
Abstract
Numerous school-based prevention programs have been developed by scientists and practitioners to address sexual violence in adolescence. However, such programs struggle with two major challenges. First, the effectiveness of many well-established practitioner programs has not been rigorously evaluated. Second, effective scientific programs may be hard to implement into everyday school practice. Combining the knowledge of scientists and practitioners in a scientist-practitioner program could be a helpful compromise. The aim of the present study is to evaluate the effects of a scientist-practitioner program and a practitioner program using a cluster-randomized experimental design. Twenty-seven school classes were randomly assigned to either one of two programs or a control group. Outcome variables (knowledge, attitudes, behavior, and iatrogenic effects) were assessed at pretest, posttest, and a 6-month follow-up for 453 adolescents (55% female, Mage = 14.18). Short-term effects were found in both programs regarding general knowledge, knowledge of professional help, and victim-blaming attitudes. Long-term effects were found in both programs regarding general knowledge and knowledge of professional help and, in the practitioner program, in a reduction of victimization. No other effects were found on attitudes and behavior. No iatrogenic effects in the form of increased anxiety were found. Both the scientist-practitioner and the practitioner program show promise for the prevention of sexual violence in adolescence; in particular, the practitioner program may be a more cost-effective method.
Introduction
Sexual violence (SV) is a worldwide health problem that can occur at every stage of life (Barth, Bermetz, Heim, Trelle, & Tonia, 2013; Krebs et al., 2016; Leen et al., 2013; Pereda, Guilera, Forns, & Gómez-Benito, 2009). The negative consequences of SV have been thoroughly documented (Exner-Cortens, Eckenrode, & Rothman, 2013; Foshee, Reyes, Gottfredson, Chang, & Ennett, 2013; Lormand et al., 2013; Oddone Paolucci, Genuis, & Violato, 2001; Roberts, Klein, & Fisher, 2003; Smith, White, & Holland, 2003; Widom, DuMont, & Czaja, 2007). While help services, such as therapy and counseling, aim to assist those who have already experienced SV, prevention offers the opportunity to reduce the rates and consequences of SV in the first place. Especially helpful may be school-based prevention programs, as they can reach many students and therefore may help reduce SV through societal impact. However, many SV prevention programs lack rigorous evaluation and are based on practice experience and not on scientific evidence (Anderson & Whiston, 2005; DeGue et al., 2014; Yeater & O’Donohue, 1999). In contrast, evidence-based programs for adolescents such as Safe Dates (Foshee et al., 2005) and Shifting Boundaries (Taylor, Stein, Mumford, & Woods, 2013) show promising results in the reduction of SV. However, these programs require certain conditions that may be difficult to implement into everyday school practice because many schools have limited time for extracurricular programs (Greytak, 2003). Therefore, the present study aims to evaluate the effectiveness of (a) a well-established but not yet rigorously evaluated practitioner program (PP), which takes into account the limitations of everyday school settings, and (b) a scientist-practitioner program (SPP), which takes into account both the evidence of prevention research and the practical time limitations in schools.
Basile, Smith, Breiding, Black, and Mahendra (2014) defined SV as “a sexual act committed or attempted by another person without freely given consent of the victim or against someone who is unable to consent or refuse” (p. 11). This includes, for instance, forced or drug-facilitated penetration of a victim, nonphysically pressured unwanted penetration, intentional sexual touching, or nonphysical acts of a sexual nature. However, there is no common scientific definition of SV, which makes it difficult to give an accurate overview of its prevalence (Leen et al., 2013).
SV can occur at every stage of life, but high rates of SV victimization and perpetration have often been reported during adolescence (Leen et al., 2013; Roberts et al., 2003; Smith et al., 2003; Stöckl, March, Pallitto, & Garcia-Moreno, 2014; Williams et al., 2014; Young, Grey, & Boyd, 2009). Williams and colleagues (2014) found in a U.S. sample that 22% of female and 13% of male adolescents experienced some form of SV victimization. Also, SV victimization in dating situations, such as in first romantic partnerships, have been investigated more in recent years (Cutbush, Williams, & Miller, 2016; Garthe, Sullivan, & McDaniel, 2017; Hamby, Finkelhor, & Turner, 2012; Lundgren & Amin, 2015; Stöckl et al., 2014). In Germany, the Federal Centre for Health Education (BZgA) found that 20% to 22% of female and 4% to 6% of male adolescents have experienced some form of SV victimization in dating situations (Heßling & Bode, 2015). However, there is still limited data on the prevalence of SV during adolescence in Germany, and in general, prevalence data need to be compared with caution, because frequency reports often use different study designs. For example, Williams and colleagues (2014) used a 12-month prevalence design, whereas the BZgA used lifetime prevalence (Heßling & Bode, 2015). Although it is difficult to make an exact comparison between countries and studies, the current data nevertheless suggest a high SV victimization rate in Germany, which seems to be comparable with U.S. studies.
Because Krahé (2009) found that only a small proportion of SV derives from dating violence, it is reasonable to take into account other forms of SV. Furthermore, the high rates of SV victimization in adolescence call for effective prevention strategies, which could help reduce the rate of SV victimization in dating and other situations. Currently, the only effective programs for reducing SV victimization and perpetration have targeted adolescents, suggesting that adolescence may be a critical and important time to intervene (DeGue et al., 2014; Whitaker, Murphy, Eckhardt, Hodges, & Cowart, 2013).
Many prevention programs adopt universal prevention strategies, which “can be advocated confidently for the general public” (Gordon, 1983, p. 108). Furthermore, a lot of programs target specific age groups and can be conducted in the school setting (Fryda & Hulme, 2015; Topping & Barron, 2009). Also, school-based programs have the advantage of reaching students more easily and thus can be implemented in a cost-efficient manner (Greytak, 2003; Topping & Barron, 2009). To give a brief overview of school-based prevention of SV, we briefly describe the general conditions and evaluation results of programs targeting adolescents.
General Conditions of School-Based Prevention
Certain general conditions, namely, student participation, number of sessions, and gender of the audience, seem to have an impact on program effectiveness (Anderson & Whiston, 2005; Davis & Gidycz, 2000; Vladutiu, Martin, & Macy, 2011). In general, active participation in programs, for instance, through role-playing, results in greater effect sizes (Davis & Gidycz, 2000). However, the extent of participation differs due to the mode of presentation, which is most often didactic with a form of discussion (Morrison, Hardison, Mathew, & O’Neil, 2004); some programs have featured video or slide presentations (Hilton, Harris, Rice, Krans, & Lavigne, 1998; Lavoie, Vézina, Piché, & Boivin, 1995; Pacifici, Stoolmiller, & Nelson, 2001), role-playing (Pacifici et al., 2001; Wright, Akers, & Rita, 2000), and worksheets (Hilton et al., 1998).
Prevention research has also shown that programs with several sessions show greater effect sizes in contrast to programs with one brief session (Davis & Gidycz, 2000). However, the number of sessions in evaluation studies varies widely (DeGue et al., 2014), which makes it difficult to give an ideal reference number. Also, many programs are implemented in one brief psychoeducational session (DeGue et al., 2014), which may be, in part, due to everyday school restrictions that limit time for extracurricular programs (Edwards & Hinsz, 2014; Greytak, 2003). Although it seems reasonable that implementing several sessions may result in stronger outcomes, limitations within everyday school practice call for prevention programs that are as brief as possible.
Regarding audience, most programs targeting adolescents implement mixed-gender groups (Morrison et al., 2004); however, research has shown conflicting findings on whether mixed-gender or single-gender audiences yield higher effects in SV outcomes (Espelage, Low, Polanin, & Brown, 2015; Vladutiu et al., 2011; Wolfe et al., 2009). A combination of mixed- and single-gender aspects seems to be promising, as it includes advantages of both approaches (Anderson & Whiston, 2005; Vladutiu et al., 2011).
In sum, although prevention research has shown the benefits of various general conditions, such as several sessions, active participation by students, and maybe a combination of mixed-gender and single-genders aspects, these conditions are difficult to implement into everyday school practice due to time restrictions (Edwards & Hinsz, 2014; Greytak, 2003). Thus, a scientist-practitioner approach that takes into account the results of previous prevention research, and also, the limitations of school practice could be a realistic and helpful compromise. Also, only a few studies have investigated differences in certain general conditions for prevention programs. For example, Taylor and colleagues (2013) contrasted a classroom intervention with a building-based intervention and found that only the building-based intervention showed significant effects. It is nessescary to continue investigating certain general conditions that may affect program effectiveness.
Evaluation of Prevention Programs Targeting Adolescents
The overall findings from reviews show that school-based SV prevention programs for adolescents are effective (DeGue et al., 2014; Fryda & Hulme, 2015; Morrison et al., 2004; Topping & Barron, 2009). Morrison and colleagues (2004) found seven distinct outcome variables in school-based SV prevention programs aimed at adolescents including (a) enhanced general knowledge about SV; (b) enhanced knowledge about professional help services; (c) reduced attitudes in rape myths, such as victim-blaming attitudes; (d) increased skills/strategies developed as a result of the program, such as perceptions and appraisal of personal space; (e) altered dating behavior, such as increased use of communication and conflict skills; (f) reduced victimization; and (g) reduced perpetration.
Of these, the most commonly investigated outcome variables in adolescent SV prevention are changes in knowledge and attitudes (Daigneault et al., 2015; Ting, 2009). Ting (2009) found in a meta-analysis that effect sizes for changes in knowledge (r = .35) and attitudes (r =.32) were similar in magnitude.
Recently, some studies have focused more on behavioral outcomes (Daigneault et al., 2015; Foshee et al., 2005 Taylor et al., 2013). For example, evidence-based programs that have shown a positive impact on SV behavioral outcomes are the Safe Dates program (Foshee et al., 2005) and the Shifting Boundaries program (Taylor et al., 2013). The Safe Dates program consists of nine mixed-gender sessions of 50 min, a 45-min theater play performed by students, and a poster contest. The nine sessions include the following topics: (a) defining caring relationships; (b) defining dating abuse; (c) why do people abuse? (d) how to help friends; (e) helping friends; (f) overcoming gender stereotypes; (g) equal power through communication; (h) how we feel, how we deal; and (i) preventing dating sexual abuse. Although the program focuses on dating violence, there are many overlaps to SV prevention because they tackle similar risk-factors. Overall, Foshee and colleagues (2005) found that this program does indeed reduce SV victimization.
The Shifting Boundaries program (Taylor et al., 2013) consists of a classroom curriculum with six sessions including the following topics: (a) construction of gender roles, (b) setting and communicating of boundaries in interpersonal relationships, (c) healthy relationships, (d) the role of bystander as intervener, (e) consequences of perpetrating, and (f) state and federal laws related to dating violence and sexual harassment. The program focuses on dating violence and sexual harassment and therefore integrates factors for both forms of violence. The program also has a school-level intervention affecting the entire school building. While Taylor and colleagues (2013) did find that SV was reduced when the classroom curriculum was combined with the school-level intervention, they did not find positive effects from the classroom curriculum only.
Some studies have investigated the iatrogenic effects of prevention programs, such as an increase in anxiety about SV, but did not find any negative outcomes (DeGue et al., 2014; Fryda & Hulme, 2015). However, it is still important to control for possible iatrogenic findings such as anxiety, because some have questioned whether the benefits of prevention programs actually outweigh possible negative effects (Fryda & Hulme, 2015). In addition, many SV prevention studies lack a follow-up measure, a control group, and/or some form of controlled randomization (DeGue et al., 2014; Fryda & Hulme, 2015), which show the need for more rigorous prevention research.
Also, as Sears, Byers, Whelan, and Saint-Pierre (2006) pointed out, many SV evaluation studies for adolescents have relied on measures that were initially designed for college students and do not particularly reflect adolescents’ ideas of sexual and/or dating violence. Thus, several authors have devised their own outcome measures or heavily adapted standardized tools (Fryda & Hulme, 2015). Furthermore, many existing instruments are expressed in a gender-stereotypical way. For example, the Illinois Rape Myth Acceptance Scale (McMahon, 2010) consists mostly of items in which females are possible victims and males are possible perpetrators. Although female victimization rates are on average higher, many male adolescents have experienced severe forms of SV, which is why we consider gender sensitiveness in evaluation measures and program delivery to be very important.
In Germany, SV prevention programs generally include the same components documented by Anglo-American literature, but only a few prevention programs have been rigorously evaluated (Krahé & Knappert, 2009). The first aim of the present study is to provide a systematic and rigorous evaluation of a universal SV prevention program for adolescents. Although SV prevention research has shown that certain adolescents are more at risk of SV than others (e.g., Garthe et al., 2017), targeting specific subgroups during a school curriculum in Germany could easily lead to stigmatization. This is why we preferred a universal prevention programing approach targeting all adolescents instead of a selective prevention approach. Based on the evaluation model of Kirkpatrick and Kirkpatrick (2006), we included outcome variables at different evaluation levels, thus allowing for a more detailed interpretation of program effectiveness. A second aim is to contrast two versions of the prevention program on their short- and long-term effectiveness.
Evaluation Model
To make accurate conclusions about the effectiveness of a prevention program, we applied a utility-oriented evaluation model. In this model, as described by Kirkpatrick and Kirkpatrick (2006), there are four distinct and hierarchical levels for program evaluation. The first level, reaction, describes the overall satisfaction with and acceptance of the prevention program. Positive effects on the reaction level, namely, satisfaction, is an essential precondition for effects on the other levels. The second level, learning, considers effects with respect to knowledge, attitudes, and other nonbehavioral constructs. The third level, behavior, describes effects on concrete behavior, such as victimization and perpetration. The fourth level, results, includes long-term changes on a societal level. The present study examines the effects of the prevention program on the first, second, and third levels. At the first level, we investigated participants’ satisfaction with the program. At the second level, we investigated general knowledge about SV, knowledge about professional help, victim-blaming attitudes, anxiety, and personal space perception and appraisal. The third level, behavior, was examined by participants’ victimization and perpetration.
Prevention Programs
Two school-based prevention programs were administered in cooperation with a local counseling center, (Zartbitter Muenster), which offers professional help for female and male victims of SV and offers multiple forms of SV prevention, for instance, through school-based programs or trainings for professionals in social work. The school-based prevention programs were delivered by a female and a male psychologist from the counseling center so that students had an explicit contact person for professional help in case of victimization and also so that female and male students were addressed in a gender-sensitive way. Both facilitators delivered all sessions and had several years of experience in the practice of SV prevention and in SV prevention research, as they conducted an evaluation of an SV prevention program prior to the study. Both programs focus on SV in general, although aspects of dating violence are also explicitly discussed. Teachers did not participate to create a private environment for adolescents. The programs were designed to be administered in either the eighth or ninth grade to coincide with developmental aspects of adolescence, such as first dating or sexual experiences.
The prevention programs applied in this study—the PP and the SPP—differed in their duration, active participation by students, and the gender composition of the audience, but they did not differ with regard to content. While both programs (PP and SPP) used a fixed curriculum to deliver the same program topics in every class in the same way, the programs are not standardized parts of an SV prevention program. The curriculum included the following content: (a) general knowledge about SV: providing a definition and general information about SV; (2) knowledge about professional help: providing information about local and online professional help services; (3) victim blaming: discussing rape myths, in particular, victim-blaming attitudes, through various sample cases; and (4) personal space: raising the perception and appraisal for one’s own and others’ personal space through practical exercises.
The curriculum of the prevention programs included personal space because Taylor, Stein, and Burden (2010) found that it was a dimension in a factor analysis of SV attitudes. The authors also found that personal space attitudes influenced the outcomes of a gender violence and sexual harassment prevention program (Taylor et al., 2010). Furthermore, in Germany, exercises for personal space (or boundaries) have also been implemented in many specialized counseling centers’ programs for SV. For example, in an exercise for personal space where students actively participate, one of the program trainers walks slowly toward a student (who has consented to participate in the exercise), and the student then has to say “stop” whenever his or her personal space has been reached. With this exercise, trainers can highlight many different aspects of personal space perception and appraisal and also actively involve the students in the program. Finally, we considered personal space (and victim blaming) as an item that represent attitudes about SV, which allowed us to include in our evaluation model (based on Kirkpatrick & Kirkpatrick, 2006) several measures for the second level of learning (knowledge and attitudes).
As mentioned above, the programs we evaluated (PP and SPP) did not differ in content, but just in the way they were implemented (duration, active participation by students, and the gender of the audience). The PP, a combination of psychoeducational and active participation elements, was implemented in a mixed-gender audience only. Content was delivered via input presentations, worksheets, and quizzes. It consisted of one 90-min session; therefore, the PP is likely easy to implement into everyday school practice. For the SPP, the first SPP session was identical to the PP. The SPP also consisted of a second 90-min session, where students were separated by gender and dealt with the subject more actively through role-playing and group discussions. As previous prevention research has shown that active participation, the use of several sessions, and a combination of mixed- and single-gender aspects yield greater effect sizes for knowlede acquisition and attitude changes (Anderson & Whiston, 2005; Davis & Gidycz, 2000; DeGue et al., 2014; Vladutiu et al., 2011), the SPP therefore integrated elements that should facilitate the program’s effectiveness. Ideally, more sessions should be included in the SPP, but in Germany, an SV prevention program with more than two sessions would be hard to implement into everyday school practice because of the limited time available for extracurricular programs.
We hypothesized that in comparison with the control group, both program groups would (1) increase general knowledge of SV; (2) increase knowledge of professional help services; (3) reduce victim-blaming attitudes; (4) show no iatrogenic findings, namely, no increased anxiety regarding SV; (5) increase personal space perception and appraisal; (6) reduce rates of SV victimization; and (7) reduce rates of SV perpetration. As the SPP consisted of an additional session with more active participation and role-playing, which have been shown to be more effective regarding knowledge acquisition and attitude changes (Anderson & Whiston, 2005; Davis & Gidycz, 2000; DeGue et al., 2014; Vladutiu et al., 2011), we therefore hypothesized that the SPP would be more effective than the PP for the following outcome variables: (a) increasing general knowledge of SV, (b) increase knowledge of professional help services, (c) reducing victim-blaming attitudes, and (d) increasing personal space perception and appraisal. Finally, we investigated gender effects and short-term and long-term effects in a 6-month follow-up.
Method
Design and Procedure
Data were collected between May 2014 and June 2015 with a clustered randomized controlled pre–post follow-up design with two intervention groups and a control group. Classes were randomly assigned to either the SPP, the PP, or the control group. The participants in the intervention groups and the control group received a follow-up measure 6 months after the intervention. One week later, the control group received the PP. Thus, the control group received the PP 6 months and 1 week after the intervention groups.
A paper-and-pencil questionnaire was administered 1 week before the programs began (T1), immediately after the programs finished (T2), and after a 6-month follow-up (T3). The temporal intervals between each measurement were the same in the intervention groups and the control group. All measures remained identical across the time points. Data from all time points were matched using a personalized five-digit code that prevented personal identification. After matching the data, the code was deleted to ensure anonymity.
The study received approval from the local ethical committee of the Institute of Psychology and Sports Sciences of the University of Muenster. All participating schools, teachers, and students were given information on the purpose and design of the study, and about active consent. For consent, a research assistant verbally informed all possible participants about the study aims and afterward handed them a written consent form for them and their parents (or legal guardians) to sign. For study participation, active consent was required from adolescents and their parents (or legal guardians). We received active consent from 94.32% of all students (and their parents/legal guardians) in the schools. Forty-one students did not participate in the study because they did not give consent.
Both the PP and SPP were conducted in classes consisting of around 25 participants. Single-gender parts of the SPP were conducted in female-only and male-only groups, each consisting of around 10 to 15 participants. The two sessions of the SPP were separated by 1 week. For example, if a school had four participating classes with one class receiving the PP, two classes receiving the SPP, and one class in the control group, we delivered the PP and first session of the SPP in one day during the school. The second session of the SPP was then delivered a week after the first session. If there were several classes receiving the PP in a school, we held the programs back to back on a single day. Thus, contamination effects are possible, especially in the control group.
Sample
We excluded n = 74 participants as they indicated (dichotomous: yes, no) that they filled in the questionnaire “just for fun” in at least one of the measurements and another n = 154 participants dropped out at either at T2 or T3, resulting into complete data for N = 453 (55.0% female) participants. Participants were between 12 and 16 years old (M = 14.18, SD = 0.71), and attended the eighth (n = 174) and ninth (n = 279) grade. In total, 95% had German as their first language. Data were collected in 27 classes in five urban secondary schools (German Gymnasiums). The SPP group consisted of 10 classes (n = 166, 53.0% female), the PP group consisted of eight classes (n = 130, 56.1% female), and the control group consisted of nine classes (n = 157, 56.1% female).
Measures
All measures were self-reported. Many existing instruments did not fit the purpose of the study because they were written in a gender-specific way, that is, they suggested only female victimization and male perpetration and not vice versa. We therefore created new measures using gender-neutral item wording based on the principles of psychological test construction (Kaplan & Saccuzzo, 2012). To assure face validity, we generated items for each prevention goal, and therefore, we developed a process model. This method can be described as experience based, because we also used the opinions of SV prevention experts in the generation of the instruments (Kaplan & Saccuzzo, 2012).
We further used the Kirkpatrick and Kirkpatrick (2006) model as a guideline for developing each of the first three levels of evaluation: (a) reaction, (b) learning, and (c) behavior. As a measure for the first level, we generated items for satisfaction. The second level, learning, relied on items for knowledge (general knowledge, knowledge of professional help) and attitudes (victim blaming, personal space). The third level, behavior, was operationalized via items on victimization (dating situations, other situations) and perpetration (dating situations, other situations).
Previous SV prevention measures also served for some instruments. We used the Revised Version of the Illinois Rape Myth Acceptance Scale (McMahon, 2010) to generate the victim-blaming items, and we used items from the Shifting Boundaries evaluation measures on personal space (Taylor et al., 2010) to develop the personal space items. We used the list of tactics by Struckman-Johnson, Struckman-Johnson, and Anderson (2003) as the basis for generating the items on victimization and perpetration. Finally, we consulted with SV prevention experts and used SV research facts (i.e., prevalence of SV, strategies on SV perpetrators) and SV definitions from the Centers for Disease Control and Prevention (e.g., Basile et al., 2014) as the basis for generating the items on general knowledge. All measures were first tested in a pilot study.
Satisfaction
Students in the program groups rated their satisfaction for the program with six items (for instance, “Overall I’m satisfied with the program”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”) at T2. Higher scores indicate more satisfaction with the program. Cronbach’s alpha was α = .83.
General knowledge of sexual violence
A multiple-choice questionnaire was developed to assess students’ general knowledge of SV (for instance, “Sexual violence . . . A—can only happen if someone is physically forced to have sex, B—happens most often through physical violence, C—can be verbal and/or physical, D—cannot happen verbally”). The questionnaire was matched to the content of the prevention programs, and each item was presented with four alternative responses, out of which students had to mark the most appropriate one. The questionnaire consisted of 16 items. However, one item did not meet the inclusion criteria (item difficulty over .85 at T1), and therefore, the final questionnaire resulted in 15 items. Sum scores were calculated so that a maximum score of 15 could be achieved. Higher scores indicate more general knowledge about SV.
Knowledge of professional help
The knowledge of professional help services was measured with two items concerning local and online help services (“I know of professional local help services regarding sexual violence” and “I know of professional online help services regarding sexual violence”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). Higher scores indicate more knowledge of professional help services.
Victim-blaming attitudes
Victim-blaming attitudes were measured using adapted items from the “she asked for it” subscale of the Illinois Rape Myth Acceptance Scale (revised version, McMahon, 2010) using six items (for instance, “If a person gets raped while being drunk, it is his or her own responsibility”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). Cronbach’s alpha was α = .67 at T1, α = .76 at T2, and α = .72 at T3.
Anxiety
Iatrogenic findings in the form of anxiety about SV were measured using six items (for instance, “I am afraid that I could experience sexual assault”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). Cronbach’s alpha was α = .87 at T1, α = .88 at T2, and α = .89 at T3.
Personal space perception
We measured the perception of one’s own and others’ personal space using six items (for instance, “I clearly sense if someone is getting uncomfortably close to me”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). Cronbach’s alpha was α = .69 at T1, α = .77 at T2, and α = .78 at T3.
Personal space appraisal
We measured the appraisal of one’s own and others’ personal space using five items (for instance, “It’s important for me that I’m not getting uncomfortably close to someone else”) on a 5-point Likert-type scale ranging from 1 (“completely disagree”) to 5 (“completely agree”). Cronbach’s alpha was α = .66 at T1, α = .62 at T2, and α = .64 at T3.
Victimization
The 6-month prevalence of victimization was estimated based on six separate statements, which were arranged in a hierarchy of severity of victimization (for instance, “I have been kissed against my will”; “I have been forced to do sexual acts against my will”) on a 4-point Likert-type scale ranging from 1 (“never”) to 4 (“frequently”). Participants were instructed to rate these items according to the past 6 months and to differentiate between victimization in a dating situation (Cronbach’s alpha was α = .74 at T1, α = .83 at T2, and α = .86 at T3) and other situations (Cronbach’s alpha was α = .69 at T1, α = .79 at T2, and α = .81 at T3). Because the frequencies of such incidences were reported to be low, we transformed the items into dichotomized responses (“victimization” vs. “no victimization”) and computed two sum-score scales ranging from 0 (“no experienced victimization during the past 6 months”) to 6 (“experienced every of the six forms of SV in the past 6 months”) for victimization in dating situations and victimization in other situations.
Perpetration
The six statements for victimization were rephrased for perpetration (for instance, “I have kissed someone against his or her will”; “I have forced someone else to do sexual acts against his or her will”). Participants were instructed to rate these items according to the past 6 months and to differentiate between perpetration in a dating situation (Cronbach’s alpha was α = .84 at T1, α = .76 at T2, and α = .90 at T3) and other situations (Cronbach’s alpha was α = .76 at T1, α = .73 at T2, and α = .86 at T3). Because the frequencies of such incidences were reported to be low, we transformed the items into dichotomized responses (“perpetration” vs. “no perpetration”) and computed two sum-score scales ranging from 0 (“no perpetration during the past 6 months”) to 6 (“performed every of the six forms of SV in the past 6 months”) for perpetration in dating situations and perpetration in other situations.
Statistical Methods
To test the effectiveness of the two intervention groups in comparison with the control group, a series of mixed-effects linear regression models that included random effects for class and time and fixed effects for group and gender were computed. By specifying class as a random effect, we controlled for the clustered design of the data. Adjusted coefficients were estimated via restricted maximum likelihood estimation. Main effects for time, group, and gender and two-way interactions (i.e., Time × Group) were tested. Multilevel modeling was conducted with R using the lme4 package (Finch, Bolin, & Kelley, 2014). Effect sizes for the intervention effects in the form of Cohen’s d were computed according to Morris (2008) using the mean scores and standard deviations.
Results
Baseline and Descriptive Analyses
There were no significant group differences for age, gender, general knowledge, knowledge of professional help, victim blaming, anxiety, personal space perception, and personal space appraisal at baseline (T1). Table 1 shows the means and standard deviations for the outcome variables at T1, T2, and T3. At baseline (T1), students were able to correctly answer almost half of the items from the general knowledge of SV test. Furthermore, at T1, medium levels were found for knowledge of professional help and anxiety. In addition, at baseline, low victim-blaming attitudes and high levels of personal space perception and appraisal were found.
Means and Standard Deviations for Outcome Variables.
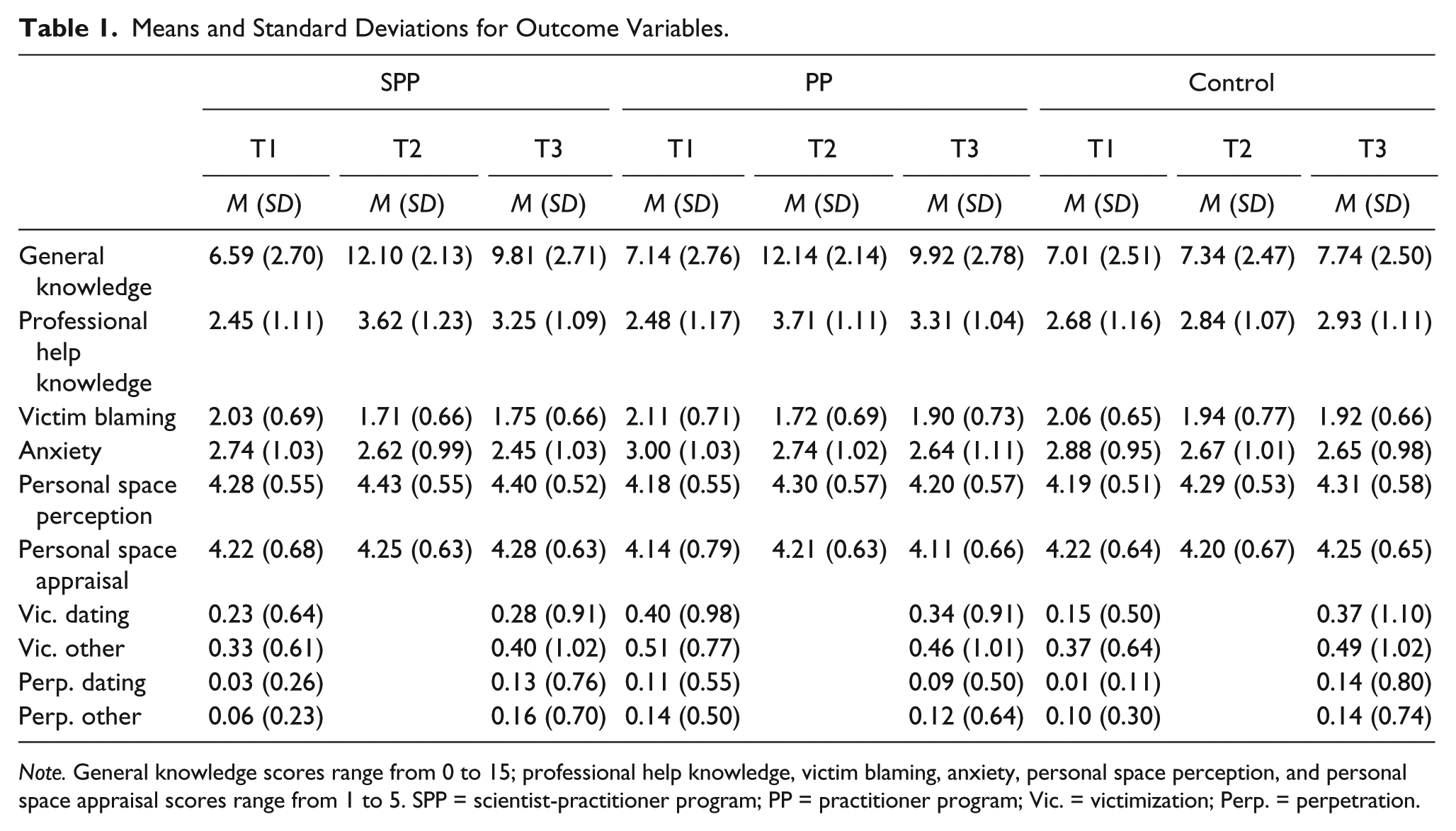
Note. General knowledge scores range from 0 to 15; professional help knowledge, victim blaming, anxiety, personal space perception, and personal space appraisal scores range from 1 to 5. SPP = scientist-practitioner program; PP = practitioner program; Vic. = victimization; Perp. = perpetration.
Attrition Analyses
A total of 98 students were lost in the posttest measure and another 130 students in the follow-up measure resulting in a total dropout rate of 33.48%. Dropout analyses showed no significant differences in group affiliation, age, school affiliation, victim blaming, anxiety of SV, victimization, and perpetration at T1. However, dropouts were significantly more often boys, χ2(1) = 13.13, p < .001, and dropouts had less general knowledge of SV (M = 5.80, SD = 2.44) than those who participated in the posttest and follow-up measurement (M = 6.89, SD = 2.66), t(501) = −3.50, p < .001 at T1.
Evaluation Level 1—Reaction
Program satisfaction
Participants in the SPP showed a mean satisfaction score of M = 4.43 (SD = 0.51), whereas the PP showed a mean score of M = 4.35 (SD = 0.59) indicating participant satisfaction for both program groups. No group differences on satisfaction were found.
Evaluation Level 2—Learning
Knowledge of sexual violence
Table 2 shows the fixed effects and relevant interaction effects for general knowledge, knowledge of professional help, victim blaming, anxiety, personal space perception, and personal space appraisal with time (T2 and T3) in reference to T1 and with group (SPP and PP) in reference to the control group. The results for general knowledge about SV showed a significant interaction effect for the SPP at T2 (p < .001) and for the PP at T2 (p < .001). This indicates immediate short-term effects for both program groups in comparison with the control group. These gains in knowledge were also apparent at T3 (SPP: p < .001; PP: p < .001). Results for general knowledge also show a main effect for gender at T1 (p < .001), indicating that at baseline, female participants had greater general knowledge of SV. There were no other main or interaction effects.
General and Professional Help Knowledge, Victim Blaming, Anxiety, and Personal Space.

Note. Adjusted coefficients estimated via restricted maximum likelihood estimation of mixed-effects linear regression model that included random effects for class and time and fixed effects for time, group, and gender. Group effects had the control group as reference. Gender effects had male as reference. SPP = scientist-practitioner program; PP = practitioner program.
p < .05; **p < .01; ***p < .001.
Knowledge of professional help
The results for knowledge of professional help revealed a significant interaction for both program groups with T2 (SPP: p < .001; PP: p < .001) and T3 (SPP: p < .01; PP: p < .01), indicating short-term and long-term effects for both program groups. No main effects or other interactions were found.
Victim blaming
The results for victim blaming showed that both program groups had a significant interaction effect with T2 (SPP: p < .05; PP: p < .01), but not with T3, indicating only short-term effects for both programs in reducing victim-blaming attitudes. A significant gender effect was found at T1 (p < .001), indicating that at baseline, female participants showed lower victim-blaming attitudes than males. No other main effects or other interactions were found.
Anxiety
No significant effects were found for both intervention groups at T2 and T3. These findings suggest no iatrogenic effects on anxiety of SV related to both programs. However, there was a significant main effect of time at T2 (p < .05) and T3 (p < .05), indicating that anxiety levels decreased over time in the program groups and the control group. There was also a significant gender effect at T1 (p < .001), indicating that at baseline, females had higher levels of anxiety surrounding SV. No other main effects or other interactions were found.
Personal space perception and appraisal
No effects for both intervention groups were found regarding personal space perception and appraisal at T2 and T3. There was a significant main effect of gender in personal space appraisal at T1 (p < .001), indicating that at baseline, female participants had higher levels of personal space appraisal. No interaction effects for group, time, and gender were found.
Evaluation of Level 3—Behavior
Victimization and perpetration
Table 3 shows the interaction and main effects for victimization and perpetration in dating and other situations with time (T2 and T3) in reference to T1 and with group (SPP and PP) in reference to the control group. We found a significant effect for the PP at T3 for victimization (p < .05), indicating a small reduction of victimization in dating situations over time. No other significant effects were found for victimization and perpetration. Gender effects for victimization in dating situations at T1 (p < .05) and victimization in other situations at T1 (p < .01) indicate that at baseline, female participants had higher victimization rates than did male participants. Gender effects for perpetrating SV in dating situations at T1 (p < .001) and in other situations at T1 (p < .001) indicate that at baseline, male participants had higher rates of perpetrating SV than did female participants. No interaction effects for group, time, and gender were found.
Victimization and Perpetration.
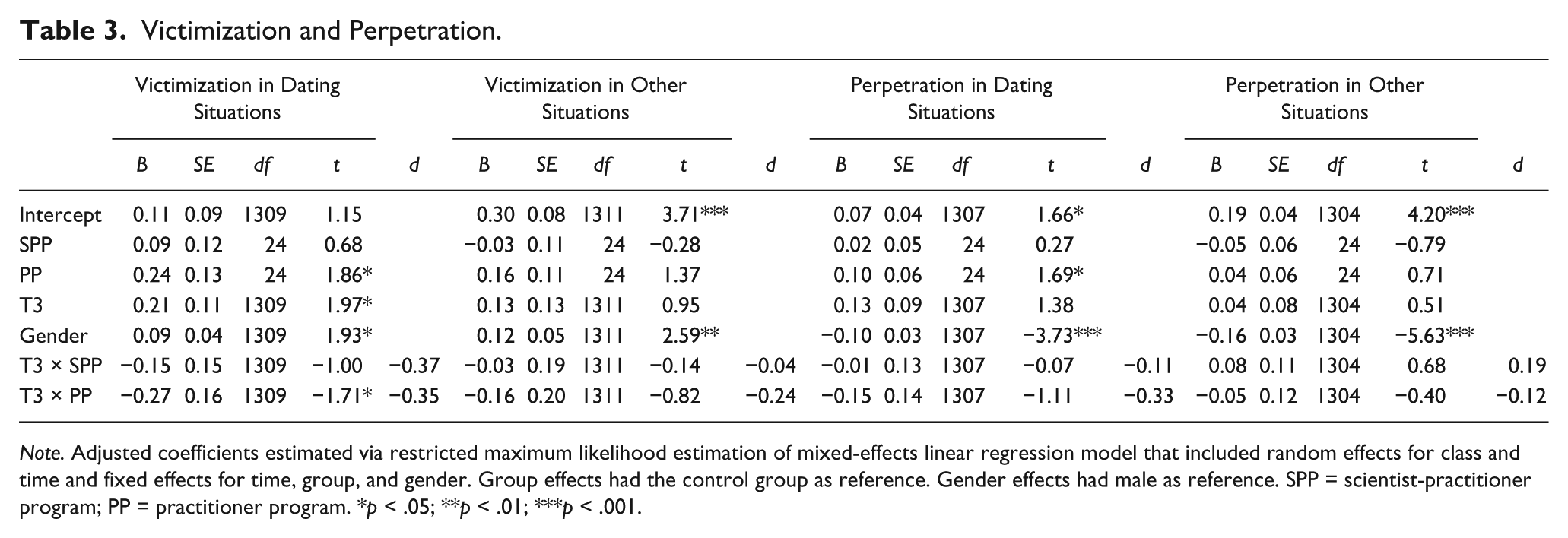
Note. Adjusted coefficients estimated via restricted maximum likelihood estimation of mixed-effects linear regression model that included random effects for class and time and fixed effects for time, group, and gender. Group effects had the control group as reference. Gender effects had male as reference. SPP = scientist-practitioner program; PP = practitioner program. *p < .05; **p < .01; ***p < .001.
Discussion
The present study evaluates the short-term and long-term effectiveness of a SPP and PP for the prevention of SV in adolescence at three levels (Kirkpatrick & Kirkpatrick, 2006). On the first evaluation level of reaction, results indicate that participants were satisfied with both programs, which is an essential precondition for further effects on other levels.
On the second evaluation level of learning, results show large short-term and long-term effects on general knowledge for both programs, supporting our first hypothesis. These results are in line with previous evaluation studies indicating effectiveness of SV programs on general knowledge acquisition (DeGue et al., 2014; Edwards & Hinsz, 2014; Ting, 2009). The large effects found here are higher than the medium effect sizes found by Ting (2009). However, it should be noted that changes in knowledge acquisition do not necessarily reflect changes on the behavioral level, which may ultimately be more important in the prevention of SV (Tharp et al., 2011). Effects for the acquisition of knowledge about professional help were large in the short term and medium in the long term for both programs, supporting our second hypothesis. Both programs showed short-term but not long-term effects on victim-blaming attitudes, which partially supported our third hypothesis. It is important to note that victim-blaming rates were already low at baseline, and therefore, there was little room for further reduction. No iatrogenic effects on anxiety were found in any group, supporting the fourth hypothesis. Apparently, the anxiety levels toward SV significantly declined in both intervention groups and the control group. A possible explanation could be that due to mere exposure of the paper-and-pencil questionnaire, anxiety levels diminished. No effects were found for the perception and appraisal of personal space in both programs, indicating that the fifth hypothesis cannot be supported. However, scores for personal space were already high at baseline, indicating a possible ceiling effect, which made further increases difficult.
On the third evaluation level of behavior, we found a marginal effect in the reduction of SV victimization in dating situations in the PP, but no effects on victimization in other situations in both programs, which only partially supported our sixth hypothesis. No program effects on SV perpetration in dating or other situations were found for both programs, and thus, these results did not support for the seventh hypothesis. However, the results on this level should be interpreted with caution. First, the reduction in dating victimization in the PP showed only a marginal significant effect and had a small effect size. Second, as indicated by the intercept coefficients and means, the rates of both victimization and perpetration were very low in general. Third, as with the other outcome variables, social desirability may have had an impact on students’ interpretations and statements of victimization and perpetration. Students filled out the questionnaire in the classroom, and some may have been intimidated because of the social circumstances under which the questionnaire was administrated. Future research on SV should take into account the difficulty of measuring highly personal and potentially incriminatory items, such as victimization and perpetration, in a classroom setting.
Main effects for gender were found in general knowledge of SV, knowledge of professional help, victim blaming, anxiety, personal space appraisal, victimization, and perpetration at T1. These results indicate that in general, female adolescents have more general knowledge of SV and knowledge of professional help for SV, higher rates of anxiety regarding SV, personal space appraisal, and SV victimization. In general, female students also showed lower rates of victim blaming and perpetration in comparison with male students. However, we did not find any interaction effects of group, time, and gender, indicating that both female and male adolescents similarly benefited from the prevention programs. Information on gender differences at baseline could be useful for adapting mixed- and single-gender aspects of prevention programs. For example, female adolescents had more general knowledge and more knowledge about professional help. In Germany, many specialized SV counseling centers offer help for children, female adolescents, and women. Male adolescents and men, on the contrary, have far fewer options for professional help, and thus, information on professional help for male victims could be implemented into the single-gender sessions. Also, female adolescents showed a higher rate of anxiety concerning SV, and male adolescents showed higher rates of victim-blaming attitudes. These factors could also be incorporated into the single-gender sessions, for example, by implementing more risk-reduction strategies in the single-gender session for female adolescents and more discussion on gender stereotypes and victim-blaming attitudes in the single-gender session for male adolescents.
With the exception of victimization in dating situations, we found no differences between the SPP and the PP. It is possible that the programs were not different enough. In fact, the first session of the SPP and the PP was identical. We hypothesized that the addition of a second session with more active participation and separation into single-gender audiences would yield higher effects on attitudinal and behavioral change, because students would have more time for self-reflection and to discuss the topic with their classmates. It could be that more than two sessions would be needed to achieve these results.
These results should be interpreted with caution. Both programs included psychoeducational and active participation elements, and it is possible that the active participation elements in the first session had the most impact on student learning. It could be that the elements of the second session did not yield any “new” information, and thus, there were no advances in knowledge or attitudinal changes in the SPP. Although DeGue and colleagues (2014) stated that brief and psychoeducational-only oriented prevention programs should be interpreted with caution, we found positive effects in the single-session PP. However, the PP did include active participation by the students, and this may be an important link to the effectiveness of a prevention program. Although the PP program’s effects on reducing victimization in dating situations were only marginally significant and showed a small effect size, this program may be a cost-effective way to promote SV prevention in everyday school practice.
Study Strengths and Limitations
The main strength of the study is the inclusion of a rigorous evaluation design with multiple evaluation levels regarding short-term and long-term effects. Another strength is the contrast of two prevention programs with different general conditions. The SPP was designed based on the results of prevention research, such that it included multiple sessions, mixed- and single-gender aspects, more active participation of the adolescents, while incorporating limitations of everyday school practice. The PP consisted of one session in a mixed-gender audience with active student participation, which was identical to the first session of the SPP. Although research on SV prevention has shown that student participation, number of sessions, and gender of the audience all affect outcomes (see Weisz & Black, 2009, for an overview), few studies have contrasted two prevention programs with differences in these conditions. Our results did not show advantages of the two-session SPP in contrast to the single-session PP. Another strength was our sample, which included both female and male adolescents to address gender sensitivity in the study. A further strength was the direct practical implication for school-based prevention. Both prevention programs can be directly implemented into everyday school practice, although the PP may be more cost effective. Also, all students had the opportunity to disclose possible victimization experiences with a female or male co-worker from the counseling center and thus resulting into a low threshold for seeking professional help services.
The present study had also several limitations. First, although we used a cluster-randomized controlled design, we selected five urban secondary schools (German Gymnasiums) for the intervention, which is not representative of the general public because, on average, students achieve a higher educational degree in these schools. Thus, the large effects on general knowledge acquisition may also be due to the students’ generally high capacity for learning. Also, a more diverse sample with multiple ethnic backgrounds could have yielded more heterogeneous views on gender-based stereotypes, date rape, and victim-blaming attitudes, which could have explained more variance in the effectiveness of the prevention programs (Geiger, Fischer, & Eshet, 2004). Second, the study showed an attrition rate of 33.48% from T1 to T3, which is comparable with other prevention studies using subject-generated identification codes (Daigneault et al., 2015). However, dropouts were significantly more often boys and had less knowledge of SV compared with other participants, which may be a high-risk group for SV perpetration. Third, we created new measures especially for a gender-sensitive approach without explicably framing a victim as female and a perpetrator as male. These new measures resulted in fair to good reliability, but they are not validated. Also, the study relied on a self-report questionnaire, which could have several limitations such as recall problems, under-reporting or exaggeration of behavioral outcomes, or social desirability. Another problem might have been that students were not able to assess certain variables correctly. For example, the items on knowledge of professional help only measured subjective knowledge about where to find professional help on the Internet and via local services. Also, it is not clear what exactly the students considered professional help when they completed the questionnaire at T1. In Germany, numerous counseling centers offer various assistance services, but these should not be automatically labeled as professional help for victims of SV. Both the PP and SPP gave much information about specialized counseling centers for victims of SV, which are considered professional helping services in Germany. However, the items we used for knowledge of professional help were not able to differentiate students’ knowledge of these services, so these results should be interpreted with caution. Future studies could use an open item format in which participants should note which helping services they are familiar with, which would give a more accurate estimate on knowledge of professional help.
Practical Implications and Future Developments
The present study showed promising results regarding the prevention of SV. Both the SPP and the PP showed large effects on the acquisition of general knowledge. More importantly, the PP showed small effects on the reduction of SV victimization in dating situations after a 6-month follow-up. These findings are noteworthy because, to date, only prevention programs that involve several sessions have shown reductions in SV victimization in adolescents (Foshee et al., 2005; Taylor et al., 2013). The single-session PP may be a cost-effective way to prevent SV. The PP could also be used as a “treatment as usual” program for future comparisons with other programs. Also, future research should further investigate the relationship between certain general program conditions and SV prevention to yield additional effects that may also impact SV victimization and perpetration.
Footnotes
Acknowledgements
The authors would like to thank the counseling center Zartbitter Muenster for the cooperation in this project and Dr. Celeste Brennecka for proofreading the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the German organization “Franz Bröcker Stiftung.”