
Abstract
Individuals with histories of interpersonal trauma are at increased risk for posttraumatic stress disorder (PTSD). Risk of PTSD is particularly salient during critical periods of development, such as adolescence and emerging adulthood. However, little is known about the unique effects and interactions of protective factors and interpersonal trauma on PTSD symptoms in adolescents and young adults. The current study tested whether positive peer and family experiences decrease the associations between interpersonal trauma and PTSD symptoms and whether these associations differed by victim–perpetrator relationships. Participants included 3,618 adolescents and young adults (aged 14-24 years) who completed the Behavioral Health Screen—a web-based screening tool that assesses psychiatric symptoms and associated risk factors—during a routine visit across 10 primary care sites in Pennsylvania. In support of the stress buffering hypothesis, results revealed that positive peer and family experiences buffered the effects of interpersonal trauma by a romantic partner and an adult in the home. Future research should examine whether programs aimed at improving peer or family relationships improve outcomes for traumatized youth.
Approximately 25% of adolescents are victims or witnesses of physical violence, and 11% of youth have experienced sexual trauma by the age of 16 (Copeland, Keeler, Angold, & Costello, 2007). Interpersonal trauma during childhood and adolescence (e.g., physical and sexual abuse) can have serious psychological consequences, including the development of posttraumatic stress disorder (PTSD) symptoms (Berenz et al., 2016). Indeed, adolescence and emerging adulthood are critical periods of development characterized by elevated onset of mental health problems (Kessler et al., 2005), with the complex interaction of psychosocial stressors and substantial neurobiological development that occur during these periods influencing this heightened risk for mental health problems (Byrne et al., 2017). The unique social, physical, and emotional challenges experienced during adolescence make this age group particularly vulnerable to interpersonal traumas, which threaten their sense of safety and security (Charuvastra & Cloitre, 2008).
Conversely, both intrapersonal and interpersonal factors, such as prosocial behaviors, positive experiences, and social companionship with family and friends, are associated with fewer mental health problems for adolescents and young adults (O’Loughlin, Althoff, & Hudziak, 2017). More specifically, family support is associated with increased self-esteem (Wilburn & Smith, 2009) and psychological well-being (Harding et al., 2015) among adolescents and young adults, and lack of prosocial peer interactions is associated with the maintenance of depressive symptoms during adolescence (Herres & Kobak, 2015). The stress-buffering hypothesis (Cohen & Wills, 1985) posits that such support can decrease the maladaptive effects of interpersonal trauma, including community violence (Brookmeyer, Henrich, Cohen, & Shahar, 2011), domestic violence (Cluver, Fincham, & Seedat, 2009), and childhood sexual abuse (Hyman, Gold, & Cott, 2003), and protect against the development of PTSD (Charuvastra & Cloitre, 2008).
The influence of interpersonal trauma on PTSD symptoms has also been shown to vary by victim–perpetrator relationships. For instance, the negative effects of interpersonal traumas are stronger for individuals assaulted by known individuals rather than strangers (Lawyer, Ruggiero, Resnick, Kilpatrick, & Saunders, 2006). However, little is known about whether the protective effects of positive interpersonal experiences could differ depending on both the source of the trauma and the support. As adolescents and young adults decrease their reliance on parents to meet attachment needs, they increasingly seek out peers and romantic partners for support (Wrzus, Hänel, Wagner, & Neyer, 2013). During this particular developmental period, various attachment figures (parents, peers, and romantic partners) may be differentially associated with the development of PTSD symptoms.
The current study examined the differential impact of interpersonal trauma perpetrated by a romantic partner versus an adult in the home among pediatric primary care patients who completed the Behavioral Health Screen (BHS; Diamond et al., 2010). We also examined the unique moderating effects of positive family and peer experiences. We hypothesized that adolescents with histories of interpersonal trauma (either at the hands of a romantic partner or an adult in the home) would endorse more PTSD symptoms, and adolescents who reported positive peer and family experiences would endorse fewer PTSD symptoms. In accordance with Cohen and Wills’ (1985) stress-buffering model, we also hypothesized that positive peer and family experiences would buffer against the effects of interpersonal trauma on PTSD symptoms. Finally, we explored whether these buffering effects of positive peer and family experiences differed by the perpetrator of the interpersonal trauma (romantic partner vs. an adult in the home).
Method
Participants
Participants were 3,618 adolescents and young adults (14-24 years old, Mage = 16.28, SDage = 2.16) who presented for routine medical exams at 10 primary care settings across semiurban Pennsylvania. The majority of the sample was identified as female (64% female), 59.2% identified as White, 7.2% as Black/African American, 2.9% as Asian, 1.7% as Native Hawaiian/Other Pacific Islander, 0.8% as American Indian/Alaskan Native, 13% as more than one race, and 15.1% as unsure.
Procedure
Patients were asked by medical staff to complete the BHS, a web-based screening tool, prior to their medical exam. According to medical staff, the large majority of patients agreed to participate, though the exact percentage of those who declined is not available. Institutional review boards at the (removed for blind review) approval of the study procedures and participants provided consent for their data to be used in research prior to completing the survey, which took approximately 5-10 min to complete.
Measure
The BHS (Diamond et al., 2010) was designed to screen for mental health problems in medical settings using questions derived from the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000). Fifty-five core questions and 38 follow-up questions assessed the following areas: demographics, medical, school, family, safety, substance abuse, sexuality, depression, anxiety, nutrition/eating, suicide, psychosis, and PTSD. The current study examined the PTSD symptoms module of the BHS, which comprised four items assessing whether participants had experienced intrusive recollection, avoidance, hyperarousal, and numbing during the past 2 weeks. This scale has shown good convergent and discriminant validity through strong correlations with established measures of traumatic stress and good sensitivity and specificity in distinguishing between individuals with and without clinically significant PTSD symptoms (Diamond et al., 2010). Cronbach’s alpha for the current sample was .79. We also used participants’ responses on four items (dummy coded 1 = yes) regarding whether participants (a) had been physically or sexually hurt by a romantic partner, (b) had been physically or sexually hurt by an adult in their home, (c) had a family member to confide in, and (d) spent time with friends during free time at school.
Data Analysis
Analyses were conducted using SPSS version 23. An analysis of covariance (ANCOVA) controlling for age, minority status, and gender tested differences in PTSD symptoms between participants with and without a history of interpersonal trauma from a romantic partner or adult in the home and between participants who did and did not report positive peer and family experiences. We also examined interactions between interpersonal trauma and positive peer/family experiences. Missing data was minimal (ranging from 0% to 0.6% across main study variables).
Results
A total of 1,087 participants (30.04%) endorsed interpersonal trauma from a romantic partner, 1,086 (30.01%) endorsed interpersonal trauma from an adult in the home, 437 (12.08%) endorsed positive peer experiences, and 1,088 (30.07%) endorsed positive family experiences. The ANCOVA was significant, F(12, 3430) = 17.24, p < .001, η2 = .08. Table 1 presents F statistics for the main effects as well as mean PTSD symptoms across the groups. Participants who experienced interpersonal trauma from either a romantic partner or an adult in the home endorsed more PTSD symptoms than those without a history of interpersonal trauma. Participants with positive peer experiences endorsed fewer PTSD symptoms. Positive family experiences did not have a main effect on PTSD symptoms.
Results of ANCOVA Main Effects on PTSD Symptoms.

Note. ANCOVA = analysis of covariance; PTSD = posttraumatic stress disorder.
p < .01. **p < .001.
There was a significant interaction between interpersonal trauma from a romantic partner and positive peer—F(1, 3434) = 9.45, p = .002—and family—F(1, 3434) = 5.48, p = .02—experiences. Although participants with a history of interpersonal trauma from a romantic partner reported more PTSD symptoms, this effect was weaker for participants who reported positive peer and family experiences. There was also a significant interaction between interpersonal trauma from an adult in the home and positive family experiences—F(1, 3434) = 5.48, p = .02—but not peer experiences—F(1, 3434) = 0.36, p = .55. Although the presence of interpersonal trauma from an adult in the home increased PTSD symptoms across the entire sample, this effect was weaker for participants who reported positive family experiences. All significant interactions are shown in Figure 1.
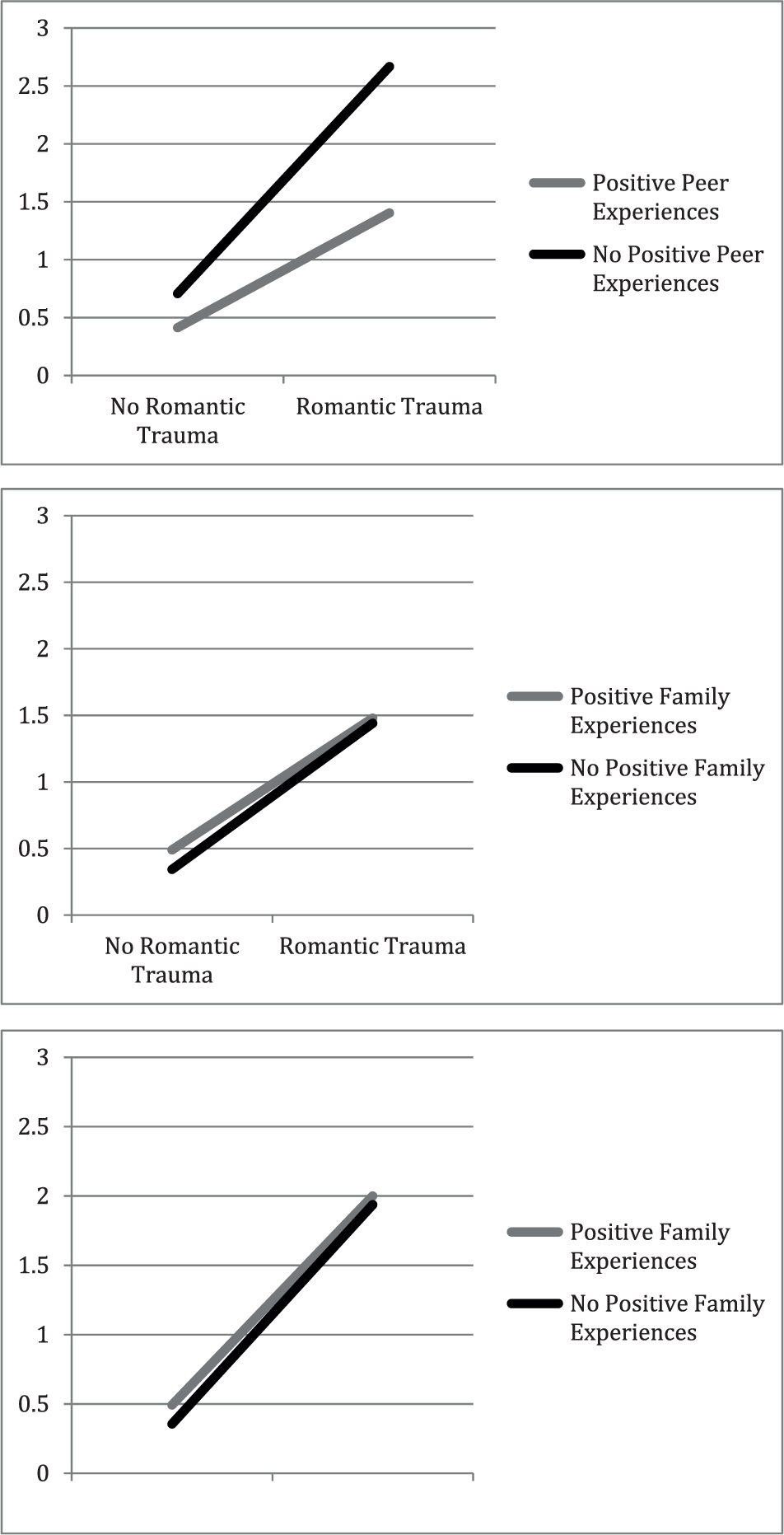
Buffering effects of positive interpersonal experiences on PTSD symptoms.
Discussion
Adolescents and young adults with histories of interpersonal trauma endorsed more PTSD symptoms, whereas participants who reported positive peer experiences, regardless of trauma history, reported fewer PTSD symptoms. These results extend previous research demonstrating the negative consequences of interpersonal trauma and benefits of positive peer experiences on PTSD symptoms to a community sample of adolescent and young adult primary care patients. The lack of a main effect for positive family experiences could be due to the fact that participants with greater PTSD symptoms sought the support of their family members to cope with these symptoms. In this case, positive family experiences may have served as a protective factor in buffering the effects of interpersonal trauma, rather than a promotive factor (i.e., main effect), on PTSD symptoms. Indeed, while positive family experiences did not have a main effect on PTSD symptoms, these experiences significantly buffered the effects of interpersonal trauma from both a romantic partner and an adult in the home. The positive effects of close family ties are well established (Fuller-Iglesias, Webster, & Antonucci, 2015), and our results further suggest that family experiences are particularly important and beneficial in the context of interpersonal traumas. Similarly, positive peer experiences buffered against the effects of interpersonal trauma perpetrated by a romantic partner. These findings are consistent with the stress-buffering hypothesis and previous findings demonstrating protective effects of social support (Cohen & Wills, 1985; Wohlgemuth & Betz, 1991).
Although the effect of interpersonal trauma from an adult in the home on PTSD symptoms was also weaker for participants endorsing positive peer experiences, this interaction was not statistically significant, indicating that the protective effects of positive peer experiences may be significantly weaker for adolescents and young adults who experience abuse within the home. Although adolescence and young adulthood is characterized by increased attachment and dependence on peer relationships, those who experience ruptures in familial attachment bonds may feel less capable and be less willing to establish close bonds with their peers. In addition to ruptures in attachment bonds, parental abuse is associated with greater shame and stigma (Bennett, Sullivan, & Lewis, 2005), which—in turn—can lower individuals’ perceptions of acceptance and have a negative impact on friendships (Feiring, Rosenthal, & Taska, 2000). Although the current study assessed abuse from adults within the home rather than exclusively from parents, it is plausible that the effects of abuse at the hands of adults in the home would show similar effects on shame and stigma. Adolescents and young adults who internalize these attitudes may feel embarrassed and attempt to conceal this abuse from their peers, which may preclude the formation of a strong peer support network and thus decrease the protective effects of peer relationships.
Our findings should be considered in context of the study’s limitations. The single-item measures of interpersonal trauma and positive peer and family experiences, as well as the subjective nature of these questions, may not have completely or objectively captured the nature or timing of participants’ experiences. The cross-sectional nature of our study also precludes assumptions about causality. Future research should use longitudinal methodology to determine whether, among adolescents and young adults with histories of interpersonal trauma, greater support from peers and families predicts decreased PTSD symptoms.
These findings could inform prevention and early intervention programs for adolescents and young adults who have experienced interpersonal trauma. For instance, future research should examine whether group-based (Grassetti et al., 2015) and family-based therapies (Ewing, Diamond, & Levy, 2015; Kobak, Zajac, Herres, & Ewing, 2015) reduce posttraumatic stress by improving relationships with peers and families. If identified as a mechanism of change in treatment for PTSD, focusing on therapeutic techniques that promote positive interpersonal relationships could improve outcomes for adolescents and young adults who have experienced interpersonal trauma, although the cross-sectional nature of the current study makes any conclusions about these clinical implications premature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Behavioral Health Screening tool is owned by Children’s Hospital of Philadelphia (CHOP) and licensed to Medical Decision Logic, Inc., a health science informatics and computer science engineering company which makes the screening tool commercially available. G.D. might one day receive a small royalty payment from CHOP for their part in developing the tool. S.B.W. and J.H. report no biomedical financial interests or potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by Substance Abuse and Mental Health Services Administration (SAMHSA; 5U79SM058386, 1U79SM060387, 1U79SM061750) Garrett Lee Smith Suicide Prevention Programs.