
Abstract
Some research shows that sexual assault victimization is associated with increased engagement in risky sexual behavior (e.g., intercourse without use of a condom or contraceptives), whereas other research indicates sexual assault victimization is related to sexual aversion. The purpose of the current study was to examine whether posttraumatic stress symptoms, alcohol use, and sexual assertiveness mediated the relationship between adolescent/emerging adulthood sexual assault (ASA) and risky sexual behavior, and whether posttraumatic stress symptoms mediated the relationship between ASA and sexual aversion, among college women. A sample of 462 women from a Midwestern university completed online questionnaires assessing ASA, child sexual abuse (CSA), posttraumatic stress symptoms (i.e., intrusion, avoidance, hyperarousal, and dissociation), alcohol use, sexual assertiveness, risky sexual behavior, and sexual aversion. CSA was considered as a covariate in the mediation models. Results of mediation analyses showed that the relationship between ASA and risky sexual behavior with a new partner was partially mediated by greater alcohol use and lower sexual assertiveness and that the relationship between ASA and risky sexual behavior with a regular partner was partially mediated by greater alcohol use. Results of a model examining mediators of ASA and sexual aversion detected no significant mediators. Results suggest that college women with a history of ASA would benefit from psychoeducation on the effect of alcohol on sexual decision-making, as well as from sexual assertiveness skills training, to reduce potential risks associated with risky sexual behaviors, particularly with lesser known partners, including sexually transmitted infections and sexual revictimization.
Approximately 45% of college women report experiencing adolescence/emerging adulthood sexual assault (ASA; Krebs, Lindquist, Warner, Fisher, & Martin, 2009). Exposure to sexual assault victimization is associated with greater risk for a range of symptomatology including posttraumatic stress symptoms, depression, substance use, and sexual dysfunction (e.g., see Gidycz & Kelley, 2016 for a discussion). Research has also focused on the relationships between sexual victimization and sexual behaviors, including engagement in risky sexual behavior and sexual aversion. Given varying patterns of results across studies examining the relationship between sexual assault and sexual behavior, and the variety of sequelae of sexual assault experienced across women, it is important to identify mechanisms (e.g., mediators) that explain how sexual victimization is associated with these sexual behaviors (Rellini, 2008). Thus, the purpose of this study was to explore, in a sample of college women, whether posttraumatic stress symptoms, alcohol use, and difficulties with sexual assertiveness mediated the relationship between ASA and risky sexual behavior, and whether posttraumatic stress symptoms mediated the relationship between ASA and sexual aversion.
Risky sexual behavior refers to sexual behaviors that have a potential for impaired health and risk to safety (e.g., sexual activity without the use of a condom or while under the influence of substances). These behaviors can place women at greater risk for the development of sexually transmitted infections (STIs) and unintended pregnancies, two health concerns that are identified as top priorities for reduction among young adults (U.S. Department of Health and Human Services, Office of Population Affairs, 2010). Some research with college women shows that a history of sexual assault is associated with increased rates of risky sexual behavior (e.g., Littleton, Grills, & Drum, 2014; Testa, Hoffman, & Livingston, 2010). Previous research also points to the importance of the type of sexual partner when conceptualizing this behavior, such that sexual behavior with regular, versus new or just-met, partners have different correlates (e.g., Messman-Moore, Walsh, & DiLillo, 2010; Parks, Hsieh, Collins, Levonyan-Radloff, & King, 2009; Scott-Sheldon, Carey, & Carey, 2010). It is possible that mediators of the relationship between sexual victimization and risky sexual behavior are more salient in the context of behaviors with a stranger as compared with a regular partner. For example, Messman-Moore et al. (2010) found in a sample of college women that emotion dysregulation associated with child abuse predicted risky sexual behavior with a partner just met (i.e., a stranger), but not with a regular partner.
Sexual aversion refers to an inclination to avoid situations that may lead to sexual behavior. It is often conceptualized as a form of anxiety reflecting fear of perceived negative consequences of sexual behavior, and underlying impairments in interpersonal and sexual functioning (e.g., Staples, Rellini, & Roberts, 2012). Although it is less often studied in college women than is risky sexual behavior, prior research found a relationship between sexual assault and lower numbers of sexual partners (Merrill, Guimond, Thomsen, & Milner, 2003), which may be reflective of sexual aversion. It is important to identify variables that contribute to college women’s experience of sexual aversion or risky sexual behavior as healthy sexual functioning and experiences are important parts of women’s health and well-being. The college-aged years are a time when issues related to sexuality are often at the forefront due to the associated developmental stage (Higgins, Mullinax, Trussell, Davidson, & Moore, 2011).
It is reasonable to expect a variability in the sequelae of ASA across women (e.g., Campbell, Dworkin, & Cabral, 2009), including sexual behavior. Thus, there are likely mechanisms that explain how some women with a history of sexual assault experience sexual aversion and some experience increased risky sexual behaviors (Rellini, 2008). The identification of mediators of the relationships between ASA and these sexual behavior domains has implications for the development of interventions to prevent or reduce negative long-term effects of these behaviors (e.g., impaired interpersonal functioning, sexual dysfunction, increased risk for STIs, and sexual revictimization). Previous studies have examined distal, psychological mediators (e.g., alcohol use, depression, and trauma symptomatology), and proximal mediators (e.g., immediate sexual–emotional responses to sexual stimuli) of relationships between sexual abuse and a number of sexual health outcomes (e.g., George et al., 2014; Morokoff et al., 2009; Testa et al., 2010). Much of this research has focused on mediators of the relationships between sexual abuse and sexual revictimization (e.g., Kelley, Orchowski, & Gidycz, 2016; Messman-Moore et al., 2010; Testa et al., 2010), number of sexual partners (e.g., Merrill et al., 2003), or problems with sexual functioning (e.g., Rellini & Meston, 2011), or has examined these relationships in community samples (e.g., George et al., 2014; Morokoff et al., 2009). The current study contributes to this existing literature by identifying variables, which are amenable to intervention, associated with college women’s experiences of risky sexual behavior or sexual aversion.
Rellini (2008) outlined a theoretical model to explain how some women with a history of childhood sexual abuse (CSA) may experience “hypersexuality” (i.e., the tendency to engage in sexual activity in impulsive or risky situations, with an unknown partner, or without protection) or “hyposexuality” (i.e., problems with avoidance of sexual activities and inhibited desire, arousal, and orgasm). This model was used as a guiding framework in the current study to understand how women with a history of ASA may experience risky sexual behavior or sexual aversion. Rellini proposed that first- and second-order internal processes determine a woman’s subjective and physiological response to sexual stimuli (e.g., a sexual advance from a partner). Each order of processing is determined by cognitive, affective, and physiological variables that may be influenced by a woman’s previous experience of sexual assault. First-order processes are the immediate, implicit responses to sexual stimuli, and can include activation of an implicit sexual memory (e.g., of sexual assault). Second-order processes are affected by contextual information (e.g., mood, social norms, and sexual self-views). Both first- and second-order processes can be excitatory or inhibitory, and it is the summation of these responses that determine a women’s real-time response to sexual stimuli. Rellini (2008) purported that responses to sexual stimuli among women with a history of CSA may reflect hypersexuality or hyposexuality, via the effect of CSA on the first- and second-order processes.
It is reasonable to propose that the construct of hypersexuality is reflected in risky sexual behavior, and the construct of hyposexuality is reflected in sexual aversion. Based on Rellini’s (2008) model, in the context of sexual aversion, women with a history of sexual assault may have implicit sexual memories of the abuse that, when activated, are paired with negative affective (e.g., fear), cognitive (e.g., over-estimation of threat; “sex is dangerous”), and physiological (e.g., traumatic hyperarousal that may interfere with sexual arousal) responses. Alternatively, women with a history of sexual assault who engage in risky sexual behavior may have more difficulty with inhibitory processes and with the pairing of sexual stimuli with pleasure. For example, these women may be less able to inhibit the activation of sexually relevant thoughts, emotions, and behaviors related to sexual excitation. Difficulty with inhibition of intrusive sexual responses may lead to over-preoccupation with sex and higher engagement in sexual activities to cope with such responses (Rellini, 2008). Rellini reviewed support for this theoretical model in a series of studies examining responses to sexual stimuli in women with a history of CSA (see Rellini, 2008, for a discussion) and further proposed that this model be tested for survivors of sexual abuse experienced across the lifespan (e.g., ASA).
In short, Rellini’s (2008) model outlines the role of psychological and behavioral mechanisms that determine women’s response to sexual stimuli, which can result in sexual aversion or risky sexual behavior. Based on previous research and in line with this theoretical model, variables that may contribute to the relationship between ASA and sexual behavior that were considered in the current study include posttraumatic stress symptoms (i.e., intrusive experiences, avoidance, hyperarousal, and dissociation), alcohol use, and sexual assertiveness. Certainly, ASA is a traumatic experience that can be associated with posttraumatic stress symptoms including maladaptive cognitive, behavioral, and physiological responses (e.g., Gidycz & Kelley, 2016; Johnson, Murphy, & Gidycz, 2017; Walsh, Latzman, & Latzman, 2014). These symptoms may affect women’s responses to sexual stimuli, as sexual stimuli could serve as cues for the sexual trauma (e.g., sexual thoughts). Thus, posttraumatic stress symptoms may mediate the relationship between ASA and risky sexual behavior. For example, Walsh and colleagues (2014) found that intrusive symptoms partially mediated the relationship between child sexual and physical abuse and risky sexual behavior among college women. However, the Walsh et al. study did not assess history of ASA or other posttraumatic stress symptoms (e.g., hyperarousal). Further, there is a lack of previous research examining whether posttraumatic stress symptoms mediate the relationship between ASA and sexual aversion. Such a relationship might exist and would be consistent with Rellini’s (2008) model, such that for some women, ASA could lead to the pairing of posttraumatic stress responses (e.g., anxiety) with sexual stimuli, leading to sexual aversion.
Greater levels of alcohol use may also be associated with both ASA and risky sexual behavior in college women. Previous research indicates that increased alcohol use is associated with both exposure to sexual assault and engagement in risky sexual behavior (Champion et al., 2004; Parks et al., 2009). Consistent with alcohol myopia theory (Steele & Josephs, 1990), alcohol use is associated with greater intentions to engage in sexual activity and is likely to disinhibit sexual behaviors by restricting cognitive capacity to attend to and process multiple cues (e.g., sexual risk versus sexual arousal cues, for example; Scott-Sheldon et al., 2016). Within Rellini’s (2008) theoretical model, alcohol use could contribute to difficulties with inhibition of sexual thoughts and behaviors and difficulties with attending to cues that may elicit sexual inhibition, such as risk cues (e.g., lack of condom use). Walsh and colleagues (2014) proposed that college students who engage in problematic levels of alcohol use are more likely to attend to the perceived short-term benefits over the consequences of sexual behavior, consistent with alcohol myopia theory. Perhaps this is especially true for women with a history of ASA, who may either be seeking temporary relief from distress stemming from ASA or be attempting to regain control and positive affect related to their sexuality and sexual behavior (e.g., Kelley & Gidycz, 2015). Indeed, George et al. (2014) found that alcohol use mediated the relationship between sexual assault and sexual risk taking in a sample of community women.
Finally, lowered sexual assertiveness may also contribute to the relationship between ASA and increased risky sexual behavior. Previous research showed a reciprocal relationship between sexual assault and lower sexual assertiveness (Kelley et al., 2016; Livingston, Testa, & VanZile-Tamsen, 2009). Lower sexual assertiveness is also associated with greater engagement in risky sexual behaviors (Parks et al., 2009). In the context of Rellini’s (2008) model, difficulties with inhibition of sexual thoughts and behaviors may result in impaired assertiveness in sexual situations (e.g., not requesting a condom), ultimately resulting in more risky sexual behavior.
The current cross-sectional study was conducted to explore whether posttraumatic stress symptomatology, alcohol use, and difficulties with sexual assertiveness mediated the relationship between ASA and risky sexual behavior. Given previous research examining the role of partner type in conceptualizing sexual behavior, these mediational relationships were hypothesized to exist in the context of risky sexual behavior with a new partner. Examination of this mediational relationship was exploratory in the context of risky sexual behavior with a regular partner (e.g., a boyfriend). In addition, the current study explored whether posttraumatic stress symptomatology mediated the relationship between ASA and sexual aversion. Given a documented relationship between CSA and sexual behavior (e.g., Merrill et al., 2003; Senn, Carey, & Vanable, 2008), CSA was considered as a covariate in these relationships. The research question and hypotheses are as follows:
Method
Participants and Procedure
Women were recruited from a mid-sized Midwestern university as part of a larger study examining the relationship between ASA and female sexual functioning (Kelley, 2015). Participation served as an option for partial course credit for participants, who were recruited from undergraduate introductory courses in psychology. Participants completed online questionnaires via the Qualtrics (2013) online system on a computer of their choosing and received information for clearing browser history. The title of the study was advertised as “Women’s Social and Health Experiences.” Informed consent was obtained from all participants, and all participants received debriefing information (e.g., information about the study and referral sources). All study procedures were approved by the local institutional review board.
Of an original sample of 495 participants, 13 were excluded because they were over the age of 23 to preserve homogeneity of the sample in line with the intended focus on college-aged women (nontraditional students or students above the typical college age may have sexual experiences that are not reflective of this population; R. Hayes & Dennerstein, 2005). An additional 20 participants were excluded due to missing data on the study measure(s). In the final sample of 462 women, the average age was 18.87 (SD = 1.13). The majority of participants (62.9%) reported they were in their first year of college. Most (97.4%) endorsed entirely or mostly heterosexual, or more heterosexual than homosexual, sexual activity. The most common self-identified racial identity was Caucasian (endorsed by 89.3% of the sample), followed by Asian/Pacific Islander (3.7%), mixed/multiracial (3.3%), African American (3.0%), American Indian or Alaska Native (0.4%), and Middle Eastern (0.2%). Most of the women (57.0%) reported an annual household (e.g., parents’) income of greater than US$50,000.
Measures
CSA
The Child Sexual Victimization Questionnaire (CSVQ; Finkelhor, 1979) assessed history of CSA (sexual assault occurring before the age of 14). Participants responded to the eight behaviorally descriptive items reflecting incidents of CSA to indicate whether or not they experienced that incident. A sample item is, “Another person touched or stroked your sex organs.” For each item, if a participant responded “yes,” they completed three follow-up questions assessing characteristics of the incident (i.e., their relationship to the perpetrator, age of the perpetrator, and the main tactic used by the perpetrator). An experience was coded as CSA if any of the following criteria were met: (a) the perpetrator was an older adult, authority figure, or caregiver; (b) the perpetrator was at least 5 years older than the victim; or (c) the perpetrator used some form of coercion or force. Participants’ responses were coded ordinally into the following categories based on the most severe form of CSA reported: (a) no CSA history, (b) sexual exhibition, (c) fondling, and (d) penetration. Concurrent validity was demonstrated for the CSVQ by Risin and Koss (1987), who found that a large majority (93%) of participants who endorsed CSA experiences during an interview endorsed these items on the CSVQ.
ASA
The Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2007) is a seven-item measure used in this study of young adults to assess ASA experiences occurring on or after the 14th birthday. Items are behaviorally descriptive, and participants indicated the number of times they experienced each item. Various perpetrator tactics are also listed, for example, the perpetrator’s use of coercion (e.g., threatening to spread rumors), use of threat of physical harm, and use of physical force. The specific sexual behavior and the tactic used by the perpetrator are both used to determine the scoring category of victimization that a participant’s response is placed into (see Koss et al., 2007). A sample item (reflecting completed rape) is, “A man put his penis into my vagina, or someone inserted fingers or objects without my consent by using force, for example, holding me down with their body weight, pinning my arms, or having a weapon.” Each participant received an ordinal score based on the most severe event reported as follows: (a) no sexual victimization history; (b) unwanted sexual contact; (c) sexual coercion; (d) attempted oral, anal, or vaginal rape; or (e) completed oral, anal, or vaginal rape. Reflective of predictive validity, scores of victimization on the SES-SFV were positively correlated with total scores on the Trauma Symptoms Checklist (Briere & Runtz, 1989) in a study by Johnson et al. (2017).
Dissociation
The RAND Peritraumatic Dissociative Experience Questionnaire (RANDPDEQ; Marmar, Weiss, & Metzler, 1997; Marshall, Orlando, Jaycox, Foy, & Belzberg, 2002), an eight-item measure, was used to assess peritraumatic dissociation experienced during a traumatic event. Women who indicated a history of ASA completed this measure in reference to their most severe (or only) ASA experience. Women without a history of ASA completed this measure in response to a self-identified “stressful interpersonal or relationship situation” (e.g., relationship break-up) that served as an index stressor. For each item, participants indicated how true the statement was for them during or immediately after the event on a scale of 1 (not at all true) to 5 (extremely true). A sample item is, “I ‘blanked out’ or ‘spaced out’ or in some way felt that I was not part of what was going on.” Total scores were derived by summing across items; higher scores indicate greater dissociation. Previous research revealed convergent validity by a positive correlation between the RANDPDEQ total scores and symptoms of posttraumatic stress disorder (PTSD) measured by the PTSD Checklist–Civilian Version (Marshall et al., 2002). Internal consistency reliability for the current sample was excellent (Cronbach’s α = .93).
Post-traumatic stress symptoms
The Impact of Events Scale–Revised (IES-R; Weiss & Marmar, 1997), a 22-item measure, was used to assess symptoms of posttraumatic stress experienced over the past 4 weeks. For each item, participants indicated the level of distress associated with the difficulty described on a 5-point scale ranging from 0 (not at all) to 4 (extremely). Women with a history of ASA responded to items on the IES-R in reference to their most severe (or only) ASA experience endorsed, whereas women without a history of ASA responded to items in reference to their self-identified interpersonal index stressor. Three subscale scores were obtained consisting of intrusion (8 items; a sample item is, “I thought about it when I didn’t mean to”), avoidance (8 items; a sample item is, “I stayed away from reminders about it”), and hyperarousal (6 items; a sample item is, “I was jumpy and easily startled”) by summing across respective items. Higher scores reflect greater levels of symptoms in that subscale. Sundin and Horowitz (2002) reviewed evidence of convergent validity for the IES-R; subscale scores on the IES-R were positively associated with symptoms of PTSD assessed on the Symptom Checklist-90–Revised (SCL-90-R; Derogatis, 1986). Cronbach’s alpha values for the current sample were all excellent: intrusion (.95), avoidance (.92), and hyperarousal (.93).
Alcohol use
The Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993) is a 10-item measure assessing alcohol consumption, drinking behavior, and alcohol-related problems. Participants selected the response that best described their behavior for each question based on quantity and frequency of alcohol use; scoring anchors vary across items. A sample item is, “How often do you have four or more drinks on one occasion?” A total score was obtained, and higher scores reflect greater frequency of alcohol use and related problems. Adequate validity was demonstrated with a college student sample; the AUDIT detected 91% of high-risk drinkers identified by the timeline follow-back quantity-frequency measure of 28-day alcohol consumption (Kokotailo et al., 2004). Internal consistency was good for the current sample (Cronbach’s α = .85).
Sexual assertiveness
The Sexual Assertiveness Scale for Women (SAS-W; Morokoff et al., 1997) was used to assess sexual assertiveness related to initiation, refusal, and prevention behaviors against STIs and pregnancy. Participants responded to each of the 18 items indicating the extent to which they agreed with the statement on a 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). A sample item is, “I have sex without a condom or latex barrier if my partner doesn’t like them, even if I want to use one.” A total score was derived by summing across all items; higher scores reflect higher sexual assertiveness. Previous research demonstrated construct validity for this measure; assessment of condom self-efficacy, sexual self-acceptance, and sexual experience predicted higher sexual assertiveness measured by the SAS-W (Morokoff et al., 1997). For the current sample, Cronbach’s alpha was acceptable (.77).
Risky sexual behavior
The Cognitive Appraisal of Risky Events–Revised–Frequency of Incidence Scale (CARE-R-FOI; Fromme, Katz, & Rivet, 1997; E. Katz, Fromme, & D’Amico, 2000) Risky Sexual Behavior subscale was used to assess participants’ frequency of engagement in risky sexual behavior over the past 4 weeks (e.g., sex without use of a condom or while under the influence of alcohol). The seven items asked about participants’ risky sexual behavior occurring with (a) a regular partner (self-defined by the participant; for example, a boyfriend) and (b) with someone they just met or do not know well (e.g., a stranger). Participants selected the number of times they engaged in the behavior described on a 7-point scale ranging from 0 (never/not at all) to 6 (31 or more times). A sample item is “had sexual intercourse while under the influence of alcohol.” Two subscales reflecting risky sexual behavior with a regular partner and with a new partner were derived by summing across responses to each item in terms of the respective partner type. Higher scores indicate greater frequency. Previous research demonstrated that the frequency of incidence scales of the full CARE-R were positively associated with impulsive unsocialized sensation seeking (Fromme et al., 1997). For the current sample, the Cronbach’s alpha was good for the regular partner (.88), and excellent for the new partner (.92), subscales.
Sexual aversion
The Sexual Aversion Scale (SAS; R. C. Katz, Gipson, Kearl, & Kriskovich, 1989) Sexual Avoidance subscale was used to assess sexual aversion experienced over the past 4 weeks. Participants responded to each of the eight items on a 4-point scale ranging from 1 (not at all like me) to 4 (a lot like me), indicating how much the statement related to them. A sample item is, “I have repeatedly avoided all or almost all genital sexual contact with a sexual partner.” A total subscale score for each participant was calculated by summing across all eight items; higher scores reflect greater sexual aversion. Concurrent validity was evidenced by positive correlations between SAS total scale scores and scores on the Fear Survey Schedule (R. C. Katz, Gipson, & Turner, 1992). Cronbach’s alpha for the current sample was good (.88).
Data Analytic Plan
Frequency statistics regarding history of CSA and of ASA, and means and standard deviations of the study variables were calculated for descriptive purposes. Prior to the main inferential analyses, a series of Pearson’s r correlations was conducted among all study variables to determine the mediation models to be tested. Mediation models were then tested using the A. F. Hayes (2013) PROCESS macro for SPSS. The mediation models tested were determined according to the hypotheses and research question, when supported by the bivariate correlation analyses as follows: Contemporary models of mediation do not require a direct effect between the independent variable (i.e., ASA) and the dependent variable (i.e., specific sexual behavior variable) for mediation to exist. Thus, a model for each dependent variable (i.e., risky sexual behavior with a regular partner, risky sexual behavior with a new partner, and sexual aversion) was tested in conditions when the independent variable (i.e., ASA) was bivariately correlated with the hypothesized mediator(s) (i.e., hyperarousal, avoidance, intrusion, dissociation, alcohol use, and/or sexual assertiveness), and the hypothesized mediator(s) was correlated with the specific dependent variable. PROCESS (A. F. Hayes, 2013) allows for testing of these models with consideration of a covariate (i.e., CSA) and multiple mediators tested in parallel. The macro also allows for examination of the total indirect effect of the independent variable on the dependent variable via all mediators entered into the model using bias-corrected and accelerated bootstrapped confidence intervals of the indirect effect. It similarly allows for examination of the specific indirect effect of each individual mediator. This bootstrapping method is documented to be more powerful, even for small samples, and makes fewer assumptions than other inferential methods (e.g., the Sobel test, for example, MacKinnon, Lockwood, & Williams, 2004). The number of bootstrap samples used in each model tested was 10,000.
Results
Frequency statistics revealed that 25.8% of the sample reported some form of CSA. According to the most severe form of CSA reported, 14.3% (n = 66) indicated sexual exhibition, 8.7% (n = 40) reported fondling, and 2.8% (n = 13) reported penetration. In addition, 29.7% of the sample reported some form of ASA, with 6.9% (n = 32) reporting unwanted sexual contact, 6.0% (n = 28) indicating sexual coercion, 3.7% (n = 17) reporting attempted rape, and 13.0% (n = 60) indicating completed rape as the most severe incident experienced. Among the full sample, 13.9% (n = 64) of women reported experiencing some form of both CSA and ASA. Means, standard deviations, and bivariate correlations of the study variables are presented in Table 1.
Means, Standard Deviations, and Correlations of Sexual Abuse, Hypothesized Mediators, and Sexual Behavior Variables.

Note. ASA = adolescent/emerging adulthood sexual assault; CSA = childhood sexual abuse.
p < .05. **p < .05. ***p < .001.
Results of correlation analyses (see Table 1) revealed that ASA was positively correlated with CSA. In terms of relationships between ASA and the hypothesized mediators, ASA was positively associated with alcohol use, avoidance, and dissociation, and negatively associated with sexual assertiveness. ASA was not correlated with risky sexual behavior with a regular partner, but was positively associated with sexual aversion and risky sexual behavior with a new partner. CSA was positively associated with avoidance, intrusion, and dissociation. CSA was also positively associated with sexual aversion. In terms of relations between the hypothesized mediators and sexual behavior variables, greater avoidance, intrusion, hyperarousal, alcohol use, and lower sexual assertiveness were each associated with risky sexual behavior with a new partner. Greater avoidance, intrusion, hyperarousal, and dissociation were all related to greater sexual aversion. Finally, greater avoidance, intrusion, hyperarousal, and alcohol use were each associated with risky sexual behavior with a regular partner. Based on these correlations, three mediation models were tested with PROCESS (A. F. Hayes, 2013), and results of these models are described below.
Research Question 1: Risky Sexual Behavior With a Regular Partner
ASA was associated with greater alcohol use (B = 0.71, SE = 0.16, p < .001) but was not related to avoidance (B = 0.38, SE = 0.22, p = .093) or risky sexual behavior with a regular partner (B = −0.18, SE = 0.19, p = .364). In terms of the covariate, CSA was not related to alcohol use, avoidance, or risky sexual behavior with a regular partner (B = 0.08, SE = 0.36, p = .826), (B = 0.96, SE = 0.53, p = .074), (B = 0.47, SE = 0.57, p = .408), respectively. Alcohol use was related to more frequent risky sexual behavior with a regular partner (B = 0.31, SE = 0.07, p < .001), whereas avoidance was not related to risky sexual behavior with a regular partner (B = 0.08, SE = 0.05, p = .124). The full model accounted for about 7% of the variance in risky sexual behavior with a regular partner. The total indirect effect of ASA on risky sexual behavior via both potential mediators was significant (B = 0.25, SE = 0.08, 95% confidence interval [CI] [0.12, 0.44]), and the specific indirect effect via alcohol use was significant (B = 0.22, SE = 0.07, 95% CI [0.11, 0.39]), but the specific indirect effect via avoidance was not (B = 0.03, SE = 0.03, 95% CI [−0.002, 0.12]). See Figure 1 for a conceptual depiction of the final significant model.
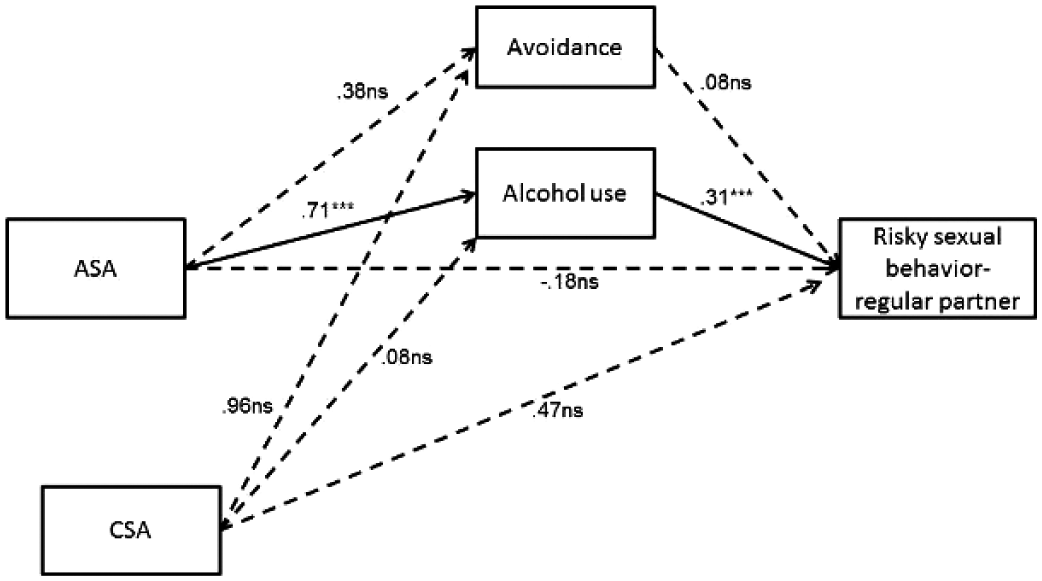
Depiction of tested model for Research Question 1 examining mediators between ASA and risky sexual behavior with a regular partner.
Hypothesis 1: Risky Sexual Behavior With a New Partner
ASA was associated negatively with sexual assertiveness (B = −0.85, SE = 0.29, p < .01) and positively with alcohol use (B = 0.71, SE = 0.16, p < .001), but was not associated with avoidance (B = 0.38, SE = 0.22, p = .093). In the presence of CSA and the proposed mediators, ASA was not associated with risky sexual behavior with new partner (B = 0.06, SE = 0.07, p = .403). Further, lower sexual assertiveness (B = −0.03, SE = 0.01, p < .01) and greater alcohol use (B = 0.14, SE = 0.03, p < .001) were both associated with more frequent risky sexual behavior with a new partner, whereas avoidance (B = 0.02, SE = 0.02, p = .214) was not associated with risky sexual behavior with a new partner, in the presence of the other variables. In terms of the covariate, CSA was not associated with sexual assertiveness (B = −0.14, SE = 0.62, p = .820), alcohol use (B = 0.08, SE = 0.36, p = .826), or avoidance (B = 0.96, SE = 0.53, p = .074), or risky sexual behavior with a new partner (B = 0.05, SE = 0.19, p = .778) in the presence of all other variables in the model. With all variables entered in the model, 13% of the variance in risky sexual behavior with a new partner was represented. The total indirect effect of ASA on risky sexual behavior with a new partner via all three potential mediators was significant (B = 0.13, SE = 0.03, 95% CI [0.07, 0.20]). The specific indirect effect via sexual assertiveness was also significant (B = 0.02, SE = 0.01, 95% CI [0.01, 0.06]), as was the specific indirect effect via alcohol use (B = 0.10, SE = 0.03, 95% CI [0.05, 0.16]). However, the specific indirect effect via avoidance was not significant (B = 0.01, SE = 0.01, 95% CI [−0.002, 0.04]). See Figure 2 for a conceptual depiction of the final model.

Depiction of tested model for Hypothesis 1 examining mediators between ASA and risky sexual behavior with a new partner.
Hypothesis 2: Sexual Aversion
Both ASA (B = 1.42, SE = 0.24, p < .001) and CSA (B = 1.69, SE = 0.57, p < .01), were associated with greater dissociation. Neither ASA (B = 0.38, SE = 0.22, p = .093) nor CSA (B = 0.96, SE = 0.53, p = .074) was associated with avoidance. Further, avoidance was positively associated with sexual aversion, B = 0.10, SE = 0.04, p < .01. However, none of the remaining variables consisting of dissociation (B = 0.03, SE = 0.04, p = .364), ASA (B = 0.07, SE = 0.14, p = .611), and CSA (B = 0.57, SE = 0.32, p = .074) were related to sexual aversion. All four variables considered concurrently accounted for about 6% of the variance in sexual aversion. The total indirect effect of ASA on sexual aversion via both dissociation and avoidance was not significant (B = 0.09, SE = 0.05, 95% CI [−0.01, 0.20]). Similarly, the specific indirect effects via dissociation (B = 0.05, SE = 0.05, 95% CI [−0.05, 0.16]) and via avoidance (B = 0.04, SE = 0.03, 95% CI [−0.0001, 0.12]) were each not significant.
Discussion
The current study was conducted to identify possible mediators of the relationships between ASA and risky sexual behavior and between ASA and sexual aversion in a sample of college women. Although analyses were cross-sectional, precluding conclusions about causality and requiring caution when interpreting results, this study is an important first step in identifying potential mediators of these relationships amenable to intervention. Results provided some preliminary support for Hypothesis 1 regarding risky sexual behavior with a new partner, but did not support Hypothesis 2 regarding sexual aversion. Results for Research Question 1 confirm the conceptual importance of examining partner type (i.e., regular vs. new partner) in understanding college women’s engagement in risky sexual behavior (e.g., Messman-Moore et al., 2010). Generally, results were supportive of Rellini’s (2008) theoretical model, suggesting psychological and behavioral mechanisms behind relationships between ASA and sexual behavior.
Regarding Hypothesis 1, ASA was associated with lower sexual assertiveness and greater alcohol use, and lower sexual assertiveness and greater alcohol use were each associated with more frequent risky sexual behavior with a new partner. This is partially consistent with the study by Walsh and colleagues (2014), whereby traumatic intrusions and alcohol use mediated the relationship between childhood physical and sexual abuse and risky sexual behaviors in college women. In the context of Rellini’s (2008) model, it is possible that alcohol use is associated with difficulties with sexual inhibition in some women with a history of ASA. In addition, in terms of Research Question 1, ASA was associated with greater alcohol use, and greater alcohol use was associated with more risky sexual behavior with a regular partner. It is possible that women with a history of ASA engage in increased alcohol use as a means of coping with the sexual trauma, which can be problematic because of its link with risky sexual behavior. Given that previous research indicates a reciprocal relationship between sexual assault and alcohol use (Bryan et al., 2016), and shows that decreased relational sexual assertiveness mediates the relationship between ASA and sexual revictimization (Kelley et al., 2016), alcohol use and sexual assertiveness appear to be two possible targets of interventions to reduce college women’s risk for negative consequences (e.g., STIs, sexual revictimization) of risky sexual behavior with a new or unknown partner.
Interestingly, results did not support the hypothesis that posttraumatic stress symptoms would mediate the relationship between ASA and sexual aversion (Hypothesis 2). This may be partially reflective of the sample characteristics regarding level of symptomatology; the mean score on the sexual aversion scale in this sample appeared generally low. Further, ASA was not bivariately correlated with some of the posttraumatic stress symptoms; this may be indicative of a relatively healthy, young sample in terms of traumatic stress. There were, however, significant bivariate relationships of small magnitude between sexual aversion and posttraumatic stress symptoms. Previous research identifies acute trauma symptoms as particularly important when understanding trajectories following sexual assault; posttraumatic stress symptoms tend to be evident in a higher proportion and at greater severity in the immediate time period following sexual trauma (e.g., 1 month; Steenkamp, Dickstein, Salters-Pedneault, Hoffman, & Litz, 2012). Thus, the salience of trauma symptoms assessed in the current study may have decreased across time following the ASA incident. Other symptoms may also be associated with sexual aversion among some women with a history of ASA—and would be consistent with Rellini’s (2008) theoretical model—such as negative alterations in cognition, appraisals about sexual situations (e.g., hypervigilance to risk or pain cues), or coping strategies (e.g., Kelley & Gidycz, 2015).
It is also interesting to note that CSA was not individually associated with the sexual behavior variables in the presence of the other variables in the PROCESS models. The nature of the sample included is important to consider; young women with a history of CSA who attend college may experience less severe negative effects of CSA, or have more protective and resilience variables that buffer them from the potential negative impact of CSA (e.g., socioeconomic status and other health variables), than women with a history of CSA who do not attend college. Indeed, previous research identified variables that reduce the likelihood of psychological sequelae and of later sexual assault among women with a history of CSA, including positive social support, positive coping (e.g., reframing), and internal locus of control (e.g., see Walsh, Blaustein, Knight, Spinazzola, & van der Kolk, 2007, for a discussion). Such resiliency variables, though not assessed in this study, could potentially affect sexual behavior among college women. Alternatively, given that a history of CSA is associated with subsequent ASA (e.g., Maker, Kemmelmeier, & Peterson, 2001), it is likely that a large amount of variance in CSA was accounted for by ASA in the models.
In general, there is likely a natural range across women in terms of preferences for and patterns of sexual behavior. In this sense, it is important to not over-pathologize young women’s sexual behavior. Results suggest resilience among many women with a history of sexual victimization, given the lack of direct relationships between ASA and risky sexual behavior in the PROCESS models. This is especially important when considering the context of college campuses and college student populations and what may be normative sexual behavior that exists in this setting. However, there is still likely a proportion of women with a history of ASA who experience distressing or high-risk disruptions in sexual behavior, suggesting the continued importance of identifying mediators of the relationships between ASA and risky sexual behavior and sexual aversion. Even if a relatively small proportion of women, it remains important to study risky sexual behavior due to its potential deleterious effects (e.g., increased risk for STIs and sexual victimization).
The results of the current study are limited by the use of a retrospective, cross-sectional, self-report methodology, which is subject to recall bias and precludes the interpretation of temporal or causal relationships among the study variables. For example, it is possible that earlier alcohol use, lower sexual assertiveness, or risky sexual behavior was associated with greater risk for the ASA experiences reported in this sample. In addition, the alcohol-use measure assessed general alcohol use; we could not detect whether this represented alcohol use immediately prior to sexual behavior. Furthermore, this study was intended to focus on a sample of young college women given the significance of sexual health and development, and high rates of sexual abuse in this population. However, this represents a relatively homogeneous sample, and the patterns of results may not generalize to other populations (e.g., older women presenting to mental health clinics). As discussed above, college women may have unique sexual experiences not reflective of nontraditional students or women in middle or late adulthood (R. Hayes & Dennerstein, 2005). Given our focus on sexual victimization experienced in adolescence and emerging adulthood, results may not generalize to women who experience sexual victimization in later developmental stages. Further, the vast majority of the participants identified as heterosexual, precluding generalization of our findings to sexual minority samples. Finally, other variables confounded with sexual victimization that may affect sexual behavior were not assessed in this study (e.g., problems in family relationships; educational resources related to sexual health) and may modify the role of the hypothesized mediators examined in this study.
Despite these limitations, there are several possible clinical and research implications of the current study. Results regarding Hypothesis 1 suggest that women with a history of ASA may benefit from assertiveness skills training particularly in sexual contexts, to help reduce potential risks associated with sexual behavior with a new partner (e.g., risk for STIs or revictimization). Furthermore, results of both Hypothesis 1 and Research Question 1 suggest that women with a history of ASA would benefit from psychoeducation on the effect of alcohol use on sexual decision-making (Scott-Sheldon et al., 2016) and communication with both regular and new partners. Considering the cross-sectional nature of the current study, women without a history of ASA may also benefit from such psychoeducation and assertiveness skills training to potentially reduce the risk for ASA, although this should be tested in future research. Indeed, future research should expand on the current study using longitudinal methods to test the hypothesized temporal relationships between study variables. With such methods, variability in the patterns of relationships between sexual trauma, posttraumatic stress, alcohol use, sexual assertiveness, and sexual behavior across time would be possible (e.g., to examine differential patterns in the acute period following ASA vs. years following ASA).
Future research should also examine additional variables that may play a role in college women’s engagement in risky sexual behavior and sexual aversion. Variables to consider include other mental health variables (e.g., anxiety and depression; Harris & Valentiner, 2002), emotion regulation, relationship status and functioning, and coping strategies in response to sexual trauma. Contextual variables are likely of importance as suggested by the role of sexual assertiveness (e.g., partner characteristics, and alcohol use immediately prior to sexual behavior) and consistent with the role of second-order processes in Rellini’s (2008) model. Such examinations are needed to continue identifying variables that may promote healthy sexual behavior and resiliency in women with a history of sexual victimization. Future research should examine these hypothesized mediation models among other diverse groups of women. For example, testing these hypotheses among non-Caucasian women may yield different patterns of relationships, as previous research showed differences between college women who self-identified as Caucasian and non-Caucasian in cognitive and affective aspects of sexuality (e.g., sexual self-esteem; Kelley & Gidycz, 2015), which may affect sexual behavior. In addition, future research should test these hypothesized mediators in women across developmental age groups (e.g., mid-life) as other contextual variables (e.g., marital status, menopause status) may affect sexual behavior.
Footnotes
Authors’ Note
Erika L. Kelley is now at the Sierra-Pacific Mental Illness Research, Education, and Clinical Center, Veterans Affairs Palo Alto Health Care System, and the Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine. This research project was conducted while the first author was a graduate student at Ohio University. The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Department of Psychology, Ohio University. Dr. Kelley’s work was supported in part by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Mental Illness Research and Treatment, the Medical Research Service of the Veterans Affairs Palo Alto Health Care System, and the Department of Veterans Affairs Sierra-Pacific Mental Illness Research, Education, and Clinical Center (MIRECC).