchical cluster analysis was chosen, because it has been found to perform better than most cluster analyses when attempting to provide a solution based on a minimal within-cluster variation (Cunha & Goncalves, 2013; Huss & Ralston, 2008). The measurements of the severity of psychological violence for the recent past and distant past were entered as a single scale in the cluster analyses (Cronbach’s alpha = .723), but the items for physical violence were entered separately as they revealed a low correlation (r = .19; Cronbach’s alpha = .037). The other three dimensions had an extremely high alpha and thus were entered as a whole. 1 Prior to conducting the cluster analyses, all variables included in the cluster analyses had been transformed into z scores to nullify the impact of different measurement ranges.
Two sets of variables measuring the descriptive dimensions were used to produce the clusters. This was done because criminal history and antisocial patterns correlated very highly (r = .709; p = .000), and variables with a correlation higher than .50 can skew the F score, resulting in a disproportional weight in creating the clusters (Sambandam, 2003). The first set of variables included all dimensions except for antisocial pattern, while the second set included all dimensions except for criminal history.
In line with the previous batterer typology literature, four criteria were used to determine the optimal cluster solution (Holtzworth-Munroe et al., 2000; Huss & Langhinrichsen-Rohling, 2006; Huss & Ralston, 2008). These four criteria were as follows: (a) a careful consideration of the literature, (b) an inspection of the dendrogram, (c) a plot of the change of agglomeration coefficient between steps, and (d) additional k-means cluster analysis techniques used to validate the original findings. Regarding this last criterion, the cluster centers produced by Ward’s method were entered as seeds in the k-means cluster analyses, setting the solution for two, three, four, and five clusters. The batterers’ placement in a cluster by both Ward’s and k-means was then compared to see which solution best fitted the data for both sets of variables. Final cluster membership was determined by placing the batterers in the cluster where they were placed most often by all four analyses. The clusters that were created were then compared using one-way ANOVAs with post hoc Bonferroni tests to investigate group differences on the descriptive dimensions. To test differences in PD diagnoses and extra-familial violence, we compared the batterers using chi-square tests. The differences in treatment types were also analyzed using chi-square analyses.
Results
Patient Characteristics
The mean age of the patients was 37.4 years (min = 18, max = 56, SD = 9.48). Of the 110 participants, 21 (19.1%) were married, 32 (29.1%) were living together, 20 (18.2%) were in a relationship but not living together, 26 (23.6%) were separated but still involved with their ex-partners, four (3.6%) were involved in a new relationship, and seven (6.3%) were not actively involved in a relationship. The vast majority of the sample were ethnically Dutch (84 participants, 76.4%); the other patients came from a wide variety of ethnic backgrounds. Regarding the level of education, two (1.8%) had no diploma, 19 (17.3%) had only a primary education degree, 48 (43.6%) had finished secondary education, and 36 (32.8%) had acquired a tertiary degree. For five patients, their level of education was unknown.
Cluster Analyses and Batterer Subtypes
Based on the criteria mentioned before, it was determined that all four different forms of cluster analyses yielded a four-cluster solution. The first set of variables placed the most patients (98) in the same cluster for the two- and four-cluster solution. Comparing the second set of variables resulted in the most patients (103) also being placed in the four-cluster solution. Based on the cluster analyses, we concluded that the four-cluster solution best fitted the data.
When determining final cluster membership, only 81 batterers could be placed in a cluster through a comparison of cluster placement by the four analyses. For the remaining 29 batterers, it was decided to place them into the cluster as determined by Ward’s cluster analysis using the first set of variables (where antisocial pattern was excluded). This was done because, first of all, the first set used a measure of general violence (criminal history) while the second set did not. Second, Ward’s method had previously been found to be more reliable than k-means analysis (Holtzworth-Munroe et al., 2000; Huss & Ralston, 2008). In the end, 35 batterers were placed in the FO group, 21 in the BD group, 30 in the GVA group, and 24 in the LLA group. This confirmed the expectations that all groups could be classified but that more antisocial batterers would be identified.
Group differences in the descriptive dimensions
The subgroups mostly differed along the lines of the model proposed by Holtzworth-Munroe and Stuart (1994; see Table 1). Interestingly, FO batterers scored highly on physical IPV for the recent past (previous 12 months), whereas LLA batterers scored very low. When comparing the scores of the physical IPV for the distant past (the years before the previous 12 months), FO batterers scored the lowest while LLA batterers scored second highest. GVA and BD batterers showed a more stable pattern of physical IPV. All the batterers did reveal a more consistent pattern of psychological violence where FO batterers consistently scored the lowest, and BD batterers scored consistently the highest. Thus, from these results it can be observed that some of the batterers tended to fluctuate in their level of violence. Regarding general violence and psychopathological measures, all the batterers scored in the predicted directions. Our analyses on extra-familial violence revealed that FO batterers were the least likely to have committed violence toward a nonfamily member (22.8%), followed by BD (47.6%), LLA (70.8%), and GVA batterers (80.0%); χ2(3, N = 110) = 24.88, p = .00.
ANOVAs on Descriptive Dimensions Used in Cluster Analysis—Descriptive Dimensions in Typology: Group Means, Standard Deviations, and Significant Group Differences.

Note. Subscript denotes significant group difference after Bonferroni correction (p < .05); a = FO; b = DB; c = GVA; d = LLA. FO = Family-Only; BD = Borderline-Dysphoric; GVA = Generally Violent Antisocial; LLA = Low-Level Antisocial.
p < .01.
Batterer types and PDs
FO batterers showed relatively few PDs, while GVA and LLA batterers had received mostly antisocial diagnoses (see Table 2). However, the diagnoses revealed different results for BD batterers. While they did have the most borderline diagnoses, they also scored high on narcissistic and NOS diagnoses.
Chi-Square Tests Comparing Personality Disorder Diagnoses—Personality Disorder Diagnoses: Number of Patients, Percentages, and Significant Group Differences.
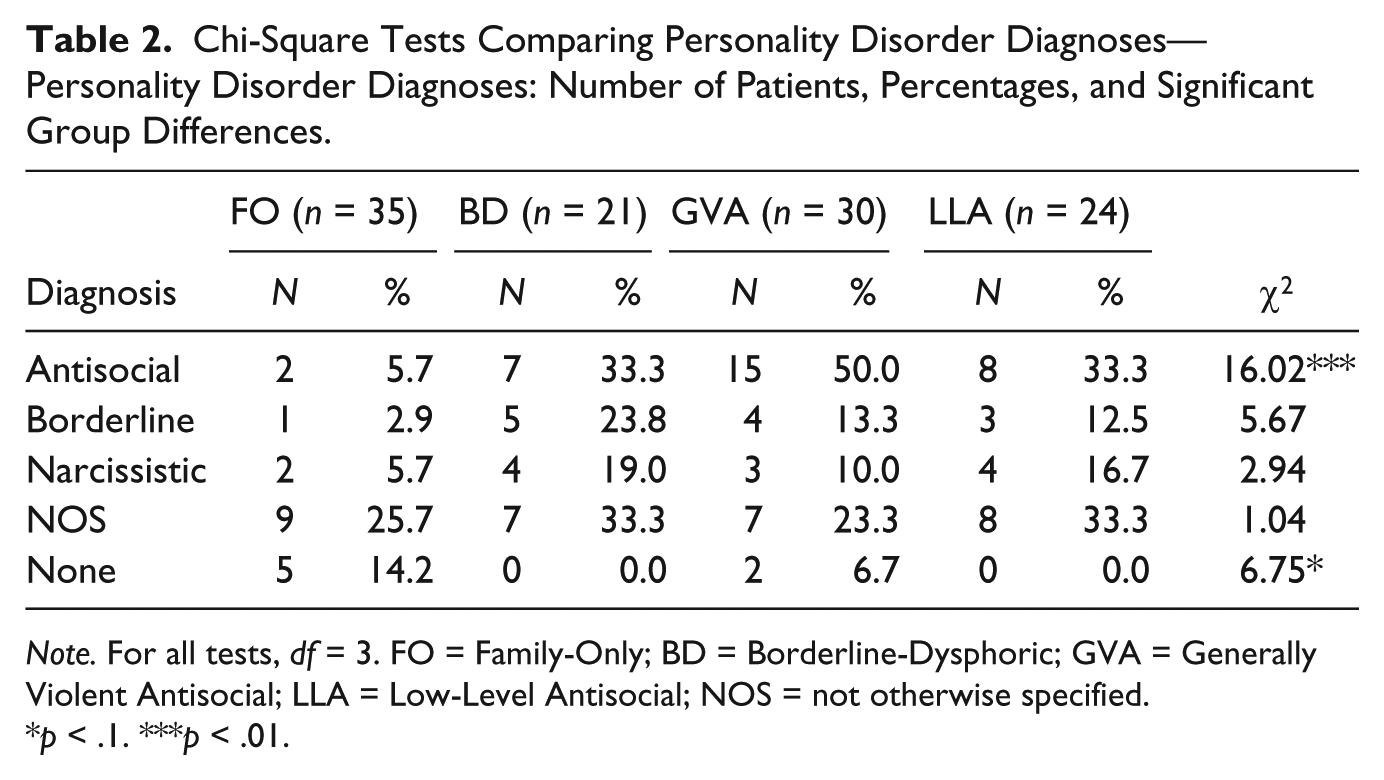
Note. For all tests, df = 3. FO = Family-Only; BD = Borderline-Dysphoric; GVA = Generally Violent Antisocial; LLA = Low-Level Antisocial; NOS = not otherwise specified.
p < .1. ***p < .01.
Batterer types and sample characteristics
On the sample characteristics, the batterer types did not reveal any significant differences. The only exception was legal framework: BD batterers were most likely to enter treatment mandatorily (47.6%), followed by GVA (43.3%), LLA (25%), and FO (14.3%) batterers; χ2 (3, N = 110) = 9.84, p = .02.
Group Differences in Treatment Allocation
In Table 3, the distribution of the treatment types between the batterer types can be observed. As the findings show, there are some differences between the subtypes. Most FO batterers were assigned to the group-based domestic violence therapy (SHG), while the LLA batterers were the least likely to be assigned to this group although the chi-square value almost failed to reach conventional statistical significance (p = .054). There are significant differences in the ART group: The two antisocial subtypes (GVA and LLA) were most likely to be assigned to these therapies (p = .030). The same can be said about the PSS group where the antisocial subtypes were also in the majority although the difference did not amount to conventional statistical significance (p = .081). All the other treatment types did not reveal any significant differences between the subtypes. We also analyzed five more treatment types not shown in the table (psychiatric consultation, individual psychotherapy, therapy aimed at patients with intellectual disability, posttraumatic therapy, and relapse prevention therapy). None of these reached statistical significance, but this might be due to the very small number of patients assigned to these therapies. No significant differences were found in the amount of treatment types the batterers were assigned to.
Chi-Square Tests Comparing Treatment Types and Batterer Subtypes—Treatment Types: Number of Patients, Percentages, and Significant Group Differences.

Note. For all tests, df = 3. FO = Family-Only; DB = Borderline-Dysphoric; GVA = Generally Violent Antisocial; LLA = Low-Level Antisocial; SHG = group-based domestic violence treatment; ART = aggression replacement training; PMT = psycho-motor therapy; PSS = psychosocial supervision; MBT = mentalization-based therapy; PRT = partner relationship therapy.
p < .1. **p < .05.
Discussion
This study replicated a batterer typology originally reported by Holtzworth-Munroe and Stuart (1994) using a Dutch sample of forensic psychiatric outpatients. Unlike previous replications of this typology, physical violence for the recent and distant past was included separately. The results showed that in the recent past FO, BD, and GVA batterers hardly differed in their levels of physical partner violence, but that LLA batterers revealed very low levels. However, for the distant past, FO batterers committed less physical partner violence, whereas LLA batterers displayed higher levels of violence. BD and GVA batterers revealed a more stable pattern of physical violence in the sense that there was not much difference between the severity of physical violence in the recent and distant past. This supported our expectations that BD and GVA batterers engage in physical violence structurally, while FO and LLA batterers are only incidentally physically violent to their partners. On the other dimensions, the batterer types differed in the expected manners, with the exception of PDs where a clear borderline group could not be distinguished. The analyses of the different treatment types revealed that there were differences in the domestic violence therapy, PSS, and ART although only the latter reached conventional statistical significance.
The results of the cluster analyses showed that it is important to consider the physical violence of an entire batterer’s life because it allows for the possibility to differentiate between batterers who commit incidental and structural violence. Only measuring the physical violence in the recent past might skew the findings as a result. Moreover, our findings suggest that it is important to examine violence over time and to investigate what factors contribute to increasing or decreasing levels of IPV. As Capaldi and Kim (2007) have stated, it might be important not only to study the perpetrator but also to explore the characteristics of the partner in a dyadic model. Fluctuations in violence could also be accounted for by distinguishing between impulsive and premeditated batterers (Stanford, Houston, & Baldridge, 2008). Chase, O’Leary, and Heyman (2001) also suggested that the Holtzworth-Munroe and Stuart typology might be more useful if framed in such a bimodal classification. It might seem surprising that FO batterers scored very high on physical IPV in the recent past while LLA batterers scored very low, but there are a number of possible explanations for this. First, given their low rates of general violence, FO batterers might enter treatment specifically for IPV, which would be expected to have escalated recently. LLA batterers, however, might be in treatment for general aggression, and thus their level of physical IPV might happen to be low. Second, LLA batterers seemed to display a lot of psychological aggression which is not measured by the B-SAFER (such as cursing, yelling, and throwing with objects). Perhaps if such verbal and nonverbal forms of aggression were taken into account a different picture would arise.
The results from comparing the PDs revealed an interesting picture. In line with the original model, GVA batterers showed the highest number of diagnoses of antisocial PD, and FO batterers revealed relatively few disorders. The BD group scored the highest on borderline diagnoses, but they also scored the highest on diagnoses for narcissistic PD. Thus, while this group clearly possessed psychological problems, it could not be concluded that they are distinctly batterers showing borderline characteristics (see also Cunha & Goncalves, 2013; Thijssen & De Ruiter, 2010). The same can be said for LLA batters; they did have a very high number of antisocial diagnoses but there was also a large amount of diagnoses of narcissistic PD and PD-NOS. One explanation for these findings is that the original model as proposed by Holtzworth-Munroe and Stuart (1994) is too limited on its psychopathological dimension to fully explain the heterogeneity in the batterer population. If this model is to be used to explain the variety in IPV perpetrators, both theoretically and clinically, the variations in PDs should be more carefully investigated because different PDs often require different treatment types. Moreover, there is some debate about the clinical usefulness of batterer typologies (Sartin et al., 2006). As Holtzworth-Munroe and colleagues (2000) pointed out as well, it is important to investigate whether a 2 × 2 model (Antisocial × Borderline characteristics) is a fruitful approach to batterer typologies. One possibility is that a more dimensional approach to personality might assist in identifying the different types of personality of IPV perpetrators, instead of using a categorical approach (Leibing, Jamrozinski, Vromfelde, Stahl, & Doering, 2008; Livesley, 2007). For example, Widiger and Mullins-Sweatt (2004) argued that a possible extension could be to include the five-factor model of general personality functioning, which could help provide a more specific description of the differences between the batterers. Furthermore, not all patients could be reliably placed in the used subtypes which might be caused by the limited number of dimensions on which these types are based and a reduction of reality caused by the use of subtypes instead of a dimensional approach of IPV behavior (see also Ross & Babcock, 2010). A consequence might be that treatment is not personalized and therefore not as effective as possible.
The findings on the treatment types revealed that clinicians were apparently more likely to believe that therapy which focuses on regulation aggression (ART) would be more suitable to the antisocial subtypes. However, the clinicians indicated that the less antisocial types (FO and BD) would be more likely to benefit from the group-based domestic violence therapy. However, these differences were not substantial which might mean that this batterer typology does not always correspond to the judgment of the clinicians. One example of note is the MBT, which was originally designed with borderline PD patients in mind, but the results of this study revealed that none of the BD groups were assigned to this therapy. As the subtypes have been found to be predictive of future violence, perhaps more effort should be made to introduce such classifications to clinicians to optimize the needs of the patients to the therapies available.
Limitations and Future Research
There are several limitations to this research, which should be mentioned. First, most of the data on the severity of violence were based on self-reported descriptions, which is known to be biased toward revealing less violence than actually occurred (Holtzworth-Munroe et al., 2000). Second, the operationalization of these data was also limited in the sense that not all types of violence, such as yelling or throwing with objects, were taken into account. Furthermore, borderline personality traits as used in the original model could not accurately be measured. Although we did not have measures to clearly operationalize borderline traits, the BD subtype we encountered did largely correspond with most of the descriptive dimensions found by Holtzworth-Munroe et al. (2000). However, using validated measures for assessing personality is recommended. Moreover, the sample size was relatively small, especially when comparing subgroups. Future researchers should employ larger samples to promote generalizability. Furthermore, although this study was conducted on a Dutch sample, adding measures of distal and recent violence may strengthen the insight into the typologies in other settings. However, the findings regarding treatment allocation might not be comparable with other countries and jurisdictions. Dutch forensic outpatient facilities generally follow the national guidelines in this respect, and this might not be comparable with guidelines in other countries. Many of the included forensic outpatients did not follow treatment mandatorily but were referred by general practitioners or general psychiatric services. This might lead to a typical population, compared with patients who are in forensic treatment in other countries. Especially, motivation to enter and stay in treatment may differ. However, voluntary treatment for IPV perpetrators can be conditional. For instance, in some cases, patients are forced to follow treatment under the pressure of a partner who threatens to press charges unless the patient enters treatment. In this study, treatment motivation was not examined and could have guided treatment allocation.
This study has elaborated on the existing literature. First of all, by basing the typology on violence committed throughout the entire patient’s life, it came to light that for the recent past the level of physical violence of the batterers differed in surprising ways. The level of physical violence committed by FO batterers hardly differed from GVA and BD batterers, even though they theoretically should display less physical violence. This means that it is important to take into account the entire history of violence lest typology-based research is skewed by momentary escalations in IPV. Second, this research demonstrated that there were discrepancies between the judgment of trained clinicians and statistically derived subtypes. If batterer subtypes should ever be introduced into clinical settings, it is imperative to synthesize empirical subtypes and qualitative clinical judgment.
Future research should continue to investigate differences between batterers using subtypes. As it was uncovered that some batterers committed incidental forms of IPV, it should be investigated why these men suddenly engaged in violence. Instead of a social learning approach on which the model reported by Holtzworth-Munroe and Stuart (1994) is based, their behavior could possibly be explained through a life event or stress theory framework (Fox, Benson, DeMaris, & Van Wyk, 2002). More attention should also be paid to studying the effectiveness of batterer treatment using a typology framework. It is important to study which type of treatment works best for which type of batterer because this could open up the possibility to develop specialized treatment programs that cater to the specific needs of the patient and might therefore reduce recidivism.
Footnotes
Acknowledgements
First, we would like to thank all the patients who gave permission to use their data for this study. Next, our gratitude goes out to the students who have been involved in this project, mainly for data gathering. Finally, we would also like to thank Jochem Tolsma for his valuable comments regarding this publication and the Master thesis on which this is partly based.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.