
Abstract
Recent literature on exposure to domestic violence (DV) highlights the need for increased understanding of the dynamics of domestic violence and abuse (DVA). The current aims were to explore whether two separate dimensions, physical and psychological DVA, were evident in adult children’s reports of their exposure to DVA in their family of origin, and whether these dimensions affected psychological well-being and perceived satisfaction with emotional support (hereafter referred to as social support satisfaction). Young adults (N = 465, aged 17-25, 70% female) reported their experiences of DVA as perpetrated by their parents/caregivers, as well as psychological well-being and social support satisfaction, in an online survey. Using confirmatory factor analysis (CFA), we verified the presence of a two-factor model (physical and psychological DVA). Hierarchical linear regression analysis demonstrated the differing impact of these two factors: Specifically, although exposure to psychological DVA (domestic abuse [DA]) was related to reduced psychological well-being, there was no significant effect of exposure to physical DVA (DV). However, mediation analysis suggested the presence of a suppression effect; there was a magnification of the negative relationship between exposure to psychological DA and social support satisfaction when exposure to physical DV was accounted for. Although findings are preliminary, they provide strong evidence to support theoretical arguments regarding the need for future research to conceptualize exposure to DVA in terms of both physical and psychological dimensions. Our findings also highlight that to improve service response and provide effective interventions, it is essential to include exposure to psychological DA in risk assessments of such young adults.
Keywords
Research over the last two decades has clearly established that child exposure to domestic violence and abuse (DVA) can have a negative impact on children’s cognitive, emotional, behavioral, and social functioning (Holt, Buckley, & Whelan, 2008), which can continue into adulthood (Cater, Miller, Howell, & Graham-Bermann, 2015; Naughton, O’Donnell, & Muldoon, 2015). To date, quantitative research has tended to focus on exposure to the more clearly definable physical aspect of DVA (Haselschwerdt, 2014); however, recent qualitative research suggests that the children are exposed to a wide range of types of DVA (Haselschwerdt et al., 2019). As such, although physical domestic violence (DV) is important, the nonphysical aspect (hereafter referred to as psychological domestic abuse [DA]) may also be imperative to our understanding of child adjustment (Callaghan, Alexander, Sixsmith, & Fellin, 2018; Izaguirre & Calvete, 2015). Grych and Hamby (2014) have argued that our understanding of phenomena is limited by how we conceptualize it. This suggests a need to more fully understand the complex phenomenon, that is, child exposure to DVA. For example, to the best of our knowledge, there is no quantitative research within the exposure to DVA literature (hereafter termed exposure literature) examining whether or not exposure to psychological and physical DVA are in fact two distinct dimensions.
Recent theoretical arguments (e.g., Haselschwerdt, 2014; Haselschwerdt et al., 2019) suggest a need to further our understanding of the impact of child exposure to various types of DVA on adjustment. Although Haselschwerdt et al. (2019) suggest that children are indeed exposed to a wide variety of forms of DVA, there has been a tendency to conceptualize child exposure as a physical violence model (Katz, 2015). Furthermore, given the overreliance on the physical model for assessing the risk of those exposed to DVA (Naughton, O’Donnell, Greenwood, & Muldoon, 2015), it is essential that we explore whether there is evidence to support that exposure to the physical dimension of DVA contributes to reductions in well-being over and above those explained by exposure to the psychological dimension.
In addition, to the best of our knowledge, quantitative research on child exposure has not yet considered the possibility that different dimensions of DVA might also affect social and psychological functioning in different ways. For example, as psychological DA is associated with social isolation, both for adult victims (Goodman & Smyth, 2011) and the children within such families (Levendosky, 2013), it is plausible to suggest that exposure to the psychological dimension might have an effect on young adults’ satisfaction with available social support that exposure to the physical dimension does not. The overarching aim of the current study was, therefore, to investigate whether there were two distinct dimensions of child exposure to DVA as experienced by young adults and whether such dimensions affected differently on different psychosocial outcomes.
In the current study, exposure to DVA refers to young adults’ (aged 17-25) perception of the occurrence of intraparental DVA in their homes, specifically where the perpetrator and the victim are the person’s parents/caregivers. Whereas physical DV encapsulates behaviors such as hitting, choking, kicking, hair pulling, and threatened or actual use of a deadly weapon (knife, gun), psychological DA is conceptualized broadly to include verbal abuse (shouting, screaming, name calling), emotional abuse (humiliation, intimidation), controlling, isolating, damage to belongings, and purposeful harming of a pet (Edleson, Shin, & Armendariz, 2008). In the general DVA literature, psychological and physical violence are established as two intercorrelated, yet distinct, pathological phenomena (Kelly, 2004). However, although there is an emerging cognizance of the importance of the power dynamics in which exposure to physical DV may occur—specifically whether aversive stimuli are or are not used by one parent to control the other, referred to as coercive control (Haselschwerdt, 2014; Jouriles & McDonald, 2015)—there is scant research that explores whether or not exposure to psychological DA, in the absence of physical DV, has consequences for children or indeed for adult children.
Thus far, there is limited literature on the differing effects of physical and psychological DVA. Tschann et al. (2008) identified that increased emotional distress (depression, anxiety, and anger) and negative appraisals were both associated with nonviolent parental conflict but not interparental physical violence. Furthermore, Gonzalez, MacMillan, Tanaka, Jack, and Tonmyr (2014) investigated the differing outcomes for children below 15 (Mage = 6.05 years). Operationalizing exposure to subtypes of DVA (direct physical, indirect physical, and emotional) and also child functioning (internalizing/externalizing) as dichotomous variables (present/absent) based on child welfare workers reports, they found that exposure to both psychological and physical DVA resulted in the greatest risk to child well-being. In addition, Litrownik, Newton, Hunter, English, and Everson (2003) investigated the impact of exposure to family aggression (inclusive of all “grown-ups in the house,” p. 63) in a longitudinal study on young children. Using single items to record child reports of physical and psychological aggression in the family, they identified that where both child and mother reported the occurrence of physical family aggression at baseline (age 4), depression/anxiety was more likely in the child at follow-up (age 6). Child reports of psychological forms of aggression alongside mothers’ reports of physical aggression within the family at age 4, however, predicted aggressive behaviors at age 6.
These studies highlight a need to account for exposure to both dimensions of DVA on child/young adult adjustments. This is consistent with a growing recognition not only within the broader DVA literature (Kelly, 2004; Sullivan, 2013) but also emerging within the qualitative exposure literature (Callaghan et al., 2018; Katz, 2015), of the detrimental impact of the psychological dimension of DVA. Indeed, the broader DVA literature highlights that psychological DA is the most common form of DVA and may occur in the absence of physical DV (Henning & Klesges, 2003; Sullivan, 2013). Furthermore, Callaghan et al. (2018) suggest that as father’s controlling behavior can extend to the children, they may be directly drawn into the dynamic of psychological DA, making it a particular concern.
Aims of the Current Study
To date, despite the recent theoretical concerns around psychological DA, the exposure to DVA literature has tended to assess DVA as typically reflecting physical DV (Artz et al., 2014; Haselschwerdt, 2014). However, Edleson et al. (2008) constructed the Child Exposure to Domestic Violence (CEDV) measure to incorporate exposure to both the physical and psychological dimensions of exposure. Yet both the original CEDV measure and adapted versions (e.g., Cater et al., 2015) operationalize CEDV as a unidimensional construct. The current study employs the Edleson et al. (2008) measure, adapted to be gender neutral, to assess exposure to DVA among a sample of young adults. This scale was chosen as it was developed specifically to capture children’s/adult children’s perceptions of their own exposure to DVA as opposed to parent’s/caregivers’ or other key informants’ perceptions. First and foremost, we aimed to establish whether there is empirical evidence for physical and psychological dimensions of DVA. Our second aim was to investigate the potentially different impacts of these two dimensions of DVA on two conceptually distinct outcomes: psychological well-being and social support satisfaction.
CEDV has been shown to affect various facets of psychological well-being (Artz et al., 2014). However, another centrally important and likely area for DVA to affect is in relation to social support satisfaction. Indeed, in the context of child exposure to violence, social support is considered the most frequently studied protective factor (Grych, Hamby, & Banyard, 2015). However, within the exposure literature to date, social support has been investigated as a moderator (i.e., the impact of social support on the strength of the relationship between exposure to DVA and outcomes; for example, Tajima, Herrenkohl, Moylan, & Derr, 2011) or a mediator (i.e., how social support explains the relationship between exposure to DVA and outcomes; for example, Owen, Thompson, Shaffer, Jackson, & Kaslow, 2009). As such, to date, there is a scarcity of literature that investigates social support directly as an outcome, that is, studies that examine the direct effect of exposure to DVA on levels of social support. Furthermore, Ford et al. (2014) established in a longitudinal study that adverse childhood experiences (including exposure to DVA) predicted reduced levels of social support in adulthood. In addition, Sperry and Widom (2013) suggest a need to orient to how child maltreatment affects the level of perceived social support. Thus, in the current study, orienting to the theoretical arguments that link trauma to social support (Muldoon & Lowe, 2012), we explore the impact of exposure to both physical and psychological dimensions of DVA on young adults’ reports of their perceived satisfaction with their current social support.
To further our understanding of the impact of CEDV on young adults, we propose the following two hypotheses.
Method
Participants and Procedure
Following ethical approval, in 2014, an email was sent to the student population of an Irish university, inviting students aged between 17 and 25 to participate in an online study titled “Social factors and well-being of young adults who may have experienced traumatic life events.” As an acknowledgment of their time, participants were given an opportunity to be entered into a prize draw for an Amazon voucher valued at £40. Participants responded to the following measures: CEDV, general health questionnaire, social support satisfaction questionnaire, and demographics, in that order. Although a total of 465 students completed the CEDV measure (the first measure in the survey), 23.66% failed to complete all measures, resulting in a final sample size of 355. There was no significant group difference, t(463) = −1.60, p = .11, in the level of reported CEDV between participants who completed all measures (n = 355) and those who dropped out (n = 110; (Naughton, O’Donnell, & Muldoon, 2015)). Participants (n = 355) had a mean age of 20.07 years (SD = 2.08 years); 70.6% of them identified as female, ethnicity was not sought as the student population is predominantly White Irish.
Measures
Demographics
As a measure of socioeconomic status (SES), participants were asked whether they were in receipt of income-assessed government funding to attend university. As the young people may not be familiar with the intimate details of their parents’ income and this funding is based on a governmental assessment of such, this was an appropriate operationalization of SES for the current study; 53.5% of participants indicated that they were not in receipt of government funding, and therefore were classified as being from higher SES backgrounds. Participants were also asked to record their age and gender.
CEDV
Edleson et al.’s (2008) validated measure for CEDV was used to assess (adult) child exposure to DVA. Whereas the original scale contained three sections, in the current study, nine items from Section 1 were used. These nine items were adapted to capture DVA as perpetrated by either or both the participant’s parents/caregivers, rather than assessing father-only perpetration as in the original measure. Items are available in Table 1. This measure has previously been validated with U.S. children (10-16 years) and also adapted to measure retrospective CEDV in Swedish young adults (Cater et al., 2015). Haselschwerdt (2014) highlights this measure as having the potential to tap into the different types of CEDV; however, to the best of our knowledge, all published studies to date have used the measure as a single dimensional measure with higher total scores indicating higher levels of exposure. Participants rated nine items on a five-point Likert-type scale (0 = never, 1 = rarely, 2 = sometimes, 3 = often, 4 = a lot) indicating the frequency of occurrence of the behavior. As we know that young adults can continue to be exposed to intraparental DVA (Haselschwerdt et al., 2019), we did not limit their exposure to childhood (below 18 years) but rather measured lifetime exposure. Briefly, participants indicated whether their exposure had occurred within the last 6 months (ongoing) or previously (historical; see Naughton, O’Donnell, & Muldoon, 2015) Psychometric details for CEDV are included in the “Results” section.
Individual Items Which Cluster on the Psychological Factor, Physical Factor, and Excluded Item With Means and SD.
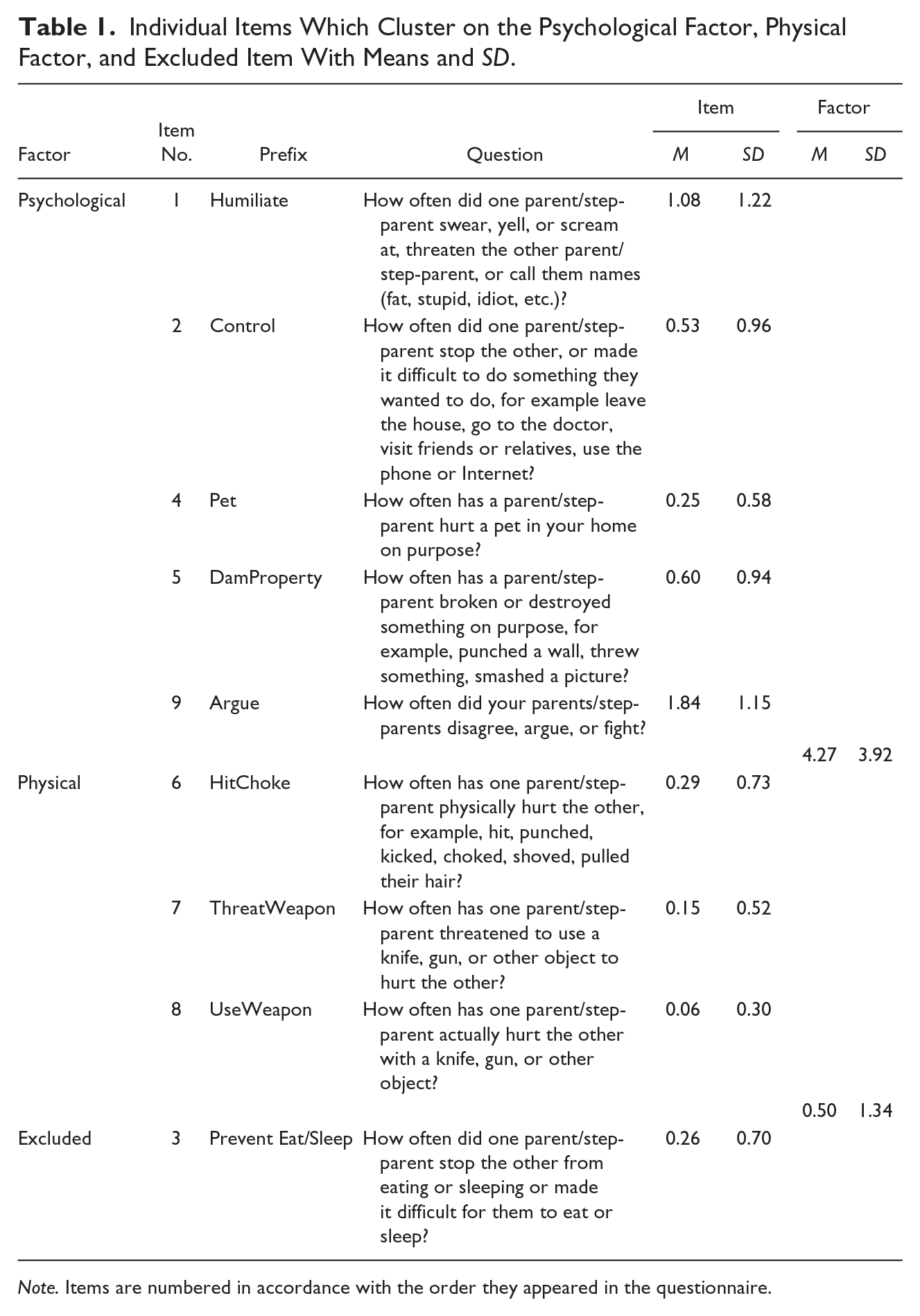
Note. Items are numbered in accordance with the order they appeared in the questionnaire.
General Health Questionnaire (GHQ)
Goldberg’s (1992) 12-item measure, GHQ, has been used extensively in population-based studies to assess disruption in normal psychological functioning (Goldberg et al., 1997). Participants rated 12 items on a four-point Likert-type scale (from 1 = not at all to 4 = a lot) to indicate how much each item related to them. Negative items were reverse scored. The mean was calculated to give a range of 1 to 4, with higher scores indicating higher levels of psychological well-being. Reliability was excellent, with a Cronbach’s alpha of .91 for the current study.
Social Support Questionnaire (SSQ6)
Sarason, Levine, Basham, and Sarason’s (1983) six-item SSQ measure was used to assess current satisfaction with perceived emotional support. It is of note that the term social support satisfaction is used to denote this construct throughout the article. The measure contains two sections. In Section A, participants were asked to name up to four individuals from whom they could count on obtaining emotional support. For example, “Please name the people you can really count on help you feel relaxed when you were under pressure or tense?” Then, in Section B, they rated on a seven-point Likert-type scale (from 1 = very dissatisfied to 7 = very satisfied) how satisfied they were with this perceived available emotional support. In this study, the Section B—SSQ6 items were used to denote social support satisfaction. The mean was calculated to give a range of 1 to 7, with higher scores indicating higher social support satisfaction. Reliability was excellent, with a Cronbach’s alpha (internal consistency) of .92.
Analytic Strategy
The findings are presented in two distinct parts. Initially, CFA was employed to investigate Hypothesis 1. CFA tests the fit of the current data to a hypothesized model. In accordance with Jöreskog and Sörborn’s (1984) “alternative modeling strategy,” separate CFAs were undertaken for three proposed models for the CEDV variable: Model A, a single-factor model; Model B, a theoretically driven two-factor model; and Model C, a data-driven, adjusted two-factor model. The established statistical evidence for the presence of two distinct dimensions; physical and psychological DVA facilitated the testing of Hypothesis 2. In Part 2, hierarchical linear regression was employed to investigate how exposure to both physical and psychological DVA impact on both psychological well-being and social support satisfaction. This also enabled us to comment on the validity of a two-dimensional approach to understanding CEDV. Finally, we used PROCESS Model 4 (Hayes, 2013) to further explore the findings from the linear regression analysis; that is, the idea that exposure to physical DV exerted a suppression effect on the relationship between exposure to psychological DA and social support satisfaction.
Results
Part 1. Evidence for a Two-Dimensional Model of Adult Children’s Exposure to DVA
In line with our first hypothesis, we undertook a CFA using AMOS, SPSS statistical software to determine whether a single- or two-factor model of CEDV best fit the current data. We initially tested Model A (single factor, with all nine items) for goodness of fit. As predicted, this model was a poor fit for the current data (relative chi-square [CMID/DF] = 14.10, comparative fit index [CFI] = 0.89, root mean square error of approximation [RMSEA] = .18). As the one-factor model was a poor fit, we proceeded to test the first two-factor model, a theoretically derived model (Model B). Here, consistent with theoretical arguments, the nine items were loaded on two distinct but correlated factors, namely, psychological and physical CEDV. Fit estimates for Model B were in the expected direction, but did not have an acceptable model fit (CMID/DF = 6.62, CFI = 0.93, RMSEA = .10).
On further investigation, the modification indexes (M.I.) indicated that Item 3 (“prevent eat/sleep”), which was clustered on the psychological factor, also correlated with the physical factor (M.I. = 6.33); this suggests that this item loads similarly on both factors. Modification indexes also indicated that correlations existed between error terms of two items, which loaded on the psychological factor (Item 1, “humiliate” and Item 9, “argue”; M.I. = 6.99) and two items that loaded on the physical factor (Item 7, “threaten weapon” and Item 8, “use weapon”; M.I. = 9.9). Because the items tap into similar constructs, we assumed that the correlations reflected nonrandom measurement error stemming from content overlap. Taking account of these findings, we then tested the fit of the adjusted two-factor eight-item model (Model C), in which the error terms were allowed to be correlated and Item 3 was dropped. This adjusted interrelated two-factor model had good fit estimates (CMID/DF = 2.32, CFI = 0.99, RMSEA = .05), verifying that two factors underlie the higher order CEDV variable. Fit estimates are presented in Table 2, while Figure 1 illustrates the best fit model (Model C). As predicted the two factors were intercorrelated (.81).
Goodness-of-Fit Estimate Values for Alternative Models in the CFA Together With Recommended Values Denoting a Good Fit.

Note. CMID/DF = relative chi-square; RMSEA = root mean square error of approximation; CFI = comparative fit index.
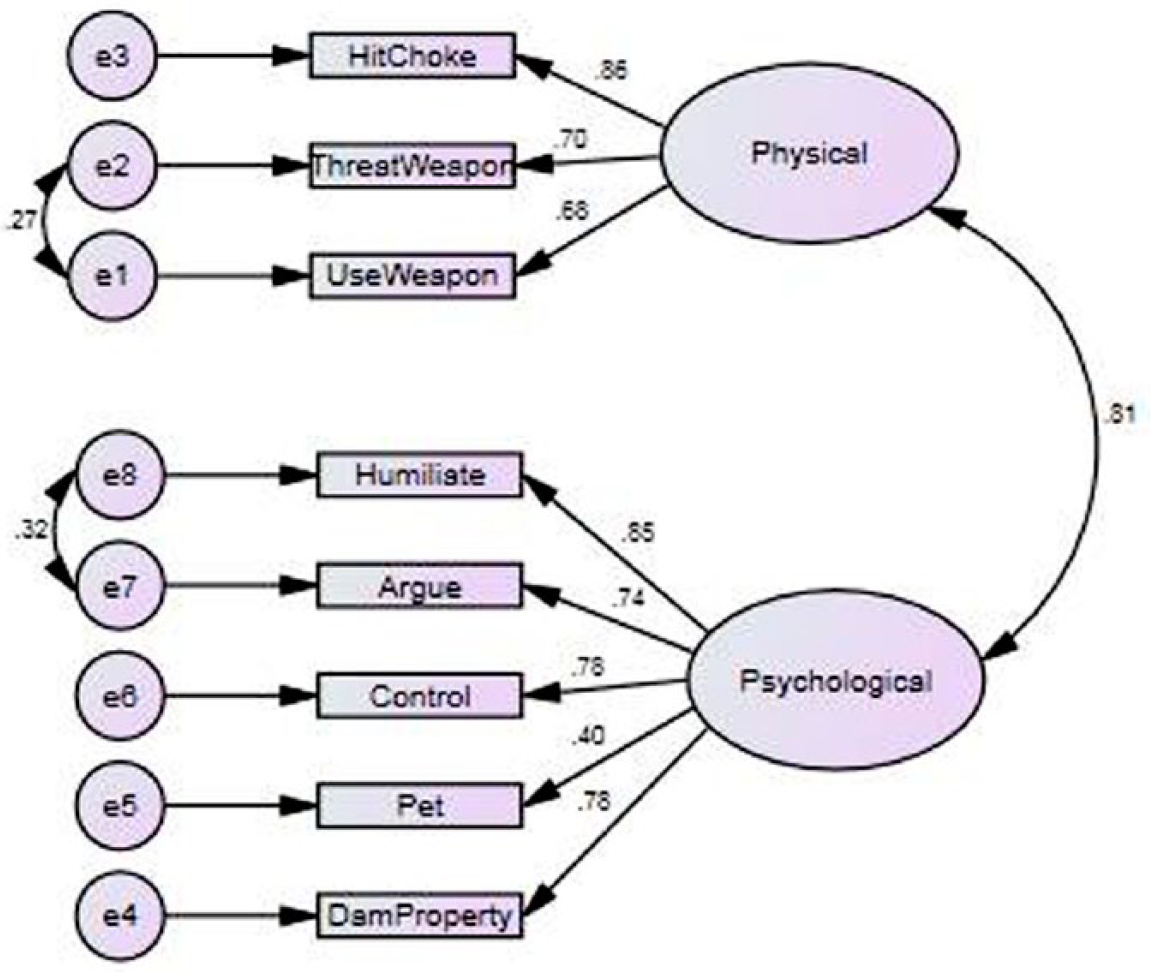
Diagram of the confirmatory two-factor for Model C, with standardized regression coefficients and correlations values.
Reliability was analyzed through Cronbach’s alpha. Both exposure to physical DV (α = .76) and psychological DA (α = .85) demonstrated very good reliability. Items were totaled to give final scores between and 0 and 12 for exposure to physical DV and between 0 and 20 for exposure to psychological DV, with high scores indicating high levels of exposure. However, as low scores (<3) of exposure to psychological DA were regarded as more consistent with exposure to low-level conflict and not psychological DA, exposure to psychological DA was defined as a score of 3 and greater; 21.6% of participants (n = 92) reported exposure to physical DV (defined as a total score of 1 or more), while 55.7% (n = 259) reported exposure to psychological DA (defined as a total score of 3 or more).
Part 2. Exposure to Psychological and Physical Domestic Violence and Psychological Well-Being and Social Support Satisfaction
To determine the association between the variables of interest, Pearson correlations were performed. Descriptive statistics and Pearson correlations are presented in Table 3.
Pearson Correlations, Means, Standard Deviations for Exposure to Psychological DA, Exposure to Physical DV, Psychological Well-Being, Social Support Satisfaction, and SES.

Note. Exp. = exposure; DA = domestic abuse; DV = domestic violence; Sat. = satisfaction; SES = social economic status.
p < .001. **p < .01. *p < .05.
In line with Hypothesis 2, two separate hierarchical linear regression analyses were performed, with criterion variables of psychological well-being and social support satisfaction, respectively. To control for the possible impact of SES on outcomes, this variable (coded 0 = lower SES, 1 = higher SES) was added in Step 1. As the correlations between gender and age with predictor and criterion variables were nonsignificant, they were not included in the regression model. As we did not have an a priori hypothesis as to which of the underlying factors (psychological or physical) of CEDV would explain unique variance, both factors were added in Step 2 using forced entry. Furthermore, as the variance inflation factors (VIFs) for all variables were less than 2, multicollinearity was not an issue. Results are presented in Table 4.
Hierarchical Multiple Regression Analysis Predicting Psychological Well-Being (GHQ) and Social Support Satisfaction (SSQ6) Using Exposure to Psychological and Physical DVA.
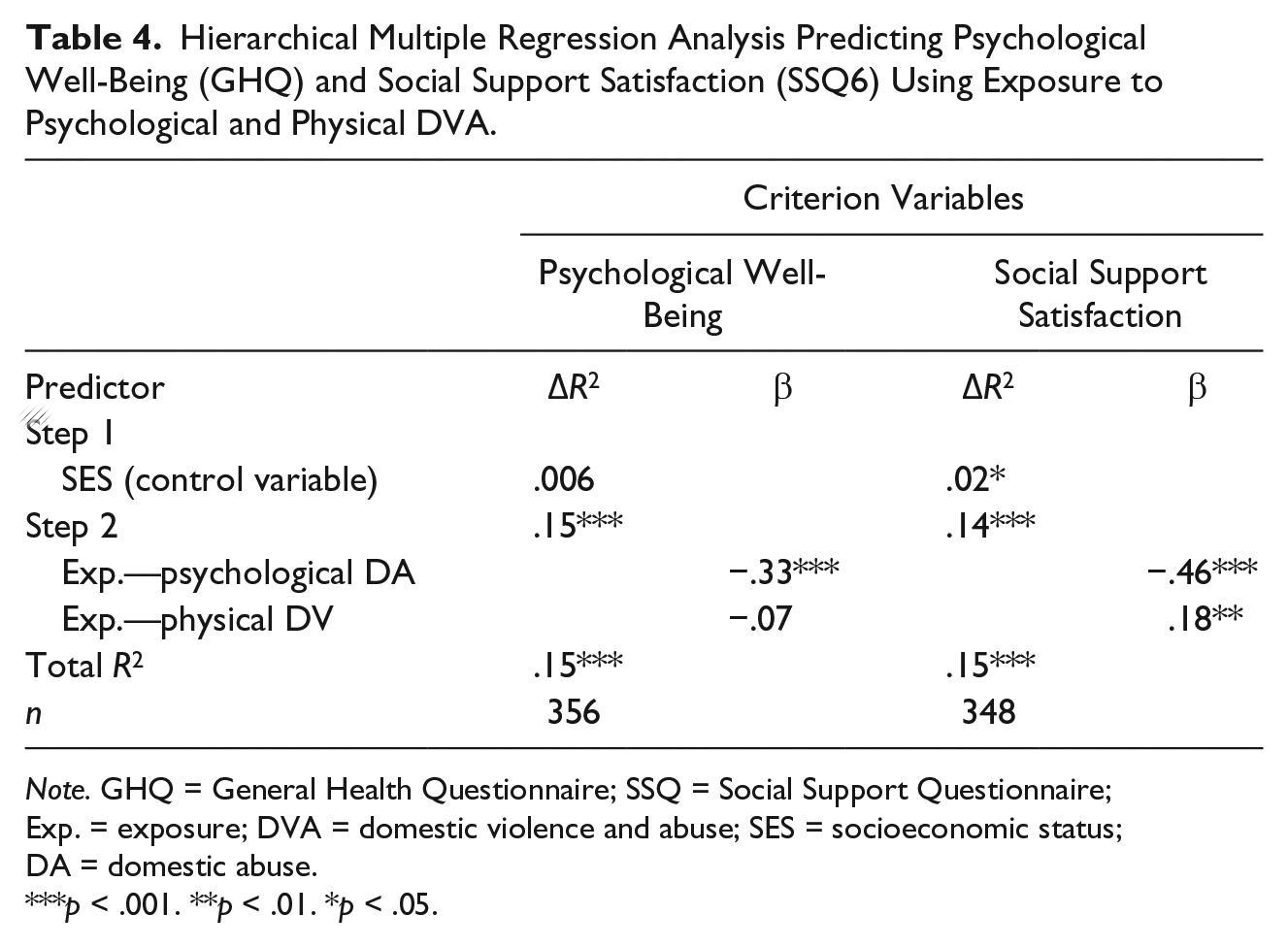
Note. GHQ = General Health Questionnaire; SSQ = Social Support Questionnaire; Exp. = exposure; DVA = domestic violence and abuse; SES = socioeconomic status; DA = domestic abuse.
p < .001. **p < .01. *p < .05.
Exposure to psychological DA (β = −.33, p < .001) was the sole significant predictor and explained 15% of the variance in psychological well-being, F(2, 352) = 30.34, p < .001. Higher levels of exposure to psychological DA predicted reduced levels of psychological well-being. There was no unique predictive effect for exposure to physical DV on psychological well-being (β = –.07, p > .05).
SES (β = .15, p = .02) explained a significant 2% of the variance (F(2, 346) = 3.98, p = .02) for the criterion variable social support satisfaction. Higher SES predicted increased levels of social support satisfaction. Exposure to psychological (β = –.46, p < .001) and physical (β = .18, p = .008) DVA explained 14% of the variance in social support satisfaction (F(2, 344) = 27.87, p < .001). Higher levels of exposure to psychological DA predicted reduced levels of social support satisfaction. However, as the beta value for exposure to physical DV was positive, this suggests that when controlling for exposure to psychological DA, increased levels of exposure to physical DV predicted an increase in levels of social support satisfaction.
To further elucidate the findings of the hierarchal linear regression for social support satisfaction, a mediation analysis using PROCESS model 4 (Hayes, 2013) was conducted. This was the preferred statistical tool as 78.4% of participants reported no exposure to physical DV, thus limiting the utility of the inclusion of an interaction term in multiple linear regression models.
Bootstrapping was applied as this makes no assumptions about the normality of the sampling distribution and reduces the likelihood of type 1 error (Preacher & Hayes, 2004). Bootstrapping involved drawing 10,000 random samples from the data pool to estimate each pathway’s effects, with computed bias-corrected and accelerated 95% confidence intervals (CIs) determining the significance of each pathway. Results are presented in Table 5, while the model is presented in Figure 2.
Parameter Estimates of the Model Examining the Mediating Role of Exposure (Exp.) to Physical DV in the Relationship Between Exposure (Exp.) to Psychological DA and Outcome Social Support Satisfaction.

Note. Regression weights a, b, c, and c’ are illustrated in Figure 2. The 95% CI for a × b is obtained by the bias-corrected bootstrap with 10,000 random resamples. Exposure to psychological DA is the independent variable, exposure to physical DV is the mediator, and social support the outcomes. R2 is the proportion of variance explained. CI [lower bound, upper bound] of 95% confidence interval. DA = domestic abuse; DV = domestic violence; CI = confidence interval; Exp. = Exposure; = Sat. = satisfaction
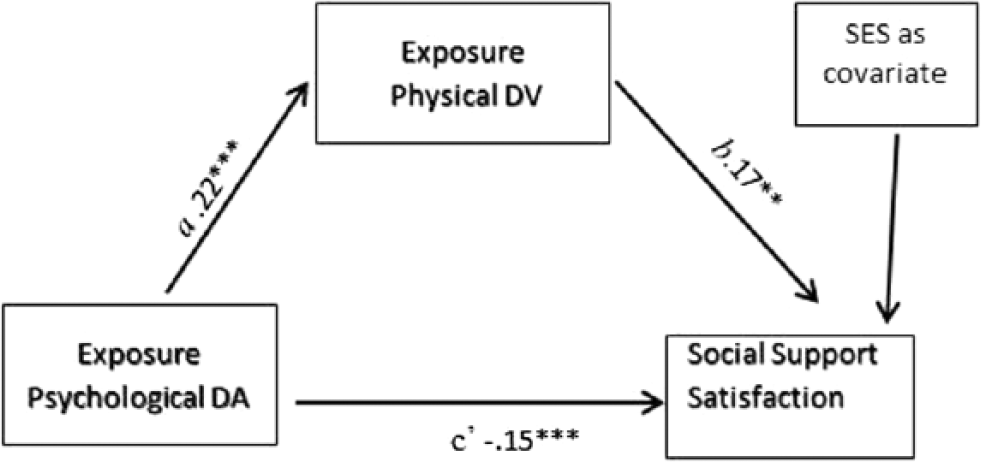
Suppression effect of exposure to psychological DA on social support satisfaction by exposure to physical DV.
As SES was shown to contribute to variance in social support satisfaction in the hierarchical linear regression analysis, it was added as a covariate to the mediation model. Exposure to psychological DA predicted increased exposure to physical DV (B = .22, p < .001), which in turn predicted increased social support satisfaction (B = .17, p = .008). The direct effect was negative (B = –.15, p < .001), with exposure to psychological DA predicting reduced levels of social support satisfaction. However, as the indirect effect was positive (B = .04, 95% CI = [0.01, 0.07]), the statistical adjustment for exposure to physical DV within the model resulted in an increase in the predictive power of exposure to psychological DA for social support satisfaction. This is referred to as a suppression effect, which is statistically similar, though conceptually different, to a mediation effect. It occurs when you have incongruent mediation—opposite signs for direct and indirect effects (MacKinnon, Krull, & Lockwood, 2000)—as in the current findings, where there is a negative direct effect and positive indirect effect (see above). As such, within the current data set, for the young adults who reported high levels of exposure to psychological DA, those who also reported higher levels of exposure to physical DV fared better in terms of perceived social support satisfaction than those who reported lower levels of physical DV.
Discussion
To date, studies based on the CEDV measure (Edleson et al., 2008), including adaptations, have conceptualized CEDV as a unitary construct, with higher total scores indicating higher levels of exposure. However, consistent with our first hypothesis, our findings evidence two distinct dimensions of young adults’ reported experience of their exposure to DVA. These two distinct, yet related, underlying factors can be thought of as physical and psychological dimensions of DVA. We suggest that this is both a novel and important finding. The verification of two statistically distinct factors facilitated the analysis of the differing impact of being exposed to both the physical and psychological dimensions of DVA. The two dimensions appear to drive different psychosocial outcomes. We argue that this more complete and nuanced understanding of the nature of CEDV will facilitate our longer term understanding of the consequences of exposure to DVA.
In line with Hypothesis 2a, which proposed a differing relationship between the underlying factors and psychological well-being, the patterns within our data suggest that it was exposure to the psychological dimension of DVA that explains the reductions in psychological well-being for young adults, with no unique variance explained by the physical dimension when accounting for the impact of the psychological dimension.
The establishment of the psychological dimension as the driving factor in reduced psychological well-being is consistent with the broader DVA literature, which highlights the deleterious impact of psychological DA on victims (Kelly, 2004). The current findings are also in line with previous exposure literature. For example, Tschann et al. (2008), using the Revised Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996), identified that parental reports of nonviolent parental conflict, but not interparental violence, were associated with adolescents’ increased emotional distress.
A possible explanation for the current findings may be the higher levels of exposure to the psychological factor when compared with physical factor. However, our findings were consistent with those found by Cater et al. (2015) who, with a similar aged population, also used an adapted form of the CEDV instrument to capture child exposure. Their young adults also reported higher levels of exposure to the individual items that cluster on the current study’s psychological factor, when compared with the individual items that cluster on the current study’s physical factor of CEDV.
Consistent with Hypothesis 2b, there would be a differing relationship between the distinct dimensions (physical and psychological) and social support satisfaction. Our findings suggest that although exposure to both dimensions contributed to variations in young adults’ levels of social support satisfaction, exposure to the psychological dimension predicted reduced levels of social support satisfaction, whereas exposure to the physical dimension predicted increased levels of social support satisfaction while accounting for the psychological dimension and SES. Reinforcing this finding, we established a suppression effect; when we accounted for exposure to physical DV, the negative impact of exposure to psychological DV on the levels of social support satisfaction was magnified. Thus, in terms of levels of social support satisfaction, exposure to increased levels of physical DV can be said to reduce the negative impact of exposure to increased level of psychological DA.
Although we cannot address the underlying mechanism that may explain these findings based on the current data, it is possible that the clearly visible parameters that underlie physical DV (kicking, punching, use of weapon) render it easier to make sense of and categorize as an unacceptable behavior, therefore facilitating disclosure and increased levels of social support satisfaction. However, as psychological DA lacks physical parameters, it may be more difficult to comprehend as abusive, and indeed less amenable to understanding from others. This argument is consistent with findings from a linked qualitative study (Naughton, O’Donnell, & Muldoon, 2015), which identified that the occurrence of extreme physical violence facilitated the young people to disclose the occurrence of DVA in their homes and enabled them to seek external help.
Although the current findings establish that exposure to psychological DA explains 14% and 16% of variations in psychological well-being and social support satisfaction, respectively, previous research has established other constructs that may account for the remainder of the variance. For example, exposure to a wide range of violence including community violence, direct childhood abuse, and sibling abuse, also contribute to maladjustments (Margolin, Vickerman, Oliver, & Gordis, 2010). Furthermore, mediators such as young adults’ family identification (i.e., their perceived embeddedness within the family group; Naughton, O’Donnell, & Muldoon, 2015), threat appraisal (Grych, Jouriles, Swank, McDonald, & Norwood, 2000), parental warmth (Miller, Cater, Howell, & Graham-Bermann, 2015), and maternal mental health (Miranda, de la Osa, Granero, & Ezpeleta, 2013) have all been identified as underlying processes in the link between exposure to DVA and adjustments.
Limitations
This study’s primary focus was to demonstrate the underlying factors of DVA and the consequences of exposure to both physical and psychological DVA; thus, it was imperative to limit the scope of this study to focus solely on the psychological and physical factors of the higher order CEDV variable. The authors do wish to indicate the need to interpret these results with some caution. The current study captured both ongoing and past exposure to DVA so may be subjected to recall bias (Hardt & Rutter, 2004). The cross-sectional design precludes demonstration of causal effects, therefore, the current findings should be considered preliminary.
Diversity and Culture
Participants in the current study were predominantly White Irish Catholic, so analyses of ethnic group differences were not possible. It is also worth noting that how Irish young people are affected by exposure to both physical and psychological DVA, and how this affects their perceived satisfaction with social support satisfaction, may be culturally distinct. As such, replications of the study with diverse populations are warranted to determine the generalizability of the current study’s findings. Although previous studies have found gender differences in outcomes for young adults (Cater et al., 2015), no such patterns were identified within the current data set (Naughton, O’Donnell, & Muldoon, 2015). Furthermore, in the current study, SES explained 2% of the variation in social support satisfaction, and although statistically significant, 2% may not hold practical significance. The current study accessed SES based on the young people’s receipt of government assisted funding to attend university. Future research may benefit from increased attention to the young people’s social environment including SES.
Research Implications
Following from the above stated limitations, it is, therefore, important that future studies should investigate the generalizability of the present results by investigating the differing impacts of exposure to both physical and psychological DVA for younger children, at-risk groups and community groups of various culture backgrounds, and in the context of other adverse childhood experiences. Our novel findings do extend previous literature and serve to clarify less conclusive results regarding the overall impact of child exposure to DVA (Kitzmann, Gaylord, Holt, & Kenny, 2003). The current findings evidence two distinct dimensions of young adults’ reported experience of their exposure to DVA; importantly, they highlight how the differing impact of the underlying factors can vary between distinct psychosocial outcomes. The patterns within our data, therefore, clearly suggest a need for future research to account for the effect of exposure to both physical and psychological DVA when investigating the impact of this phenomenon. However previous quantitative child exposure literature has tended to operationalize child exposure as physical DV only and where psychological DA is included as a unidimensional construct, as, for example, in the CEDV instrument (Edleson et al., 2008). Our findings, however, are consistent with recent concerns raised by Grych and Hamby (2014). In their contribution to the advancement of the measurement of violence, they highlight methodological issues; for example, their concerns on the ability of total scores on self-report violence instruments to fully capture the construct under investigation. Therefore, the current findings augment Grych and Hamby’s recommendations that researchers desist from oversimplifying complex phenomena such as DVA.
The verification of the psychological dimension as the driving force in reduced psychological well-being also has implications for future research. Follingstad (2011) highlights the difficulty that academic researchers have in defining and conceptualizing psychological DA. Perhaps, because of this, previous research in this area has tended to focus on exposure to physical DV (Jouriles & McDonald, 2015). Sullivan (2013) recommends that the broader DVA literature places a “critical foci” on psychological DA and the co-occurrence of different types of DVA (p. 123). The current findings suggest this is also an important issue when considering children’s exposure to DVA.
It is, however, also possible that the current findings do not hold for younger children. Vu, Jouriles, McDonald, and Rosenfield (2016), in a review of longitudinal studies, highlighted that the impact of child exposure on well-being increases with age. Future research is required to investigate the impact of exposure to both physical and psychological DVA across the life span. It is also imperative that future longitudinal studies further elucidate the suppression effect of exposure to physical DV on the association between exposure to psychological DV and social support satisfaction.
There is an onus on social scientific research to provide reliable and valid evidence to inform interventions to facilitate the recovery of children and young adults who grow up in homes affected by DVA. Grych and Hamby (2014) suggest that our understanding of a phenomenon is limited by how we conceptualize it. Consistent with theoretical arguments, the current findings suggest that it is essential that this complex phenomenon is not only conceptualized broadly (Haselschwerdt, 2014) but also not reduced to a unitary homogeneous construct (Grych & Hamby, 2014).
Clinical and Policy Implications
There is a need for increased awareness among practitioners and policy makers regarding the potential negative consequence of exposure to psychological DV. For example, much research in this area has highlighted the necessity for interventions to encourage the development of both peer relationships (Levendosky, Huth-Bocks, & Semel, 2002) and parent/child relationships (Owen et al., 2009) as protective factors for children who are exposed to DVA. The current findings suggest that low levels of exposure to physical DV, in conjunction with high levels of exposure to psychological DA, may be problematic in terms of young adults’ perceived satisfaction with social support. As such, young adults with exposure to low levels of physical but high levels of psychological DVA are arguably (at least) equally in need of such intervention as those who are exposed primary to physical DV. It is, therefore, essential that this specific population is not excluded by systems that prioritize exposure to physical DV in their risk assessments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.