
Abstract
Domestic violence (DV) against women is a serious problem with its negative effects on all family members and the society. Women exposed to DV not only have physical but also psychological damage. This study investigates prevalence of DV and its relations with some descriptive and clinical features in a psychiatric outpatient population in Turkey. A total of 277 female outpatients were included in the study. After a semistructured clinical interview, they were assessed by sociodemographic data form, DV questionnaire, Hamilton Depression Rating Scale (HDRS), Hamilton Anxiety Rating Scale (HARS), Dissociative Experiences Scale (DES), and Somatoform Dissociation Questionnaire (SDQ). Prevalence of exposure to DV by intimate partner is found to be 58.8% (n = 163). The current study provided strong evidence that occupation status of the woman, education level of the partner, and family type are predictors of DV. Another predictor of DV exists where the child is battered by either parent. Prevalence of depression, conversion disorder, and other somatoform disorders are higher in women exposed to DV. These women also have higher scores from HDRS, HARS, DES, and SDQ compared with female patients who have not experienced DV (p < .001). Number of women scoring above cutoff levels for DES and SDQ were significantly higher in women exposed to DV (p < .001).
Introduction
Definition and Epidemiology of Domestic Violence (DV)
The United Nations defines violence against women as any act of gender-based violence that results in, or is likely to result in, physical, sexual or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life.
According to the definition of World Health Organization (WHO), intimate partner violence refers to behavior by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse, and controlling behaviors (WHO, 2016). Michael P. Johnson defines four major types of intimate partner violence; one of which is termed as intimate terrorism. It is defined as coercive controlling violence which occurs when one partner in a relationship uses coercive control and power over the other partner, using threats, intimidation, and isolation. Intimate terrorism may involve sexual, sadistic control, economic, physical, emotional, and psychological abuse; thus resembles the WHO definition of intimate partner violence (Johnson & Ferraro, 2000). In the present study, we principally use WHO definition of intimate partner violence.
DV against women is an important public health problem in the world and in our country. According to the results of research from 15 different regions, WHO reported that the lifetime prevalence of physical violence against women from their spouses or intimate partners is between 13% and 61%. Physical and/or sexual violence varies between 15% and 71% (Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). In a research about violence against women conducted in 2013 in 28 European Union countries, prevalence of physical or sexual violence against women from their spouses or intimate partners varied between 13% and 32% with a mean of 22% (European Union Agency for Fundamental Rights [FRA], 2014).
In a research about DV against women in Turkey conducted by Hacettepe University (Directorate General on the Status of Women [DGSW], 2014), 36% of married women reported that they were exposed to physical violence from their intimate partners at least once in their lifetime. It was reported that 12% of women were exposed to sexual violence, 44% were exposed to emotional abuse such as threatening, insult, and swearing, and 30% were exposed to financial abuse. Sociodemographic features such as marital age, education level, and residence were found to be related with the prevalence of violence. The research suggested a significant association between DV and some physical and psychiatric symptoms of women. Experiencing or witnessing violence in childhood, low income level, low education level, lack of social support, male-dominated cultural and religious features, alcohol use, and presence of psychopathology are among the risk factors for DV (Page & Ince, 2008).
DV and Psychopathology
DV is an important correlate for psychiatric morbidity (Stephenson, Winter, & Hindin, 2013). Among the most frequently reported psychological consequences are depression (Scholle, Rost, & Golding, 1998), high suicide risk (Olson et al., 1999), anxiety, somatic symptoms, posttraumatic stress disorder (Astin, Lawrence, & Foy, 1993), and dissociative symptoms (Iverson et al., 2013). Disorders of psychosomatic origin such as somatization disorder, hypochondriasis, pain disorder, and conversion disorder are also common in abused women (Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008; Ozyurt, & Deveci, 2011). The negative impact of violence is not only limited to the abused one but also transferred from generation to generation. Children who grow up in families with intimate partner violence may suffer from behavioral and emotional disturbances that can be associated with the perpetration or experiencing of violence later in life. Experiencing or witnessing violence in childhood is an important reason for psychiatric morbidity (Flaherty et al., 2006; Vahip, & Doganavsargil, 2006).
According to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000), dissociation is generally viewed as a disruption in the usually integrated functions of consciousness, memory, identity, and perception of the environment. Somatoform functions and reactions could also be results of dissociation. They are manifested in a loss of the normal integration of somatoform components of experience, bodily reactions, and functions, and are termed somatoform dissociation. Psychological dissociative symptoms are those that phenomenologically involve psychological variables, and somatoform dissociation designates dissociative symptoms involving the body (Nijenhuis, 2000).
Somatization is accepted as culture specific expression of distress, which serves to normalize experience of distress (Kirmayer, Da, & Smith, 1998). In certain cultures, such as the Turkish culture, there may be a stigma against psychological disorders. However, bodily symptoms of distress are accepted by the society. Therefore, bodily symptoms, such as a lump in the throat and back pain, serve as a way of expressing distress (Cinarbas, 2014). Gureje, Simon, Ustun, and Goldberg (1997) examined the prevalence of somatization and other psychological disorders in 14 different countries, including Turkey and the United States, and found out that 25.2% of patients from Turkey had a somatization disorder compared with 9.8% of patients from the United States. Ulusahin, Basoglu, and Paykel (1994) reported that Turkish patients had higher scores for somatic symptoms of depression compared with their British counterparts, who had higher scores for psychological complaints such as guilt and pessimism.
Among all psychiatric disorders, dissociative disorders are the ones mostly dependent on environmental factors such as trauma (Sar, 2008). There is an established association between dissociative phenomena and the existence of traumatic events in the person’s life (Spiegel, 2006) However, there are limited data reporting an increase in dissociative symptoms in victims of DV (Kaymaz, Ozturk, & Bagcioglu, 2014).
Although psychiatric service users are found to report a higher prevalence of DV, it still remains largely undetected by mental health services worldwide, with between 10% and 30% of cases documented in case notes (Howard et al., 2010). The relationship between mental health issues and violence against women is complex. DV is a risk factor for developing a mental illness and having a mental illness increases vulnerability to physical and sexual violence. Thus, awareness and understanding of family violence among mental health care professionals is crucial (Akyuz, Kugu, Dogan, & Ozdemir, 2002).
Present Study
In the present study, we will use three types of measures which have been linked to DV in studies of other samples. The first of these is the demographic data. Sociodemographic variables known to be related with DV such as education, occupation, income (Kocacik & Dogan, 2006), family type, marital age, marriage pattern (DGSW, 2014) are investigated with sociodemographic data form prepared by the researchers.
The second measure is the results of the clinical interview as measured by the Structured Clinical Interview for DSM-IV (SCID-1) (First, Spitzer, Gibbon, & Williams,1997). In the Turkish validity and reliability study, Ozkurkcugil, Aydemir, Yıldız, Danacı, and Koroglu (1999) reported reliability among interviewers with kappa coefficient of 0.52 to 1.00. Consonance rate for all diagnoses was reported as 98.1% with kappa coefficient of 0.86.
The third measure is the clinical scales. Depression (Scholle et al., 1998), anxiety (Astin et al., 1993), dissociative thoughts and behaviors (Iverson et al., 2013), and symptoms of somatoform behaviors (Ozyurt, & Deveci, 2011) are some of the important variables that have been associated with DV victimization. In the present study, these variables will be measured by Hamilton Depression Rating Scale (HDRS; Hamilton, 1960), Hamilton Anxiety Rating Scale (HARS; Hamilton, 1959), Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), and Somatoform Dissociation Questionnaire (SDQ; Nijenhuis, Spinhoven, Van Dyck, Van der Hart, & Vanderlinden, 1996), respectively.
Reliability and validity of the Turkish version of the HDRS by Akdemir et al. (2001) calculated a Cronbach’s alpha coefficient of .75. For our sample, we calculated a Cronbach’s alpha coefficient of .77. Reliability and validity of the Turkish version of the HARS by Yazıcı, Demir, Tanrıverdi, Karaagaoglu, and Yolac (1998) calculated a Cronbach’s alpha coefficient of .72. For our sample, we calculated a Cronbach’s alpha coefficient of .74.
In the Turkish reliability and validity study of Turkish DES, Yargic, Tutkun, and Sar (1995) calculated Cronbach’s alpha .97 as the measure of internal consistency. Cronbach’s alpha coefficient was calculated to be .92 for our sample. The Turkish form of SDQ was adapted by Sar, Kundakci, Kiziltan, Bakim, and Bozkurt (2000) and was shown to have internal consistency with Cronbach’s alpha coefficient of .94. For our sample, we calculated a Cronbach’s alpha coefficient of .89.
Regarding the vitality of awareness of DV by mental health professionals, we conducted a study aiming to address prevalence of DV against women in psychiatric outpatients and determine descriptive and clinical correlates. We planned to compare two groups of patients; the first group consisted of patients exposed to DV from their intimate partners and the second group included female patients who have not experienced DV (non-DV, NDV). Our hypotheses are the following:
Method
Participants
This study was conducted at Psychiatry outpatient units of two state hospitals located in two neighboring districts of Konya, Turkey, in a 6 months period of time. The exclusion criteria for the patients were as follows: illiterate patients, psychotic, demented or mentally retarded patients, alcohol or substance abusers, and patients who had a chronic disease. After applying the exclusion criteria, 310 literate women, who were married, widowed, or divorced and aged 18 to 65 years applying to psychiatric outpatient units were recruited. Thirty three of them did not want to participate in the study and 277 patients were included in the study. Patients underwent a psychiatric examination comprised of a semistructured clinical interview of the DSM-IV-TR, which has a framework of psychiatric symptoms to be diagnosed. The local ethical committee approved the study. All subjects gave written informed consent to participate in this study. Women who experienced DV were compared with those who were not exposed to DV.
Measures
Sociodemographic data form
A form prepared by the researchers to obtain sociodemographic data. It includes detailed data about marital history (marriage type, duration, age at onset of marriage, etc.). The researchers tried to include parameters revealing cultural background of family structure when preparing this form. Sociodemographic forms used in intimate partner violence research in Turkey (Akyuz et al., 2002; Vahip, & Doganavsargil, 2006) lead the researchers in designing this form.
Semistructured clinical interview
The patients underwent a semistructured clinical interview with a trained psychiatrist. The patient is interviewed in a semistructured way and after having completed the interview, the SCID schedule is filled in and the patient is diagnosed according to DSM-IV-TR.
DV questionnaire
This questionnaire is constituted by the researchers with the help of DV form (Akyuz et al., 2002) and DV Clinical Interview (Doganavsargil & Sertoz, 2007) conducted by different researchers in Turkey. DV is still a taboo in our society, and the patients are reluctant to express it (Vahip & Doganavsargil, 2006). For this reason, the researchers preferred to use the questionnaire that they developed instead of using standardized questionnaires from different cultures. The questionnaire inquires about history of DV by partner, history of experiencing or witnessing physical violence between parents in childhood, if the children experienced physical violence by parents or witnessed physical violence between parents, personal opinions about DV, and help-seeking behaviors. In our study, we classified violence as emotional/verbal (humiliation, threatening, scolding, etc.), physical (smacking, kicking, attacking with a tool), sexual (forced sexual intercourse, using sexuality as a means of threat, etc.), and financial (leaving without money, taking her salary, etc.). This classification is consistent with WHO definitions of violence (Garcia-Moreno et al., 2006).
HDRS
A form developed by Hamilton (1960) consisting of 17 questions was used, and a score of ≥14 indicates depression. The reliability and validity study of the Turkish version were conducted by Akdemir et al. (2001).
HARS
The form designed by Hamilton (1959) for determining the level of anxiety and distribution of symptoms in individuals was used in the study. The HARS consists of 14 questions that investigate physical and mental symptoms. The reliability and validity study of the Turkish version were conducted by Yazıcı et al. (1998).
DES
The scale, developed by Bernstein and Putnam (1986), is a 28-item self-report measure that assesses the frequency of dissociative experiences, such as amnesia, gaps in awareness, depersonalization, derealization, absorption, and imaginative involvement. A DES score equal or greater than 30 is considered to be the threshold point for dissociative disorders in the Turkish population (Yargic et al., 1995).
SDQ
The SDQ, developed by Nijenhuis et al. (1996), is a 20-item self-report instrument that uses 5-point Likert-type scales to rate the severity of somatoform dissociation symptoms. The Turkish form of the SDQ was adapted by Sar et al. (2000).
Statistical Analysis
Study data were analyzed using the Statistical Package for Social Sciences (SPSS) for Windows Version 22.0 (IBM Corp., 2013). Descriptive statistics were presented as mean, standard deviation, median, and frequency (percentage). Normal distribution of the variables was tested by visual (histogram and probability graphs) and analytical methods (Kolmogorov-Simirnov Test). While evaluating the study data, the chi-square test was used to evaluate the relationships between the categorical variables and Mann–Whitney U test was used for nonparametric variables. For the multivariate analysis, the possible factors identified with univariate analyses were further entered into the logistic regression analysis to determine independent predictors of DV. Hosmer–Lemeshow goodness-of-fit statistics were used to assess model fit. A 5% Type I error level was used to infer statistical significance.
Results
Sociodemographic Features
A total of 277 patients were recruited in the study. Of the 277 patients, 58.8% were in DV group and 41.2% were in NDV group. The analysis was done in three steps. In Step 1, the DV and NDV groups were compared on the sociodemographic items and on characteristics previously research has found to be related to DV. In Step 2, variables that were statistically significant in Step 1 were entered into a logistic regression to determine which variables made independent contributions to the prediction of membership in the DV or NDV. In Step 3, group differences on depression, anxiety, and dissociation scores were determined.
In the comparison of the DV and NDV groups on the sociodemographic items and on some characteristics previously had been found to be related to DV, nominal demographic data were analyzed with chi square tests and continuous variables were analyzed with the Mann–Whitney test.
Table 1 illustrates the comparison of sociodemographic features between groups of DV and NDV. There are statistically significant differences between two groups in terms of marital status (p = .013), marriage age (p = .001), marriage age of husband (p = .014), marriage pattern (p = .039), education level (p < .001), occupation status (p < .001), monthly income (p < .001), husband’s education level (p < .001), husband’s occupation status (p = .029), and family type (p = .001). These data confirm our Hypothesis 1. There is no difference between groups in terms of marriage number and number of children. Prevalence of alcohol use by partner was higher (17.8%) in DV group compared with NDV (5.3%) group (p = .002). Only 9% of patients reported a relation between violence and alcohol use. There is only one reported substance abuse by the partner in DV group.
Comparison of DV and NDV Groups in Terms of Sociodemographic Features.
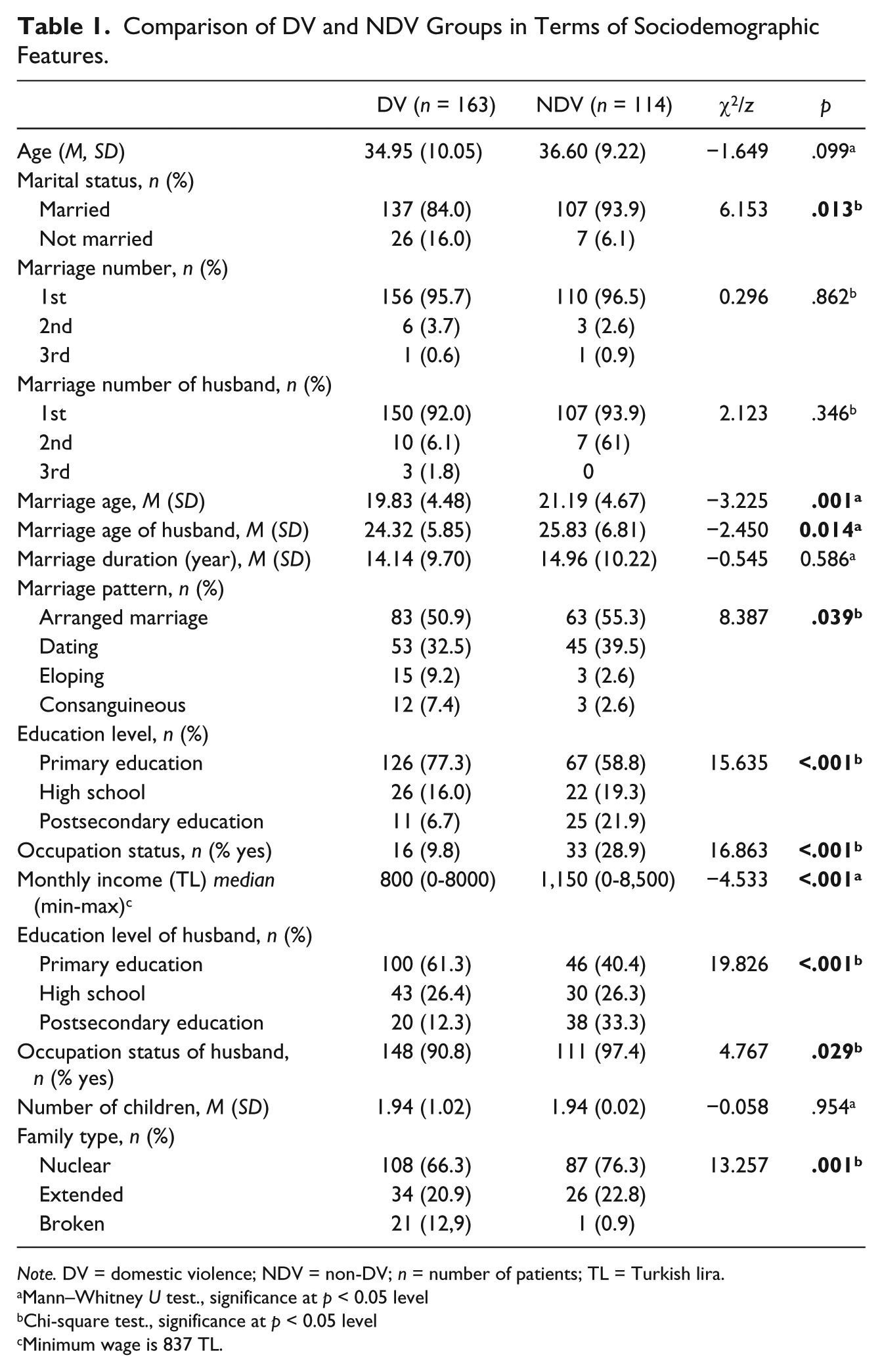
Note. DV = domestic violence; NDV = non-DV; n = number of patients; TL = Turkish lira.
Mann–Whitney U test., significance at p < 0.05 level
Chi-square test., significance at p < 0.05 level
Minimum wage is 837 TL.
Characteristics Related With DV
Comparison of groups in terms of some characteristics related with DV is given in Table 2. Experiencing physical violence in childhood were more in DV group (49.1%) compared with NDV group (36.0%; p = .030). Witnessing physical violence between parents in childhood was also higher in DV group (p = .012). These two data verify our Hypothesis 2. Women from DV group (68.1%) battered their children more compared with women from NDV group (43.9%; p < .001) which confirms our Hypothesis 3. Partners of women from DV group also battered their children more (p < .001).
Comparison of DV and NDV Groups in Terms of Some Characteristics Related With Domestic Violence.
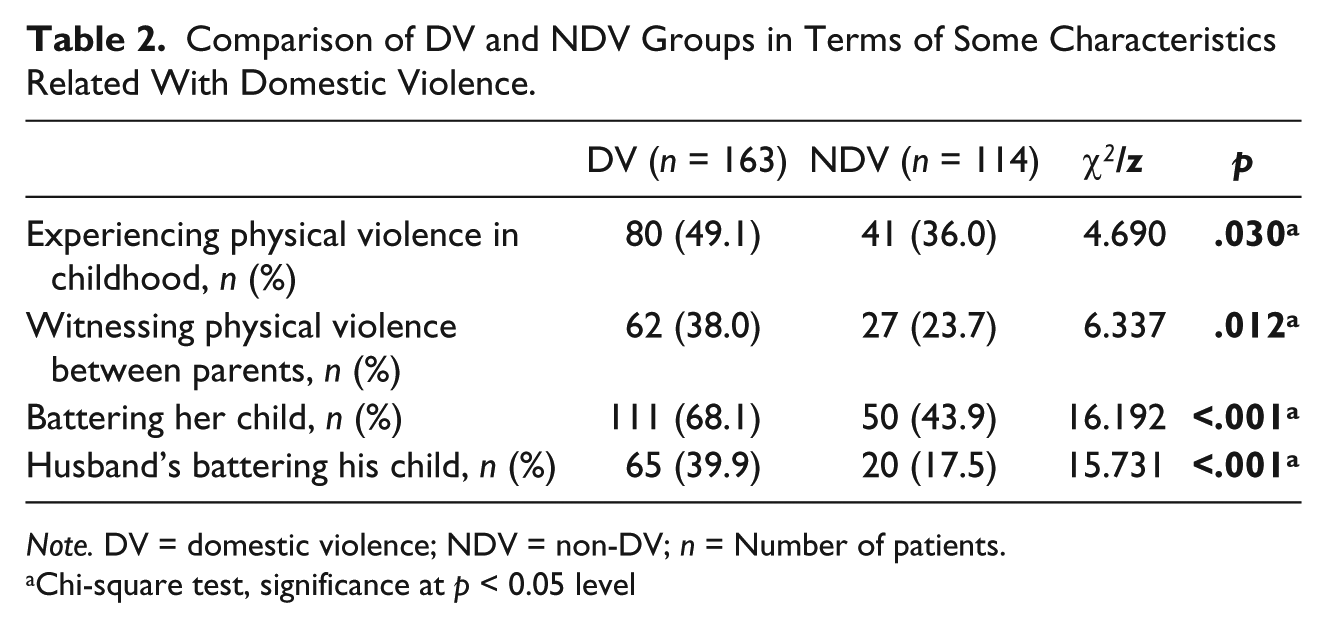
Note. DV = domestic violence; NDV = non-DV; n = Number of patients.
Chi-square test, significance at p < 0.05 level
Variables that were statistically significant were entered into a logistic regression to determine which variables made independent contributions to the prediction of membership in the DV or NDV groups. The data are given in Table 3. According to the results of logistic regression analysis, occupation status, husband’s education level, family type, woman’s battering her child and husband’s battering his child are important predictors of DV (p<0.05). If the woman had a job, risk of being exposed to DV decreased 3.4 times. If the husband had postsecondary education level instead of primary education, risk decreased 2.9 times. Risk of being exposed to DV increased 6.4 times if the family is of broken type, 2.2 times if the woman battered her child, and 2.3 times if the husband battered his child.
Results of Logistic Regressions on Some Characteristics Related With Domestic Violence.
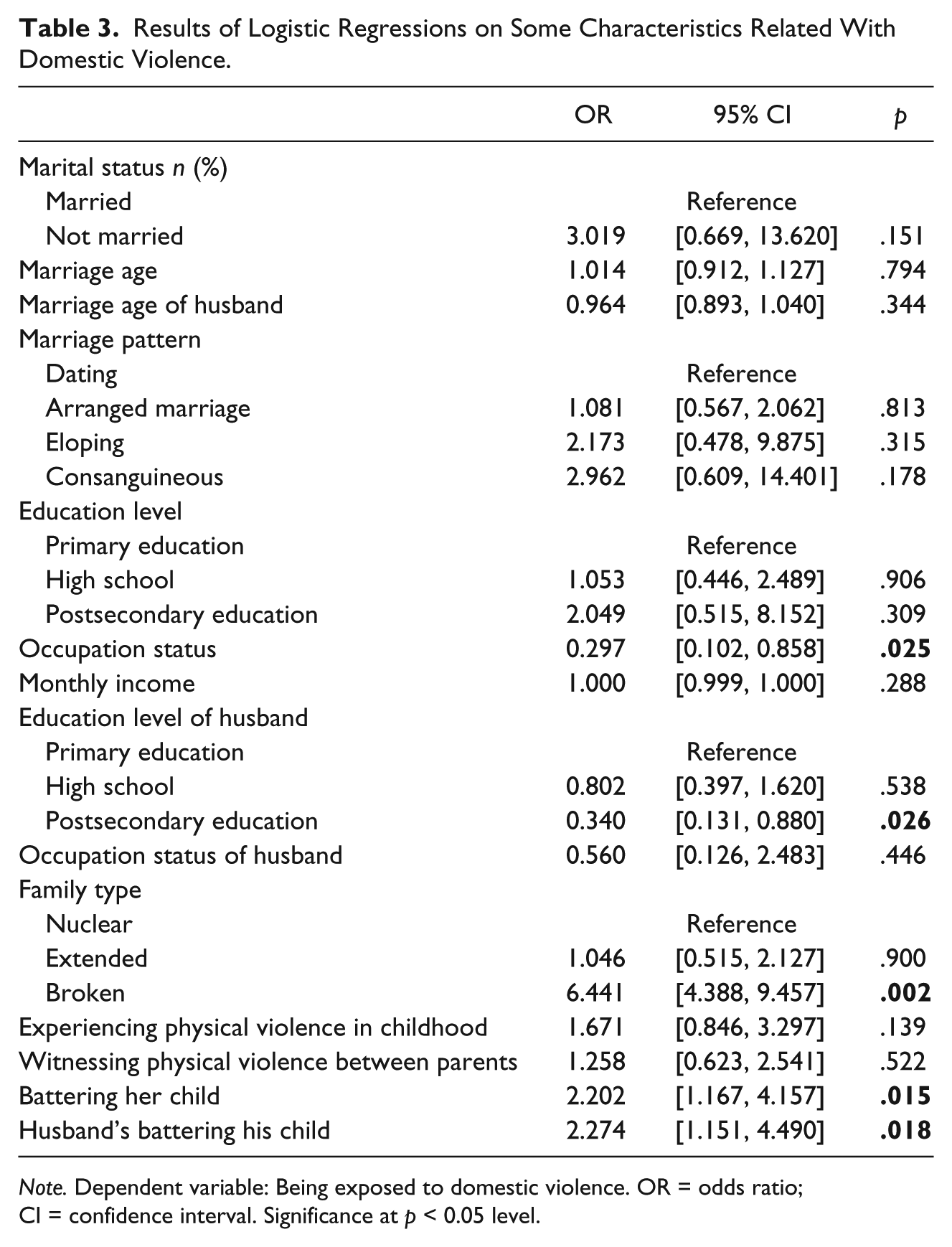
Note. Dependent variable: Being exposed to domestic violence. OR = odds ratio; CI = confidence interval. Significance at p < 0.05 level.
In all, 94.6% of all women expressed the opinion that there is no justifiable violence; 4.7% agreed with the idea that husbands have the right to batter their wives in some instances. In terms of exposed types of violence, 100% (n = 163) of women from DV group were exposed to emotional/verbal violence, 85.3% (n = 139) to physical violence, 52.1% (n = 85) to financial abuse, and 41.7% (n = 68) to sexual violence. Children of 47.9% of patients from DV group witnessed physical violence between partners.
In all, 51.5% of women from DV group mentioned about their experience of violence to their families, 22.7% to their friends, and 4.9% to their relatives; 20.9% talked about violence with nobody. Only 10.4% of the women experiencing violence asked for help from a person or institution. 68% of women from DV group and 61% from NDV group had knowledge about the law on the protection of the family.
Psychopathology Related Features
Of all the patients, 9.0% had no psychiatric diagnosis, 27.8% were diagnosed with an anxiety disorder, 20.9% with major depressive disorder, 13.5% with adjustment disorder, 10.8% with conversion disorder, 9.7% with dysthymic disorder, and 8.3% with a somatoform disorder. All the women belonging to DV group had a psychiatric diagnosis. Prevalence of depression, conversion disorder, and other somatoform disorders were higher compared with NDV group (p < .001; Table 4). This is in concordance with our Hypothesis 4.
Distribution of Psychiatric Diagnoses Between Groups.
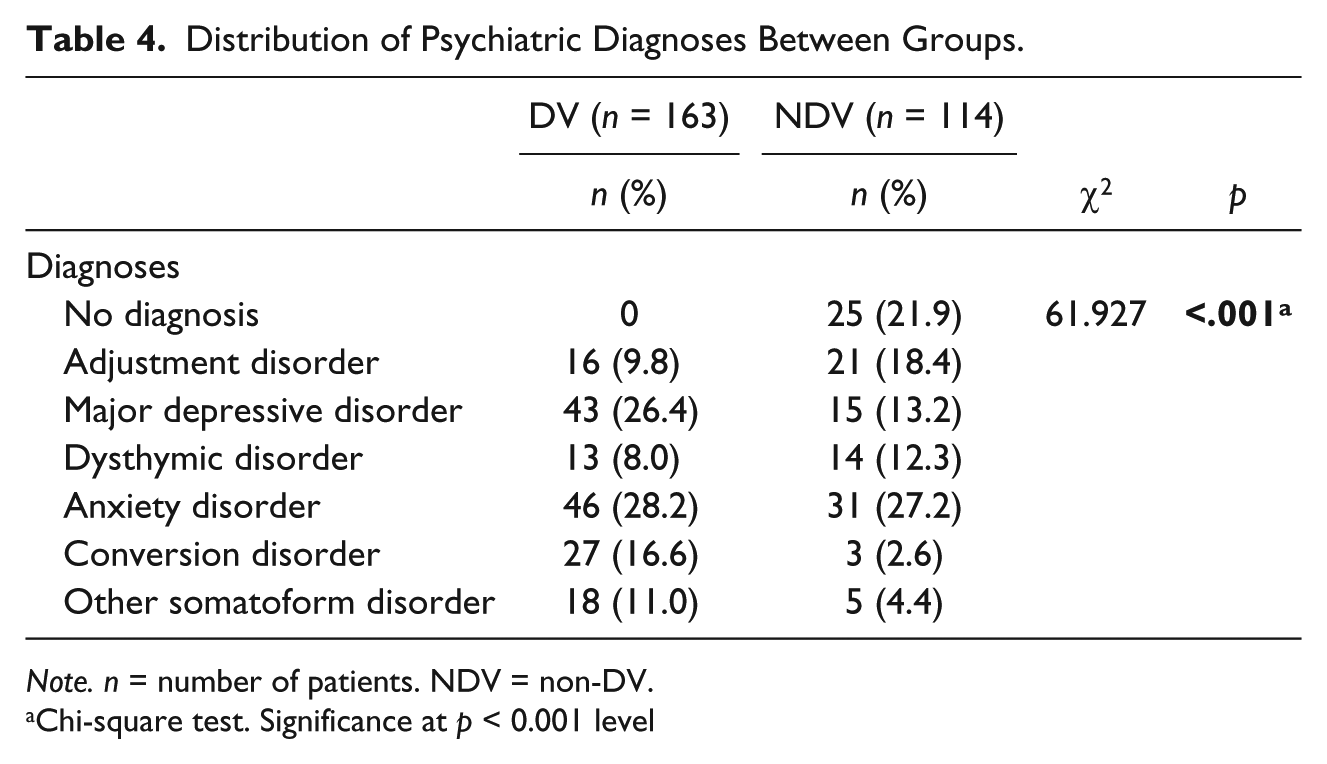
Note. n = number of patients. NDV = non-DV.
Chi-square test. Significance at p < 0.001 level
Women from DV group had higher depression (HDRS), anxiety (HARS), dissociative experience (DES), and somatoform dissociation (SDQ) scores compared with NDV group (p < .001). In other words, women experiencing intimate partner violence are more depressed, more anxious, and have more dissociative symptoms compared with women who do not experience this kind of violence. Number of women scoring above cutoff levels for DES and SDQ were significantly higher in DV group compared with NDV group (p < .001; Table 5). These data are in line with our Hypothesis 5.
Comparison of DV and NDV Groups in Terms of Scale Scores.

Note. DV = domestic violence; NDV = non-DV; HDRS = Hamilton Depression Rating Scale; HARS = Hamilton Anxiety Rating Scale; DES = Dissociative Experiences Scale; SDQ = Somatoform Dissociation Questionnaire.
Mann–Whitney U test. Significance at p < 0.001 level
Chi-square test. Significance at p < 0.001 level
Discussion
The present study investigated DV in a group of women applying to outpatient units of two neighboring district state hospitals, including its rate, related demographic and marital factors, and connection with psychopathology. In our sample, 58.8% of women stated that they experienced DV. This high ratio is in concordance with other studies in Turkey (Akyuz et al., 2002; Doganavsargil & Sertoz, 2007; Karaoglu et al., 2005; Kaymaz et al., 2014; Kocacik & Dogan, 2006; Vahip, & Doganavsargil, 2006). This ratio is higher than that of European Union countries (FRA, 2014), the United States (Haggerty & Goodman, 2003), and South Africa (Jewkes, Levin, & Penn-Kekana, 2002). However, we should bear in mind that findings on the prevalence of DV vary greatly between studies due to methodological differences, different definitions of violence, cultural reasons, and attitude of interviewer (Watts & Zimmerman, 2002). High ratio of DV in our sample is perhaps due to the fact that our sample consists of patients applying to a psychiatric outpatient unit. We have revealed that the most prevalent type of violence was the emotional/verbal type, followed by physical, financial, and sexual violence, similar to most of other studies (Kaymaz et al., 2014; Kocacik & Dogan, 2006).
Univariate analyses revealed that education level and occupation of both the woman and the partner were significantly related with the rate of DV. In NDV group, ratios of university graduates and civil servants were higher compared with DV group. This indicates the protective effect of education and economic independence against violence. In literature, it is consistently reported that low education is a risk factor for DV (Akyuz et al., 2002; Doganavsargil & Sertoz, 2007; Garcia-Moreno et al., 2006; Karaoglu et al., 2005; Kaymaz et al., 2014; Kocacik & Dogan, 2006; Vahip, & Doganavsargil, 2006). İlliterate women were excluded in our study. It is probable that the prevalence of DV would increase if they were included. About 91% of women exposed to violence were housewives, as opposed to civil servants and workers who together reached the rate of 9%. This ratio was 72% to 28% in NDV group which confirms the protective effect of economic independence (Erlick Robinson, 2003; Kocacik & Dogan, 2006). Income level was found to be related to DV according to univariate analyses similar to other studies (Karaoglu et al., 2005; Kocacik & Dogan, 2006; Koenig et al., 2003). In multivariate analysis, among demographic factors, only occupation level of the woman and education level of the partner was found to predict DV.
According to both univariate and multivariate analyses; family type was another important predictor of DV. In DV group, the ratio of broken families was higher compared with NDV group. Kocacik and Dogan (2006) reported higher sexual violence ratio in broken families. Violence could be one of the reasons for divorce or living separated.
Young age of marriage is reported to be a risk factor for DV (Begum, Donta, Nair, & Prakasam, 2015; Directorate General on the Status of Women, 2014). Couples usually marry at a young age when they marry by eloping, which is a common way of marriage in some regions of Turkey. Shaikh, Kayani, and Shaikh (2014) stated that consanguineous marriages do not protect women from DV. It could rather increase the risk of DV as these marriages are usually executed by parents’ will. In the present study, age of marriage and marriage pattern were found to be related with DV in univariate analyses, but not in multivariate analyses.
Prevalence of experiencing and witnessing physical violence was higher in DV group. Literature data say that women who have been abused in childhood or witnessed violence between parents are at higher risk of being victimized and may perceive violence as a normal part of intimate relationships (Bensley, Van Eenwyk, & Wynkoop Simmons, 2003; Jirapramukpitak, Harpham, & Prince, 2011). However, multivariate analyses did not reveal experiencing and witnessing physical violence in childhood as independent risk factors for being exposed to DV in contrary to our hypothesis. Women and partners of women from DV group used physical violence against children more compared with NDV group and children in line with the study of Vahip and Doganavsargil (2006). Not surprisingly; the present study reveals that other predictors of DV exist where children within a close personal relationship are battered by either parent.
Strong links have been found between alcohol use and the occurrence of DV in many countries (Testa, Quigley, & Leonard, 2003). Prevalence of alcohol use by partner was higher (18%) in DV group compared with NDV (5%) group in our study, but only 9% of patients reported a relation between violence and alcohol use. This ratio is lower compared with many other countries. It may be because of the fact that Islam, which forbids alcohol consumption, has a great impact on daily lives in the region.
In our study, the ratio of talking about violence to someone was higher compared with a large population-based research in Turkey in 2014 (KSGM, 2014). In that research, 44% of women reported that they talked about their DV experience with nobody. This difference could be explained by several factors. As said before, illiterate women were not included in the study, and education is correlated positively with telling about violence. Second, subjects from our sample had the opportunity to apply to a psychiatrist for their psychological problems and therefore may not exactly represent the regional population. High ratio of women had knowledge about the law on the protection of the family. Although the ratio of telling about violence and knowledge about the law is high, only 10% asked help from a person or institution similar to ratios in the population-based research (KSGM, 2014). We did not ask about the reason why the women did not seek help for DV. We may think about some factors. Feeling of disgrace, reluctance about revealing family secrets, financial worries, belief that police and law could not protect them, and fear about being exposed to more violence could have retained them from asking help from a person or institution.
Although there are regional differences, our culture is predominantly a male-dominated culture in which sexual roles are rigidly differentiated. The Islamic rules suggest obedience to women, and opposing their husband is not allowed. These factors are considered as risk factors for DV (Page & Ince, 2008). Our finding is that more than 90% of women defended the opinion that there is no justifiable violence in such a conservative setting which instills hope to gain success in the struggle with violence.
In the present study, although all the women from DV group had a psychiatric diagnosis, 21.9% of women from NDV group did not have a psychiatric diagnosis. These are patients applying mostly for counseling purposes. When compared with NDV group, depression, conversion disorder, and other somatoform disorders were significantly more prevalent in DV group. This finding is in line with literature data stating that traumatic experiences such as being subject to violence can lead to a range of mental health problems and increase vulnerability to develop psychopathology (Kessing, Agerbo, & Mortensen, 2003; Sayed, Iacoviello, & Charney, 2015).
Women from DV group had higher depression, anxiety, and dissociation scores compared with women from NDV group in line with the study of Kaymaz et al. (2014). One of the primary mental health responses of women experiencing DV is depression (Wong, Tiwari, Fong, & Bullock, 2016). In their review, Dillon, Hussain, Loxton, and Rahman (2013) reported a positive association between a history of intimate partner violence and increased levels of anxiety in women.
Dissociation is the marker of the psychological impact of trauma and violence. There are few studies reporting that dissociative experience was considerably elevated in the DV sample compared with the comparison group (Dorahy, Lewis, & Wolfe, 2007; Kaymaz et al., 2014; Marchiori, Rossi, & Colombo, 2004). Somer, Ross, Kirshberg, and Bakri (2015) reported that average DES score among Arab women subjected to DV exceeded the commonly accepted cutoff score of 30, a suggested boundary between normal and abnormal dissociation. In our sample, almost half of the woman from DV group had a score of 30 and more from DES in concordance with that study. Somatoform dissociation has been found to be associated with reported trauma (El-Hage, Darves-Bornoz, Allilaire, & Gaillard, 2002). To our knowledge, there is no study in literature reporting an association of somatoform dissociation with intimate partner violence. In our study, 41.7% of patients from DV group had scores 40 and above from SDQ compared with 7.9% of NDV group, suggesting a significant relationship of somatoform dissociation with DV. We propose that many of abused women in conservative, male-dominated cultures, such as the one we sampled from, use both psychologic and somatoform dissociation as a coping strategy to manage painful memories, threatening environments, and aching bodies.
There are some limitations of our study. First of all, it is a cross-sectional study, and the results are limited for the inference of causality. Second, we included patients applying to psychiatric outpatient unit and therefore cannot generalize the results to whole population. Third, we did not include illiterate women which could have affected the results. Fourth, there is a probability that some patients did not want to report DV although they experienced it. Cultural issues such as shame, fear, cultural tradition discouraging disclosure may affect women’s disclosure of DV.
In conclusion, the prevalence of DV is high in patients applying to psychiatric outpatient units. Occupation status of woman, education level of partner, family type, woman’s battering her child, and husband’s battering his child are independent predictors of DV. Prevalence of having a psychiatric diagnosis is higher in women from the DV group and they have elevated depression, anxiety, and dissociation scores compared with women who have not experienced intimate partner violence.
It is crucial for mental health workers to increase their knowledge and awareness about DV to evaluate violence in depth during psychiatric interview and to guide patients to get support. It is important to hold in mind that DV is a problem handing down from generation to generation. Therefore, the impact of interventions about violence would exceed the present and affect future generations. Further research will enable us to establish appropriate strategies to prevent DV and to ensure optimal care of this vulnerable population.
Footnotes
Acknowledgements
The authors thank all the participants.
Authors’ note
All the authors have substantially contributed to the preparation of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.