
Abstract
The role of pregnant adolescents as perpetrators of intimate partner violence (IPV) is not well understood. Socioecological factors associated with IPV (physical assault and injury, and psychological aggression) perpetrated by pregnant adolescents and the association between IPV and attitudes toward the use of physical punishment to discipline children were examined among 246 pregnant adolescents. Pregnant adolescents were more likely to report perpetrating both physical assault (24%) and psychological aggression (52.7%) than being the recipient (12.2% and 38.6%, respectively) and having been physically injured (7%) than inflicting injury (4.1%). Risk factors for perpetrating physical assault included prior assault by partner, being African American, exposure to community violence, being in trouble with the police, and multiple lifetime drug use. IPV perpetrators had more favorable attitudes toward the use of physical punishment. Interventions should address IPV and parenting attitudes in young couples to maximize the health and safety of both mother and unborn child.
Introduction
Intimate partner violence (IPV) is the intentional physical, sexual, or psychological abuse inflicted by one’s current or former partner or spouse (Centers for Disease Control and Prevention [CDC], 2015a). National studies suggest approximately one in 10 women in the United States has been raped by an intimate partner, one in six has experienced sexual abuse other than rape, one in four has experienced severe physical violence, and one in two has experienced psychological aggression (CDC, 2014a). In the same data set, African American (44%) and Hispanic women (54%) were more likely to experience IPV compared with White women (35%). Women ages 16 to 24 years experience the highest rates of sexual assault (Family Violence Prevention Fund, 2010). In addition, pregnant adolescents consistently report higher rates of physical abuse compared with pregnant older women (Goodwin, Gazmararian, Johnson, Gilbert, & Saltzman, 2000; Saltzman, Johnson, Gilbert, & Goodwin, 2003; Wiemann, Agurcia, Berenson, Volk, & Rickert, 2000).
IPV during pregnancy significantly increases risk of pregnancy trauma (National Institute of Justice [NIJ], 2013) and is linked with poor birth outcomes such as preterm labor, depression, and low birth weight (Alhusen, Ray, Sharps, & Bullock, 2015; NIJ, 2013; Pavey, Gorman, Kuehn, Stokes, & Hisle-Gorman, 2014). Data from the World Health Organization (WHO; 2012a, 2012b) indicate IPV during pregnancy increases the likelihood of having premature and low birth weight babies that can lead to neonatal mortality. Adolescents who experience IPV during pregnancy are also more likely to experience IPV during the postpartum period (Harrykissoon, Rickert, & Wiemann, 2002; Scheiman & Zeoli, 2003). Studies suggest homes that experience IPV during the first 6 months of a child’s life are more than 3 times as likely to experience physical child abuse and are also 2 times more likely to experience psychological abuse or neglect compared with households with no IPV (Casanueva & Martin, 2007; Harper, Ogbonnaya, & McCullough, 2016; Herrenkohl, Sousa, Tajima, Herrenkohl, & Moylan, 2008).
Although females are often recognized as victims of IPV (De Koker, Mathews, Zuch, Bastien, & Mason-Jones, 2014; McMahon, Huang, Boxer, & Postmus, 2011), female partners can also perpetrate violence, predominantly through psychological aggression (54.4%; Whitaker, 2014). IPV studies investigating differences in gender perpetration among adult samples have shown comparable rates of male-on-female and female-on-male violence; however, female-perpetrated IPV was less severe than male-perpetrated IPV (Birkley & Eckhardt, 2015; Shneyderman & Kiely, 2013; Whitaker, 2014). Among adult pregnant women, those who participate in reciprocal IPV, meaning both perpetration and victimization, are at highest risk for adverse health outcomes (Shneyderman & Kiely, 2013). Less is known about perpetration of IPV by pregnant adolescents, whether IPV is reciprocal, and the frequency with which injury results.
Several studies of women of mixed ages have identified risk factors associated with female IPV victimization (Abramsky et al., 2011; Bazargan-Hejazi et al., 2014; Miszkurka, Zunzunegui, & Goulet, 2012), but few have examined the profile for female perpetration. The few studies on IPV perpetration found female perpetrators of all ages were more likely to drink and use drugs, experience depression, be exposed to interparental violence, and feel less happy about their pregnancies (Bazargan-Hejazi et al., 2014; Shneyderman & Kiely, 2013; Temple, Shorey, Tortolero, Wolfe, & Stuart, 2013). Physically aggressive pregnant adolescents also exhibit higher rates of maternal complications, such as preterm birth and low birth weight, and psychological consequences, such as depression and anxiety, than those who are nonviolent (Shneyderman & Kiely, 2013).
Although studies have documented IPV risk factors in large population-based samples of women (Breiding, Black, & Ryan, 2008; Renner & Whitney, 2012; Saltzman et al., 2003), there is a paucity of research data on IPV risk factors in pregnant adolescents (Wiemann et al., 2000). In addition, the role of pregnant adolescents as IPV perpetrators is not well understood. Therefore, the present study evaluated different forms (victimization, perpetration, and reciprocal violence) and kinds (physical assault and psychological aggression) of IPV among pregnant adolescents, and used a socioecological framework to examine intrapersonal, interpersonal, family, and community correlates associated with IPV perpetration. As vulnerability for IPV is affected by multiple risk factors, the Social Ecological Theory framework was adopted to guide the study. According to Social Ecological Theory, an individual’s development and behavior are affected by various systems: intrapersonal, interpersonal, family, and community/society (Bronfenbrenner, 1979). These systems, in turn, affect an individual’s health and well-being. Intrapersonal includes interactions with oneself, interpersonal includes interactions with partners, family includes interactions with individual family members and the family as a whole, and community/society includes interactions with community members who influence the pregnant females, their partners, and their families. This framework has been identified as ideal for studying violence because the influence interpersonal, family, and community/society factors have on the individual is known to increase or decrease the risk for IPV and child abuse (Little & Kantor, 2002). This exploratory study also examined the relationship between IPV and attitudes toward the use of physical punishment on children.
Method
Participants
Participants were pregnant adolescents recruited to a community-based prenatal care intervention to promote healthy pregnancy outcomes. Eligibility criteria included pregnant and planning to carry pregnancy to term; aged 15 to 18 years; attending one of five teen health clinics, or referred by a community school or agency; English-speaking; and free of obvious cognitive impairment. These urban community–based clinics provide free to low-cost reproductive health care to low-income adolescents and young adults. Of the 426 pregnant adolescents approached about participating, 346 met eligibility criteria and 249 (72%) were enrolled. The 97 who declined participation said they were not interested (n = 60), lived too far away or had transportation barriers (n = 16), or were receiving prenatal care elsewhere (n = 11). Although demographic data were not collected on pregnant adolescents who did not consent to participate, the demographic profile of participants closely mirrored those of the two clinics from which they were recruited.
Procedure and Measures
All research protocols were approved by the affiliated Institutional Review Board for Human Subjects Research. A case manager or research assistant approached eligible adolescents about participating in the program. Each participant formally consented, and parental consent was obtained for participants less than 18 years of age. A research assistant provided instructions on how to complete the baseline assessment using Audio Computer-Assisted Self-Interview (ACASI), which took about an hour to finish. ACASI was used to enhance data accuracy and eliminate low literacy as a potential barrier (Beauclair et al., 2013; Metzger et al., 2000).
IPV
IPV was measured using the Revised Conflict Tactics Scale (CTS2) and the Safe Dates Measurement for Psychological Abuse Victimization (SDM). The CTS2 is the most commonly used instrument for identifying IPV (Straus, 2007). The SDM specifically measures IPV variables among middle and high school students involved in dating relationships (Foshee et al., 2004). The CTS2 measures negotiation, psychological aggression, physical assault, sexual coercion, and injury. Items from each of the CTS2 subscales were utilized except for those in sexual coercion, due to reporting requirement concerns. The survey resulted in 74 total items. For each item, participants first reported on behavior toward their partner (perpetration), followed by their partner’s behavior toward them (victimization). Both the CTS2 and SDM have a range of severity levels from less severe to more severe behaviors. Severity is based on the associated harm resulting from behavioral acts.
CTS2 and SDM subscales have been tested and validated as screening tools for IPV in relationships involving adolescents (Callahan, Tolman, & Saunders, 2003; Miller et al., 2010). Cronbach’s alpha coefficients ranged from .79 to .95 across studies that utilized the CTS2. For the SDM, Foshee et al. (2000) reported Cronbach’s alpha levels ranging from .65 to .81.
Intrapersonal correlates
Intrapersonal correlates included self-reported race/ethnicity, limited economic resources, an unplanned current pregnancy, lifetime use of harmful licit and illicit substances, and having repeated one or more grades in school. Economic resources were considered limited if the pregnant adolescent reported she did not have enough money, food, clothing, or health care to live on (Raneri & Wiemann, 2007). To determine substance use, participants were asked whether they had ever smoked cigarettes, drank alcohol (beer, wine, and hard liquor), used marijuana or other illegal drugs, used prescription drugs or diet pills without medical supervision, or sniffed glue. The resulting variable included use of no substances, use of one substance, or use of two or more different substances.
Interpersonal correlates
Interpersonal correlates included prior physical, sexual, or verbal abuse, and limited contact with the father of the baby. Prior physical or sexual assault was affirmed if participants reported ever having been hit, slapped, kicked, or physically hurt by anyone; touched or forced to touch someone sexually; or forced to have sexual intercourse without consent. Verbal abuse was defined as ever having been called ugly names, “like dumb, bitch, no good.” An additional question asked whether the pregnant adolescent wished she could see the father of her baby more often, less often, about the same, or not at all. The resulting variable was coded as wanting to see the baby’s father more often versus the other options combined.
Family correlates
Participants were asked about the amount of criticism they received from family members using five items (such as “My family tries to run my life” or “My family tells me I am too young to be a mother”) on a 5-point scale from always true to never true. A total score, which was divided by five, had a possible range of 0 to 4 (Raneri & Wiemann, 2007). Cronbach’s alpha coefficient is .70 for the sample of pregnant adolescents.
Community correlates
Exposure to community violence was assessed by a series of items that asked the number of times, during the pregnant adolescent’s lifetime, she had ever seen someone attacked with a weapon, carried a weapon for protection, or been afraid of being hurt by other teens (Raneri & Wiemann, 2007). The resulting variable was then collapsed into any versus no exposure to community violence. A general support variable was created by asking pregnant adolescents to indicate, on a 5-point scale (always true to never true), the amount of emotional, financial, informational, and transportation support they received from anywhere (Raneri & Wiemann, 2007). The resulting variable (Cronbach’s α coefficient = .89) was calculated by summing the responses to each item and dividing by the six total number of items.
Attitudes toward physical punishment
The Adult–Adolescent Parenting Inventory (AAPI) was used to measure alternatives considered instead of using physical punishment on children (Bavolek, 2001). This AAPI subscale contains 11 items, each with five possible response options scored 1 to 5, yielding total scores that range from 11 to 55 (Cronbach’s alpha coefficient = .83). Higher scores indicate more alternatives to physical punishment considered.
Data Analysis
All analyses were conducted using SPSS, version 23.0. Bivariate analyses (Student’s t test or chi-square) were used to identify intrapersonal, interpersonal, family, and community correlates associated with perpetrating IPV toward a male partner. Three pregnant adolescents did not complete the CTS2 and SDM measures, leaving a final analysis sample of 246. Factors associated with IPV, p < .20, were entered into logistic regression analyses. Multicollinearity among variables was evaluated using correlation (Pearson’s r or Spearman’s rho) or chi-square analyses, depending on the level of measurement. ANOVA was used to compare attitudes toward avoiding the use of physical punishment among groups of pregnant adolescents divided according to whether they were engaged in IPV victimization, perpetration, reciprocation, or none of the above.
Results
Sociodemographic Profile
The sample was predominantly African American (38.2%) and Hispanic (54.5%). The mean age for the participants was 16.9 years (range = 15-18, SD = 1.2 years). The majority (71.4%) was attending high school, 9.0% had dropped out of school, and 17.1% were high school graduates or had received a General Education Development Test (GED). The majority (98.0%) of participants reported their marital status as single/living with family/engaged.
IPV
A total of 59 (24%) pregnant adolescents reported physically assaulting their partners. Thirty (12.2%) pregnant adolescents reported being physically assaulted by their partner and 20 (8.1%) engaged in reciprocal IPV (Table 1). Pregnant adolescents who reported physically assaulting their partner were significantly more likely to perpetrate psychological abuse than nonphysically aggressive females and, as might be expected, they were also more likely to cause injury. Physically abusive females were also significantly more likely to be victims of physical and psychological violence, and to experience injury from their partner, than nonviolent females. Over 90% of pregnant adolescents reported that they used negotiation strategies with their partners and this did not differ by whether they perpetrated physical assault.
Types of IPV Experienced and Perpetrated By Pregnant Adolescents for the Sample Stratified by Whether She Reported Physically Assaulting Her Partner.
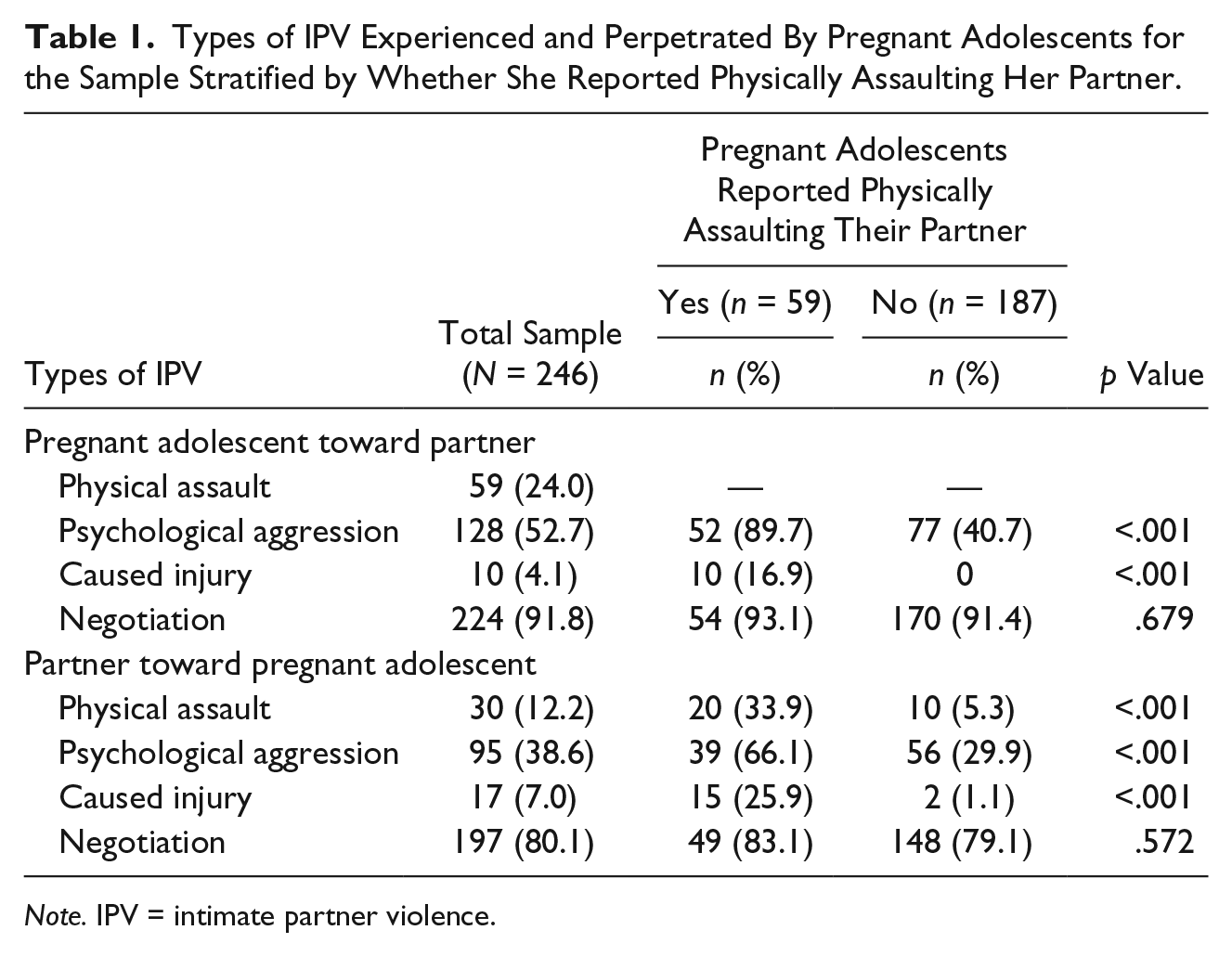
Note. IPV = intimate partner violence.
Intrapersonal, Interpersonal, Family, and Community Correlates
Bivariate analyses revealed that several intrapersonal factors were associated with perpetrating physical assault against a male partner (Table 2). Participants who reported assaulting their partners were more likely than adolescents who did not report assaulting their partners to be African American (vs. Hispanic or White/Other), to be a multiple lifetime drug user, to have repeated at least one grade in school, to report moderate-to-severe depressive symptoms, and to have been in trouble with the police or a teacher. Interpersonal factors associated with perpetrating physical assault included having experienced prior physical, sexual, or verbal abuse (Table 2). Family and community factors associated with perpetrating physical assault included higher family criticism and lower overall support, having been exposed to community violence, stolen something from a store, stayed out with friends past 2:00 a.m., and attended school while drunk or high (Table 3).
Intrapersonal and Interpersonal Socioecological Factors for the Sample Stratified by Whether Pregnant Adolescent Reported Physically Assaulting Her Partner (n = 246).

Other = Asian, American Indian or Alaska Native, Mixed.
Family and Community Socioecological Factors For the Sample Stratified By Whether Pregnant Adolescent Reported Physically Assaulting Her Partner (n = 246).

Results of the logistic regression analyses identified six factors significantly associated with pregnant adolescents perpetrating IPV (Table 4). These included the following intrapersonal factors: being African American (vs. Hispanic: adjusted odds ratio [AOR] = 5.35; 95% confidence interval [CI] = [2.40, 11.92]; p < .001), reporting multiple lifetime drug use (AOR = 1.42; 95% CI = [1.12, 1.81]; p = .004), having repeated one or more grades in school (AOR = 2.47; 95% CI = [1.20, 5.10]; p = .014), and having been in trouble with the police (AOR = 2.85; 95% CI = [1.28, 6.39]; p = .011). One interpersonal factor—having been physically assaulted by her partner (AOR = 7.03; 95% CI = [2.67, 18.53]; p ≤ .001)—and one community factor—exposure to community violence (AOR = 2.32; 95% CI = [1.07, 5.03]; p = .032)—were also associated with perpetrating IPV. The Hosmer and Lemenshow Goodness-of Fit-Test = 2.76 (8), p = .95, indicated an acceptable fit to the data.
Logistic Regression Model of Physically Assaulting Partner (n = 243).
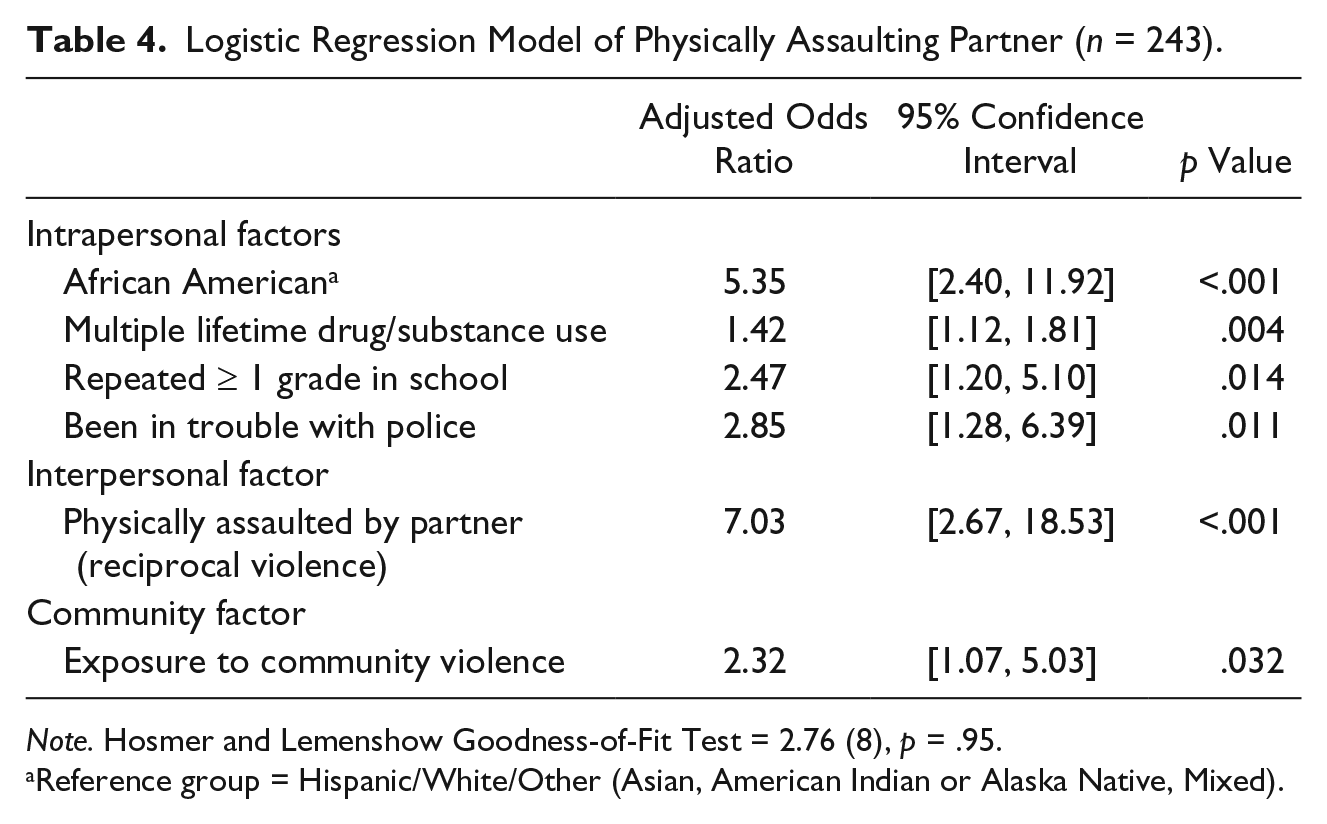
Note. Hosmer and Lemenshow Goodness-of-Fit Test = 2.76 (8), p = .95.
Reference group = Hispanic/White/Other (Asian, American Indian or Alaska Native, Mixed).
Results of ANOVA indicated that attitudes toward alternatives to physical punishment were higher, F(3, 240) = 5.857, p = .001, moderate effect size = 0.068, among pregnant adolescents who were neither the perpetrator nor the recipient of physical assault (n = 175, 37.6 ± 8.0) than those who were perpetrators only (n = 39, 33.0 ± 5.5) or who reported reciprocal physical assault (n = 20, 32.3 ± 8.8), but did not differ from those who were victims only (n = 10, 35.9 ± 7.7).
Discussion
The results of this exploratory study indicated nearly one in four (24%) pregnant adolescents reported having perpetrated IPV. In addition, 12.2% reported being victims of IPV, and 8.1% participated in reciprocal IPV. Although few studies have examined IPV perpetration and reciprocation among pregnant adolescents, prior research on perpetration by female adolescents (Haynie et al., 2013) and pregnant women (Shneyderman & Kiely, 2013) reported lower rates than the current study. Studies involving similar demographic samples of pregnant adolescents have reported comparable rates of IPV victimization (Harrykissoon et al., 2002; Wiemann et al., 2000). Prior studies with pregnant IPV victims (Asheer, Berger, Meckstroth, Kisker, & Keating, 2014; Shneyderman & Kiely, 2013; Wiemann et al., 2000) as well as female adolescent IPV perpetrators (Haynie et al., 2013) have reported similar risk factors.
The results of this study suggest that intrapersonal, interpersonal, family, and community factors were associated with IPV perpetration and victimization. This supports the utility of the socioecological framework that focuses on the dynamic and complex relationship between the individual and the environment (CDC, 2015b, 2016; Little & Kantor, 2002; WHO, 2012b). Participants who reported assaulting their partners were more likely than adolescents who did not report assaulting their partners to be African American (vs. Hispanic or White/Other). Prior studies of dating violence have reported that after controlling for socioeconomic status, the highest rates of dating violence perpetration were among African American adolescents, particularly females, followed by Latino and White adolescents (Foshee et al., 2008; Foshee, Reyes, & Ennett, 2010). Destructive communication skills, a measure composed mostly of items assessing destructive responses to anger, were reported significantly more often by minority adolescents, and destructive communication skills predicted dating violence perpetration (Foshee et al., 2008). Foshee et al. (2010) suggested that Black adolescents may have built up anger from a history of racism and blocked opportunities. Further research is needed to explore reasons for the higher rates of violence reported by pregnant African Americans in our study.
The pattern of exposure to interpersonal and community violence suggests a cycle of victimization, perpetration, and revictimization. Trauma research has found that victims may experience a fluidity of abuse, as they move between identifying as a victim and as a perpetrator (Lord, 2008). Such fluidity impacts an individual’s ability to develop and maintain healthy relationships (Pearlman & Courtois, 2005). Studies have pointed to an intergenerational transmission of IPV, with exposure to IPV in childhood predicting increased risk for experiencing IPV in adulthood (Cannon, Bonomi, Anderson, & Rivara, 2009; Insetta et al., 2015). Both victims and perpetrators of IPV are significantly more likely to have not only witnessed family violence in childhood but also adopted normative beliefs toward physical partner violence (Bensley, Van Eenwyk, & Wynkoop Simmons, 2003; Ernst et al., 2009; Reyes et al., 2015).
Research on IPV trauma among pregnant and parenting women has found IPV negatively affects parenting outcomes, such as warmth, sensitivity, and responsive caregiving, and child outcomes, such as emotional and behavioral development (Carpenter & Stacks, 2009; Insetta et al., 2015; Levandosky & Graham-Bermann, 2000). In our study, alternatives considered instead of physical punishment on children were significantly fewer among pregnant adolescents who were perpetrators of physical assault or who reported reciprocal physical assault than those who were neither perpetrator nor recipient. These results were also lower than those reported for other samples of parenting adolescents (Barnet, Liu, DeVoe, Alperovitz-Bichell, & Duggan, 2007; Woods et al., 2003). Studies have found female parents who experience and harbor normalized beliefs toward domestic violence are more likely to report using physical and psychological disciplinary practices with their children (Kelleher et al., 2008; Lansford, Deater-Deckard, Bornstein, Putnick, & Bradley, 2014).
As perpetrating or participating in reciprocal IPV is associated with adverse outcomes among pregnant adolescents, interventions are crucial. The CDC (2014b) listed several steps to prevent IPV, and the Substance Abuse and Mental Health Services Administration (SAMHSA; 2014) has developed the Trauma-Informed Care Protocol (TIP) to help behavioral health service providers effectively empower people exposed to trauma. IPV interventions specific to adolescents indicate the most effective interventions use trauma-informed and culturally sensitive care; engage the support of adults, such as teachers and parents; take place in multiple domains, such as in school and community settings; target dyadic communication and conflict management skills; address individual personalities and psychopathologies; and focus on different forms and kinds of IPV (De Koker et al., 2014; Langhinrichsen-Rohling & Turner, 2012; O’Leary & Slep, 2012; Ward, McMahon, & Ingram, 2006).
The results of the current study underscore a need for interventions to acknowledge cultural diversity and social perceptions and behaviors pregnant adolescents maintain in managing conflicts with their partners and children. The high rate of IPV perpetration among African American pregnant adolescents underscores the need to take into consideration cultural perspectives in designing interventions to reduce health disparities. Culturally sensitive interventions must both prevent IPV among adolescents and promote healthy dating communication and behavior. This study reveals IPV prevention programs tailored to pregnant adolescents should address risk factors such as substance use and depression, as well as cultural norms and beliefs associated with gender- and race-based influences.
Study Limitations
This study has several limitations, which should be noted. First, assessments relied on self-report, which can be influenced by social desirability bias. In addition, participants in this program came from a single urban community, limiting generalizability. Despite these limitations, this study had a larger sample size compared with previous studies and also simultaneously examined multiple risk and protective factors. The findings of the study emphasize the importance of addressing IPV among pregnant adolescents.
Clinical Implications
This study makes an important contribution by examining IPV perpetration by pregnant adolescents and the associated risk factors. Whereas prior studies have assessed IPV within adolescent relationships or involving pregnant women (Breiding et al., 2008; Renner & Whitney, 2012), few have examined the role of the pregnant adolescent as perpetrator. Results of this study reinforce the need for interventions during pregnancy that will help pregnant adolescents develop the competencies and skills they need to protect against negative health and birth outcomes (NIJ, 2013), postpartum abuse (Harrykissoon et al., 2002; Martin, Mackie, Kupper, Buescher, & Moracco, 2001; Wiemann et al., 2000), and parental aggression against the child (Kelleher et al., 2008; Lansford et al., 2014). In addition, as studies indicate IPV during pregnancy may lead to neonatal death (WHO, 2012a, 2012b), addressing IPV during pregnancy as a way of reducing health disparities is crucial.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Department of Health and Human Services, Office of Adolescent Pregnancy Programs (OAPP; APHPA 006069), Harris County Commissioners Court, and the O’Neil Foundation.