
Abstract
We aimed to compare traumatic experiences among the groups of perpetrators with or without violent pedigree, and establish a structural model of posttraumatic stress disorder (PTSD) symptoms as mediators of traumatic experiences and severe intrafamilial physical violence among Chinese male perpetrators. A cross-sectional survey and a face-to-face interview were conducted to examine intimate partner violence (IPV) perpetration and violent pedigree, childhood maltreatment, other traumatic events, PTSD symptoms, and severe intrafamilial physical violence in a community sample of 229 abusive men and 303 controlled men in China. Using structural equation modeling (SEM) techniques, the scores of the questionnaires were entered into the theoretical model and calculated. Findings demonstrated that the numbers of the traumatic events in four groups were significantly different with a declining trend, and the SEM data had an adequate fit. The loadings of pathways from childhood witness domestic violence (DV) to severe physical violence (SPV) were more salience than other pathways, and the indirect effect of every pathway, except for the childhood witness DV to PTSD symptoms, on severe intrafamilial physical violence in the model was significant. The results suggest that PTSD symptoms cluster as mediator of the intergenerational transmission of SPV perpetration in Chinese abusive men. Childhood witness IPV has effects on adulthood perpetration of IPV.
Keywords
Intimate partner violence (IPV) still exists everywhere irrespective of origins, ethnics, and regions. IPV is a serious but preventable public health problem that affects many Chinese people. There is an increasing number of research on IPV in China in the recent years. A large epidemiological study involving 32,720 participants from 9,451 households in urban, rural, and industrial areas of Hunan, China, reported the lifetime prevalence of IPV as 16.2% (Cao, Zhang, & Chang, 2006; Cao, Zhang, & Yang, 2008). On the basis of a series of researches and practice in preventing from IPV in China, a new law on IPV has taken effect. Under the law, IPV is no longer considered a “family affair,” but a legal issue that demands action from the courts and the police.
Exposure to family-of-origin violence has been associated with IPV perpetration or violence outside during adulthood (Machisa, Christofides, & Jewkes, 2016; Milaniak & Widom, 2015; Song, Wenzel, Kim, & Nam, 2017; Will, Loper, & Jackson, 2016). A meta-analysis about the intergenerational transmission of physical abuse showed that the relative risk of abuse transmission was 12.6 (95% confidence interval [CI] = [1.82, 87.2]) (Ertem, Leventhal, & Dobbs, 2000). Another research from Wave 4 of the National Longitudinal Study of Adolescent Health explained the importance of genetic factors in the etiology of IPV (Barnes, TenEyck, Boutwell, & Beaver, 2013), which suggested the intergenerational transmission of IPV from biological perspective. Therefore, it is critical to explore the mechanism of the intergenerational transmission of IPV by comparing the differences among the families with or without violent history.
Posttraumatic stress disorder (PTSD) symptom is a potential risk factor for perpetration of IPV. Violent trauma exposures, including child abuse, are risk factors for PTSD. PTSD is a psychiatric disorder which is understood as a “normal” reaction to “abnormal” events (Jones, Hughes, & Unterstaller, 2001). PTSD symptoms, as defined in Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013), include reexperience/intrusion, avoidance, negative alterations in cognitions and mood, and marked alterations in arousal and reactivity. Negative alterations in cognitions and mood refer to inability to recall key features of trauma, negative affect, and difficulty experiencing positive affect, which is possible to increase the problems of emotional regulation and anger management. The final cluster, labeled alterations in arousal and reactivity, is similar to the hyperarousal cluster of symptoms described in Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000). Military populations may experience more severe forms of domestic violence (DV) than the general population. Previous studies have documented strong relationships between PTSD and IPV perpetration among veterans from Vietnam, Iraq, and Afghanistan (LaMotte, Taft, Weatherill, Scott, & Eckhardt, 2014). However, it is unclear whether PTSD or PTSD symptoms moderate the relationship between previous traumatic experiences and current IPV perpetration in community samples. There are a number of potential confounding variables as moderators to the relationship between PTSD and IPV perpetration, including emotional regulation and anger management skills, social information processing, dependency schemas, and so on (Kachadourian et al., 2013; Kar & O’Leary, 2013). Taft et al. (2015) took interview with spouses of the U.S. veterans in DV and found that social information processing factors represented pathways through PTSD symptoms related to anger expression and IPV perpetration (Taft et al., 2015). Among the PTSD symptom clusters, hyperarousal symptoms were most strongly associated with anger expression and IPV perpetration. Cognitive biases mediated PTSD and anger expression, which suggested that social information processing mediated the relationship between PTSD symptoms and aggression (Taft et al., 2015). A new systematic review showed that mental disorders among military personnel are associated with past year DV perpetration, especially PTSD, but current data review cannot confirm whether PTSD represents a similar risk for perpetration of IPV in the general population (Trevillion et al., 2015). Wolf and his colleagues (2013) focused on the dyadic analysis of influence of trauma exposure and PTSD on IPV in trauma-exposed veterans and their spouses using structural equation modeling (SEM), which suggested that trauma experiences and possible presence of PTSD in both partners may be a point of IPV intervention. Another investigation examined the relationship between clinical diagnosis and IPV in 190 (34% female) adult IPV offenders, and bipolar and PTSD diagnosed participants were more likely to perpetrate IPV (Crane, Hawes, Devine, & Easton, 2014). Literatures about relationship between IPV and traumatic experiences showed experiencing DV and other traumatic events may induce chronic PTSD symptoms, including recurrent intrusion, hypervigilance, and avoidance. A community sample study found the strong relationship between childhood physical violence experience and adulthood physical violence perpetration, especially in the group with special avoidance symptoms (Milner et al., 2010).
To sum up the above, few studies have examined the relationships between PTSD or PTSD symptoms and IPV in community IPV perpetrator samples, especially in China. Furthermore, many of current studies have done retrospective studies about only one generation with IPV aggression, but few studies focus on the special families with violent pedigree. Based on previous investigations, we hypothesize the following:
Therefore, it is also predicted that childhood maltreatment or witness DV, or other nonviolent traumatic experiences may increase the likelihood of being a perpetrator of SPV in Chinese abusive men. The purposes of our current study are to explore whether PTSD symptoms mediate the intergenerational transmission of violence from different families and, at the same time, to examine the effect of childhood maltreatment or other traumatic experiences on PTSD symptoms and the relationship between PTSD symptoms and IPV perpetration in Chinese male civilians. These objectives have clinical and forensic implications for assessing the etiology and typology of severe physical perpetration and steering the intervention of abusive men in the Chinese community.
Method
Sample and Procedure
Participants of the study were drawn from six communities in three cities in Hunan, middle of China, including Changsha, Xiangtan, and Yueyang. From March 2009 to September 2010, we identified cases of DV based on the appeals for help to local Women’s Federations, Residents’ Community Committee, police stations, and the judicial branch of city governments. We recruited 252 families with known history of male-perpetrated intrafamilial SPV to participate in the study. Face-to-face interview was carried out with individual perpetrators, and self-reported measures were adopted to evaluate the frequency and extent of intrafamilial physical assaults. We identified the relevant materials of perpetrators and physical assaults through interviewing with other family members, including parents and children or neighbors above the age of 6. Twenty-three families were excluded because they failed to complete all parts of the assessment or were lost to follow-up. We also investigated 303 male controls (nonabusers) in the same communities. The age of the samples was from 19 to 58 years old. All participants were Han ethnicity without severe physical disease and psychosis.
Two psychiatrists and two volunteers from a local police station and the Women’s Federation, after completing training on interview skills and assessment methodology, were responsible for all interviews. All participants were informed of the purpose of the study and assured that all information would be strictly kept confidential. All participants agreed to participate and signed informed consent document. The study was approved by Ethics Committee of the Central South University.
Measures
Semistructured Domestic Violence Screening Questionnaire (DVSQ)
The DVSQ was used to evaluate perpetrators, victims, and witnesses of DV during the interview. The questionnaire asks whether the individual has ever been a victim, perpetrator, or witness of eight behaviors toward a member of their family and also provides a space to provide information on other similar behaviors. If the respondent answered “yes” to any of the three questions, the next step is to specify the time frame and concrete details of perpetration or victimization. The questionnaire had ever been used to the early epidemiological survey on the prevalence of DV in Hunan, China, in 2003, which showed its excellent internal reliability and validity (Cao et al., 2006).
Conflict Tactics Scale–Revised (CTS-2)
CTS-2 is an instrument with strong reliability and validity widely used in the majority of research of DV (Straus & Douglas, 2004; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). We translated the scale into Chinese to assess intimate partner physical violence. To make the scale suitable for our study, we replaced “partners” with “family members.” In this study, the Cronbach’s alpha coefficient of the Physical Abuse subscale was .876.
Self-Edited Childhood Witness Domestic Violence Scale (CWDVS)
According to CTS-2, we expanded the items to investigate the forms and frequencies of witness DV in the past year. We changed “I have ever to my partner . . .” into “I have ever seen my father and mother . . .” We used the scale combining with the interview materials, indicating good reliability and validity. The internal consistency reliability was .882 for this scale in this study.
Childhood Trauma Questionnaire–Short Form (CTQ-SF)
The CTQ-SF was used to assess perpetrators’ experiences with childhood abuse and neglect. Respondents were presented with a 5-point Likert-type scale on how often various events occurred before the age of 16, ranging from never (1) to very often (5). The CTQ-SF assesses physical abuse, emotional abuse, emotional neglect, sexual abuse, and physical neglect. The Cronbach’s alpha coefficient for the Chinese Version has been found to be .64 with .75 reliability, indicating good reliability and validity (Zhao, Zhang, Li, & Zhou, 2005). For the purpose of this study, we used the added scores of five subscales. The internal consistency reliability was .90 for this scale in this study.
Traumatic Life Event Questionnaire (TLEQ)
The TLEQ is a self-report retrospective questionnaire used to investigate the past traumatic experiences, including almost all traumatic events that possibly trigger PTSD, such as war, natural accidents, vehicle accidents, being assaulted, robbed, spousal or IPV, childhood physical abuse, sexual abuse, and so on, consistent with the DSM-IV PTSD Diagnostic Criteria A1 (Kubany et al., 2000; Peirce, Burke, Stoller, Neufeld, & Brooner, 2009). The Chinese version was translated and revised according to local situations, replacing “war” to “other traumatic events.” It has been indicated to have good reliability and validity by Huang, Zhang, Xiang, and Zhou (2006).
Impact of Event Scale–Revised (IES-R)
The IES-R edited by Horowitz, Wilner, and Alvarez (1979) and revised by Marmar, Weiss, et al. (1996) was used to assess three major symptoms of PTSD, including intrusion, avoidance, and hypervigilance. Respondents were presented by themselves regarding how often symptoms occurred with a 4-point scale, ranging from “never” to “often.” The more total scores are, the more severe the symptoms are. Huang et al. (2006) translated the scale into Chinese and used in the female prisoners, indicating good reliability and validity (Horowitz, Wilner, and Alvarez, 1979; Huang et al., 2006). The internal consistency reliability was .94 for this scale in this study.
Statistical Analysis
Descriptive data analysis and correlation analysis were performed using SPSS 15.0; p values <.05 were considered significant. We utilized maximum likelihood parameter estimation (MLE) with SEM techniques using AMOS 18.0 to analyze the hypothesized theoretical model. The measurement models consisting of the latent construct of PTSD symptoms including three major symptoms were administrated to explain the observed data. The two structural models were computed to test the adequacy of the hypothesized structural equation models, including the latent variable and three observed variables, respectively. The theoretical models included four observed variables: witness DV in the CWDVS, childhood abuse in the CTQ, traumatic experiences in the TLEQ, and perpetration of severe intrafamilial physical violence in the DVSQ, CTS-2, and interview materials for all perpetrators of intrafamilial SPV.
Model fit was based on generally accepted thresholds for the chi-square index, goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), root mean square error of approximation (RMSEA), normed fit index (NFI), comparative fit index (CFI), and parsimonious normed fit index (PNFI). If the p value associated with the chi-square is higher than .05, the model is considered appropriate. The GFI, AGFI, NFI, and CFI range from 0 to 1, with values exceeding 0.9 demonstrating a good fit to the data. If the RMSEA is lower than 0.05, the model is considered a close fit, and if it is lower than 0.08, the model is considered appropriate (Preacher & Hayes, 2008).
The indirect and direct effects and the significance of the indirect effects were calculated by AMOS 18.0 and its bootstrapping method to clarify the confidence of all pathways in the final models (Preacher & Hayes, 2008).
Definition of Intrafamilial SPV
In this study, we defined intrafamilial SPV as the presence of the following four features through the interview: (a) evidence of physical injury of victims, including brain or visceral trauma, fractures, burns, scalds or injuries from hitting and kicking that resulted in skin petechiae, hematomas, or scars, and so on; (b) evidence of psychological injury of victims; (c) severity: (i) necessity of medical observation or intervention for over 1 week (with medical records), (ii) necessity of intervention by local Women’s Federation for over 3 times, (iii) records of police station, and (iv) one of the above three items; and (d) frequency: above three episodes in 1 year. Based on previous investigation, we modulate the definition to be more rigid (Liu et al., 2012).
We defined violent pedigree as two or more generations of violent perpetrators exist in one family. Nonviolent pedigree is a family without violent perpetrators in more than two generations. We identified the four groups according to the family features: abusers with violent pedigree (AP group), abusers with nonviolent pedigree (ANP group), nonabusers with violent pedigree (NAP group), and nonabusers with nonviolent pedigree (NANP group). A total of 229 male perpetrators of intrafamilial SPV group were analyzed. We identify two groups of perpetrators, one group is with violent pedigree (AP group, n = 136) and another is with nonviolent pedigree (ANP group, n = 93). Between the two groups of nonabusers, one group is with violent pedigree (NAP group, n = 105) and another is with nonviolent pedigree (NANP group, n = 198).
Results
Descriptive Analysis
Descriptive statistics of the sample characteristics including age, marital status, family composition, years of education, and economic status show that, except for years of education (χ2 = 86.776**), there are no statistically significant differences in age, marital status, family composition, and economic status among four groups (χ2 = 1.871, Fisher = 12.110, 16.515, and 11.320, p = .138, .141, .333, and .075, respectively). Descriptive statistics of various traumatic events and their numbers in TELQ among the four subgroups are showed in Tables 1 and 2. In Table 1, we found that experiencing natural accidents, being robbed or assaulted, spousal violence, sexual violence, and other traumatic events were significantly different among four groups (Pearson χ2 = 25.683**, 9.392*, 8.698*, 18.931**, and 16.911**, respectively). It is very interesting that the NANP group experienced more special traumatic events including violence outside and illness of relatives than other groups. In Table 2, we found the numbers of traumatic events in four groups were significantly different with a declining trend: AP group (Median = 7) > ANP group (Median = 6) > NAP group (Median = 4) = NANP group (Median = 4), Fisher = 59.286**. Descriptive statistics of three major PTSD symptoms in IES-R are shown in Table 3; the three major symptoms and the summed scores of PTSD symptoms are significantly different in four groups (χ2 = 22.642**, 23.411**, 18.462**, and 23.538**, respectively).
Descriptive Statistics of Various Traumatic Events.
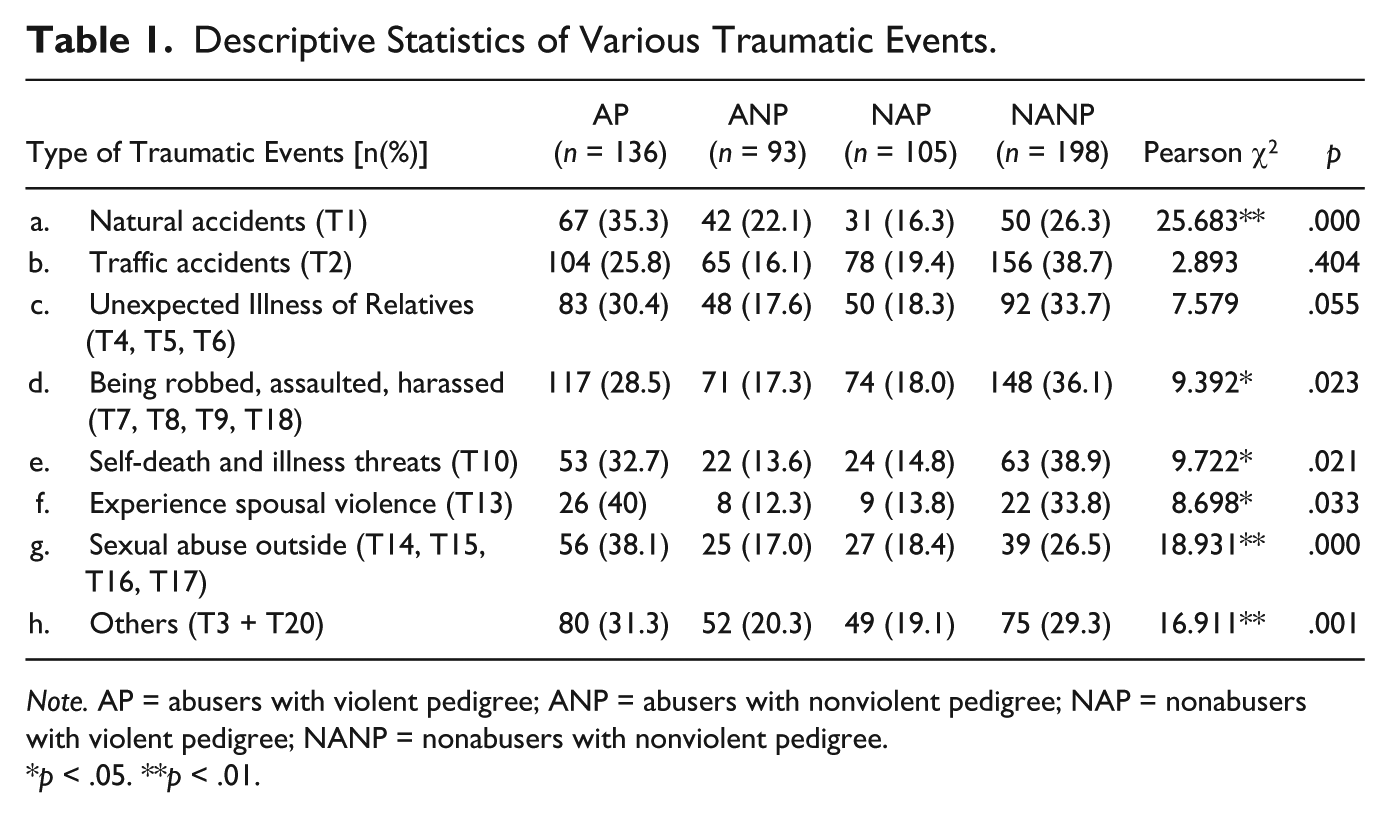
Note. AP = abusers with violent pedigree; ANP = abusers with nonviolent pedigree; NAP = nonabusers with violent pedigree; NANP = nonabusers with nonviolent pedigree.
p < .05. **p < .01.
Descriptive Statistics of Numbers of Traumatic Events.

Note. AP = abusers with violent pedigree; ANP = abusers with nonviolent pedigree; NAP = nonabusers with violent pedigree; NANP = nonabusers with nonviolent pedigree.
p < .05. **p < .01.
Descriptive Statistics of PTSD Symptoms.
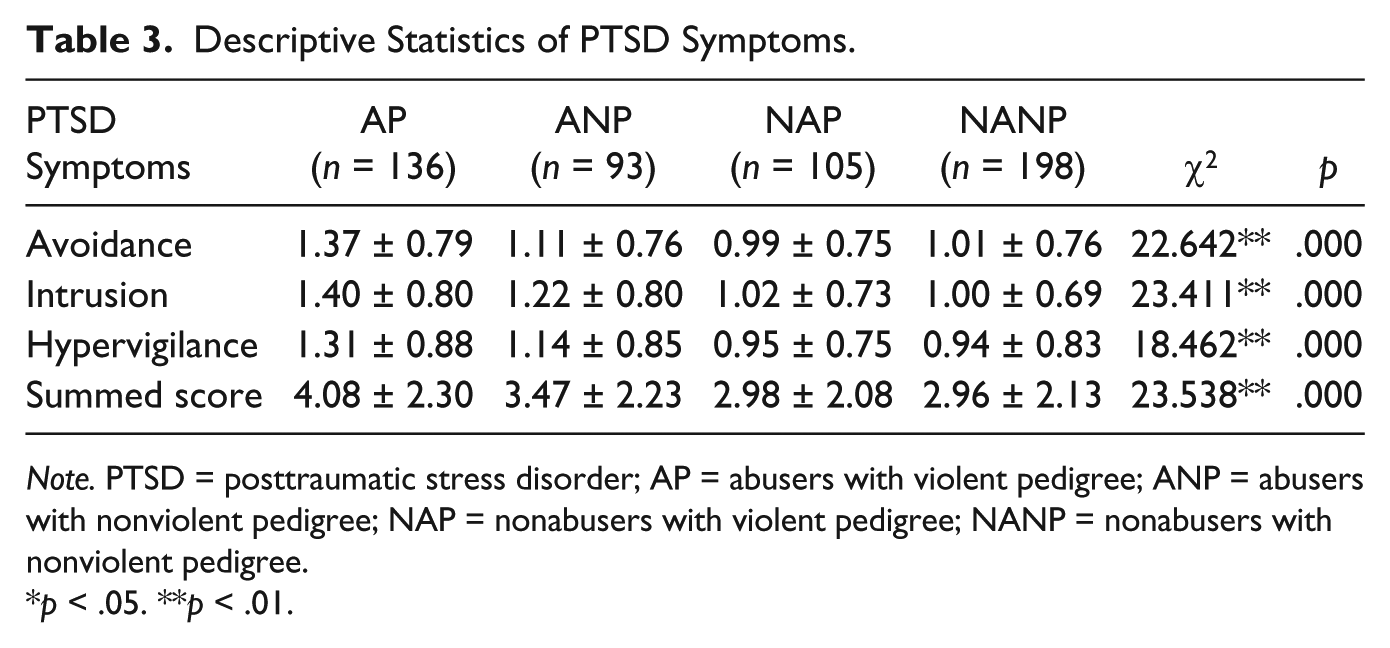
Note. PTSD = posttraumatic stress disorder; AP = abusers with violent pedigree; ANP = abusers with nonviolent pedigree; NAP = nonabusers with violent pedigree; NANP = nonabusers with nonviolent pedigree.
p < .05. **p < .01.
Bivariate Correlations Analysis
According to the correlation analysis, all of the variables were significantly and directly related to each other except for childhood emotional and physical neglect. Witness DV, childhood emotional abuse, childhood physical abuse, childhood sexual abuse, and TELQ were positively correlated with three major PTSD symptoms (r = .153**, .198*, .133**, .192*, and .268**, respectively; p < .01**, p < .05*), and childhood abuse has significantly positive relationship with three major PTSD symptoms: intrusion, avoidance, and hypervigilance (r = .168**, .168**, and .138**, respectively; p < .01**).
Model Analysis
SEM was used to test the hypothesis that the relationship between childhood experiencing abuse and adulthood perpetration of SPV is mediated by PTSD symptoms. The path model analyses in all participants are shown in Figure 1 and Table 4. A measurement model was calculated to identify the determination of every pathway. The model both contained four observed scale scores: childhood DV, traumatic experiences, childhood abuse and adulthood perpetration of SPV, and one latent variable: PTSD symptoms (identified by three observed variables: avoidance, intrusion, and hypervigilance). After being calculated and deleted one path without significant effect—from childhood witness DV to PTSD symptoms—fit indices suggested an adequate fit in Figure 2: χ2(df = 2, N = 532) = 11.895, χ2/df = 5.947, CFI = 0.997, NFI = 0.973, and RMSEA = 0.097.

Defaulted model.
SEM-Fitting Degree of Mediating Effects.
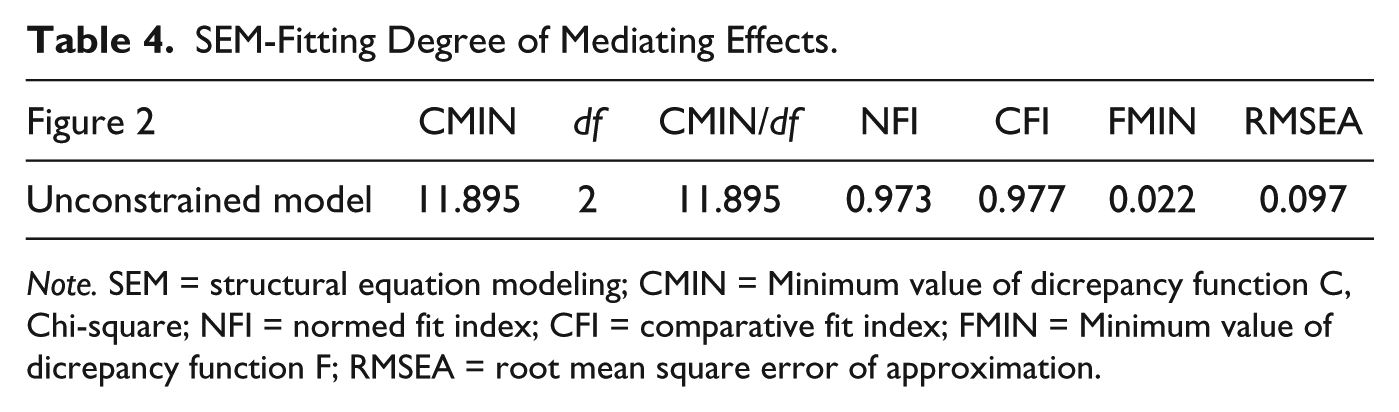
Note. SEM = structural equation modeling; CMIN = Minimum value of dicrepancy function C, Chi-square; NFI = normed fit index; CFI = comparative fit index; FMIN = Minimum value of dicrepancy function F; RMSEA = root mean square error of approximation.
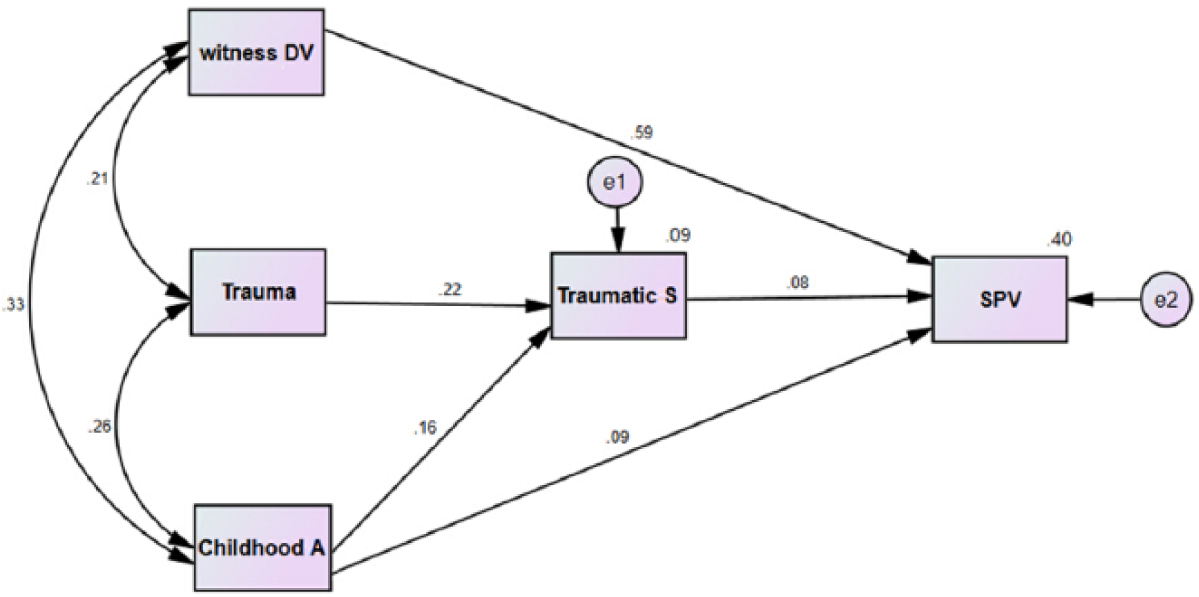
Trimmed model.
According to Figure 2, the regression coefficients of the pathways were depicted, and the loadings except for childhood witness DV to PTSD symptoms were statistically significant. As seen in Model 1, childhood witness DV was significantly related with traumatic experiences and childhood abuse, respectively (beta = .21, and .33, respectively; p < .05); traumatic experiences were significantly related with childhood abuse (beta = .26, p < .01); traumatic experiences were significantly related with PTSD symptoms (beta = .22, p < .001); childhood abuse was significantly correlated with PTSD symptoms (beta = .16, p < .001); and PTSD symptoms were positively correlated with SPV (beta = .08, p < .05). Childhood abuse and witness DV were significantly related with SPV, respectively (beta = .68, p < .001 and beta = .08, p < .05, respectively). Interestingly, the loadings of pathways from childhood witness DV to SPV were more salient than other pathways.
We determined the indirect and direct effects of predictors on perpetration of severe intrafamilial physical violence and utilized Bootstrapping method (Preacher & Hayes, 2008) to test the two-tailed significance of the standard indirect effects using AMOS. Results indicated that the indirect effects of variables except for childhood witness DV to PTSD symptoms on severe intrafamilial physical violence were significant. The indirect effect in the model of childhood abuse on severe intrafamilial physical violence via PTSD symptoms was significantly different (standardized effect = 0.012, 0.017, p < .05). In addition, the indirect effect from traumatic experiences to severe intrafamilial physical violence via PTSD symptoms was significantly different (standardized effect = 0.017, p < .05). Nevertheless, the total effects and direct effects of the pathways from childhood witness DV to severe intrafamilial physical violence via PTSD symptoms were more significant rather than indirect effects (standardized effect = 0.591, 0.585, p < .01).
Discussion
Overview of Major Findings and Implications
Traumatic experiences may increase the intergenerational transmission of IPV in violent pedigrees
Recent literature indicates that PTSD symptoms mediate the correlation between childhood abuse victimization and IPV perpetration among veteran samples, but with few among the community samples. In this study, we investigated various traumatic experiences in one’s life, including adolescence and adulthood. Results demonstrated that the medians of numbers of experiencing traumatic events were significantly different from four groups according to perpetrators with or without violent pedigree, and the medians of numbers of experiencing traumatic events of perpetrators with violent pedigree group (AP group) were more than other groups. The cumulative proportions of more than six traumatic events were 66.1%. The numbers of the four groups (from AP to ANP, NAP, and NANP groups) had a downward trend. Then, we divided and integrated 20 kinds of traumatic events, and found that AP group experienced more natural accident, spousal violence, and sexual abuse outside than the other groups, which demonstrates that perpetrators with violent pedigree may experience more special events mentioned above. And NANP group may experience varying degree of trauma, and some special trauma, including being robbed, assaulted, and harassed, or illness of self or relatives, which may increase the cohesion of partners or family members and coping ability with traumatic events, and decrease the possibility of the intergenerational transmission of IPV perpetration. Therefore, this part of the study suggests us that some special traumatic experiences may be risk factors of IPV perpetration transmission, while others may become protective factors, and different traumatic experiences may produce different results in different families. Furthermore, psychological resilience and flexible coping styles in family may be positive factors of coping traumatic experiences. Therefore, not all victims of IPV may become the perpetrators or victims in the future. The study may provide a new and detailed way to focus on the effects of different traumatic events on IPV perpetration, so as to provide new perspective to intervene on the intergenerational cycle of IPV.
Childhood witness DV and experiencing abuse are related with following traumatic experiences
Previous studies have shown that childhood traumatic experiences are associated with health and well-being in adulthood, and childhood maltreatment is related to following traumatic experiences, including sexual victimization, and IPV (Ports, Ford, & Merrick, 2016; Sheikh, Abelsen, & Olsen, 2016). Repetitive childhood and adolescence abuse, as chronic severe stress and trauma, will also contribute to individual lack of psychological safety and positive support by family, which increases anxious and avoidant attachment orientation and identification disturbance. This will further influence on personality development, emotional dysregulation, behavioral problems, and interpersonal difficulties (Hosser, Raddatz, & Windzio, 2007). These developmental basis and context would produce psychological problems and increase the possibility of interpersonal conflict and experiencing traumatic events. Correlation analyses in our study showed that childhood abuse, childhood witness DV, and traumatic experiences were related to each other, with demonstrating that childhood traumatic experiences were related with the following trauma in the adolescence and adulthood. This suggests that traumatic experiences will be serial like a chain, which play an important role to early identification and intervention of childhood maltreatment.
PTSD symptoms as mediators of traumatic experiences and severe adulthood physical violence perpetration
A substantial body of literature indicates that poor mental health is a risk factor for IPV perpetration. Previous studies demonstrated that PTSD symptoms were mediators of intergenerational transmission of IPV perpetration in the veterans, but few research was conducted in the community samples or perpetrator samples. Jakupcak and Tull (2005) found that male undergraduates who experienced various kinds of traumatic events may express PTSD symptoms and be more angry and hostile, which increase the risk of violent behavior. A newer study in the nationally representative U.S. sample (N = 25,652) suggested that theoretical and empirical work linking PTSD and perpetration of IPV in military samples extends to the general population, especially with arousal/reactivity symptom clusters (Smith, Smith, Violanti, Bartone, & Homish, 2015). Findings in this study add further support for the community samples, which indicated that traumatic experiences during childhood and adolescent phase may increase the possibility of perpetration of IPV via PTSD symptoms, although the effect size of pathway is relatively smaller than other pathways.
Stress Sensitization theory indicated that individuals who experienced adversity life events may increase the sensibility and susceptibility of stressors and express higher reaction obviously in the following life (Pedrosa, 1986). From the neurobiological perspectives, early adversity may result in Hypothalamic-pituitary-adrenal(HPA) axis imbalance, and abnormal activation in the prefrontal cortex area, which increase the sensibility of the central neuron systems to the trauma in the following life, so as to raise the risk of mood disorders and anxiety disorders during the adulthood. Furthermore, previous findings suggested emotional regulation emerged as significant predictors of IPV, but PTSD symptom severity did not emerge as direct predictors of IPV (Breet, Seedat, & Kagee, 2019; Miles, Menefee, Wanner, Teten Tharp, & Kent, 2016; Watkins, Schumacher, & Coffey, 2016).
Therefore, as the study suggests, individuals who experienced trauma during childhood may experience more traumatic events in the following life with much more PTSD symptoms, which mediated the intergenerational cycle of IPV perpetration. To sum up, early identification and intervention of traumatic experiences and symptom cluster play an important role breaking out the cycle of violence perpetration. Certainly, other individuals who experienced traumatic events during childhood or the following life did not express PTSD symptom phenotype; therefore, it is of the same importance to focus on the psychological resilience of individuals.
Childhood witness DV as direct predictors of IPV perpetration
Adverse childhood experiences, including exposure to IPV, are associated with numerous risk behaviors and mental health outcomes among the youth. As the study shows, witnessing IPV in childhood has been proposed as a principal cause of adulthood perpetration. The effect size of childhood witness DV was much more than the other traumatic events in the SEM, and only direct effects were significant. Three trends of evidence support a causal relationship between witnessing IPV in childhood and perpetrating such violence in adulthood: (a) consistency of association across a large number of studies in different populations, (b) theoretical plausibility, and (c) evidence supporting the mechanisms described in the theoretical models. A meta-analysis of 39 studies found the strength of the association to be small-to-moderate (Ertem et al., 2000). Social learning theory, as one of the most popular explanatory views in the cycle of DV, can be used to explain that severe physically abusive behaviors may be learned and modeled by exposed children (Ertem et al., 2000; Milner et al., 2010). Finkelhor and Hamby et al. (2007, 2009) presented the concept of the “polyvictimization” of children to help us understand the cumulation of victimization, based on NatSCEV (see “History of the National Survey of Children’s Exposure to Violence”) and DVS (Developmental Victimization Survey). Polyvictimization tended to persist over time. Polyvictimization was highly predictive of trauma symptoms (Finkelhor, Ormrod, Turner, & Holt, 2007, 2009). Social-cognitive models emphasize that children learn to perpetrate IPV through observing and imitating such violence in their childhood homes, without developing nonviolent conflict resolution and verbal skills. Attachment theory hypothesizes that witness IPV disrupt children’s attachment to parents and lead to emotional dysregulation, abandonment anxiety, and dependent attachment style in adulthood. Furthermore, several studies demonstrated a close link between exposure marital violence and various psychosocial problems such as physical health problems, feelings of depression and stress, and use of coercion and violence in marital conflict (Straus, 1991). According to previous studies about the adverse sequelae of childhood experiencing interparental violence, we may explain the relatively direct effects of childhood witness IPV on adulthood severely physical violence perpetration (Brown, Perera, Masho, Mezuk, & Cohen, 2015).
Limitations and Future Directions
Some limitations should be considered in the results of the current study. First, retrospective studies of childhood traumatic experiences and traumatic events in the following life may result in inaccuracy of information regarding early trauma. Prospective studies should be adopted to follow-up from childhood to adolescence to adulthood. Second, although the law of IPV has taken effect, IPV is regarded as a private event in Chinese traditional culture. Most Chinese people rationalize some degree of fighting and quarreling with partners or children as normal behavior, and even if serious violence happens in a family, such violence may be evident to outsiders. Thus, assessing childhood abuse and IPV is subject to biases. Finally, future studies may integrate other measures to assess childhood witness DV or PTSD symptom clusters, like Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) to interview with perpetration to diagnose PTSD. In addition, our sample size may be too small to accurately use SEM.
Conclusion
To our knowledge, this is the first study that attempts to evaluate the PTSD symptom clusters as mediators of the intergenerational transmission of SPV perpetration in Chinese abusive men. The contributions of this study include using multimode report and interview to identify predisposing factors of IPV, and childhood maltreatment or witness DV, or other traumatic events in the following life to elicit the intergenerational transmission of SPV perpetration via PTSD symptom clusters adopting the SEM. The comparative study of traumatic experiences and PTSD symptoms in the perpetrators with or without violent pedigree may be a special contribution in the study. Childhood witness DV has effects on adulthood perpetration of IPV. The findings of this study contribute to understanding batterer typology and serving for the intervention of batterers in mainland China, especially focusing on the PTSD symptoms of the perpetrators. Moreover, it is hoped that the current study along with the growing body of research about DV in China will motivate further investigation to more comprehensively test the theoretical models of the intergenerational cycle of DV, including context-specific risk factors and exploring protective factors. In closing, the present study offers new insight into the traumatic experiences of the perpetrator in different family with or without violent pedigree in Chinese community. The study also provides new view to evaluate the trauma and PTSD symptoms and even to intervene the IPV perpetrators. Future research can assess the PTSD symptoms and even the PTSD diagnosis, identify other referentially ambiguous temporal questions, and help us develop optimal strategies for intervening the IPV and decreasing the transmission of IPV perpetration.
Footnotes
Acknowledgements
We thank the Centers for Disease Control and Prevention, police station, and women’s federation of communities in Hunan Province for assistant with data collection.
Author’s Note
Na Liu and Ning Zhang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was sponsored by the China Medical Board (01-749), National Natural Science Foundation of China (30670753), and Provincial Natural Science Foundation of Jiangsu Province (BK20150080).