
Abstract
This research examines how mental health issues associated with intimate partner violence (IPV) relate to women’s intersecting identities of race/ethnicity, disability status, and child abuse history. Data (N = 595) from a Canadian triprovincial study included women who were White (n = 263, 44.8%), Indigenous (n = 292, 49.7%), or visible minority (n = 32, 5.5%). Few demographic differences were found. None of the mental health measures (Symptom Checklist–Short Form [SCL-10], Centre for Epidemiological Studies–Depression [CES-D-10], Posttraumatic Stress Disorder [PTSD] Checklist) were in the clinical ranges. In a MANCOVA on the mental health scales, with IPV severity, racial group, disability status, and child abuse history as variables, only disability was significantly associated with more mental health symptoms.
Keywords
Violence against women (VAW) is a significant social issue that often results in injury, emotional harm, and, at worst, death (Johnson, 2006). In the General Social Survey (GSS) on Victimization in Canada (Statistics Canada, 2011), with data collected in 2009 (closest to that in the current study), about 5% of women were abused by spouses in the past 5 years. The three prairie provinces, the sites of the current study, had the highest rates of self-reported spousal violence (national average = 6%, Saskatchewan = 8.2%, Alberta = 7.6%, Manitoba = 7.4%).
Intimate partner violence (IPV) includes physical abuse and sexual abuse (Romans, Forte, Cohen, Du Mont, & Hyman, 2007). Every year, across Canada, a small number of women are murdered by their partners as the tragic result of violence in their relationships (Dawson, Bunge, & Balde, 2009). In addition, many women endure years of intense psychological abuse that affects their lives and the lives of their children (Ansara & Hindin, 2011). Women are typically abused in multiple ways, each of which can have a cumulative effect on their feeling trapped and ineffective in either coping with the violence or fleeing their abusive partners. Furthermore, women can be at increased risk of abuse after separating from their partners (Brownridge et al., 2008; Fleury, Sullivan, & Bybee, 2000).
Although the rates of IPV are important indicators of its severity as a social problem, considerable research has examined the mental health consequences of IPV, disabilities that may make women vulnerable to IPV, connections between IPV and child abuse, and differences among women from varied racial and ethnic backgrounds (e.g., Hahn, McCormick, Silverman, Robinson, & Koenen, 2014; Lacey, McPherson, Samuel, Sears, & Head, 2013). We view race as a social construct that has been claimed by some to be biological but has more to do with one’s experience in a society with unequal rankings of cultural or biological characteristics. In a dominantly Caucasian society, for instance, people not identifiable as Caucasian for whatever reason are often racialized and suffer discrimination because of that (Bhopal, 2004).
This article takes an intersectional perspective (Sokoloff & Dupont, 2005) in examining, concurrently, multiple facets (racial and ethnic backgrounds, disabilities, and experiences of child abuse) of the lives of almost 600 women abused by intimate partners who sought assistance from IPV services in Canada’s three prairie provinces. It addresses the complexities of their lives, assessing similarities and differences that could suggest unique circumstances and better ways for service providers to understand their needs.
Theoretical Orientation: An Intersectionality Framework
Intersectionality is “a theoretical or analytical approach that simultaneously considers multiple categories of identity, difference, and inequality (such as gender, race, class, sexual orientation, disability, as well as others)” (Else-Quest & Shibley Hyde, 2016, p. 155). Originally conceived as a counterpart to the idea that all women are at equal risk of IPV, intersectionality is becoming a commonly used framework in IPV (Bent-Goodley, 2007), health (Hankivsky et al., 2010), and disability research (i.e., Cramer & Plummer, 2009; Lightfoot & Williams, 2009). Although “giving voice” to marginalized populations is a common goal of research informed by intersectionality theory, it also provides a means of identifying conditions that are particularly advantageous or disadvantageous.
The following sections present a brief overview of research on the variables of interest in the current analysis, highlighting Canadian studies about the intersections of race/ethnicity, disability status, and child abuse history as related to IPV and mental health.
Racial and Ethnic Origins and IPV in Canada
Not all Canadian women face the same risks of IPV or have the same IPV experiences. In the Canadian context, Indigenous people (previously labeled “Aboriginal,” a term originally from government) are a large, important subpopulation; and yet, there is relatively little research on IPV among Indigenous Canadians. The term “Indigenous” includes First Nations, Métis, and Inuit peoples and represents about 4.6% of Canada’s population (Statistics Canada, 2013a). According to Brownridge (2008), Indigenous women are at risk of being abused by intimate partners (21%) three times higher than the risk for non-Indigenous Canadian women (7%). As noted by Brennan (2011), Indigenous women often endure the most serious physical and sexual IPV. A number of structural issues in Indigenous communities contribute to the greater risk, including high rates of poverty, lack of services, loss of traditional lifestyles, and loss of parental role models because of residential schools and colonization (Brownridge, 2008).
Other than Indigenous women, those who are non-White will be referred to as “visible minorities” and make up a noteworthy portion of the population of Canadian women. In 2011, the percentage of visible minority women and girls was 19.3% of the total female population, according to Statistics Canada (2013b), with South Asian, Chinese, and Black the most common visible minority groups, representing a continuous, upward trend since the 1980s. In a study comparing visible minority Canadian women with White Canadian women, Hyman, Forte, Du Mont, Romans, and Cohen (2009) found no differences in the self-reported rates of physical and or sexual violence in the last 5 years. Further research examining these groups is needed to more adequately understand both the risks of IPV and how it is experienced.
Women With Disabilities and IPV
The World Health Organization and World Bank (2011) takes a bio-psycho-social perspective of disability, using Leonardi et al.’s (2006) definition as, “the umbrella term for impairments, activity limitations and participation restrictions, referring to the negative aspects of the interaction between an individual (with a health condition) and that individual’s contextual factors (environmental and personal factors” (p. 4). Given the physical nature of much IPV, many women suffer long-term physical consequences (Dutton, 2009). In a recent national U.S. study, Breiding and Armour (2015) found that, compared with women without disabilities, women with disabilities were significantly more likely to report each type of IPV measured, including physical violence, stalking, and rape, a finding generally supported in U.S. research (Barrett, O’Day, Roche, & Lepidus Carlson, 2009; Hahn et al., 2014) and in Canada (Brownridge, 2006; Cohen, Forte, Du Mont, Hyman, & Roman, 2005; Yoshida, Du Mont, Odette, & Lysy, 2011).
Mental Health, IPV, and Child Abuse History
Research that considers mental health status shows that women affected by such disorders are more vulnerable to being abused by intimate partners than women without mental health issues (Du Mont & Forte, 2014). Women who have experienced chronic and ongoing abuse from their partners are often diagnosed with mental health issues such as depression and anxiety (Ferrari et al., 2014; Perez & Johnson, 2008; White & Satyen, 2015). Researchers have also found high rates of posttraumatic stress disorder (PTSD; Coker, Weston, Creson, Justice, & Blakeney, 2005; Dutton, 2009 Woods, 2005), which Perez and Johnson (2008) note can compromise women’s safety after leaving abusive partners.
Another variable associated with disabilities is a history of child abuse, which is correlated with mental health concerns (often among victims of child sexual abuse) or physical disabilities (often because of child physical abuse; Ballan et al., 2014). Abused children are at high risk of further victimization as adolescents or adults (Barnes, Noll, Putnam, & Trickett, 2009; Widom, Czaja, & Dutton, 2014). Although PTSD has been associated with childhood abuse, especially child sexual abuse (Clemmons, Walsh, DiLillo, Messman-Moore, 2007) and IPV (as noted previously), given that many women experience both (Widom et al., 2014), the interconnections are important (Becker, Stuewig, & McCloskey, 2010; Nicolaidis, McFarland, Curry, & Gerrity, 2009).
The Current Study
The current study adds to our understanding of these issues by presenting descriptive data from almost 600 women using an intersectionality framework (Bent-Goodley, 2007) that focuses on a number of social identity variables, including racial and ethnic background, childhood abuse history, and mental and physical disabilities in combination. More commonly, these social differences are presented as though they are independent and separate. For example, national studies that focus on racial background and IPV seldom collect standardized assessments of mental health symptoms (e.g., Du Mont & Forte, 2014), or studies that focus on disability status and IPV may not collect information on race and ethnicity (e.g., Cohen et al., 2005).
The Healing Journey data set includes information about numerous background variables as well as scores on standardized mental health measures and allows for a more complex picture of how women’s social locations are related to their experiences of IPV. Because Canadian statistics suggest differences in the context of abuse in White, Indigenous, and visible minority populations, it was of interest to examine potential group differences in mental health functioning. Lacey et al. (2013), Bent-Goodley (2007), and White and Satyen (2015) all suggest the importance of comparing abused women from different racial/ethnic groups because of structural factors that differentially affect their lives and help seeking. As one example, in the Canadian 2005 GSS, Indigenous women had much higher rates of postseparation IPV than non-Indigenous women (Pederson, Malcoe, & Pulkingham, 2013).
Women abused by partners often seek counseling, and health professionals need to understand the context of their presenting symptoms. Understanding their mental health concerns in conjunction with disability status and child abuse history could assist them in providing more appropriate support and interventions.
The current study had three objectives: (a) to provide a descriptive profile of women identified as having experienced IPV in the prairie provinces of Canada, taking into account their social locations as Indigenous, visible minority, or White women; (b) to explore the abuse experiences and mental health of women reporting disabilities compared with those who did not report a disability; and (c) to examine possible intersections of these key variables.
Method
Research Sample
“The Healing Journey” is a longitudinal, Canadian study of 659 abused women from the three western provinces of Alberta, Saskatchewan, and Manitoba. Both academics and community agency members of the research team assisted in designing the research, recruiting participants, and interpreting the results. Data for the entire study were collected in seven waves between 2005 and 2009, although the current article only analyzes data from Waves 1 and 2.
The research protocols were approved by the six universities associated with the academic research partners. To identify possible organizations from which to recruit, each province conducted an environmental scan of IPV agencies. The intent was to recruit broadly so as to access women seldom included in research such as those from remote communities. The organizations included VAW shelters and counseling agencies, some with specific IPV programs, across the three provinces and chosen to cover urban, rural, and northern sites. Volunteers were recruited through information sessions at agencies, sealed envelopes containing information about the study provided by agency staff, and posters. The criteria for inclusion were being a minimum 18 years of age, the most recent incident of IPV no sooner than 3 months prior to recruitment, commitment to stay in the study for the full 4 years, and no serious or debilitating mental health issues.
Research Measures
For the Healing Journey study as a whole, four surveys were created to address demographic background and history of abuse, general functioning and service utilization, health, and parenting. These surveys included standardized measures as well as open-ended and closed-ended questions developed specifically for the study. We also included questions asking the women to self-report physical and mental health conditions (whether or not these were formally assessed by medical personnel is unknown), and whether these conditions affected their employability or kind or amount of daily activity. These data were used to create a “disabilities” variable; women were identified as having a disability if their physical or mental health conditions affected employability or other activities. Child abuse history was collected via structured questions, “Were you abused as a child or adolescent? (a) physical, (b) sexual, (c) emotional/psychological, (d) witnessing abuse among family members, etc.”
The nature of the IPV was assessed by the Composite Abuse Scale (CAS; Hegarty, Bush, & Sheehan, 2005). This screening measure consists of 30 items, rated for frequency in the past 12 months on a six-point scale from never to daily, with a possible total of 150. The four subscales are Severe Combined Abuse (eight items, possible score = 0-40, suggested cutoff of 1), Physical Abuse (seven items, possible score = 0-35, cutoff of 1), Emotional Abuse (11 items, possible score = 0-55, cutoff of 3), and Harassment (four items, possible score = 0-20, cutoff of 2). The suggested clinical cutoff for the total score is 3 or 7 to minimize false positives (Hegarty & Valpied, 2013). The scale has demonstrated convergent and discriminant validity (Hegarty et al., 2005). Cronbach’s alpha for the CAS in the current study is .93.
The Symptom Checklist–Short Form (SCL-10; Nguyen, Attkisson, & Stegner, 1983) is a screening tool to assess global mental health functioning and psychological distress in the previous week. This short form of the SCL-90 (Derogatis & Cleary, 1977) includes six depression questions, two somatization items, and two phobic/anxiety items. Items (e.g., “In the past week, how much were you distressed by feeling lonely?”) are endorsed with a 0 to 4 Likert-type scale, with 0 indicating not at all and 4 indicating extremely. Higher scores indicate more psychological distress. Suggested clinical cutoff scores are one standard deviation above the mean (Jacobson, Follette, & Revenstorf, 1984). With an average of 7.8 and SD of 6.3, in Müller, Postert, Beyer, Furniss, and Achtergarde (2010), which used the SCL-10 identically to the current study, the clinical cutoff score is 14.2. Cronbach’s alpha in the current study is .89.
The Centre for Epidemiological Studies–Depression (CES-D-10), a measure developed for research purposes, is a short form of the CES-D-20 (Radloff, 1977) to document depression symptoms in the previous week (Andresen, Malmgren, Carter, & Patrick, 1994). Ten items (e.g., “In the past week I was bothered by things that usually don’t bother me?”) are rated on a 0 to 3 Likert-type scale, with 0 as rarely or none of the time (less than 1 day) and 3 as all of the time (5-7 days). Internal consistency and test–retest reliability are good (Björgvinsson, Kertz, Bigda-Peyton, McCoy, & Aderka, 2013). Cronbach’s alpha in the current study is .84. Björgvinsson et al. suggest that a cutoff of 15 has the best “sensitivity” and “specificity.”
The PTSD Checklist (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996) is a 17-item self-report questionnaire that measures the three symptom clusters of PTSD, as defined by the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994) in the previous month. The symptom clusters are reexperiencing (five items), avoidance/numbing (seven items), and hyperarousal (five items). The questionnaire was developed with a sample of primarily women sexual assault and motor vehicle accident victims. Items (e.g., “In the past month how much have you been bothered by repeated, disturbing memories, thoughts, or images of abuse or violence?”) are endorsed with a 0 to 4 Likert-type scale with 0 meaning not at all and 4 meaning extremely. Blanchard et al. recommend a clinical cutoff of 44. The scale has good psychometric properties (Cronbach’s α = .94; Blanchard et al., 1996). Cronbach’s alpha in the current study is .92.
Research Procedures
The first wave of The Healing Journey data collection commenced in 2005, with five additional waves of data collected every 6 months over 3.5 years. To provide a baseline for the subsequent longitudinal data analysis (Tutty, et al., in preparation), the current descriptive data were from the first two waves, with demographic characteristics and information on the nature of the IPV experienced coming from Wave 1 and mental health measures collected in Wave 2. At each wave, the questionnaires were administered face to face, with female interviewers reading the questions and recording the answers to ameliorate any problems with literacy. The more than 50 interviewers were a mix of upper level undergraduate and graduate university students and professionals from the communities surveyed, with training the responsibility of each province. The interviews lasted from 1 to 2 hr and the study participants were provided an honorarium of Canadian $50 each time. To minimize attrition, interviewers contacted the women at least once between waves, and each interviewer interviewed the same women as long as both remained part of the study.
Data Analysis
Categorical descriptive data were analyzed with Pearson’s chi-square analysis, with effect sizes calculated with Cramer’s V, computed when the chi-square is significant. Standardized residuals were calculated to identify the category differences responsible for the statistically significant chi-square (Field, 2009). Numerical data were compared with ANOVAs, with Bonferroni procedures as post hoc tests when findings were statistically significant. Effect sizes were interpreted using Rea and Parker’s (2002) suggested benchmarks of below .10 as a “negligible” association, between .10 and below .20 as a “weak,” between .20 and below .40 as a “moderate,” and between .40 and below .60 as a relatively “strong” association (p. 203).
Because of the interactions between many of the variables of interest, the final analysis was a MANCOVA on the scores on the standardized mental health measures, with the Composite Abuse Scale–Total score as a covariate, and racial group, disability status, and child abuse history as independent variables.
Results
Racial and Ethnic Populations and the Experience of Intimate Partner Abuse
With attrition of 70 women from Wave 1 (N = 665) to Wave 2, the total sample for the current study is 595, with 205 from Manitoba (34.5%), 185 from Saskatchewan (31.1%), and 205 from Alberta (34.5%). The 70 women who recidivated between Waves 1 and 2 differed from the women who remained in the study in the following ways: (a) they were significantly younger (33.7 vs. 36.7 years on average), (b) they had lower yearly incomes (Canadian$14.964 vs. Canadian$22,429), (c) more of them worked full time (22.6% vs. 7.5%), (d) more were from medium-sized centers (30,000-99,999; 25.7% vs. 12.6%), and (e) more had disabilities (57.1% vs. 42.5%). Notably, though, the information presented from both Waves 1 and 2 represents the first full data capture.
The women were from diverse, self-identified racial and ethnic origins: 263 (44.8%) White (self-reported as European origins, White, or Caucasian), 292 (49.7%) Indigenous (First Nations = 218, Métis = 73, Inuit = 1), and 32 (5.5 %) visible minority (the largest groups being African Canadian = 13, South Asian = 7, and Latin American = 8). As can be seen in Table 1, the average age of the women was 36.7 years (SD = 10.9 years); however, the White women were significantly older (M = 38.4 years, SD = 11.4 years) than the Indigenous women (M = 35.1 years, SD = 10.5 years), with the women from visible minority origins in the middle (M = 37.8 years, SD = 10.3 years; F = 6.6, p < .001) but not statistically different in age from either White or Indigenous women. The majority (90.3%) had children, with 70% (n = 370) of these aged 18 years or below (M = 9.2 years, SD = 5.1 years). The 162 adult children were an average of 27.8 years of age (SD = 8.2 years). There were no differences between the race/ethnic groups in either the percentage who were mothers or the percentage with children above and below the criterion for adulthood.
Comparison of Women’s Demographics Across Population Backgrounds.
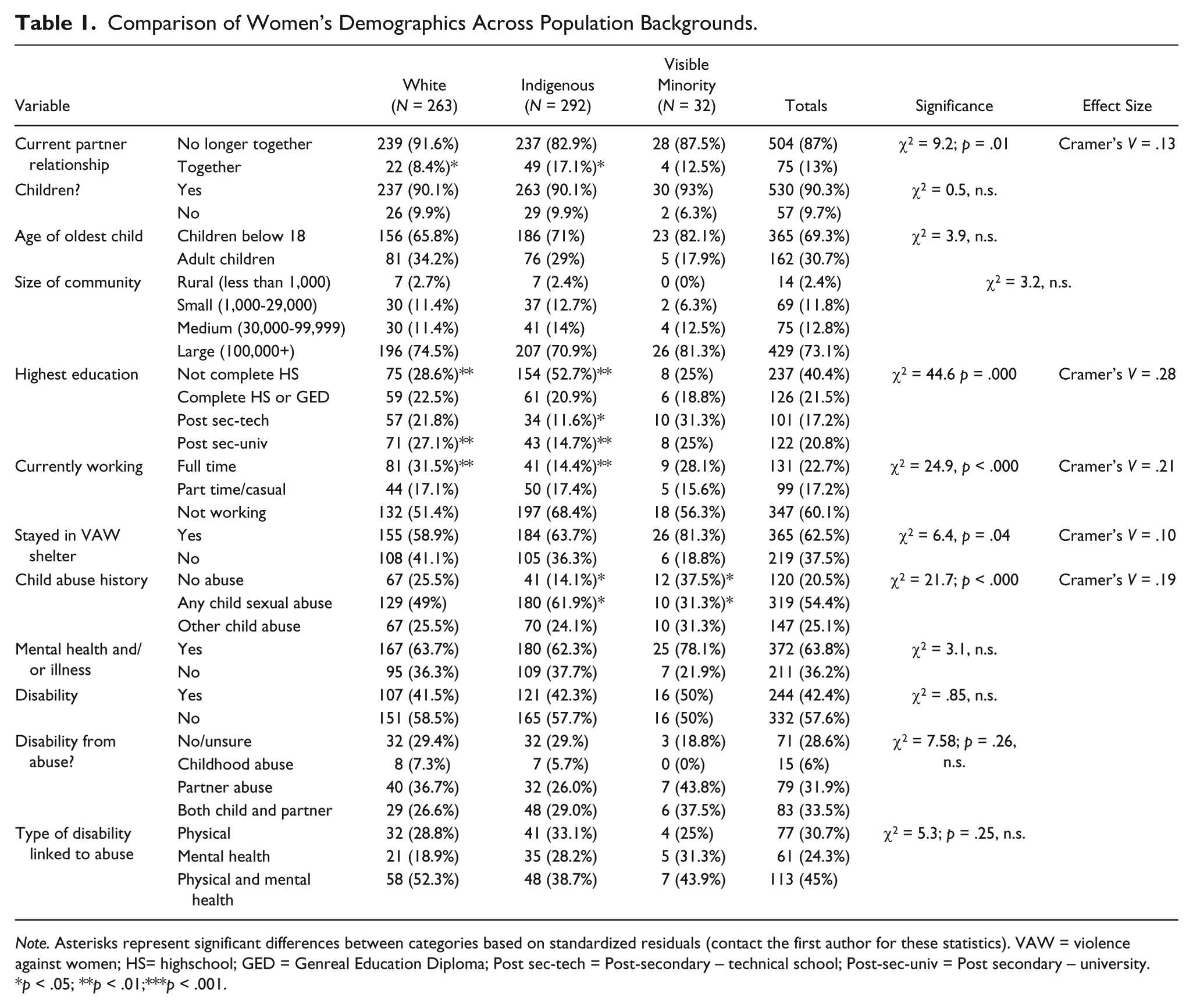
Note. Asterisks represent significant differences between categories based on standardized residuals (contact the first author for these statistics). VAW = violence against women; HS= highschool; GED = Genreal Education Diploma; Post sec-tech = Post-secondary – technical school; Post-sec-univ = Post secondary – university.
*p < .05; **p < .01;***p < .001.
The majority of women (87%) no longer lived with their abusive partners, being ex-common-law (n = 195, 32.8%), separated/divorced (n = 186, 31.3%), ex-boyfriend/girlfriend (n = 98, 16.5%), or partner deceased (n = 5). The minority who remained with abusive partners (13%) included 41 (6.9%) married, 36 (6.1%) common-law, and 33 (5.6%) boyfriend/girlfriend. More women of Indigenous origins were still with their abusive partners compared with the other two groups, although this was a weak effect (χ2 = 9.2, p = .01, Cramer’s V = .13).
Total average yearly family income from all sources in the last year was Canadian$22,504 (SD = Canadian$25,256), but there were significant differences between all three groups (F = 6.4, p < .001), with visible minority women reporting the highest average total yearly income (M = Canadian$27,300, SD = Canadian$36,804), White women next (M = Canadian$26,109, SD = Canadian$26,272), and then women of Indigenous descent (M = Canadian$18,504, SD = Canadian $21,867). Poverty lines are complicated to calculate; however, in an analysis of the economic circumstances of a subset of 414 women from this study at Wave 6, DeRiviere (2014) calculated that 52.2% of the women lived under the poverty line.
Highest level of education attained varied considerably across the sample; 40% of the women had not completed high school, whereas 38% had some postsecondary education (χ2 = 44.6, p = .000, Cramer’s V = .28). More women of Indigenous origins than White women had not completed high school and not attended postsecondary education, a moderate effect. Similarly, significantly fewer women of Indigenous origins than White women were working full time, also a moderate effect (χ2 = 24.9, p < .000, Cramer’s V = .21).
More than one third (37.8%) of the women had never stayed in a VAW shelter (see Table 1). A higher proportion of the women from visible minority populations had resided in a shelter (81% compared with 64% Indigenous and 59% White; χ2 = 6.4, p = .04, Cramer’s V = .10, a weak effect).
Because of the previously acknowledged long-term consequences of child sexual abuse, the women were classified as reporting no child abuse, any child sexual abuse (54.3%), and child abuse excluding sexual abuse (including physical abuse [56.2%], emotional/psychological abuse [66.4%], neglect [40%], and/or witnessing violence between parents or other family members [57.6%]). Although 79.5% of all women had been abused as children in some or multiple ways, significantly fewer from visible minority groups experienced child abuse compared with women of Indigenous backgrounds and fewer had been sexually abused, a weak effect (χ2 = 21.7, p < .000, Cramer’s V = .19).
Almost two thirds (63.7%) reported having some serious medical conditions and/or long-term illnesses. A complete list of the self-reported conditions is beyond the scope of the current submission, especially because a number of women disclosed multiple conditions. However, to highlight the serious and life-threatening nature of the medical concerns disclosed by some women, the most often mentioned physical illnesses were irritable bowel syndrome/Crohn’s disease (n = 36), chronic fatigue syndrome/fibromyalgia (n = 28), and hepatitis C and HIV (n = 25). Of the mental health issues identified, the most common were depression (n = 170), PTSD/anxiety (n = 103), and addictions (n = 74). Also, 13 women mentioned bipolar disorder and four others self-disclosed a diagnosis of borderline personality disorder.
The illnesses or mental health conditions reported by the women were coded as disabilities if women noted that they affected their mobility or employability, resulting in 244 of the women (42.4%) being classified with a disability. Of these, 71.4% attributed the disability to their abuse history: 6% to childhood abuse, 31.9% to partner abuse, and 33.5% to both partner and child abuse. Of the women who linked the disability to an abuse history, the largest proportion (n = 113, 45%) described both mental health and physical conditions, 61 women (24.3%) described only mental health issues, and 77 women (30.7%) listed only physical illnesses. Race/ethnic group was not related to disability status.
As can be seen in Table 2, all average scores on the CAS subscales were significantly higher than the suggested cutoff scores (Hegarty et al., 2005). With respect to average scores on the mental health scales, none (SCL-10, CES-D-10, PTSD Checklist) was in the clinical range for any of the race/ethnic groups. Moreover, few differences were identified between the three race/ethnic groups on the CAS; visible minority women reported the most emotional abuse compared with women of Indigenous origin, who scored lowest. Indigenous women reported higher CAS-physical abuse scores than White women, who scored the lowest.
Scores on Standardized Measures by Population Background.
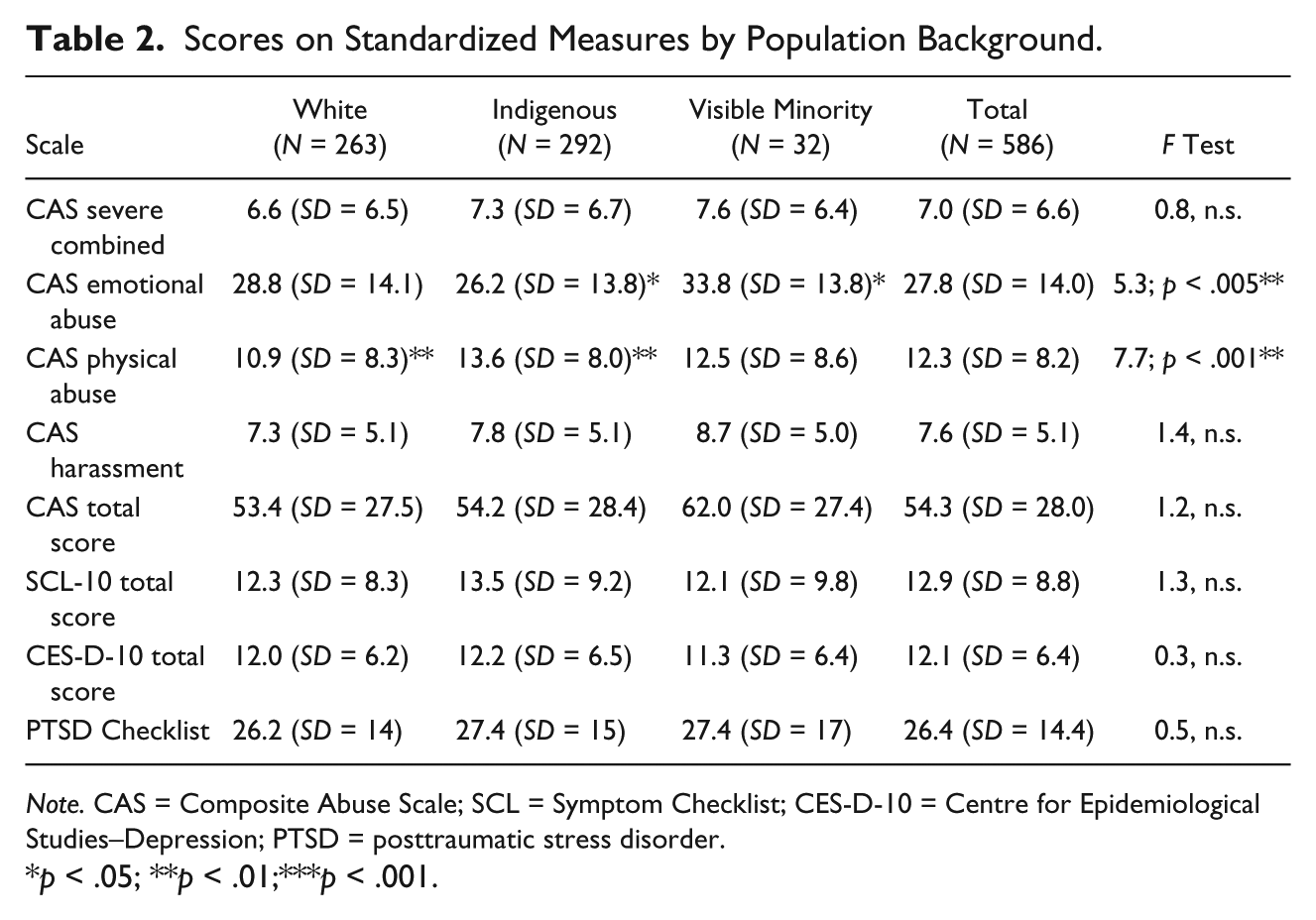
Note. CAS = Composite Abuse Scale; SCL = Symptom Checklist; CES-D-10 = Centre for Epidemiological Studies–Depression; PTSD = posttraumatic stress disorder.
*p < .05; **p < .01;***p < .001.
Interactions Between Disability Status, Intimate Partner Abuse, and Mental Health
The mental health scales and the CAS total were correlated and the SCL-10, CES-D-10, and PTSD Checklist scores were all significantly interrelated (with rs = .716-.749). Correlations with the mental health scores and the CAS total were numerically lower (rs = .14-.28) but still significant (ps of .01). Because of the interconnections between these main variables and their possible associations with the mental health measures, we conducted a MANCOVA on the standardized mental health measures as dependent variable, with the CAS total score as a covariate, and disability status (yes/no), child abuse history (yes/no), and racial/ethnic group as independent variables.
As seen in Table 3, disability status was the only significant variable, with women without disabilities reporting significantly less dysfunctional scores on the SCL-10, CES-D-10, and PTSD Checklist than women without. Neither racial/ethnic group nor child abuse history nor any interaction (including interactions with disability status) was significant.
MANCOVA of Mental Health Scores by IPV, Racial Group, Disability, and Child Abuse.
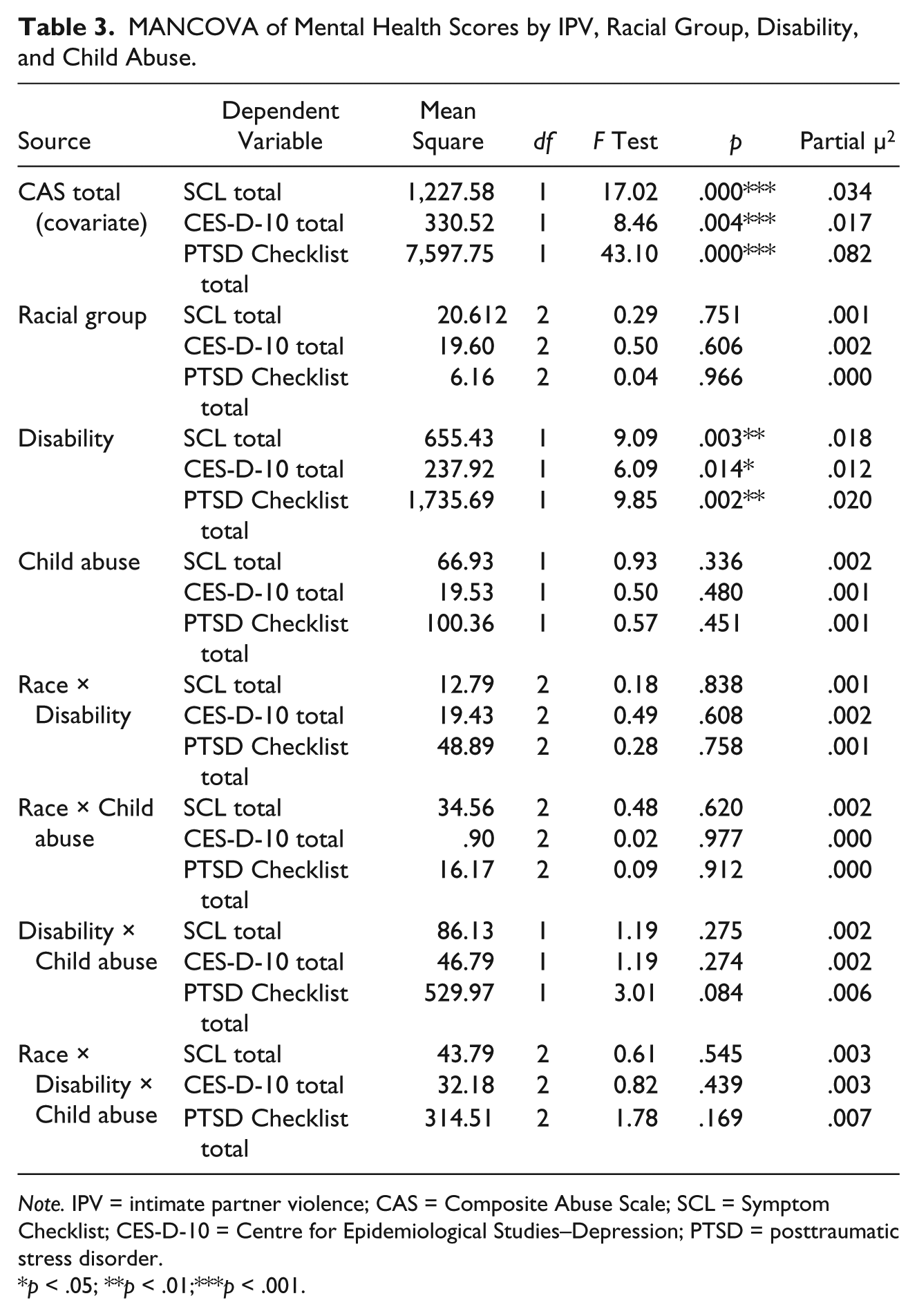
Note. IPV = intimate partner violence; CAS = Composite Abuse Scale; SCL = Symptom Checklist; CES-D-10 = Centre for Epidemiological Studies–Depression; PTSD = posttraumatic stress disorder.
*p < .05; **p < .01;***p < .001.
Discussion
Consistent with the extensive literature on women whose partners have abused them, those in The Healing Journey study has complicated lives with many reporting childhood abuse histories (79.5%), physical illnesses/mental health conditions (63.8%), and disabilities (42.4%). Intersectional studies usually anticipate finding differences in the variables associated with vulnerabilities and disadvantage, but similarities are also of interest (Cole, 2009). The general lack of differences between the three racial/ethnic groups either descriptively or on scores on the standardized measures is notable, but important not to overlook given that the women shared a history of IPV. Exceptions were that more women of Indigenous origins had lower incomes, were unemployed, still resided with an abusive partner, and reported higher levels of physical abuse (similar to Brennan, 2011). Visible minority women reported more serious emotional abuse, less child abuse, and a larger percentage had stayed in VAW shelters, which may be an artifact of how women from diverse cultures were recruited for the current study. Also, the subsample of visible minority women is relatively small and, therefore, caution in interpreting the significance tests is warranted. Despite these few areas, some of which can be attributed to structural factors such as poverty, discrimination, and Canada’s colonial history of oppression toward Indigenous people, there were no statistically significant differences across racial/ethnic groups on measures of depression, general mental health, or PTSD symptoms.
As noted, the women in the current study were not, on average, in the clinical ranges on the depression, symptom checklist, or PTSD measures. This result differs from articles implying that abused women commonly have serious mental health concerns, but that did not use clinical cutoffs (i.e., Lacey et al., 2013; Perez & Johnson, 2008). Our finding is consistent with studies that used clinical cutoffs. Specifically, depression and anxiety scores below clinical cutoffs were reported in one study (Ferrari et al., 2014), and in others, only 24% of the sample reported clinical levels of PTSD (Coker et al., 2005) and 38% reported mild depression (Nicolaidis et al., 2009). Together, these studies and ours contrast with an impression from a cursory read of the literature that women abused by partners have numerous mental health concerns. It underscores the importance of using valid cutoffs in research on mental health and IPV to identify those who may require the attention of mental health professionals.
On the face of it, the mostly nonclinical scores on the depression and PTSD standardized scales may seem to contradict the women’s self-reports, which identify depression and PTSD as the most common mental health problems. However, depression and anxiety symptoms do not necessarily result in diagnoses of these disorders. Moreover, mental health symptoms improve substantially for many women in a relatively short time with interventions such as VAW shelters or support groups (Rinfret-Raynor & Cantin, 2007; Tutty, 2015; Tutty, Babins-Wagner & Rothery, 2015). As the women were recruited through VAW shelters and other services for women who have experienced IPV, one could anticipate some “healing” by the time we interviewed them. Thus, it is important not to stereotype women whose partners have abused them as having long-standing mental health problems.
The high proportion of women in the Healing Journey study who reported histories of child abuse (79.5%), particularly child sexual abuse (54.4%) and disabilities (42.5%), is congruent with other research (Ballan et al., 2014). Although Indigenous children are acknowledged to have suffered significant child sexual abuse (Libesman & McGlade, 2016), in the current study, there were only differences in the proportion of Indigenous and visible minority groups reporting a child sexual abuse history, with no statistically significant difference between the samples of White and Indigenous women.
Having a disability was the only social location in the current study that was significantly related to more dysfunctional mental health scores and severity of IPV, consistent with a number of studies (Barrett et al., 2009; Breiding & Armour, 2015; Brownridge, 2006; Cohen et al., 2005; Hahn et al., 2014; Yoshida, et al., 2011). Thus, it is important for professionals to assess disability status when working with women abused by intimate partners. However, Baladerian (2009) has argued that there is insufficient discussion of disability in the IPV literature and few services are specific to women with disabilities and an IPV history (Ballan et al., 2014; Lund, 2011). Professionals such as social workers are not routinely educated about IPV (Black, Weisz, & Bennett, 2010), and women with disabilities have estimated that only 15% of health providers assessed for IPV (Curry et al., 2011). Clearly, this is a large gap in service provision. Finally, women with disabilities are often further disadvantaged by structural inequalities associated with race, gender, age, and socioeconomic status (Ballan et al., 2014), which could contribute to the lower levels of psychological well-being associated with women with disabilities in our study.
Limitations and Strengths
Without random selection of study participants, the results may not be generalizable to other women abused by intimate partners within the Canadian prairie provinces, particularly those not seeking some form of assistance for IPV. This is the case for much research in the field that relies on convenience samples of women with IPV histories from shelters or counseling agencies. Furthermore, we cannot assume that the self-reported physical and mental health conditions on which the disability classification was based had been corroborated by a formal diagnosis. This, however, does not undermine the importance of the results involving disability status. Although a goal of the project was to recruit a substantial sample of visible minority women, the small proportion that volunteered is a limitation. This may be a function of our recruitment methods as some have concluded that racial minority women are less likely to use social services (Hyman et al., 2009). Thus, future researchers should develop alternative recruiting strategies.
One strength of this study is that we used purposive sampling to include a larger number of women associated with marginalized groups than would result, had we used random sampling. This afforded a greater representation of marginalized women within the sample and statistical analysis is often not possible in studies that use other sampling methods. This is critical for research adopting an intersectional framework (e.g., Else-Quest & Shibley Hyde, 2016). For example, we made efforts to recruit in rural and remote locations not ordinarily included in large studies. Also, we recruited a sizable proportion of women from Indigenous origins, as this is an important group in Canada’s large and unique prairie provinces. Although they are included in national studies such as the GSS, Indigenous women are not sufficiently represented in other IPV research. A second strength was the use of standardized measures of mental health functioning as it clarified that, although women self-reported depression, other mental health symptoms, and PTSD, on average, none were in the clinical ranges.
Conclusion
This research aimed to make visible the experiences of both marginalized and mainstream women. Women abused by intimate partners vary with respect to whether or not they are dealing with mental health symptoms, physical health issues, disabilities, and child abuse histories. This study supports the need to avoid assuming that these women suffer from long-lasting mental health issues to a degree suggesting the need for clinical intervention, and underscores the need to assess disability status. Although few differences with respect to race/ethnic backgrounds were identified, it remains important to address cultural beliefs and help-seeking behaviors when assisting individual women. The structural inequalities that Indigenous and some visible minority women face must be understood to ensure their well-being.
Although considerable research has documented the traumas and negative consequences for women who have experienced IPV, this puts researchers and service providers at risk of assuming that many such women have mental health disorders. This may blind those aiming to help women’s strengths and coping abilities to both endure abuse and, ultimately, decide to leave, if that is the best decision. Because the women in the Healing Journey study differed in terms of whether or not they still resided with their abusive partners and, if having left, how long ago that occurred, we cannot know whether any clinically significant mental health concern was present earlier and was resolving or simply was not present despite the IPV. Finding ways to support the women’s diverse circumstances, histories, and strengths (Anderson, Renner, & Danis, 2012; Tutty, 2006) remains a critical aspect of both research and clinical interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Social Sciences and Humanities Research Council (SSHRC) Community University Research Alliance (CURA); Alberta Centre for Child, Family, & Community Research; Alberta Heritage Fund for Medical Research; the Prairieaction Foundation; and TransCanada Pipelines.