
Abstract
Childhood gender nonconformity has been associated with numerous adverse experiences, including peer bullying and homophobic violence. However, little is known about gender nonconformity in the context of intimate relationships, independent of sexual orientation. This study aimed to examine associations between childhood gender nonconformity and intimate partner violence (IPV) in adolescence and early adulthood. Using data from the 2007 wave of the U.S. Growing Up Today Study (N = 7,641, mean age = 22.8 years), we estimated risk ratios (RRs) for the association of gender nonconformity up to age 11 years and lifetime IPV victimization and perpetration. Models were adjusted for demographic characteristics, including sexual orientation identity. We assessed effect modification by gender and examined whether childhood abuse mediated the association between nonconformity and IPV. Males in the top decile of nonconformity were at elevated risk of IPV victimization (RR = 1.40, 95% confidence interval [CI] = [1.15, 1.71]) and IPV perpetration (RR = 2.34, 95% CI = 1.54, 3.56) compared with those below median nonconformity, adjusting for sexual orientation and demographic characteristics. There was no evidence of a similar association for females in the top decile of gender nonconformity. Childhood abuse did not mediate IPV disparities by gender nonconformity. We identify gender nonconformity as an important risk indicator for IPV victimization and perpetration among young adult males, independent of sexual orientation. Findings highlight the vulnerability of boys and men who do not conform to societal gender norms and the importance of studying gender expression as a determinant of violence. IPV prevention efforts may be improved with more explicit focus on socially constructed gender norms and support for diverse gender expressions. Further research into the pathways between nonconformity and IPV and in more diverse populations is needed to build a more comprehensive understanding of the unique experiences gender nonconforming youth face.
Keywords
Introduction
Intimate partner violence (IPV) is a widespread, but preventable, public health problem. Adolescence and early adulthood are particularly vulnerable times characterized by the exploration of romantic relationships, sexuality, identity, and values. Indeed, 71% of female and 58% of male IPV victims first experience IPV before age 25 years (Breiding et al., 2014). Consequences of IPV victimization and perpetration can be severe and long-lasting and include depression, substance abuse, antisocial behavior, disordered eating, and suicidal ideation (Banyard & Cross, 2008; Bonomi, Anderson, Nemeth, Rivara, & Buettner, 2013; Exner-Cortens, Eckenrode, & Rothman, 2013; Foshee et al., 2016; Foshee, Reyes, Gottfredson, Chang, & Ennett, 2013; Johnson, Giordano, Longmore, & Manning, 2014; Nahapetyan, Orpinas, Song, & Holland, 2014; Roberts, Klein, & Fisher, 2003; Smith, White, & Holland, 2003). Given the substantial health consequences, identifying factors that put individuals at risk for involvement in IPV is essential to creating effective prevention strategies.
Gender nonconformity (GNC)—that is, behaving or appearing in ways that do not follow conventional gender norms or are considered atypical for one’s perceived gender (Zucker & Wood, 2011)—may be one such risk factor. GNC has been associated with increased risk of depressive symptoms, posttraumatic stress disorder, and suicidality as well as decreased well-being and overall health-related quality of life (Friedman, Koeske, Silvestre, Korr, & Sites, 2006; Gordon et al., 2017; Remafedi, Farrow, & Deisher, 1991; Rieger & Savin-Williams, 2012; Roberts, Rosario, Corliss, Koenen, & Austin, 2012b; Roberts, Rosario, Slopen, Calzo, & Austin, 2013; Rosario et al., 2014). Gender differences are important since stigmatization of GNC differs for males and females, in that femininity in males is, in some contexts, less socially accepted than masculinity in females (D’Haese, Dewaele, & Van Houtte, 2016; Kane, 2006; Skidmore, Linsenmeier, & Bailey, 2006). Research on GNC has been conducted largely among samples who identify as lesbian, gay, or bisexual (LGB) and has focused primarily on bullying victimization and perpetration of aggression in peer relationships (D’Augelli, Grossman, & Starks, 2006; Toomey, Card, & Casper, 2014; Toomey, Ryan, Diaz, Card, & Russell, 2010). Little empirical evidence has been generated on GNC in the context of intimate relationships. Sexual orientation disparities in IPV have been well documented, indicating that LGB youth are at higher risk for IPV compared with their heterosexual counterparts (Dank, Lachman, Zweig, & Yahner, 2014; Reuter, Newcomb, Whitton, & Mustanski, 2017; Rothman, Exner, & Baughman, 2011). However, whether gender expression is associated with IPV independent of sexual orientation is not well understood.
One pathway linking GNC and IPV may be childhood abuse. Childhood GNC has been associated with physical, sexual, and psychological abuse victimization in childhood (Roberts, Rosario, Corliss, Koenen, & Austin, 2012a). Furthermore, child abuse is a known risk factor for IPV perpetration and victimization (Capaldi, Knoble, Shortt, & Kim, 2012; Vagi et al., 2013). Thus, if gender nonconforming children are at higher risk of childhood abuse, they may also be at greater risk of being involved in IPV compared with gender conforming children.
The present study investigates whether disparities exist in IPV involvement by childhood GNC in a community sample of U.S. young adults, independent of sexual orientation. We hypothesized that participants who reported higher levels of GNC in childhood would have higher rates of IPV victimization and perpetration compared with participants reporting lower levels of GNC in childhood, and there would be a higher magnitude association for males compared with females. We also hypothesized that childhood abuse would partially mediate the association between GNC and IPV victimization and perpetration.
Method
Participants
We use data from the Growing Up Today Study (GUTS), a national longitudinal cohort of children of participants of the Nurses’ Health Study II (NHSII), a cohort of female registered nurses across the United States (Field et al., 1999). Baseline GUTS questionnaires were mailed in 1996, and more than 16,000 youth enrolled (7,843 boys and 9,039 girls). Since then, participants completed self-administered questionnaires, annually until 2001 and biennially thereafter.
The current analysis includes 7,641 individuals who responded to the 2007 survey wave, when participants were ages 20 to 27 years old (M = 22.8 years) and provided information on the primary predictor, childhood GNC, and on the key outcomes, IPV victimization and IPV perpetration. We used multiple imputation to account for missingness in household income (18% missing). All other covariates had <0.5% missing data, so participants missing data on those covariates were excluded from the analysis. The Brigham and Women’s Hospital Institutional Review Board approved this study.
Measures
Primary predictor: GNC
Childhood GNC was measured in 2005 and 2007 with four questions from the Recalled Childhood Gender Identity/Gender Role Questionnaire (Zucker et al., 2006). The questions assessed gendered behaviors up to age 11 years, including media characters imitated or admired, roles in pretend play, preferences for toys and games, and feelings of femininity or masculinity. Responses were on a 5-point scale from always girls or women/very “feminine” to always boys or men/very “masculine,” which was reversed for males so that higher scores indicate greater GNC. A GNC score was created by taking the mean of the four responses (Cronbach’s α = .83). The score was coded into three categories separately by gender: (a) below median (most gender conforming), (b) median to below top decile, and (c) top decile (most gender nonconforming; Figure 1).

Childhood gender nonconformity, range of mean response scores by gender among young adults (ages 20-27 years) in the U.S. growing up today study (N = 7,641).
Prior GUTS studies have used similar coding because the relationship between GNC and health outcomes appears to be nonlinear, with the strongest associations found in the top 10% of nonconforming youth (Calzo et al., 2014; Roberts et al., 2012a, 2013). The 2005 assessment of GNC was used as it is most proximal to childhood. For participants missing data in 2005 (n = 1,257, 16% of participants), we used the 2007 GNC report. There was moderate agreement between the 2005 and 2007 GNC assessments—as a continuous measure, correlation = .74, and as an ordinal measure, weighted κ = 0.49, agreement = 64.6%. Participants missing all GNC responses in both 2005 and 2007 were excluded (n = 36, 0.5% of participants).
Primary outcome: IPV
IPV was measured in 2007 with questions adapted from the Abuse Assessment Screen (McFarlane, Parker, Soeken, & Bullock, 1992). Participants were first asked if they had ever been involved in an intimate relationship that lasted 3+ months. If yes, they were asked about IPV. Of all 9,863 participants in the 2007 survey, 7,768 (79%) responded yes to ever having been in a relationship for 3+ months. Excluded participants (n = 2,095, 21%) were slightly younger, more likely to be male, identify as completely heterosexual and as a race other than White but did not differ on GNC compared with included participants.
We examined two binary lifetime IPV outcomes: (a) IPV victimization (physical, sexual, or emotional/psychological) and (b) IPV perpetration (physical or sexual). Four victimization questions asked if participants had ever been made to feel afraid, ever been “emotionally abused (e.g., threatened, insulted, yelled at, degraded),” ever been “hit, slapped, kicked, or otherwise physically hurt by,” or if their partner had ever used “threats, force, or verbal pressure to do something sexual” when they did not want to. Participants were considered to have experienced IPV victimization if they responded “yes, this happened once” or “yes, this happened more than once” to any of these four questions. Two perpetration questions asked participants if they had ever “hit, slapped, kicked, or otherwise physically hurt” their partner(s) or ever used “threats, force, or verbal pressure to make your partner(s) do something sexual when she or he did not want to?” Participants were considered to have perpetrated IPV if they responded “yes, this happened once” or “yes, this happened more than once” to either of these two questions. Participants missing information on IPV were excluded (n = 63, 0.8% of participants).
Mediator: Childhood abuse
History of abuse during childhood before age 11 years was assessed in 2007 and included violence directly experienced by the participant as well as violence witnessed by the participant in the household. The questionnaire assessed emotional, physical and sexual abuse with four items from the Childhood Trauma Questionnaire (Bernstein et al., 1994), two items from the Conflict Tactics Scale (Straus, Hamby, Boney-McCoy, & Sugarman, 1996), and two items from the Sexual Maltreatment Scale of the Parent–Child Conflict Tactics Scales (Straus, Hamby, Finkelhor, Moore, & Runyan, 1998). Emotional and physical abuse were coded as never or rarely versus sometimes or more. Sexual abuse was coded as never versus ever.
Witnessing violence before age 11 years was also assessed in 2007 with six items on hearing or seeing an adult use physical force with (e.g., shove, punch) or verbally abuse (e.g., threaten, degrade) his or her mother, another adult, or a child in the household. These items were coded as two variables to indicate witnessing physical abuse and witnessing emotional abuse and dichotomized as never versus ever.
Covariates
Gender (male or female) was assessed by maternal report at baseline in 1996. Age (in years) at questionnaire return was assessed in 2007. Race was self-reported at baseline in 1996 (coded as White or all other races, given that 95% of the baseline GUTS cohort identified as White). Sexual orientation identity was self-reported in 2007 with a question adapted from the Minnesota Adolescent Health Survey about feelings of attraction (Remafedi, Resnick, Blum, & Harris, 1992) and coded as completely heterosexual versus sexual minority (includes mostly heterosexual, lesbian/gay, mostly homosexual, and bisexual). For participants who were unsure or missing data in 2007 (n = 67, 0.9%), we used the 2005 report of sexual orientation identity. Socioeconomic position (SEP) was operationalized as annual household income in 2001, as this was the only available indicator of SEP. Household income was reported by mothers in the NHSII (coded categorically: <US$50,000, US$50,000-US$74,000, US$75,000-US$99,000, US$100,000-US$149,000, ≥US$150,000). Family structure was reported in 1996 (coded categorically as living with both parents, one parent, or one parent and a stepparent/other).
Analysis
We first examined prevalence of IPV victimization and perpetration by nonconformity separately for females and males. χ2-tests were used to test for significant differences. After fitting bivariate models to assess crude associations with nonconformity, we used multivariable loglinear regression accounting for covariates including age at questionnaire return, race, household income, family structure, and sexual orientation identity. The below median nonconformity (i.e., most gender conforming) group served as the reference category. To assess whether childhood abuse mediates the association between nonconformity and IPV, we examined the fully adjusted models adding childhood abuse as independent variables. Given that there was no attenuation of the GNC associations, we did no further mediation analysis.
For all regression models, generalized estimating equations (GEE) were used to account for the nonindependence of sibling clusters in the GUTS cohort (Zeger & Liang, 1986). We estimated risk ratios (RRs) and 95% confidence intervals (CIs) using log-binomial models (Spiegelman & Hertzmark, 2005). When the log-binomial models failed to converge, we used log-Poisson models with robust error variance (standard errors), which provide valid but not fully efficient estimates of the RRs and 95% CIs (Spiegelman & Hertzmark, 2005; Zou, 2004). To test whether the associations differed by gender, we tested gender-by-GNC interaction terms. Gender modified the associations between GNC and IPV (p < .05 for gender-by-nonconformity interaction terms), so all results are presented stratified by gender.
Multiple imputation methods were implemented to account for missing data on household income and to allow for the uncertainty of the imputed values using SAS PROC MI and PROC MIANALYZE to pool results from multiple imputed data sets (Horton & Kleinman, 2007; Yuan, 2011). We checked the sensitivity of our findings by comparing the results with multiply imputed data to the results with complete data and found no substantive differences. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, North Carolina).
Results
The analytic sample included 4,997 females and 2,644 males. Participants were 20 to 27 years of age at the 2007 wave of data collection (M = 22.8 years) and were 97% White. In the sample, 16% of females and 11% of males reported GNC in the top decile, while 23% of females and 12% of males identified as a sexual orientation minority (Table 1). Although childhood GNC was strongly associated with sexual orientation identity (p < .001), most participants (61%) in the top decile of nonconformity identified as completely heterosexual (compared with 87% and 82% in the < median and ≥ median but below top decile groups, respectively). Among females, 44% reported IPV victimization and 18% reported IPV perpetration. Among males, 26% reported IPV victimization and 7% reported IPV perpetration.
Distribution of Participant Characteristics and Violence Exposure by Gender Among Young Adults (Ages 20-27 Years) in the U.S. Growing Up Today Study (N = 7,641).
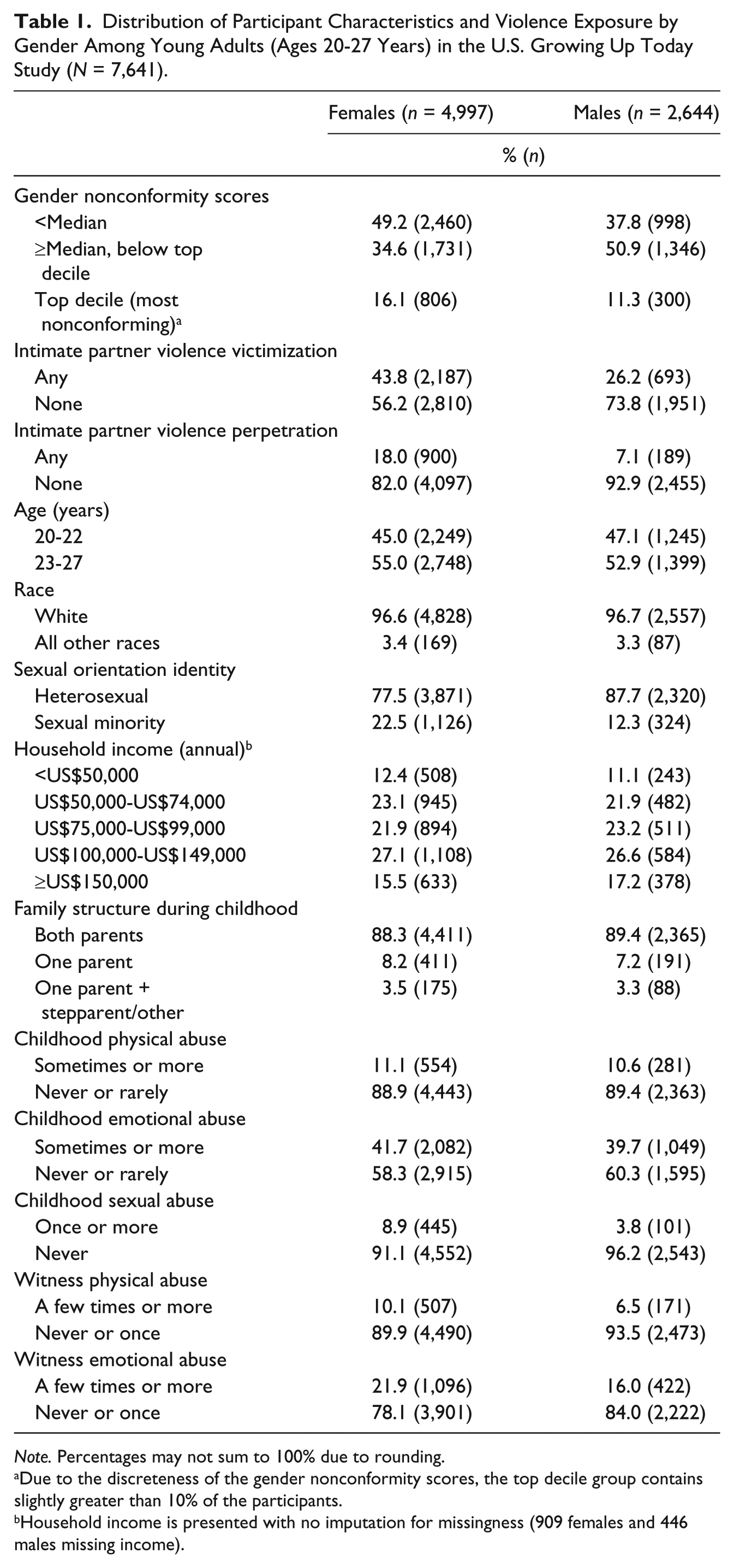
Note. Percentages may not sum to 100% due to rounding.
Due to the discreteness of the gender nonconformity scores, the top decile group contains slightly greater than 10% of the participants.
Household income is presented with no imputation for missingness (909 females and 446 males missing income).
Participants reporting higher levels of GNC in childhood had higher rates of IPV victimization and perpetration (Table 2). Among females in the top decile of GNC, 48% reported victimization and 19% reported perpetration compared with 41% and 17% for those below median nonconformity. Among males in the top decile, 38% reported victimization and 15% reported perpetration compared with 23% and 6% for those below median nonconformity. At all levels, females reported higher rates of IPV compared with males.
Prevalence of IPV Victimization and Perpetration by Childhood Gender Nonconformity Among Young Adults (Ages 20-27 Years) in the U.S. Growing Up Today Study (N = 7,641).
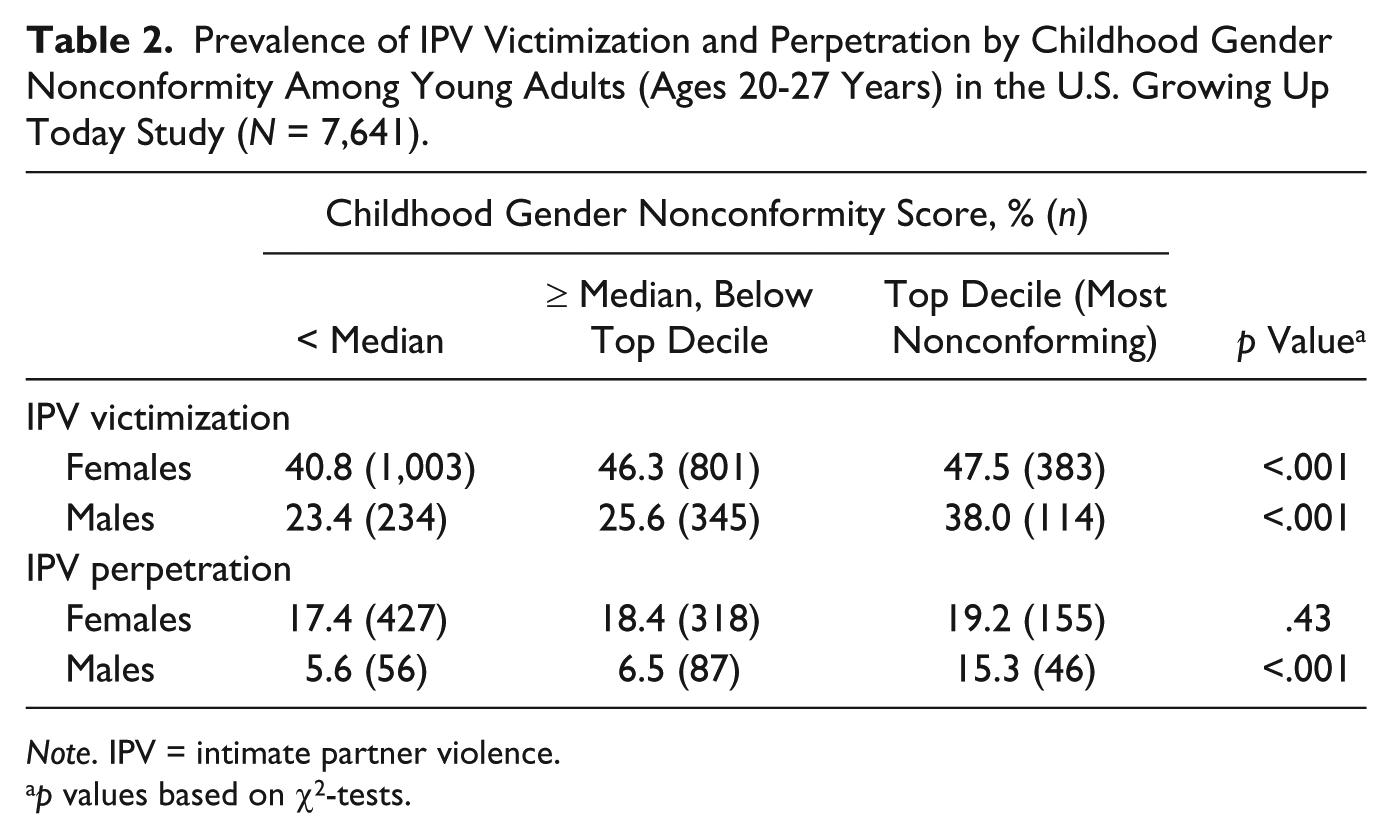
Note. IPV = intimate partner violence.
p values based on χ2-tests.
In unadjusted models (Table 3, column 1), females in the top decile of nonconformity were at elevated risk of IPV victimization (RR = 1.16, 95% CI = [1.06, 1.27]). There was no association between nonconformity and IPV perpetration for females. Males in the top decile of nonconformity were at elevated risk of both IPV victimization (RR = 1.62, 95% CI = [1.35, 1.95]) and perpetration (RR = 2.74, 95% CI = [1.89, 3.98]). After adjustment for covariates, the associations between nonconformity and IPV were attenuated (Table 3, column 2). For females, being in the top decile of nonconformity was not associated with elevated risk of experiencing or perpetrating IPV. However, males in the top decile of nonconformity had 1.4 times greater risk of experiencing IPV victimization (RR = 1.40, 95% CI = [1.15, 1.71]) and 2.3 times greater risk of perpetrating IPV (RR = 2.34, 95% CI = [1.54, 3.56]) compared with those below median nonconformity, adjusting for covariates.
Childhood Gender Nonconformity as a Predictor of IPV Victimization and Perpetration Among Young Adults (Ages 20-27 Years) in the U.S. Growing Up Today Study (N = 7,641).
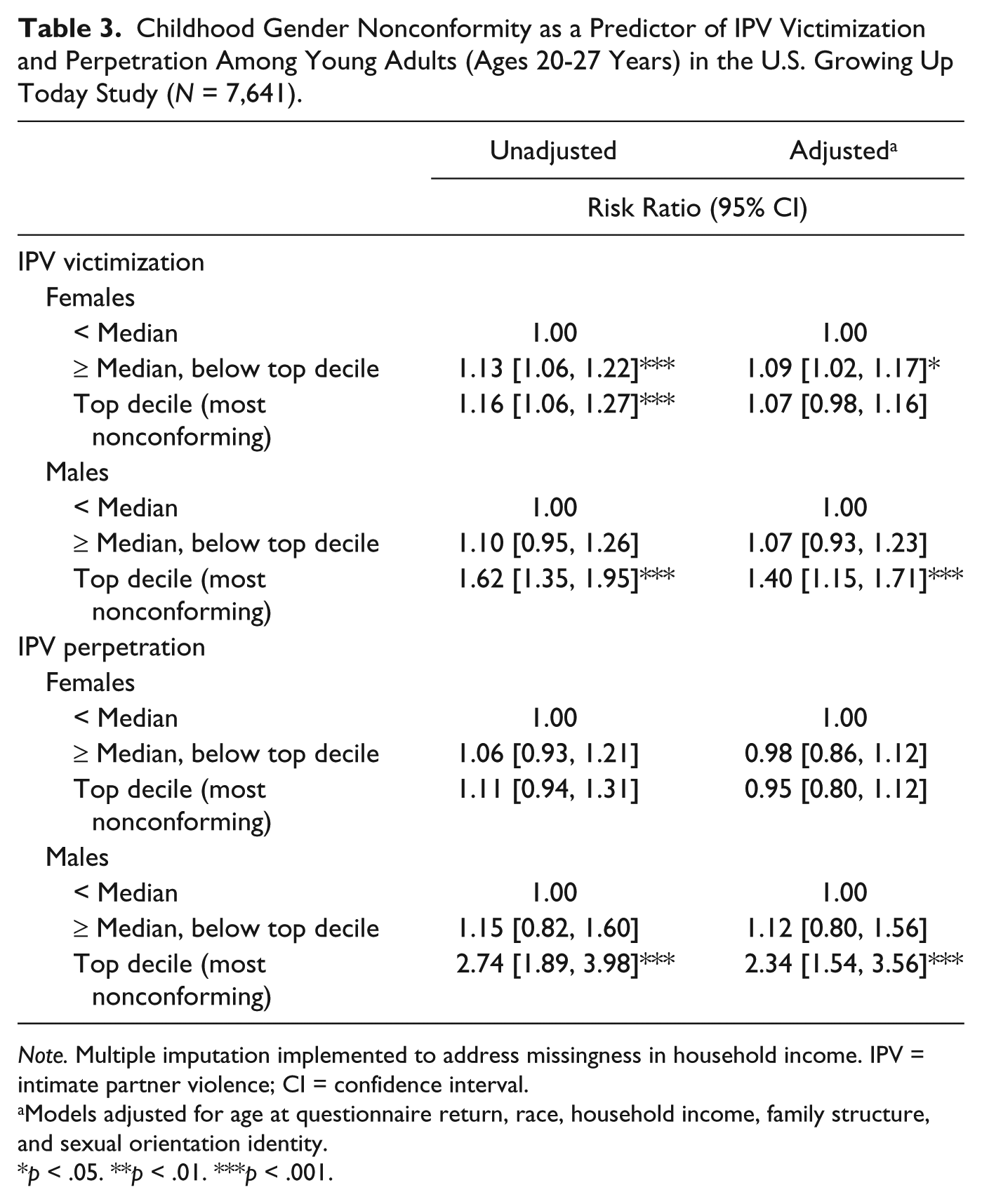
Note. Multiple imputation implemented to address missingness in household income. IPV = intimate partner violence; CI = confidence interval.
Models adjusted for age at questionnaire return, race, household income, family structure, and sexual orientation identity.
p < .05. **p < .01. ***p < .001.
We did not find support for our hypothesis of partial mediation by childhood abuse in these analyses. All five childhood abuse variables were significantly associated with GNC (p < .001). Although several of the child abuse variables were significantly associated with IPV victimization and perpetration in the adjusted models, there was no significant attenuation of the GNC effect estimates for females or males (Table 4).
Childhood Gender Nonconformity as a Predictor of IPV With Hypothesized Mediation by Childhood Abuse Among Young Adults (Ages 20-27 Years) in the U.S. Growing Up Today Study (N = 7,641).
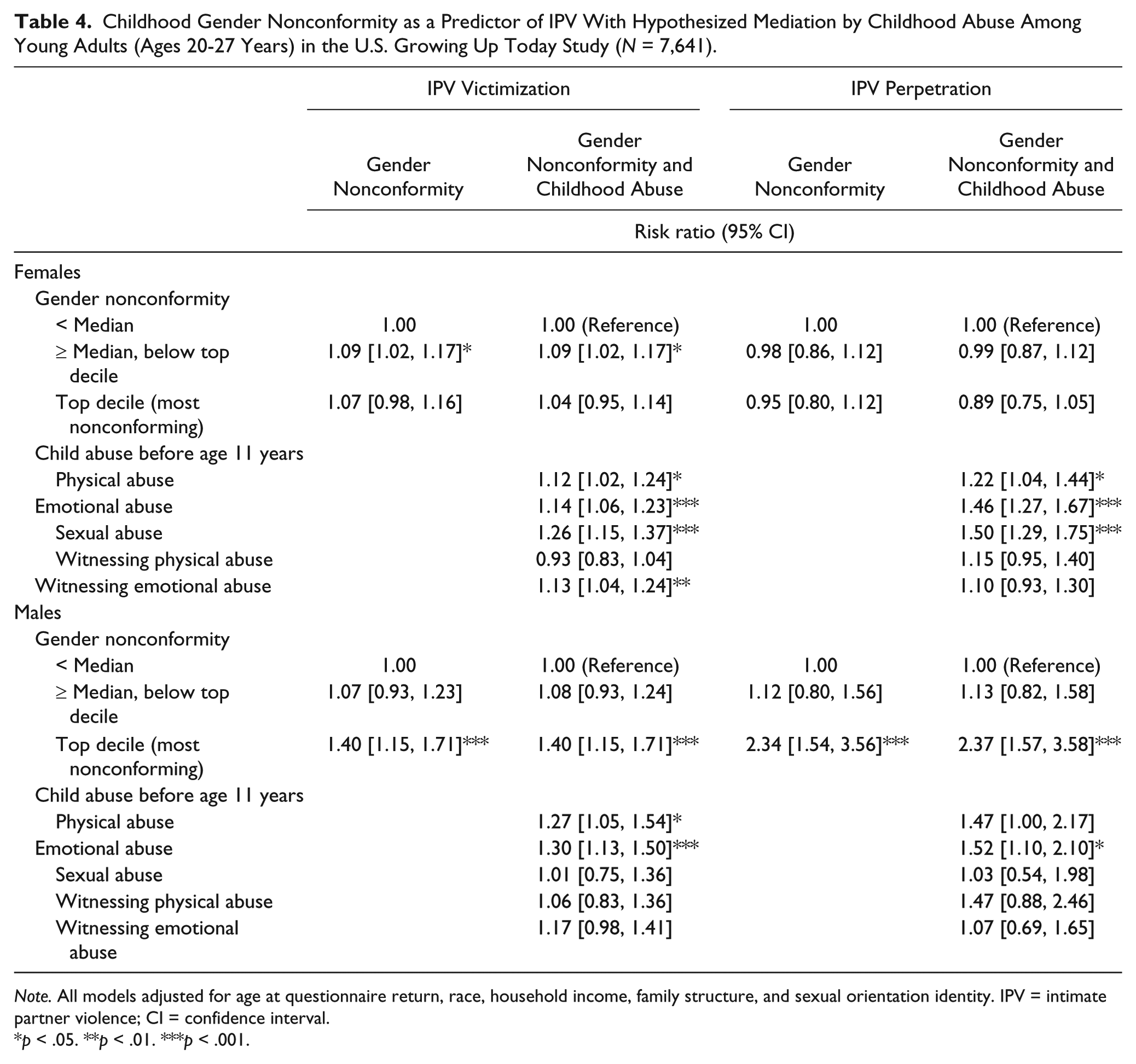
Note. All models adjusted for age at questionnaire return, race, household income, family structure, and sexual orientation identity. IPV = intimate partner violence; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Discussion
The findings from a large-scale national cohort provide evidence of a relationship between childhood GNC and involvement in IPV in adolescence and early adulthood among males. As hypothesized, young adult males in this study who reported having gender nonconforming (i.e., more feminine) behaviors in childhood were at higher risk of experiencing and perpetrating IPV compared with those below median nonconformity, independent of sexual orientation identity. Although females had substantially higher risk of IPV than males in each category of nonconformity, we found no evidence of a similar association for females in the top decile of GNC. Although most of the prior work on GNC has been conducted among LGB populations (D’Augelli et al., 2006; Ploderl & Fartacek, 2009; Skidmore et al., 2006), this study highlights the unique, independent effect of GNC in patterning IPV among heterosexual and sexual minority male young adults.
The findings of this study are consistent with prior research that individuals who transgress gender norms are vulnerable to discrimination, prejudice, and involvement in violence and aggression in a society with rigid constraints on gender expression (Gordon & Meyer, 2007; Toomey et al., 2014). The minority stress model, which suggests that individuals from stigmatized social categories experience excess stress from a range of stressors (e.g., discrimination, rejection, internalized homophobia, identity concealment) as a result of their minority social position, has been commonly applied to explain sexual orientation disparities in health outcomes and behaviors (Meyer, 2003). The concept of minority stress can apply to gender nonconforming individuals living in a society with narrow gender norms. Such individuals may be subjected to chronic stress related to stigmatization from living outside the norm. The resulting psychological disruption from the stress can lead to anxiety, depression, substance abuse, emotional dysregulation, social isolation, and poor relationship quality, which may contribute to both IPV victimization and perpetration (Hatzenbuehler, 2009). It is important to consider that IPV is often mutual and bidirectional (Langhinrichsen-Rohling, 2010), so risk factors are commonly shared, and minority stress variables have been linked to both victimization and perpetration (Capaldi et al., 2012).
A second stress pathway may link gender nonconformity to IPV perpetration specifically among men. Masculine discrepancy stress suggests men who fail to conform to conventional masculine roles (e.g., strength and self-reliance, emotional control, and pursuit of status and power) may also be at increased risk of IPV perpetration (Berke, Reidy, Gentile, & Zeichner, 2018; Fleming, Gruskin, Rojo, & Dworkin, 2015; Mahalik et al., 2003; Pleck, 1995). When males perceive themselves to be insufficiently masculine, they may experience high levels of discrepancy stress or consider actions of their intimate partners to be threatening to their masculinity, which may cause them to overconform or act out in ways that are stereotypically masculine (e.g., engaging in high-risk sexual behavior or perpetrating IPV) to prove their masculinity (Reidy, Berke, Gentile, & Zeichner, 2014; Reidy, Brookmeyer, Gentile, Berke, & Zeichner, 2016; Vandello & Bosson, 2012). This distress may also confer risk of perpetrating IPV by causing difficulties regulating emotional states, increasing pressure to suppress emotions not considered masculine and instead express emotions through anger (Berke et al., 2019).
Although the null finding for females in the top decile of GNC is consistent with literature that masculinity in females is less negatively perceived than femininity in males (Kane, 2006; Martin, 1990), we expected that nonconformity would still impact female IPV involvement through the minority stress pathway. Furthermore, a prior study found that hypermasculine men were more violent when they perceived that a woman’s behavior violated traditional feminine gender role norms, highlighting the vulnerability of women transgressing norms (Reidy, Shirk, Sloan, & Zeichner, 2009). In addition, nonconformity among females may be related to adherence to masculine norms, which has been linked to bullying behavior, anger and aggression (Gini & Pozzoli, 2006; Kinney, Smith, & Donzella, 2001). It would follow that the nonconforming females would have higher rates of IPV perpetration, but our results are not consistent with this hypothesis.
We also did not find support for our hypothesis that childhood abuse mediates the association between GNC and IPV. Nonconformity in childhood was associated with childhood abuse, as expected, as GNC may be seen as an indicator of homosexuality by family members, regardless of if and how the child identifies their sexual orientation (Kane, 2006). Parents who are uncomfortable with nonconformity or homosexuality in their children may be more likely to be abusive (Roberts et al., 2012a). However, the elevated risk of abuse for nonconforming children did not explain the relationship between GNC and IPV. In addition to the stress pathways, there may be other pathways that future research should explore as mediators, including increased substance abuse for nonconforming youth, increased peer bullying, decreased self-esteem, or decreased relationship quality due to social stigma.
Although this is the largest study to examine the contributions of GNC to IPV, the findings must be considered in light of several limitations. First, the study relied on retrospective reporting of childhood GNC, IPV, and child abuse, which may be susceptible to recall bias. The measure of GNC focused only on expression up to age 11 years, so there was no information on changes over time or expression at the time of IPV; however, at least one prior study found a positive correlation between self-reported nonconformity in childhood and adulthood, suggesting that nonconformity can be a stable trait (Rieger, Linsenmeier, Gygax, & Bailey, 2008). Importantly, gender identity was not collected by 2007 when IPV was assessed so we were not able to identify transgender participants or examine their experiences of violence.
For reporting of IPV, social desirability bias may be present. Still, research suggests that while high social desirability bias may lead to a small decrease in reports of IPV, the distortion is likely minimal (Bell & Naugle, 2007; Visschers, Jaspaert, & Vervaeke, 2015). Response bias may also be at play—individuals willing to describe their childhood behaviors as gender nonconforming may also be more willing to report IPV compared with individuals not willing to describe their behaviors as nonconforming. This may be especially true for males reporting victimization, since conformity to masculinity is a barrier to disclosing and help-seeking (Simmons, Bruggemann, & Swahnberg, 2016). In addition, sample size precluded us from stratifying by type of IPV (e.g., physical, sexual, or emotional/psychological), severity of IPV, and overlap of IPV victimization and perpetration (e.g., whether individuals were at risk of being only a victim or perpetrator of IPV or both). Although we were able to stratify by gender, we were unable to additionally stratify results by sexual orientation, a critical intersection for future studies to address. Finally, generalizability may be limited as the sample is not nationally representative as it comprises children of nurses who are predominantly White.
Conclusion
These findings from a large-scale national study highlight both the vulnerability of young adult males who do not conform to societal gender norms and the importance of studying gender expression as a determinant of violence. Independent of sexual orientation, GNC is an important risk indicator for IPV among young adult males. Building support for diverse gender expression in childhood (e.g., through the establishment of inclusive policies in institutions such as schools) and changing socially constructed gender norms may improve health outcomes. Furthermore, while the visibility of GNC places individuals at risk of IPV, these behaviors may present opportunities for pediatricians, teachers, and parents to identify children at risk, providing an avenue for prevention. Efficacy of existing IPV prevention programs should be tested among nonconforming youth, and may be improved with more explicit focus on gender expression and masculine socialization. Further research which examines pathways between GNC and IPV separately for males and females, and whether health consequences of IPV differ by conformity, in addition to research in more demographically diverse populations, is needed to build a more comprehensive understanding of the unique experiences of gender nonconforming youth.
Footnotes
Acknowledgements
We acknowledge the Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital, and Harvard Medical School for the management of Growing Up Today Study (GUTS). We would also like to express gratitude and appreciation to the team of GUTS investigators and the thousands of GUTS participants across the country.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by grants R01 HD057368 and R01 HD066963 from the National Institutes of Health (NIH). S. B. Austin is supported by the Leadership Education in Adolescent Health project, Maternal and Child Health Bureau, Health Resources and Services Administration grants T71-MC00009 and T76-MC00001. A. R. Gordon is supported by NIH grant F32 DA042505.