
Abstract
Research has consistently demonstrated that people diagnosed with serious mental illness (SMI) are at increased risk for violent ideation and behavior (VIB) and that this is especially the case for SMI patients with comorbid substance use disorders (SUD). Despite this, what is still largely unknown is the relative prevalence of VIB across diagnostic categories, whether the rates of VIB in SMI groups exceed the rates observed in people with SUD only, and which demographic factors increase the likelihood of VIB under different circumstances for people with SMI. To address these questions, we analyzed the intake records of 63,572 patients diagnosed with SMIs (i.e., schizoaffective disorder, schizophrenia, bipolar disorder, and unipolar depression), substance use disorders, and non-SMI psychiatric disorders. Raw prevalence rates for a combined metric of VIB were established and compared for each group, and a series of logistic regression analyses were performed to estimate how various demographic factors influenced the likelihood of VIB endorsement in each study group. Our results revealed that (a) patients with SMI conditions had higher rates of VIB than both patients with non-SMI psychopathology and those with substance use disorders only; (b) patients with SMI and comorbid substance use pathology were responsible for the majority of VIB within each SMI condition; and (c) men with SMI conditions had higher prevalence rates of VIB than females. In addition, we found that for every SMI diagnosis, comorbid substance use disorders and younger age were related to greater risk for VIB, and where race and gender were found to significantly alter the likelihood of VIB endorsement, African American status and female gender were independently related to greater risk. The implications of these findings and directions for future research are discussed.
Keywords
Introduction
People diagnosed with serious mental illness (SMI) are at increased risk for committing various acts of violence, with odds ratios (ORs) ranging from 1.65 to 29, depending on the study (Corrigan & Watson, 2005; Douglas, Guy, & Hart, 2009; Fazel, Gulati, Linsell, Geddes, & Grann, 2009; Fazel, Långström, Hjern, Grann, & Lichtenstein, 2009; Monahan et al., 2001; Swanson, Holzer, Ganju, & Jono, 1990, for review, see Silverstein, Del Pozzo, Roché, Boyle, & Miskimen, 2015). While the risk of violent behavior is elevated in patients with SMI, the vast majority of people with these disorders will never commit an act of serious violence. Yet, the stigma associated with SMI, partially due to violence risk, is universal. Therefore, understanding which patients are at increased risk for violent behavior is essential for the development and testing of various interventions aimed at reducing violent behavior, hospitalization, and incarceration of people with SMI (e.g., STAIR, see Yates, Kunz, Khan, Volavka, & Rabinowitz, 2010), and for efforts aimed at ensuring rational public safety policies and stigma reduction efforts.
A number of risk factors for violent behavior have been identified for people with SMI. These include younger age (Hodgins & Riaz, 2011; Large & Nielssen, 2011; Monahan et al., 2001; Swanson et al., 1990), female gender (Brennan, Mednick, & Hodgins, 2000; Fazel, Gulati, et al., 2009), and substance abuse (Boles & Miotto, 2003; Hoaken & Stewart, 2003; Johnson & Belfer, 1995). Concerning substance abuse, as in the general population, those with SMI who abuse drugs or alcohol are at greater risk for violent behavior than those who do not (Fazel, Gulati, et al., 2009; Fazel, Långström, et al., 2009; Steadman et al., 1998; Swanson et al., 2006; Swartz et al., 1998; Van Dorn, Volavka, & Johnson, 2012; Witt, van Dorn, & Fazel, 2013). Where the literature is less clear is whether SMI patients have increased rates of, or odds of engaging in, violent behavior compared with people diagnosed with substance abuse disorders only. For example, Swanson et al. (1990) and Corrigan and Watson (2005) found that rates of violent behavior were higher in people diagnosed with substance use pathology only, compared with any SMI group, whereas Van Dorn and colleagues (2012) found no such difference. Furthermore, although some studies have shown that patients with psychotic conditions are at greater risk for violent behavior than those with SUD only, Fazel and colleagues’ (2009) meta-analysis indicated equivalent risk across these two groups. For those looking to accurately and efficiently assess violence risk, understanding whether differential risk is associated with SMI conditions as compared with substance use disorders only is imperative.
Another area where the research literature is lacking concerns the differential prevalence of and risk for violent behavior associated with individual SMI diagnoses (e.g., schizophrenia [SZ], bipolar disorder [BD]). Regarding prevalence, while Swanson et al.’s analysis (1990) demonstrated roughly equivalent prevalence rates for violent behavior over the past year across SMI groups, Corrigan and Watson (2005) found the rates to be far more varied. In addition, despite much attention being paid to the influence of SZ on violence risk, a recent meta-analysis (Volavka, 2013) indicated that the risk for violence associated with BD was greater than the risk associated with SZ. Moreover, in patients experiencing a first-episode of psychosis, those who exhibit symptoms of mania are at greatest risk for aggressive behavior (Dean, Walsh, Morgan, & Demjaha, 2007). Given the emerging evidence suggesting that mood disorder symptoms may be a significant risk factor for violence in both the presence and absence of psychosis, and that researchers often collapse patients with psychosis who have varying levels of mood disturbance into one composite group (e.g., SZ and schizoaffective disorder [SZA]), research exploring both the prevalence of and differential risk for violent behavior and related constructs in individual SMI conditions is sorely needed.
Finally, despite violent ideation being a logical and empirically demonstrated antecedent of violent behavior (e.g., Sturup, Monahan, & Kristiansson, 2013), a prominent aspect of the most influential models of aggression (e.g., General Aggression Model, see Anderson & Bushman, 2002), and a ready target for intervention in evidence-based models of psychotherapy, little is known about the prevalence of violent ideation in patients with SMI. In a rare exploration of this topic, Grisso, Davis, Vesselinov, Appelbaum, and Monahan (2000) found that (a) approximately 30% of hospitalized patients with mental illness (SMI and non-SMI) had recent violent ideation and this rate was double that of community controls, and (b) a subgroup of patients who endorsed violent ideation during hospitalization continued to endorse violent ideation after discharge, and this group was roughly twice as likely to engage in violent behavior than people who only endorsed violent ideation during hospitalization. These results suggest that violent ideation is elevated in people with mental illness, and that persistent violent ideation is a risk factor for violent behavior. While Grisso and colleagues’ work was an important first step toward understanding the rates and predictive value of violent ideation in SMI conditions, little follow-up research on the topic has been conducted.
With the above in mind, our goals were (a) to determine the prevalence rates for violent ideation and behavior (VIB; operationally defined below) in patients across a range of SMI conditions; (b) to estimate the degree to which the odds of VIB endorsement were influenced by various SMI diagnoses relative to groups of people with non-SMI psychiatric diagnoses, and people with substance use disorders alone; and (c) to estimate how various demographic factors influenced the likelihood of VIB endorsement in SMI patients. We hypothesized the following:
We did not have any specific hypotheses related to race as a predictor. To test these hypotheses, we examined the intake histories of all patients diagnosed with SZ, SZA, BD, unipolar depression (MDD), substance use disorders, and other psychiatric patients (who formed a PC group; described below) who were treated at one of our university affiliated hospitals between July 1, 1998, and January 21, 2015.
Method
Participants
The intake records of 63,572 patients were included in this study. These patients were split between six diagnostic groups: (a) SZA (n = 2,788), (b) SZ (n = 2,710), (c) BD (n = 4,551), (d) MDD (n = 17,446), (e) PCs (n = 16,115), and (f) individuals with substance use disorders without psychiatric comorbidity (SUD; n = 19,962). The PC group was comprised of people diagnosed with a variety of non-SMI psychiatric conditions including anxiety and eating disorders. The SUD group included individuals diagnosed with alcohol dependence or abuse, or any form of drug dependence or abuse. All patients were 18 years of age or older. Patient diagnoses were those generated by, and entered into, the electronic medical record (EMR) database by the treating psychiatrist based on their intake interview clinical impressions. Groups were mutually exclusive, and in cases where the patient’s diagnosis changed over time, the diagnosis entered during their last visit was used. This decision was based on the idea that increased patient contact (i.e., more visits and, thus, greater appreciation of symptom history) would allow for more accurate diagnosis. All aspects of this study were reviewed and approved by the Rutgers University’s Institutional Review Board.
Variables Extracted From the EMR
The data in the EMR were obtained during the standardized, comprehensive psychiatric/psychosocial intake interview used at all Rutgers University Behavioral Health Care (UBHC) clinics. These interviews were conducted when patients were admitted for treatment and when they changed levels of care. Components of the interview were completed independently by a psychiatrist and a psychologist or master’s level clinician.
VIB
Within the psychosocial interview, there is a section related to VIB. The interviewing clinician inquires about incidents of violent ideation and then inquires about past violent behavior. The clinician is not given specific prompts or a question sequence to guide the collection of this information. If the patient endorses experiencing or engaging in either, the clinician indicates the patient is VIB positive. Therefore, the VIB variable in this study was dichotomous: VIB negative (0) or VIB positive (1). While non-optimal, given the manner in which these data are entered into the EMR system (i.e., using a single radio button to capture information about both constructs), it was not possible for us to separate violent ideation from violent behavior. In collecting these data, we considered the patient’s entire intake history over the 13 years of data available to us. For example, if a patient had five intakes, we would consider them VIB positive if they endorsed VIB in any one of their five intake interviews. We decided to consider a patient VIB positive if their intake history contained any VIB endorsement to achieve the cleanest separation between groups. Given this, our VIB variable is best considered a quasi-lifetime metric. Importantly, each patient only contributed one data point to the study, that is, they were identified as VIB negative or VIB positive.
Demographic variables
As part of the intake interview, patients were asked to indicate their date of birth, gender, and race. Gender was coded as either male or female and race was coded as Caucasian (non-Hispanic), African American (AA; non-Hispanic), Hispanic/Latino (White, Black, and Other), and Other. The Other group is composed of Asian, Native American, Native Hawaiian/Pacific Islander, Multiracial, Declined to Indicate, and any race not included in the other choices.
UBHC hospital system
UBHC’s system consists of multiple clinics throughout the state of New Jersey. It includes inpatient, acute and extended partial hospital, and outpatient treatment programs. All levels of treatment were sampled. Although our clinics are situated within various communities that vary in terms of socioeconomic status (SES), all patients treated within UBHC were either on Medicaid or uninsured and without means to pay for treatment. Individual-level data on SES were not available.
Statistical Analyses
Raw Percentages
We calculated three sets of percentage scores. First, we calculated the percentage of patients within each diagnostic group who endorsed VIB. Second, we calculated the percentage of patients within each diagnostic group that also had comorbid substance use disorders. Finally, we calculated the percentage of VIB endorsements within each diagnosis that were made by people who had comorbid substance use disorders. Importantly, these percentages were not mutually exclusive. These analyses allowed us to determine the prevalence of VIB in each diagnostic group, the frequency of co-occurring substance use pathology, and the proportion of VIB within each diagnostic group that occurred in individuals with comorbid substance use disorders. For each class of percentages, averages and ranges were calculated, and when necessary for interpretation, chi-square tests of independence were conducted.
Logistic Regressions
The nature of each logistic regression was as follows:
The reference groups for gender and race were female and other, respectively, and for age, we used the patient’s age at their last assessment. Importantly, for each variable in each analysis, the statistical test and related ORs represent the effect of and change in odds associated with that predictor when all other variables in the analyses were controlled for. Given the large number of statistical tests conducted, we used the False Discovery Rate (FDR) correction to adjust our p values (Benjamini & Hochberg, 1995). 1 We considered any statistical test with a FDR corrected p value of less than .05 to be significant and, thus, interpretable. Given the size of our samples and thus high power of our statistical tests, in this article, we focus the interpretation of our results on the ORs, as opposed to statistical significance.
Results
Demographic data are presented in Table 1. The BD, MDD, and PC groups were composed of more women than men while the SZA, SZ, and SUD groups were composed of more men than women. The average age in the study was 39.4 years old (SD = 14.11) and the SZA and SZ groups had the highest average age. The average number of intake interviews in the study was 3.05 (SD = 4.28), and patients in the SZA, SZ, and BD disorder groups had more program admissions per patient than those in the MDD, PC, and SUD groups.
Demographic Characteristics for All Participant Groups.

Note. Table cells represent either the percentage of participants that fall into a given category or the mean and standard deviation for each study group.
Raw Percentages
VIB
As can be seen in Table 2, each of the SMI groups had rates of VIB that exceeded the rate of the PC group, and all SMI groups, except for the MDD group, had rates of VIB that exceeded the rate of the SUD group. However, the difference between the substance abuse and SZ group was small and associated with a trivial phi coefficient (Φ = .02).
Rates, by Diagnosis of (a) VIB, (b) SA, and (c) Both VIB and SA.
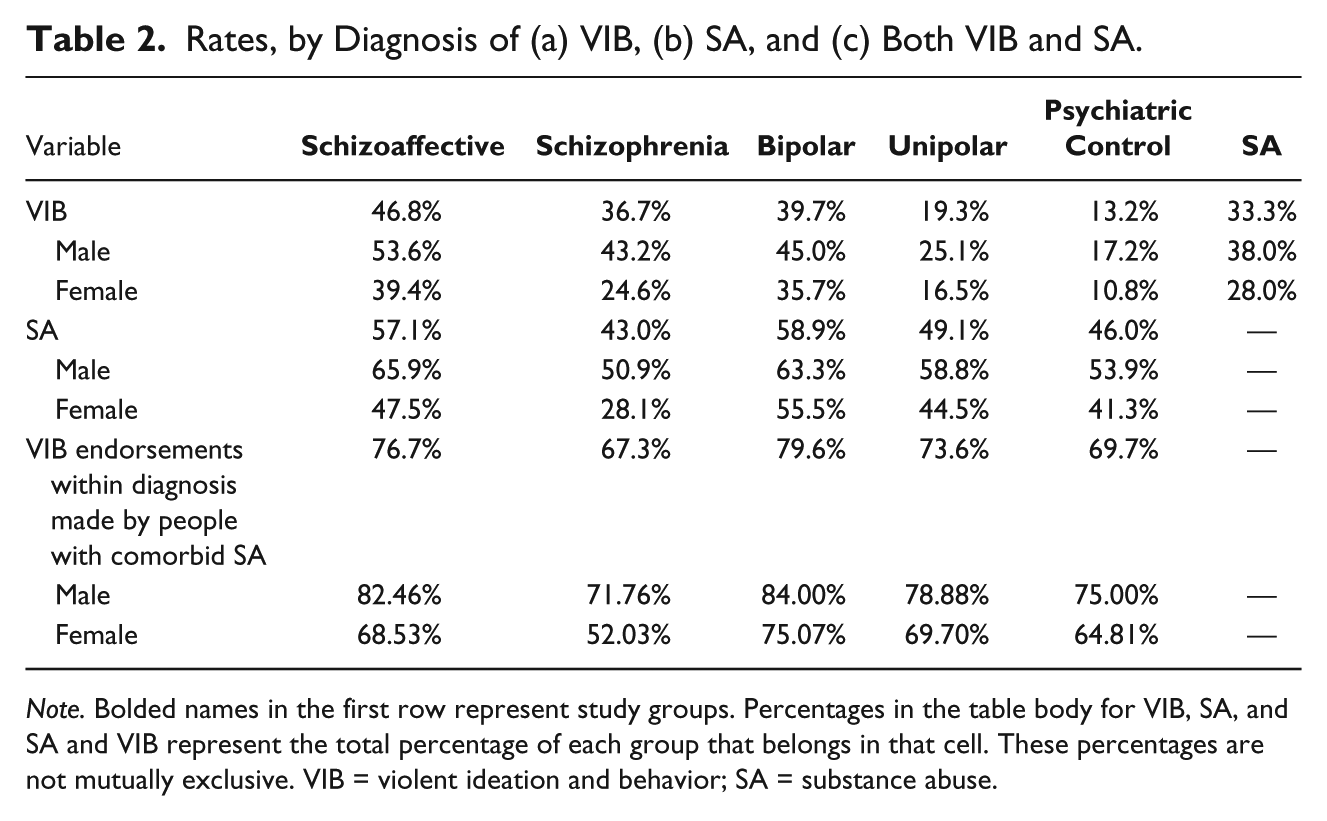
Note. Bolded names in the first row represent study groups. Percentages in the table body for VIB, SA, and SA and VIB represent the total percentage of each group that belongs in that cell. These percentages are not mutually exclusive. VIB = violent ideation and behavior; SA = substance abuse.
The average prevalence rate of VIB across all groups was 31.5%. Males (average = 37.02%) had higher average rates of VIB than females (average = 25.83%). The differences, in terms of raw percentages between genders, ranged from a low of 6.4% in the PC group to a high of 18.6% in the SZ group, with an average difference of 11.23%.
VIB prevalence rates showed marked variation between groups. For example, in terms of overall VIB prevalence, the SZA and BD groups had prevalence rates that exceeded the SZ group by 10.10% and 3%, respectively, while the MDD group had markedly lower prevalence rates than all of the other SMI groups (range of differences: 17.4%-27.5%; see Table 2). The magnitude of the differences between men and women varied across disorders and no distinct pattern emerged (e.g., men did not evidence greater prevalence rate differences consistently across disorders). For example, in the comparison of SZ with BD, women evidenced a greater between-group difference than men (11.10% vs. 1.8%), while in the comparison of SZA with BD, men evidenced a greater between-group difference than women (8.60% vs. 3.7%).
Comorbid substance use
Approximately, 49% of patients had comorbid substance use disorders and there was quite a bit of variation across groups (Table 2). In all SMI groups, males (average = 57.35%) had higher rates of substance use disorders than females (average = 43.91%) with an average gender difference of 15.22%. The largest gender difference in substance use disorders was in the SZ group (22.8%) and the smallest was in the BD group (7.8%). Patients diagnosed with SZ had the lowest rates of substance use disorders, while patients with BD had the highest overall rates.
Proportion of VIB that occurred in people with comorbid substance abuse pathology
As shown in Table 2, the majority of VIB in each study group (average 73.38%) occurred in patients with comorbid substance use pathology. In each group, substance use disorders accounted for less VIB in females than they did in males (raw percentage difference range: 8.9%-19.7%). Of particular note, VIB in females with SZ occurred with roughly equal frequency in those with and without comorbid substance use conditions.
Logistic Regressions
The ORs for each variable for each diagnostic group from each logistic regression are presented in Tables 3, 4, and 5.
Odds Ratios for the Impact of Demographic Factors on VIB Within Each SMI Diagnosis (Logistic Regression 1).
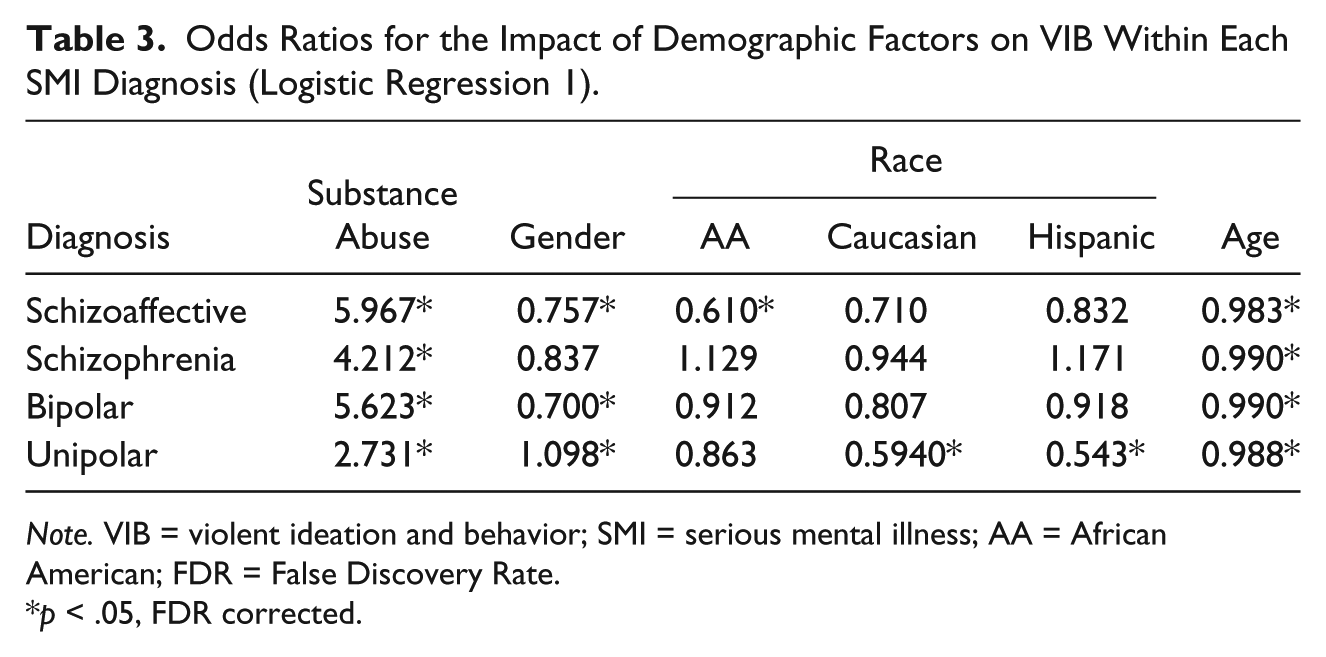
Note. VIB = violent ideation and behavior; SMI = serious mental illness; AA = African American; FDR = False Discovery Rate.
p < .05, FDR corrected.
Odds Ratios for the Impact of Diagnoses and Demographic Factors on VIB, Relative to Psychiatric Controls for Each SMI Condition (Logistic Regression 2).

Note. VIB = violent ideation and behavior; SMI = serious mental illness; AA = African American; FDR = False Discovery Rate.
p < .05, FDR corrected.
Odds Ratios for the Impact of Diagnoses and Demographic Factors on VIB, Relative to Patients With Substance Use Disorders Without Psychiatric Comorbidity for Each SMI Condition (Logistic Regression 3).

Note. VIB = violent ideation and behavior; SMI = serious mental illness; AA = African American; FDR = False Discovery Rate.
p < .05, FDR corrected.
SMI diagnoses
Within each diagnostic category, patients with comorbid substance abuse conditions were more likely to endorse VIB than patients who did not (OR = 2.73-5.97). As compared with the PC and SUD groups, with only one exception, individuals with any form of SMI were found to have increased odds of VIB endorsement (OR = 1.88-5.54 and OR = 1.45-1.97, respectively). The exception was for patients in the SZ group, who had reduced odds of VIB endorsement as compared with people in the SUD group (OR = 0.697). In all analyses comparing people with SMI to both the PC and SUD groups, when controlling for gender, race, and age, patients with SZ had the smallest increase in the odds of VIB endorsement (lowest OR).
Age
Consistent with previous research focused on violent behavior only, within each of the SMI groups, in every analysis, age was a significant negative predictor of VIB (ORs = 0.981 and 0.990), indicating the odds of endorsing VIB reduces with age.
Gender
In eight of 12 analyses, participant gender was a significant predictor of VIB. In six of these analyses, male gender was related to reduced odds of VIB endorsement (ORs = 0.70-0.88), and in two of these analyses, male gender was related to increased odds of VIB endorsement (ORs = 1.10-1.11). The six statistical tests that found male gender to be a significant negative predictor of VIB were spread across SZA, SZ, and BD diagnoses. The two analyses where male gender was related to increased odds of VIB were those associated with the logistic regressions within the MDD group alone and when this group was compared with controls.
Race
AA race was related to significantly increased odds of VIB endorsement in eight of 12 analyses (ORs = 1.22-2.10) and related to significantly reduced odds of VIB endorsement in one of 12 analyses; being Caucasian was never related to significantly increased odds of VIB endorsement, but was related to statistically significant reductions in the odds of VIB endorsement in three of 12 analyses (ORs = 0.59-0.82); Hispanic ethnicity was never related to significantly increased odds of VIB endorsement, but was related to statistically significant reductions in the odds of VIB endorsement in five of 12 analyses (ORs = 0.54-0.83).
Discussion
The purpose of this study was to estimate the prevalence and odds of, and demographic factors related to, VIB in various SMI conditions. To do so we employed one of the largest datasets (over 63,000 patients) ever used in a single study of violent behavior and ideation in SMI and posited four specific hypotheses. In turn, we review our hypotheses and the results from our analyses related to them. We then note study limitations and conclude by discussing the value of these findings and directions for future research.
Odds of Endorsing VIB: SMI Groups as Compared With PC and SUD
Our results largely supported the hypothesis that the odds of endorsing VIB would be greater in all SMI conditions than in PC and SUD groups. As compared with both the PC and SUD groups, in all cases except for one, the odds of endorsing VIB were significantly elevated for SMI conditions across analyses. The only exception was that SZ patients were less likely to endorse VIB than SUD patients. This latter result was somewhat surprising given the large body of literature related to increased risk of violent behavior in patients with SZ and other psychotic conditions. Yet, as noted in the introduction, the literature comparing patients with psychotic conditions with those with substance use disorders in terms of violence risk is equivocal. So, this result was not without precedent. It is important to note, however, that a number of published reports and our results indicate that among patients with SZ, those who have comorbid substance use disorders are more likely to commit acts of violence than those who do not.
Comorbid Substance Use and VIB
In line with our hypothesis, we found comorbid substance use disorders to be the non-SMI factor that most influenced the odds of VIB endorsement. Our prevalence rate data also suggest substance abuse as a risk factor for VIB in that 67.3% to 79.6% of VIB endorsements within each diagnostic group were from patients with comorbid substance use pathology. These results add to the large body of literature demonstrating that comorbid substance use disorders in people with SMI increase the likelihood that they will engage in violent behavior (e.g., Fazel, Gulati, et al., 2009) or ideation (e.g., Grisso et al., 2000).
SMI Conditions Characterized by Altered Mood and Odds of VIB Endorsement
We found support for the hypothesis that SMI conditions characterized by alterations in mood would have higher prevalence rates and increased odds of VIB endorsement. Across various derivations of VIB prevalence, SZA and BD patients had higher VIB endorsement rates than did patients with SZ. In terms of the odds of endorsement of VIB, SZA and BD patients had the largest increase in odds of endorsing VIB when these conditions were compared with both PC and SUD. Given the nature of our data, for the SZA and BD groups, it is not possible for us to determine whether VIB endorsements occurred during depressed or manic states, and previous research (Dean et al., 2007; Fazel et al., 2015; Volavka, 2013) suggests either mood state may potentiate risk.
Gender, Age, and VIB
Confirming our hypothesis, across all SMI diagnoses, in every logistic regression analysis, younger age was related to increased odds of endorsement of VIB. On the face of it, this finding is largely unremarkable given the large body of literature demonstrating younger age to be a risk factor for engaging in violence. When considered more closely though, the finding becomes rather curious. Pointedly, our VIB metric considered patients’ entire intake histories and, as a result, older patients potentially had longer intake histories and, therefore, more opportunity to endorse VIB. That they did not have higher VIB rates than younger patients could result from a number of factors. The first factor concerns the typical time course for violent behavior. As noted above, younger age is associated with greater risk of violent behavior and an emerging literature suggests that aggression and violent behavior, or risk thereof, are major precipitants of first hospitalizations for people with SMI (Dean et al., 2007; see Silverstein et al., 2015, for review). Therefore, information about violent behavior immediately preceding and perhaps precipitating a patient’s entry into our system may be more readily available or known to the clinician doing an intake (i.e., police dropoff or emergency screening records are available) and, as a result, recorded in the intake record. The second factor concerns when a patient entered our system of care. Generally speaking, as patients become more familiar with psychiatric treatment, they realize that endorsing violent thoughts or behaviors results in a response from their treatment team. Therefore, it is plausible that younger patients entering our system were more likely than older patients entering our system after being treated elsewhere to endorse violent ideation or behavior. The third factor concerns which patients are retained within the treatment system. Most treatment settings have strict rules against violent or aggressive behavior and speech, and take endorsements of violent ideation very seriously. As a result, those patients who engage in violent behavior, are verbally aggressive, or have violent thoughts about staff or other patients are often discharged from treatment, and treatment systems are reluctant to allow them to return. If this factor was in play, it could exert a downward influence on the age associated with VIB endorsement (i.e., younger patients were discharged and those who remained a risk for violence or aggression were not allowed to return for treatment later). The final factor concerns the type of patients treated in our system. Specifically, during the time period from which the data were accessed, UBHC primarily treated patients on Medicaid or uninsured patients, and as a result, the younger patients UBHC treated may have had more psychosocial stressors and a more serious course of illness. This more serious course of illness may be related to a number of factors associated with the incidence of violent behavior including more severe and treatment resistant symptoms (for review, see Volavka, 2013), lower insight (Buckley et al., 2004; Ekinci & Ekinci, 2013), and lower medication adherence (Alia-Klein, O’Rourke, Goldstein, & Malaspina, 2007). Alone or in concert, the above noted factors may help to explain why, despite employing a quasi-lifetime metric of VIB and using age at last intake in our regression analyses, we found younger age to be associated with increased odds of VIB endorsement.
We found partial support for our hypothesis that female gender would increase the odds of VIB endorsement. Specifically, gender was associated with significantly altered odds of VIB endorsement in eight of 12 analyses, and for 75% of these significant results, male gender was related to reduced odds of VIB endorsement. These results suggest, as has been shown in previous research focused on violent behavior (e.g., Fazel, Gulati, et al., 2009), that in the presence of a SMI, being female increases the likelihood of VIB endorsement. Importantly, while it is true in the general population and among individuals with SMI that the prevalence of VIB is higher in males than females (e.g., see Table 2), what our study shows and what previous research (Brennan et al., 2000; Fazel, Gulati, et al., 2009) has shown is that the change in likelihood of VIB when SMI is present is greater in female patients than in males. Put simply, men with or without SMI are more likely to engage in VIB than women (i.e., they have higher rates of VIB), but the change in the likelihood (i.e., odds) of engaging in VIB is influenced more by the presence of SMI in women than it is in men.
Race and VIB
Although we did not posit any hypotheses about patient race, we did include race as a predictor in our logistic regressions and found patient self-reported race to influence the odds of VIB endorsement. Specifically, AA race was associated with significant increases in the odds of VIB endorsement and Hispanic and Caucasian races were associated with significant reductions in VIB endorsement.
We believe our finding that AA patients have higher ORs for VIB endorsement deserves discussion. In particular, many of the AA patients in our study were treated in clinics in an economically disadvantaged urban neighborhood that is characterized by one of the highest crime rates in the United States (Newark, NJ; U.S. Department of Justice, 2014; for a discussion of violent victimization in Newark, see also Boyle, Lanterman, Pascarella, & Cheng, 2010). Researchers have found that AA residents of the greater Newark area are significantly more likely to suffer assault-related injuries than residents of other racial and ethnic groups (Boyle & Hassett-Walker, 2008). Furthermore, violent victimization has been found to be a risk factor for later engaging in violence in both non-SMI and SMI samples (Desmarais et al., 2014; Esbensen & Huizinga, 1991; Reed et al., 2014; Swanson et al., 2002; Swartz et al., 1998), and thus, AA patients may have been more likely to report VIB as a result of prior victimization. Moreover, socio-environmental, social learning (Kaufman, 2005; Vogel & Keith, 2015), and individual-level factors characteristic of this geographic area such as concentrated poverty and high percentages of vacant housing units (Boyle & Hassett-Walker, 2008), social disorganization (Shaw & McKay, 1942), low SES (Monahan et al., 2001; Silver, 2000), and unemployment (Monahan et al., 2001) have been repeatedly demonstrated to increase rates of violence. Concerning SES, given that nearly all subjects were on Medicaid or uninsured, this variable is at least partially controlled for in our analyses. Owing to the limitations inherent to the dataset, we were unable to determine whether the AA participants generally and especially those from Newark were concentrated in communities within the treatment center catchment areas that were particularly disadvantaged. The reader should keep these above factors in mind when considering our results.
Study Limitations
A few study limitations should be kept in mind when interpreting our results. First, given the way information was recorded in our EMR, it was impossible for us to disentangle violent ideation from violent behavior, and further, we were unable to determine the severity of each patient’s VIB. Therefore, it is imperative that the reader keep in mind the broad nature of our VIB construct (i.e., not conflate VIB with violent behavior) and our inability to determine the relative proportions of violent behavior versus ideation contained therein when considering our results. Future research should seek to both disentangle and better define the interrelationship between these two variables. Second, patient diagnoses were established based on the clinical impressions of the treating psychiatrist and not using a structured clinical interview (e.g., Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV; American Psychiatric Association, 1994] Diagnoses, SCID). However, while it is true that the use of clinical records may have increased the variability in our dataset, their use affords us a high level of ecological validity in that these data accurately reflect what clinicians are observing and responding to in real-world treatment settings. Third, beyond substance abuse, comorbid psychiatric diagnoses were not considered in our analyses and previous research has demonstrated that the complexity of patient’s psychopathology (Corrigan & Watson, 2005) as well as specific mood, anxiety (e.g., posttraumatic stress disorder [PTSD]; Sautter et al., 1999), and personality disorder (e.g., antisocial personality disorder; Hodgins, Tiihonen, & Ross, 2005) conditions increased the risk of violent behavior. Fourth, the temporal relationship between the onset of a substance use disorder and VIB is unknown. That is, even for patients with multiple intake interviews, we could not discern whether the onset of their substance abuse disorders antedated their endorsement of VIB or vice versa. Fifth, given that our sample consisted primarily of patients on Medicaid, the generalizability of our findings may be limited to those patients who experience significant disability attributable to their psychiatric condition. Finally, though not a limitation per se, the reader should keep in mind that our reported alterations in odds for VIB endorsement are best conceptualized as postdictive rather than predictive estimates, as a patient’s endorsement of either past or current VIB was regressed on our dependent variables. Despite their postdictive nature, as described above, there is a close alignment between the risk factors we identified and those identified by researchers attempting to predict future violence (e.g., substance use pathology; Fazel, Långström, et al., 2009).
Conclusion
In line with previous research on violent behavior, we have demonstrated that people with SMI have increased odds of endorsing VIB when compared with non-SMI patients and, in most cases, individuals with substance abuse pathology alone. In this way, our findings add to the growing body of literature that suggests SMI conditions are a significant risk factor for VIB. In addition, in line with the results of some previous research focused on violent behavior only, we found marked heterogeneity in rates and ORs for VIB endorsement across SMI conditions. This was particularly the case for SZ (lower) as compared with BD and SZA (higher) patients. For researchers, our findings highlight the need for those engaged in the study of violence-related constructs to reflect on the wisdom of creating composite groups composed of multiple SMI diagnoses. For clinicians, our findings demonstrate the value of data collected during standard intake interviews under the typical restrictions associated with psychiatric clinics (e.g., limited time, etc.) and suggest that these data might be gainfully used in decision making regarding enrollment in groups or treatment programs designed to address violent ideation or behavior. Future researchers should endeavor to delineate the causes of the relationship between violent ideation and behavior in various SMI conditions, and the circumstances under which this relationship is modified by static and dynamic individual, environmental, and treatment factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Roché was supported by Grant support 1K12GM093854-05.