
Abstract
Posttraumatic stress disorder (PTSD) symptoms have been repeatedly linked to intimate partner aggression (IPA), and previous research has suggested that this association may be stronger among veterans and men. However, few studies have examined veteran status and gender as moderators of the association between PTSD and psychological IPA, taking both partners’ perspectives into account (i.e., within a dyadic framework). The current study aimed to address this limitation by using dyadic multilevel modeling to examine the association between PTSD symptoms and psychological IPA perpetration among a sample of 159 Operation Iraqi Freedom and Operation Enduring Freedom veterans and their partners (N = 318 participants). Findings revealed that both one’s own and one’s partner’s PTSD symptoms were positively associated with greater psychological IPA. In addition, the effects of partner PTSD symptoms on psychological IPA perpetration differed across gender and veteran status. Results suggested that the association of partner PTSD and IPA perpetration may be stronger for male veterans than for female veterans. Findings from the current study are consistent with previous research showing associations between PTSD and IPA, and have clinical implications for treatment of PTSD and IPA among Operation Iraqi Freedom and Operation Enduring Freedom veterans.
Posttraumatic stress disorder (PTSD) symptoms can have a damaging effect on Operation Iraqi Freedom/Operation Enduring Freedom (OIF/OEF) veterans’ intimate relationships (Teten et al., 2010) by increasing risk for physical and psychological intimate partner aggression (IPA; Taft, Watkins, Stafford, Street, & Monson, 2011). PTSD symptoms are theorized to increase risk for IPA perpetration through their influence on cognitive (e.g., perception of threat, arousal, and behavioral domains; Chemtob, Novaco, Hamada, Gross, & Smith, 1997). Although a majority of past research on PTSD and IPA has focused on physical IPA, psychological IPA, which includes acts intended to cause emotional harm or threat of harm to one’s partner (e.g., insulting, degrading, or calling one’s partner names; Cyr, McDuff, & Wright, 2006), is associated with both mental and physical health problems among its victims (Coker et al., 2002; Watkins et al., 2014). In addition, individuals who experience IPA report that psychological aggression is more harmful and has longer lasting negative effects than physical aggression (see Williams, Richardson, Hammock, & Janit, 2012, for a review). The detrimental effects of psychological IPA highlight the importance of further understanding risk factors for psychological IPA. The current study uses a dyadic methodology among a sample of OEF/OIF veteran couples to examine the link between PTSD symptoms and psychological IPA and two variables that have previously been shown to moderate the relationship between PTSD and IPA: military status and gender (Taft et al., 2011).
Although the link between PTSD and IPA has been repeatedly demonstrated among veterans (Taft et al., 2011), most prior research has focused on veterans’ PTSD symptoms and aggression without considering the dyadic nature of the couple and the potential contribution of the partner’s PTSD symptoms. Dyadic analyses, such as the actor–partner interdependence model (APIM; Cook & Kenny, 2005; Kenny, Kashy, & Cook, 2006), allow for examining both actor effects (e.g., the influence of one’s own PTSD on one’s own IPA) and partner effects (the influence of one’s partner’s PTSD on one’s own IPA). A partner’s PTSD symptoms may increase the partner’s perception of threat, arousal, and irritability, which in turn may contribute to a hostile atmosphere, increasing risk for psychological IPA. The few studies that have used dyadic analyses have found both actor and partner effects of trauma exposure on veterans’ psychological IPA perpetration (Wolf et al., 2013) and actor effects of PTSD on displays of hostility and psychological abuse among both veterans and partners (Miller et al., 2013), suggesting the importance of examining both actor and partner effects of PTSD on IPA.
A meta-analysis suggested that the relationship between PTSD and physical IPA is stronger among military populations, which may be due to the differences in demographic variables between military and civilian samples (higher rates of IPA among military samples has been found to be mostly due to differences in demographics; Heyman & Neidig, 1999), the unique form of military trauma and stressors (e.g., deployment-related exposure to many life-threatening situations over long periods of time), and/or military culture and training experiences that sometimes reinforce the use of anger and aggression (Taft et al., 2011). However, the few studies that have studied both partners when examining intimate partner violence (IPV) in veterans have largely focused on male veteran–female civilian partnerships. The two studies that examined the relationship between PTSD and IPA dyadically used the same sample of couples, which included veterans from any war era, whom were mostly male (89.9%) and their partners (Miller et al., 2013; Wolf et al., 2013). No known studies have focused on IPA in women veterans’ partnerships using a dyadic approach in which both partners are included in the study design. Furthermore, it is unknown whether military/civilian status of the partner increases risk for IPA in veterans with PTSD. We are unaware of research comparing dual-military couples (i.e., both members are veterans) with couples in which only one member is a veteran. Yet when considering IPA risk in female veterans, this omission is likely obscuring important information, as nearly 48% of married women in the military have partners with military experience (Patten & Parker, 2011). While previous studies have included dual-veteran couples in addition to veteran–civilian couples (e.g., Miller et al., 2013; Wolf et al., 2013), they have not made direct comparisons between the two, instead identifying one member of the dual-veteran couples as the target veteran and grouping all partners together regardless of veteran status. Although Miller et al. (2013) found that the association between PTSD and displays of hostility and psychological abuse was equivalent for veterans and spouses, some of the individuals included as “spouses” were also veterans. Thus, it is unclear if associations between PTSD and IPA would be stronger among couples with two military members.
Another potential moderator of the PTSD and IPA association is gender, as findings from the same meta-analysis (Taft et al., 2011) suggested a stronger relationship between PTSD and physical IPA among men (including both military and civilian samples). However, this difference between genders was specifically found for physical IPA. In addition, we are not aware of previous research among veterans examining potential differences between genders in the PTSD and IPA association within a dyadic framework. Previous studies examining PTSD and IPA among military couples (e.g., Miller et al., 2013; Wolf et al., 2013) have distinguished members of the couple by an identified veteran and spouse rather than gender, which has limited the ability to fully examine potential gender effects. In dyadic studies of veterans (those that include both the veteran and their marital/romantic partners), veteran status and gender are conflated. It is important to disentangle the relative contribution of veteran (versus civilian) status with gender effects.
The current study extends previous research by differentiating the roles of military status and gender in the association between PTSD and psychological IPA among a sample of OEF/OIF veterans, who are half women, and their partners, some of whom are also veterans. The current study used dyadic modeling to examine both actor and partner effects (see Figure 1). We expected actor effects of PTSD on psychological IPA. Specifically, we hypothesized that higher levels of one’s own PTSD would be associated with greater levels of one’s own IPA, and expected this effect would be stronger for men and veterans. We also predicted partner effects of PTSD symptoms on psychological IPA consistent with previous research (Wolf et al., 2013), such that greater PTSD symptoms in one’s partner would be related to ones’ own psychological IPA perpetration.
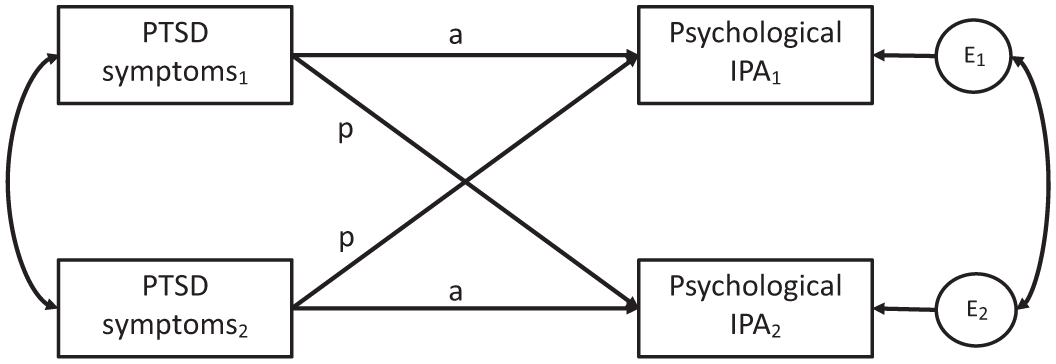
Actor–partner interdependence model.
Method
Participants and Procedure
Participants were 159 couples in which one of the members of the couple had previously participated in a larger study of OEF/OIF veterans after deployment, the Survey of Experiences of Returning Veterans (SERV) Study, which was designed to assess experiences of veterans who had combat exposure (see Laws, Mazure, McKee, Park, & Hoff, 2016; Park et al., 2017; Smith et al., 2014; Whiting et al., 2016, for more information about the SERV study). For the present couples substudy, participants who indicated they were willing to be contacted about future studies were mailed invitations to participate as well as blank surveys for themselves and their partners to complete regarding their relationship and mental health. To facilitate gender comparisons, all women veterans (n = 351) were sent invitations to participate in the couples study, and an equivalent size group of male veterans were recruited by randomly selecting 351 of the 499 male veterans from the SERV study for recruitment in the present couples substudy. Veterans and partners who returned completed surveys were included in the present study. Participants were each provided with $25 per survey ($50 total per couple). The sample included 80 women veterans and their partners, and 79 male veterans and their partners. The average age of participants was 39.16 (SD = 9.69, range = 21-69.5), and veterans from the parent study were 6.11 years from their deployment experiences on average (SD = 2.78, range = 1.12-13.40 years). Regarding gender, 162 participants (50.9%) identified as women, 155 (48.7%) identified as men, and one participant was missing gender information. One hundred couples were veteran–civilian couples (30 female veteran–civilian couples and 70 male veteran–civilian couples) and 59 couples were “dual-veteran” couples (i.e., couples in which the partner identified as a veteran or as active military). The vast majority of couples were in opposite sex relationships; however, there were seven same-sex female veteran partnerships, and four same-sex male veteran partnerships. While these sample sizes were too small to allow us to test for differences between opposite versus same-sex relationships, the modeling technique described below allowed for the inclusion of both types of couples in all analyses.
Measures
PTSD symptoms
PTSD symptoms were assessed with the PTSD checklist (PCL) civilian version for Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994; Weathers, Litz, Herman, Huska, & Keane, 1993). Participants rated the extent to which they had been bothered by each of 17 PTSD symptoms on a 5-point scale ranging from “Not at all” to “Extremely” during the past month. Items were summed to create a PTSD symptoms total score. Six participants did not complete the questionnaire and thus were missing PCL data.
Psychological IPA perpetration
The Psychological Maltreatment of Women Inventory Short Version (PMWI; Tolman, 1989, 1995) was used to assess psychological IPA. Participants indicated how often 14 actions occur on a 5-point scale from “never” to “very frequently.” The PMWI includes items such as, “My partner swore at me,” “My partner monitored my time and made me account for my whereabouts,” and “My partner yelled and screamed at me.” As the current study was interested in psychological IPA effects for both men and women, items were modified to be gender neutral. Each partner reported on his or her partner’s psychological IPA perpetration. Collateral reported relationship aggression is less prone to underestimation due to social desirability biases (Arias & Beach, 1987). Items were summed to create a composite score, with higher scores indicating greater levels of psychological IPA perpetration. Six participants were missing PMWI data.
Analytic Approach
The current study used multilevel modeling (MLM) for dyadic data using the APIM (Cook & Kenny, 2005; Kenny et al., 2006) to examine the association between PTSD symptoms and psychological IPA among couples. In the APIM framework, the data from each partner are treated as nested scores within a group of two, and the degree of nonindependence between their outcomes is estimated as a covariance with a compound symmetry covariance structure (Campbell & Kashy, 2002; Kenny et al., 2006). This approach allows for the examination of both actor effects (e.g., the influence of one’s own PTSD on one’s own IPA) and partner effects (the influence of one’s partner’s PTSD on one’s own IPA) on outcomes while accounting for the interdependence between the two members’ outcomes. The multilevel models were estimated using restricted maximum likelihood estimation within SAS PROC MIXED.
To examine differences between dual-veteran couples and couples with one veteran and one civilian, two dummy codes were created that reflect comparisons between (a) civilian partners in veteran–civilian partnerships and veterans in dual-veteran couples and (b) veterans within veteran–civilian partnerships and veterans in dual-veteran couples. In addition, a code was created for gender with men coded as 0 and women coded as 1. PTSD was centered so that 0 equaled its mean. Interaction terms were computed by multiplying variables together. In addition to the main independent variables, we controlled for age. A total R2 used to describe effect size was calculated as the square of the correlations between the measured outcome and the outcome predicted by the multilevel model (see Watkins et al., 2014).
We estimated a series of multilevel APIMs. The first model examined the impact of actor and partner main effects on psychological IPA perpetration (i.e., actor and partner effects without separating effects for veterans or by gender). The second model examined whether the actor and partner effects of PTSD on psychological IPA were modified by military status of the actor or partner (e.g., are the effects of PTSD on psychological IPA different for veterans vs. civilian actors, are the effects of PTSD on psychological IPA different for individuals with military vs. civilian partners). The third model examined whether the actor and partner effects of PTSD on psychological IPA were modified by gender (e.g., are the effects of PTSD on psychological IPA different for men vs. women). The fourth and final model examined all predictors together, including the interaction between PTSD, gender, and military status, which allows us to examine such questions as, “Does the effect of PTSD on psychological IPA among men differ between veterans versus civilians?”
Results
Descriptive Statistics
The mean PCL total among veterans was 40.3 (SD = 16.76, range = 17-84) and among civilians was 28.4 (SD = 11.06, range = 17-74). Using a cutoff of 50 indicating a likely clinical diagnosis of PTSD for those with military experience (Weathers et al., 1993), 35.4% of male veterans and 28.7% of female veterans met this criterion. For civilian populations, a slightly lower cutoff of 44 is recommended to indicate a likely clinical diagnosis of PTSD (Weathers et al., 1993), and 4% of male civilians and 16.4% of female civilians carried a likely PTSD diagnosis. Regarding psychological IPA, the mean among veterans was 23.51 (SD = 10.81, range = 14-70) and the mean among civilians was 23.15 (SD = 8.77, range = 14-60). Descriptive statistics for the primary variables of interest for each subgroup (i.e., male veteran with civilian partner, male veteran with military partner, female veteran with civilian partner, etc.) are displayed in Table 1.
Sample Descriptives.
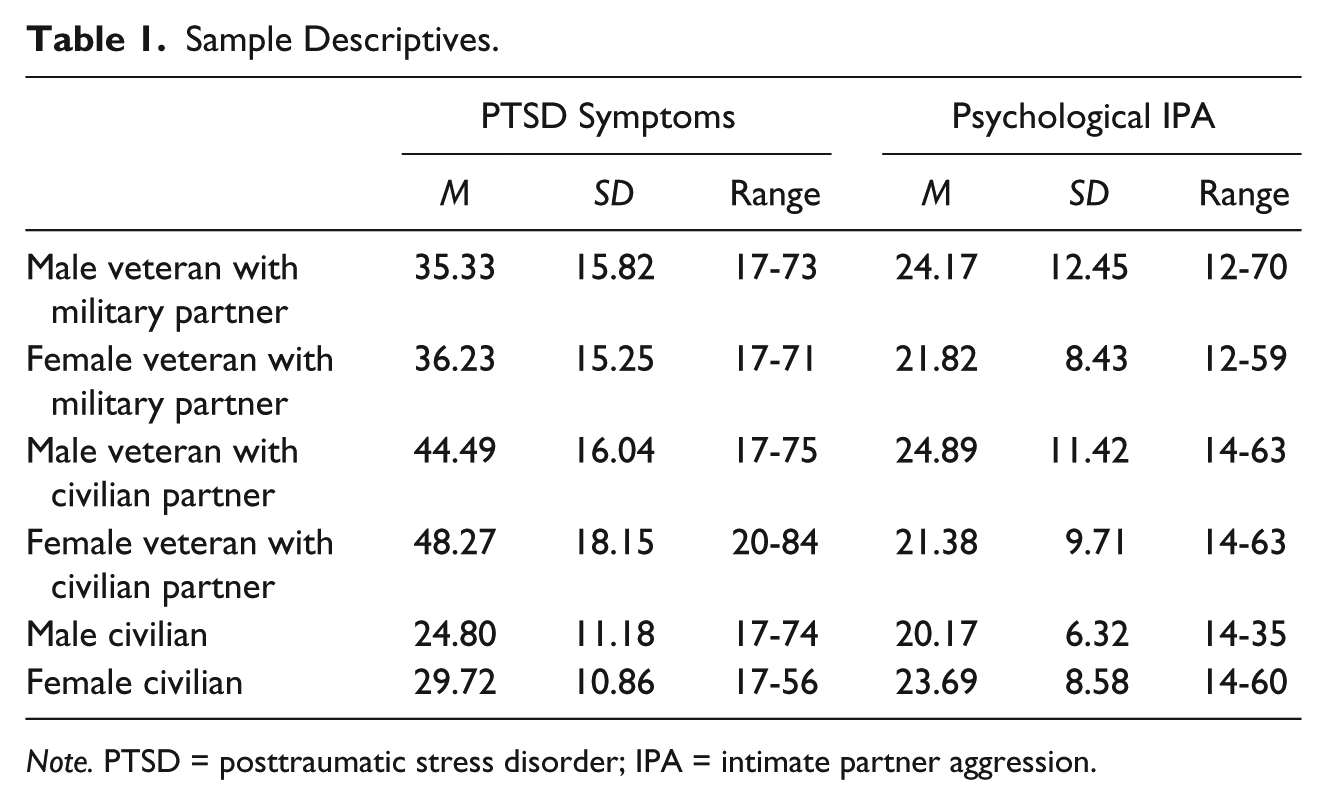
Note. PTSD = posttraumatic stress disorder; IPA = intimate partner aggression.
Multilevel Models Results
In the first APIM, we examined the main effect of actor and partner PTSD symptoms on psychological IPA. Results demonstrated a significant actor and partner effect (Est. = 0.18, p < .001, Est. = 0.21, p < .001) of PTSD symptoms on psychological IPA perpetration.
In the second APIM, we examined whether veteran status moderated the association between actor or partner PTSD and psychological IPA. This model demonstrated that the significant actor effect of PTSD symptoms on psychological IPA perpetration (Est. = 0.12, p < .05) was not impacted by the actor’s or partner’s veteran status (Est. = 0.07, p = .48, Est. = 0.06, p = .49, respectively). In addition, the partner effect of PTSD was significantly associated with IPA (Est. = 0.22, p < .05), and this effect was not affected by the actor’s veteran status (Est. = −0.04, p = .63). However, the partner effect of PTSD was stronger among individuals with a civilian partner (Est. = 0.21, p < .05) than those with a military/veteran partner.
In the third APIM, we examined whether gender moderated the relationship between PTSD and psychological IPA and did not examine veteran status. This model demonstrated a significant actor effect and partner effect of PTSD symptoms on psychological IPA perpetration (Est. = 0.18, p < .0001, Est. = 0.25, p < .0001, respectively), both of which were not moderated by gender (Est. = 0.01, p = .84, Est. = −0.10, p = .12, respectively).
In the fourth and final APIM, we examined the full multilevel model, which included veteran status, gender, and their interaction as moderators of the PTSD and psychological IPA relationship. APIM parameters are displayed in Table 2. This model accounted for 28.3% of the variance in psychological IPA. Consistent with the previous two models, none of the actor effect interactions were significant. This finding suggests that the actor effect of PTSD symptoms on psychological IPA perpetration (the influence of one’s own PTSD on one’s own IPA) was equivalent for all participants regardless of gender or military status.
Multilevel Model Results of the Impact of PTSD on Psychological IPA.

Note. PTSD = posttraumatic stress disorder; IPA = intimate partner aggression.
p < .05. ***p < .001.
However, a significant (Est. = 0.46, p < .05) three-way interaction was found between actor civilian status, gender, and partner PTSD symptoms, suggesting that the influence of one’s partner’s PTSD on one’s own IPA differed depending on whether the actor was a civilian or veteran and whether the actor was a man or woman. This three-way interaction means that the negative interaction coefficient of gender and partner PTSD symptoms was less negative among veterans versus civilians. To further illustrate this three-way interaction, follow-up simple slopes analyses of partner PTSD symptoms were estimated (see Table 3) and graphed (see Figure 2). These analyses revealed that partners’ greater PTSD symptoms were associated with greater psychological IPA perpetration among male veterans in military couples, male veterans with civilian partners, and female civilians with male veteran partners (Est. = 0.40, p < .0001, Est. = 0.48, p < .0001, Est. = 0.17, p <.01 respectively). However, the partner effect of PTSD was not significant among female veterans or male civilians.
Multilevel Model Partner Simple Effects of PTSD on Psychological IPA.

Note. PTSD = posttraumatic stress disorder; IPA = intimate partner aggression.
p < .05. **p < .01. ***p < .001.
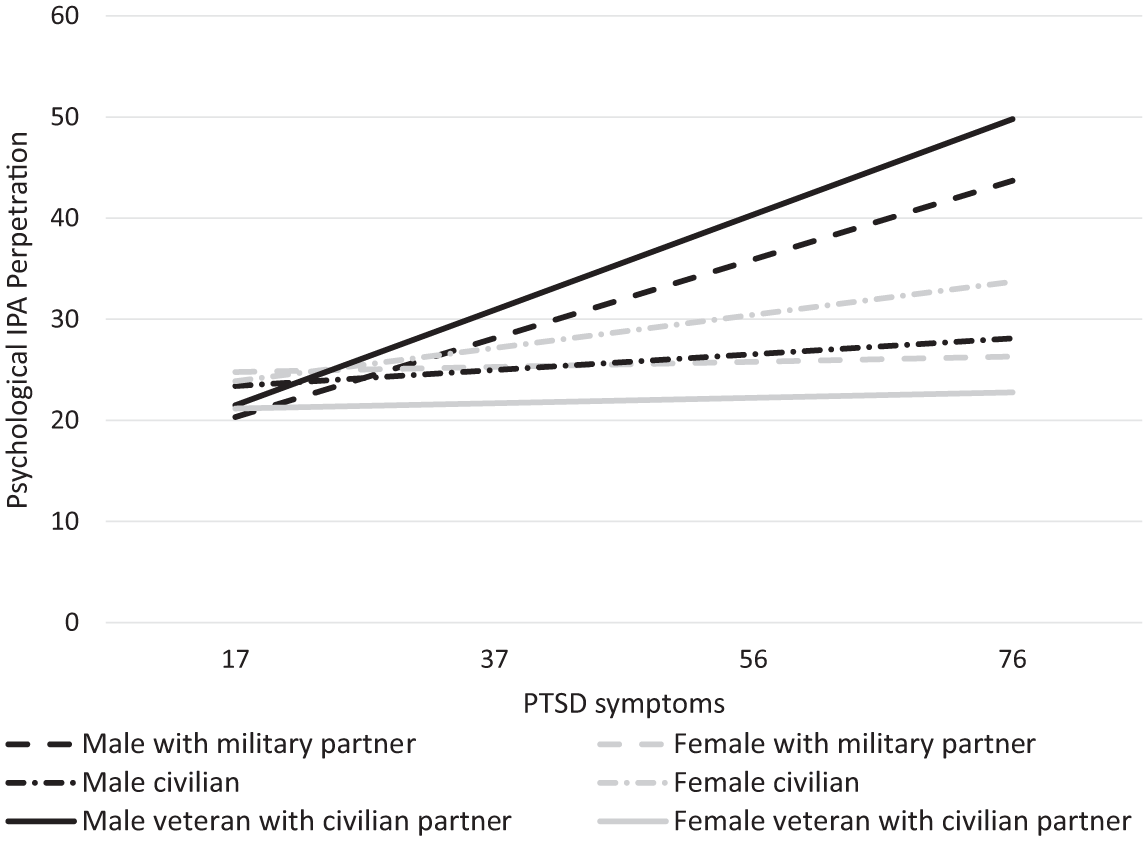
Partner effects of PTSD on psychological IPA perpetration.
Discussion
The current study examined associations between PTSD symptoms and psychological IPA perpetration among a sample of OEF/OIF veterans and their partners, some of whom were also veterans. Our study built on prior work by including an equal number of women veterans and differentiating the roles of gender and military status. In addition, the analytic modeling we used allowed us to include both opposite-sex and same-sex couples. Consistent with previous research (e.g., Taft et al., 2011), PTSD symptoms were positively associated with psychological IPA, and both actor and partner effects were found. In addition, results suggested that partner (but not actor) effects differed across gender and veteran status.
Regarding actor effects (i.e., the influence of one’s own PTSD on one’s own IPA), we found that an individual’s greater PTSD symptoms were related to his or her higher psychological IPA perpetration. This actor effect was not significantly different across gender or veteran status. This finding is in contrast to previous research showing a stronger relationship between PTSD and physical IPA perpetration among men as compared with women and among veterans as compared with civilians (Taft et al., 2011). One possibility for these null findings is that the current study is the first to have an equal number of women and men veterans. It is also possible we did not find these differences because we focused exclusively on psychological IPA, instead of physical IPA. PTSD symptoms may be more strongly associated with physical expressions of anger and hostility among men and veterans, whereas these symptoms could be equally associated with verbal expressions of anger and hostility among all individuals. In addition, the current study included a sample of couples in which at least one member was a veteran, and no couples with two civilians. Thus, it is possible the relationship between PTSD and IPA is stronger among couples with at least one veteran member as compared with civilian couples. Future research should further explore the association between PTSD symptoms and both physical and psychological IPA and potential differences of this association between genders and between couples with two veterans, one veteran and one civilian, and two civilians.
In addition to actor effects, we found several significant partner effects (i.e., the influence of one’s partner’s PTSD on one’s own IPA perpetration). Results indicated that among male veterans in dual-veteran couples, male veterans with civilian partners, and female civilians, the partner effect of PTSD symptoms was positively associated with psychological IPA perpetration. These effects significantly differed based on gender and veteran status as indicated by significant two-way and three-way interactions. Interestingly, this pattern of findings suggests partners’ PTSD symptoms are associated with greater psychological IPA perpetrated by male veterans, but not psychological IPA perpetrated by female veterans. Male veterans may have greater difficulty responding to their partners’ PTSD symptoms than female veterans, as women generally display somewhat higher rates of intimacy behaviors and emotion skills (Laurenceau, Barrett, & Rovine, 2005; Mirgain & Cordova, 2007), and thus female veterans may be able to respond to their partners’ PTSD symptoms in a more emotionally validating way. However, in contrast, veterans’ PTSD symptoms were positively associated with psychological IPA perpetrated by female civilians, but not male civilians. The reason for this difference is unclear. However, men with greater PTSD symptoms may provide less support (e.g., expressions of understanding, validation, and caring) to their partners (Hanley, Leifker, Blandon, & Marshall, 2013), creating a greater risk for relationship conflict and for women partners to be verbally aggressive. Overall, the findings of partner effects of PTSD symptoms are consistent with previous research (Miller et al., 2013; Wolf et al., 2013) and suggest the importance of continuing to use dyadic methodology and analyses in future research on PTSD and IPA.
Results from the current study have clinical implications for PTSD and couples treatment among OEF/OIF veterans. Findings from this study and previous research showing an association between PTSD symptoms and IPA perpetration suggest the importance of assessing for IPA among individuals being assessed or treated for PTSD. Furthermore, couple treatments targeting PTSD and conflict between veterans and their spouses (e.g., Monson, Fredman, & Adair, 2008) may be particularly helpful among OEF/OIF veteran couples. For example, cognitive-behavioral conjoint therapy for PTSD is a couple’s treatment for PTSD that has been shown to be effective in reducing PTSD symptoms and improving relationship quality (Monson et al., 2008; Monson et al., 2012; Monson, Schnurr, Stevens, & Guthrie, 2004). In addition, clinicians treating couples who experience psychological IPA should assess for PTSD symptoms in both members of the couple. A trauma-focused intervention for IPA, such as Strength at Homes Couples (Taft et al., 2014) that incorporates elements from interventions for PTSD and IPA and addresses common themes that may underlie trauma reactions and relationship difficulties (Taft et al., 2016), may be particularly helpful among OEF/OIF couples experiencing psychological IPA.
This study had several limitations worth discussing. The cross-sectional design does not allow for causal inferences. We also did not assess for index trauma, and thus, we are unable to link the self-reported PTSD symptoms to a particular traumatic event. It is possible, for example, that the symptom levels reported by veterans in the present study were unrelated to combat trauma or were the cumulative result of multiple traumatic experiences including their combat exposure. We used a gendered psychological abuse scale and modified it for the current study. In addition, although collateral reports of perpetration are less prone to underestimation due to social desirability biases (Arias & Beach, 1987), ideally we would have collected each member’s reports on both perpetration and victimization. In fact, our findings of interactions among partner effects and not actor effects may be due to use of collateral reports of psychological IPA perpetration (i.e., for partner effects, the same person was reporting on both predictor and outcome). In addition, our study focused solely on OEF/OIF veterans, and findings may not generalize to other veterans of other war eras or to civilian couples. Finally, we had a relatively small sample size, which may have limited our ability to find significant effects.
Despite these limitations, findings from the current study on OEF/OIF veterans build on previous literature examining the link between PTSD and IPA. Future research should continue to explore this association by examining potential mechanisms of the relationship between PTSD and IPA and examining couples with two military, one military and one civilian, and two civilians. In addition, future research should continue to examine these relationships among women veterans and same-sex couples. Continuing research in this area will help to identify and develop the most effective treatments for OEF/OIF veterans and their partners struggling with PTSD or psychological IPA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Number IK1RX002095 from the Rehabilitation Research and Development Service of the VA Office of Research and Development (PI: Laws).