
Abstract
The objective of this study is to describe the frequency and type of victimization in a Spanish child and adolescent clinical ADHD sample and to analyze the association between the types of victimization and the severity of the symptoms. The sample is composed of 106 outpatients in treatment for ADHD, according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria. Symptom severity was measured by the Conners-3 scales. ADHD and comorbid diagnostics were evaluated with the Mini-Kid interview. The victimization experiences were studied using the Juvenile Victimization Questionnaire (JVQ). Children with child maltreatment history showed a greater intensity of hyperactivity/impulsivity, aggression and behavioral disorders as well as depression and anxiety disorders. The presence of peer victimization was associated with inattention, learning disorders, executive functioning, and relationship problems. Episodes of victimization should be considered in the treatment of the ADHD. Child maltreatment history is more associated with hyperactivity-impulsivity symptoms, while peer victimization is more associated with attentional symptoms.
Introduction
Victimization experiences are, in general, a risk factor for the victim’s psychopathology (Miller-Graff, Howell, Martinez-Torteya, & Hunter, 2015). Accordingly, in this context, multiple studies have found strong associations between childhood adversity and depressive symptoms, antisocial behavior, and drug use during the early transition period to adulthood that tend to persist into adulthood. These findings indicate a critical need for prevention and intervention strategies that target these early adverse experiences and their mental health consequences.
Furthermore, children with psychiatric diagnoses have significantly higher rates of victimization than do children without psychiatric diagnoses. More specifically, psychiatric diagnoses have been associated with increased risks for poly-victimization, conventional crime victimization, maltreatment, peer and sibling victimization, and indirect violence, such as witnessing violence (Cuevas, Finkelhor, Turner, & Ormrod, 2007). This poly-victimization has also been associated with more detrimental effects on mental health and a greater severity of psychiatric symptoms (Finkelhor, Ormrod, Turner, Holt, 2009; Finkelhor, Ormrod, & Turner, 2007; Finkelhor, Turner, Ormrod, & Hamby, 2009; Turner, Shattuck, Finkelhor, & Hamby, 2016).
Attention deficit hyperactivity disorder (ADHD) is characterized by a persistent pattern of inattention and/or hyperactivity-impulsivity that is more frequently displayed and is more severe than is typically observed in individuals at comparable levels of development. For example, some hyperactive-impulsive symptoms must have been present before the age of 12 years, and some impairment from the symptoms must be present in at least two settings. Furthermore, there must be clear evidence of interference with developmentally appropriate social, academic, or occupational functioning (American Psychiatric Association, 2013). As with all complex disorders, no single risk factor is either necessary or sufficient to explain ADHD. In other words, many genetic and nongenetic or environmental factors contribute to risk, and the pattern of inheritance is multifactorial for most affected individuals (Biederman & Faraone, 2005; Thapar, Cooper, Eyre, & Langley, 2013). Although genetics and pathophysiology are important factors in the etiology of ADHD, the role of psychosocial factors in perpetuating and predisposing children to ADHD may be underestimated (Richards, 2012) as the psychosocial context may well shape ADHD presentations and alter developmental trajectories, outcomes, and impairments (Thapar & Cooper, 2016). Several studies have linked early experiences to this phenotype. For example, ADHD has been found at significantly higher rates among youth who have suffered severe experiences of neglect and abuse (Humphreys & Zeanah, 2015).
Furthermore, traumatic experiences have been linked to conduct disorder (Mohr-Jensen & Steinhausen, 2016), while other authors (Ford et al., 2000) found that ADHD increases the likelihood of exposure to physical and sexual maltreatment. In a similar vein, oppositional defiant disorder (ODD) symptoms appear to be more strongly related to bullying behavior, while victimization appears to be more strongly related to ADHD (Sciberras, Ohan, & Anderson, 2012). Other authors have found associations between exposure to violence/trauma and executive functioning tasks and school problems (Lewis et al., 2015), as well as to an increase in the severity of symptoms in poly-victimized ADHD children.
In cases of severe victimization at an early age, the type of neglect may differentially affect ADHD symptom domains. For example, inattentive type was significantly associated with the likelihood of supervision neglect, physical neglect, and physical and contact sexual abuse, while hyperactive type was associated with the likelihood of supervision neglect and physical abuse (Ouyang, Fang, Mercy, Perou, & Grosse, 2008). Other authors, meanwhile, have found that the type of symptoms associated with maltreatment may be specific to inattention and impulsivity but not to hyperactivity (Becker-Blease & Freyd, 2008).
The presence of victimization has also been linked to complications in the evolution of ADHD. For example, peer victimization has been positively correlated with anxiety–depression, social problems, delinquent behavior, and aggressive behavior in children with ADHD (Humphrey, Storch, & Geffken, 2007; Sciberras et al., 2012). Physical abuse often appears as aggravating ADHD and conduct disorders (De, Sanctis, Nomura, Newcorn, & Halperin, 2012; Schilling, Aseltine, & Gore, 2007; Teicher & Samson, 2013).
ADHD children with a comorbid diagnosis present a worse prognosis and report higher rates of peer victimization than those without a comorbid diagnosis (Bejerot & Humble, 2013). There is also a known high association between ADHD with affective disorders and a poor outcome. Approximately, 10% to 40% of youth with ADHD also meet the diagnostic criteria for an affective disorder, especially in children with a history of exposure to trauma (Daviss, Diler, & Birmaher, 2009).
This study aimed to describe the frequency and type of victimization observed in a clinical sample of Spanish adolescents with ADHD and to examine the association between types of victimization and the severity of ADHD symptoms.
We hypothesized that there is a positive association between the symptomatic severity of ADHD and having suffered some type of victimization. Accordingly, children with more frequent episodes of victimization will have higher scores of symptom severity. We also expect a positive association among externalized problems such as behavior problems, aggression, hyperactivity, and impulsivity in children who have visualized domestic violence or child maltreatment as well as higher comorbidity rates with anxiety and depression in children who have experienced victimization.
Materials and Methods
Subjects
The sample included ADHD outpatients in active treatment at the Child and Adolescent Mental Health Center. The selection of patients was performed via the incidental sampling of patients who had received a confirmed diagnosis of ADHD based on a structured clinical interview (Mini International Neuropsychiatric Interview for Children and Adolescents [MINI-KID]; Sheehan et al., 2010). The incidental sampling was conducted in the order of arrival of the patient to the Center. The following inclusion criteria were used: an initial clinical diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria with or without comorbidities, age between 6 and 18 years, a medical history, a confirmed ADHD diagnosis based on a structured clinical interview (MINI-KID; Sheehan et al., 2010), and the completion of the questionnaires by the children and their parents. The exclusion criteria included the presence of an intellectual developmental disorder, autism, psychosis or an organic brain disorder. Of the 141 subjects who met the inclusion criteria, 35 were excluded for not having completed the questionnaires or for refusing to participate. The final sample included 106 patients.
Sociodemographic and clinical variables that could affect the results were considered. In children, variables such as age, gender, academic performance, treatment duration, and current pharmacological treatment were noted. The characteristics of the sample are presented in Table 1.
Sociodemographic and Clinical Variables of the Total Sample of Children and Adolescent (N = 106).
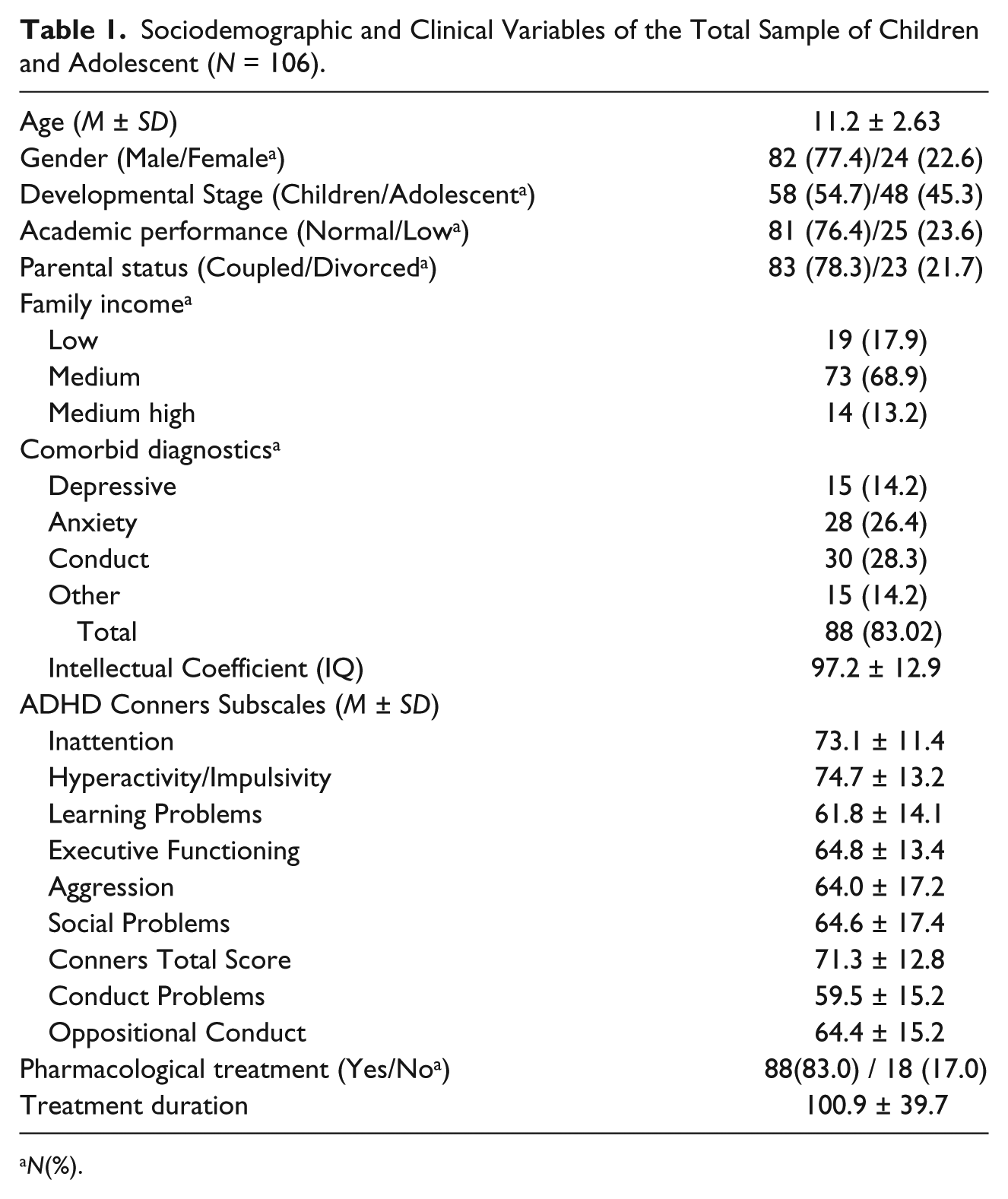
N(%).
The sample included 106 children and adolescents aged 6 to 18 years (M = 11.2, SD = 2.63). They were predominantly male (77.4%) with an average rank of intelligence (97.2 ± 12.9) and normal academic performance (76.4%), and they lived with both parents (78.3%) with a medium level of income (68.9%).
The most frequent comorbidities, measured using the MINI-KID, were behavioral disorders (28.3%), anxiety (26.4%), and depressive disorders (14.2%).
The highest scores on the subscales of the Conners-3, expressed in T scores (M ± SD), were for hyperactivity/impulsivity (74.7 ± 13.2), inattention (73.1 ± 11.4) and executive functioning (64.8 ± 13.4).
A majority of the sample (83%) was receiving pharmacological treatment at the time of the study, and the mean duration of treatment was 100.9 ± 39.7 days.
Instruments
Sociodemographic variables were collected through a specifically designed protocol. Parental marital status was either married or divorced; child academic level was classified into two categories, namely, low for children who repeated a school year or who had some type of special support measure and normal for children who were in the appropriate school year and who had school ratings within the average range; and family income included three categories, namely, low, that is, less than 1,000 euros per month; medium-low, that is, 1,001 to 3,000 euros per month; and medium-high, that is, 3,001 to 5,000 euros. Qualitative variables were presented as percentages, and quantitative variables were presented as the means and standard deviations.
The MINI-KID (Sheehan et al., 2010) was completed by parents and children when the children were below 12 years old and only by children when they were at least 12 years old. The MINI-KID interview was used to confirm the diagnoses of ADHD and comorbidities according to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). Comorbid diagnoses were grouped into the following general categories: depressive disorders, anxiety disorders, conduct disorders, and other disorders. We included in the category of other disorders those diagnoses that did not reach 10% of the sample.
The MINI-KID measure generates reliable and valid psychiatric diagnoses for children and adolescents and exhibits substantial to excellent concordance to one of the most commonly used semistructured diagnostic interviews, that is, both the present and lifetime version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS-PL) for the syndromic diagnoses including ADHD (area under curve [AUC] = 0.81-0.96, kappa = 0.56-0.87). The sensitivity of MINI-KID measure is substantial (0.61-1.00) for 15 out of 20 individual DSM-IV disorders, while the specificity is excellent (0.81 to 1.00) for 18 disorders and substantial (>0.73) for the remaining two. Interrater and test–retest kappas were substantial to almost perfect (0.64 to 1.00) for all individual MINI-KID disorders, except dysthymia (Sheehan et al., 2010). In our study, two senior evaluators, a psychiatrist and a clinical psychologist, administered the MINI-KID assessment.
The experiences of victimization were examined using the Juvenile Victimization Questionnaire (JVQ; Hamby, Finkelhorn, Ormrod, & Turner, 2005). JVQ was answered by children older than 12 years old and by parents of children who were younger than 12 years old. The JVQ explores different types of interpersonal violence from various sources, such as known or unknown adults, family members, and peers. Adapted for the Spanish population (Forns, Kirchner, Soler, & Paretilla, 2013), the JVQ categorizes the types of victimizations into five areas, namely, conventional crime, child maltreatment, peer and sibling victimization, sexual abuse, and witnessing and indirect violence. The conceptual model proposed by Finkelhor was confirmed empirically in the Spanish version for victimization data from the preceding year. The total JVQ achieved a good Cronbach’s alpha for both the preceding year (.82) and lifetime (.84) measures. Cronbach’s alpha for the different areas of victimization ranged from .49 to .70. Kendall’s tau inter-correlations between areas were positive, and nearly all were significant (Forns et al., 2013). Lifetime victimization is presented as percentages in Table 2.
Percentages of Occurrence for Each Scale and Items of the Juvenile Victimization Questionnaire for Lifetime Victimization.

The severity of ADHD was measured using the Conners-3 Rating Scale for Parents (Conners, 2008). This is a well-known, valid, and reliable scale for measuring ADHD symptoms in children aged 3 to 18 years. Subscales include inattention, hyperactivity/impulsivity, learning, executive functioning, aggression, and peer relations, as well as subscales that map onto the DSM-IV criteria for ADHD (inattentive), ADHD (hyperactive-impulsive), ADHD combined, conduct disorder, and oppositional defiant disorder. The means and standard deviations for the global index varied dependent on age. Specifically, for 6-year-olds, the mean was 5.15 with a standard deviation of 3.97, and the mean for 17- to 18-year-olds was 3.90 with a standard deviation of 4.00. The global subscale index was used to assess the severity of symptoms (Conners, 2008) and provided a good indication of psychometric properties. Internal consistency coefficients for the total sample ranged from 0.77 to 0.97, and the 2- to 4-week test–retest reliability coefficients ranged from 0.70 to 0.98. The interrater reliability coefficients ranged from .52 to .94. Support for the validity of the structure of the Conners-3 was obtained using factor analytic techniques on derivation and confirmatory samples, which yielded good levels of convergent, divergent, and discriminative validity (Conners, 2008).
To measure intelligence, we used the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV) IQ total (Full Scale Intelligence Quotient) and/or the Kaufman Brief Intelligence Test (K-BIT) compound IQ scores. The K-BIT is a brief intelligence-screening test that measures verbal and nonverbal intelligence in children, adolescents, and adults. This test consists of two subtests, namely, vocabulary and matrices, and provides a typical score for each of the subtests as well as a global composite IQ (Kaufman & Kaufman, 1997). The Spanish manual indicates reliability coefficients range from 0.76 to 0.95 for the vocabulary subtest, from 0.74 to 0.93 for the matrices subtest, and from 0.82 to 0.96 for the compound IQ. With respect to construct validity, the compound IQ K-BIT had a correlation of 0.80 with the global IQ WISC-R of 0.75 and with the WAIS-R of 0.60.
The WISC-IV (Wechsler, 2005), is a measure of intellectual ability and cognitive processing. The test which consists of four subscales, including the verbal comprehension index (VCI), perceptual reasoning index (PRI), working memory index (WMI), and processing speed index (PSI), was used to obtain a full-scale IQ score.
This scale has demonstrated to have adequate reliability coefficients and validity both in its English and Spanish versions (Wechsler, 2005). Specifically, the reliability of the Spanish adaptation of the WISC-IV presents coefficients ranging from .86 to .95, which are similar to the coefficients of the English version (Wechsler, 2005), thus demonstrating the high consistency and stability of the test.
Statistical Analysis
The presence of a link between the sociodemographic and clinical variables and the presence of episodes of victimization as measured by the JVQ were tested. For qualitative variables, the chi-square test was used, with Yate’s correction for continuity when necessary. For quantitative variables, correlational analysis was used. We used the Kolmogorov–Smirnov test to evaluate the normality hypothesis, and nonparametric tests and Spearman correlations were used when the hypotheses were rejected. An analysis of differences in the JVQ total dimension scores between groups was conducted using the Mann–Whitney U test.
Similarly, we conducted correlational analyses to examine associations among symptom severity, as measured by the Conners-3 scales, and the subtypes of victimization.
A multivariate linear regression model was performed to predict symptom severity for each dimension of the Conners scales. We included, as independent variables, the JVQ subtypes of victimization and all confounding variables that exhibited a significant correlation in the bivariate analysis. The stepwise regression method was applied.
All two-tailed p values < .05 were considered to be statistically significant. We used SPSS/ΠΧ™, version 17.0 (Armonk, NY, USA, IBM Corp).
Results
The victimization experiences found most frequently among our sample were conventional crime, which was experienced by 75.5% of the sample, and peer and sibling victimization, which was experienced by 67.9% of the sample. Other common experiences included witnessing/indirect victimization (41.5%) and child maltreatment (29.2%). Sexual victimization appeared much less frequently, with only 6.6% of the sample reporting such experiences. Table 2 displays the occurrence percentages of one or more episodes for each item in each subtype of lifetime victimization in the sample.
Witnessing/indirect victimization was present more often in those cases that required pharmacological treatment (46.6% vs. 16.7%, χ² = 5.511, p = .019) and revealed a positive correlation with age (r = .45; p = .005), with more episodes occurring in older children.
Not only was a higher association found between child maltreatment and depressive disorders (60% vs. 24.2%; χ² = 7.98, p = .005), but child maltreatment was also significantly associated with anxiety comorbidity (53.3% vs. 22.0%, χ² = 6.51, p = .011).
Moreover, the presence of any comorbidity was associated with peer victimization (75.4% vs. 56.1%, χ² = 4.29, p = .038).
There was no relation between the presence of episodes of victimization and gender, academic performance, IQ, or family income.
Correlations between the type of victimization and ADHD symptom severity were found and are displayed in Table 3. Children afflicted by conventional crime exhibited a significant positive correlation with severe symptoms of inattention (r = .34, p < .001), hyperactivity/impulsivity (r = .34, p < .001), executive functioning (r = .27, p = .006), aggression (r = .25, p = .011), social problems (r = .26, p = .007), conduct problems (r = .21, p = .030), oppositional defiant behavior (r = .20, p = .041), and Conners total score (r = .30, p = .002). Child maltreatment was also positively associated with hyperactivity/impulsivity (r = .24, p = .013), aggression (r = .22, p = .025), conduct problems (r = .21, p = .033), and Conners total score (r = .20, p = .0037). In addition, peer victimization was correlated with inattention (r = .20, p = .036), learning problems (r = .27, p = .005), executive functioning (r = .30, p = .002), and social problems (r = .23, p = .016). However, no correlations were identified for sexual victimization or witnessing/indirect victimization.
Spearman Correlation Among Child Conners Subscales, Age and JVQ Scales.

Note. JVQ = Juvenile Victimization Questionnaire.
p < .05. **p < .01.
A multivariate linear regression analysis also revealed that symptoms of ADHD, as measured by Conners scales, were associated with victimization experiences. We included all variables that exhibited a significant link in the bivariate analysis as well as those with clinical relevance, such as age, gender, family status, and all comorbidities, as presented in Table 4.
Linear Regression Analysis of the Relationship Between Conners Scores and Victimization Experiences Measured by JVQ.
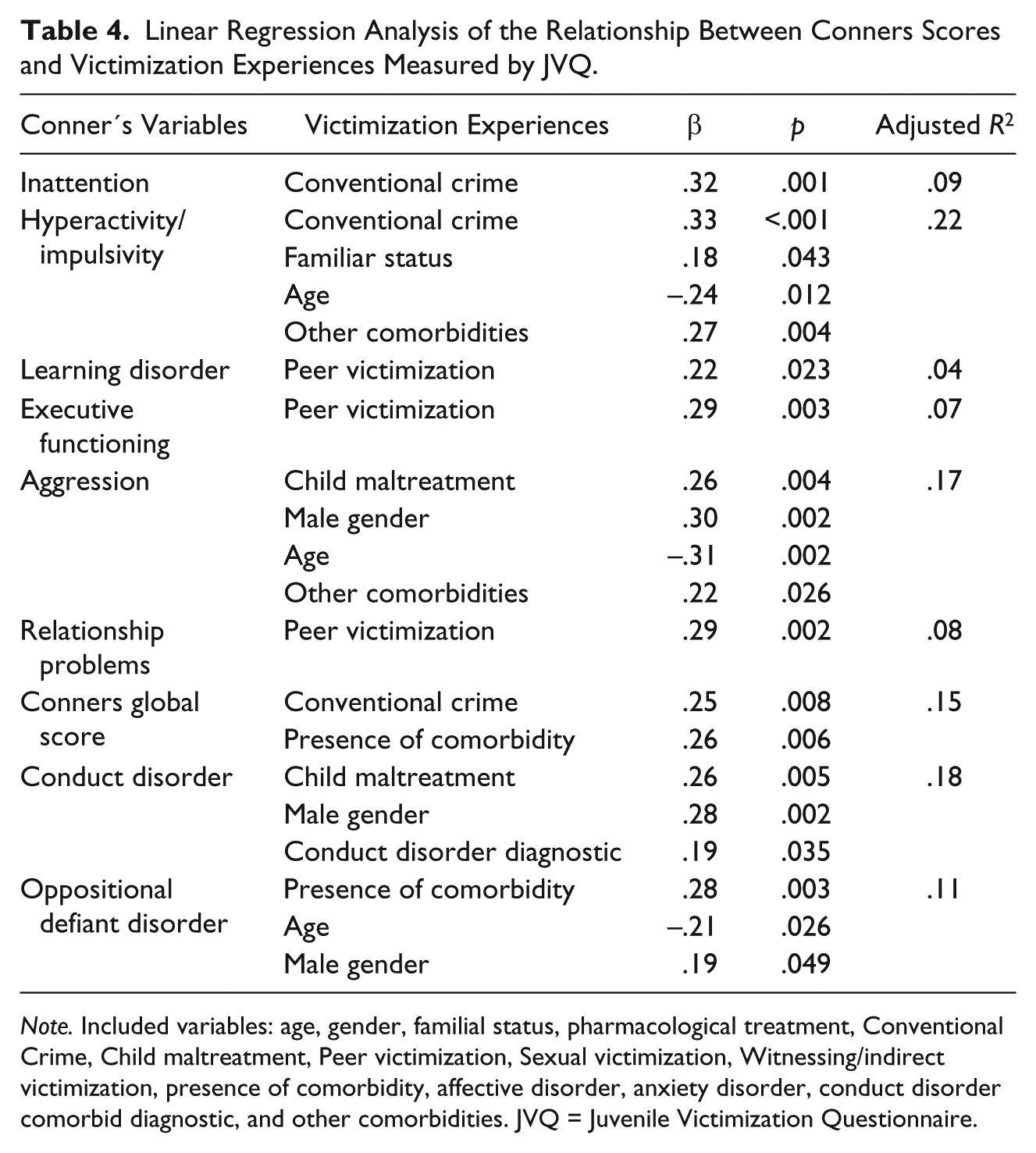
Note. Included variables: age, gender, familial status, pharmacological treatment, Conventional Crime, Child maltreatment, Peer victimization, Sexual victimization, Witnessing/indirect victimization, presence of comorbidity, affective disorder, anxiety disorder, conduct disorder comorbid diagnostic, and other comorbidities. JVQ = Juvenile Victimization Questionnaire.
The results indicate that the conventional crime scale was associated with more symptoms of inattention (β = .32; p = .001), as well as with more symptoms of hyperactivity (β = .33; p = <.001), together with lower age (β = –.24; p = .012), divorced parental status (β = .18; p = .043), and diagnostics included as other comorbidities (β = .27; p = .004). Similarly, we determined that conventional crime was associated with Conners global score (β = .25; p = .008), together with the presence of any comorbidity (β = .26; p = .006) in children. Moreover, child maltreatment was associated with the conduct disorder dimension in Conners (β = .26; p = .005), together with male gender (β = .28; p = .002), and comorbid diagnoses of conduct disorder (β = .19; p = .035). Child maltreatment was also associated with more aggression (β = .26; p = .004), together with male gender (β = .30; p = .002), lower age (β = –.31; p = .002), diagnostics included as other comorbidities (β = .22; p = .026) and oppositional defiant disorder. Finally, peer victimization experiences were positively associated with learning disorders (β = .22; p = .023), executive functioning (β = .29; p = .003), and relationship problems (β = .29; p = .002), as presented in Table 4.
Discussion
It was determined that 75.5% of the children in our sample had experienced conventional crime, compared with 60.6% identified by Finkelhor in the general population of similar age ranges (Finkelhor, Turner et al., 2009). The greater frequency of this subtype of victimization coincides with other studies (Finkelhor, Ormrod et al., 2009; Forns et al., 2013). However, our sample had higher rates of child maltreatment (29.2% vs. 10.2%) and witnessing/indirect victimization (41.5% vs. 25.3%) than did the other studies.
The first important finding of our study is that, as hypothesized, children and adolescents with ADHD often suffer episodes of victimization. Furthermore, as the presence of these experiences may be associated with more complications, episodes of victimization should be assessed and considered in the treatment of children with ADHD. However, in the case of ADHD, victimization is not always evaluated because it habitually occurs with conduct disorder (Richards, 2012).
In the obtained results, we must also emphasize the association between each type of abuse evaluated and the symptomatic dimensions of ADHD with respect to our patients.
Thus, as conventional crime was related more strongly to inattention, hyperactivity and Conners global score, we could hypothesize that inattentive children are more likely to be victimized based on their characteristics. Meanwhile, hyperactive children are more likely to engage in high-risk situations and relationships.
According to our hypothesis, with respect to our sample, child maltreatment was associated with a greater severity of externalized symptoms of ADHD, that is, hyperactivity/impulsivity, aggressiveness, and behavioral disorders, and comorbid diagnoses of anxiety and depression. These results are congruent with the literature that has indicated the presence of this association with behavioral symptoms in different contexts (Daviss et al., 2009; Ford et al., 2000; Humphreys & Zeanah, 2015; Sugaya et al., 2012) and has prompted the study of the mechanisms underlying the association (Finkelhor, Ormrod et al., 2009; Schilling et al., 2007; Shonkoff et al., 2012; Teicher & Samson, 2013).
Furthermore, consistent with our hypothesis and with the scientific literature, we found a higher rate of depressive and anxiety comorbidities with ADHD among victims of child maltreatment (Daviss & Diler, 2012; Daviss & Diler, 2014). Several studies have found clear links between child abuse and neglect with depression and anxiety (Schilling et al., 2007; Seymour et al., 2012) in adolescent and adult ADHD patients (Biederman et al., 2008; Daviss, 2008) and have indicated that child abuse and neglect play a role in the persistence of ADHD into adulthood (Lara et al., 2009; Teicher & Samson, 2013). Although the study of comorbidity was not an objective of our study, we have concluded that this topic deserves to be studied in greater depth. Furthermore, it is relevant to note that the association found between the dimensions of abuse and the symptoms of ADHD was independent of the presence of a comorbidity in our sample.
Given the high rate of this clustering of symptoms and, even more disturbing, their apparent mutual aggravation and evolutionary persistence (Daviss, 2008), evaluations and interventions should be designed with this in mind.
Another finding to emphasize is that, in contrast to other studies (Becker-Blease & Freyd, 2008; Lewis et al., 2015; Ouyang et al., 2008), no association between child maltreatment and attentional deficits was found in our study.
Peer victimization was strongly associated, in our sample, to a profile of symptoms of inattention, executive dysfunction and learning problems. We consider this association relevant because studies in the literature have also found this link with ADHD without differentiating symptomatic subtypes (Becker, Mehari, Langberg, & Evans, 2017; Bejerot & Humble, 2013; Turner, Vanderminden, Finkelhor, Hamby, & Shattuck, 2011). This result further coincides with our clinical impression that inattentive children are more vulnerable to bullying by peers and thus, it can be relevant when developing monitoring and prevention strategies for this population. Peer victimization is known to also be related to internalized, depressive, anxious, and psychosomatic symptoms and to exhibit a tendency to persist and intensify in adulthood (Copeland, Wolke, Angold, & Costello, 2013; Leadbeater, Thompson, & Sukhawathanakul, 2014). These same complications have been described with respect to the symptoms of inattention, thereby emphasizing the complexity of the interactions among symptoms, environmental factors and the evolution of the disorder in patients.
In contrast to other studies (Becker et al., 2017), there was no specific increase in the likelihood of affective disorders in children experiencing peer victimization, although they were more likely to exhibit other comorbidities.
The witnessing/indirect victimization in our sample was not associated with the intensity of ADHD symptoms or the presence of associated psychopathology, which is in contrast to the findings of other studies (Johnson et al., 2002; Lewis et al., 2015).
Among our sample, witnessing/indirect victimization occurred more frequently with increasing age and when parents were separated. In this sense, the visualization of violence at an older age may also reflect a greater awareness in older children and their tendency, based on their characteristics and their greater autonomy, to be involved in situations with more risk. Accordingly, Finkelhor, Turner and colleagues (2009) reported a substantial increase in exposure to violence after age 10. Hence, we suggest that it would be good practice to examine the relationship between exposure to violence and ADHD symptoms in older children.
Furthermore, it is possible that, in the case of the younger children whose questionnaires were completed by their caregivers, the caregivers were not aware of the child’s exposure to this type of victimization due to ignorance or to the unwillingness of the to share this information. In this case, it would be desirable to include an additional means of evaluation given the possible influence of witnessing/indirect victimization on neurodevelopment (Teicher & Parigger, 2015).
Nonetheless, despite the fact that our study did not find an association between the visualization of violence and any symptomatic subtype or the presence of a specific comorbidity, the percentages found of this type of victimization were almost double what has been described for other populations (Finkelhor, Ormrod et al., 2009), which, in itself, makes the detection of this type of abuse relevant.
It has been estimated that approximately 10% to 20% of the children in the United States witness intimate partner violence (IPV) every year, which is approximately 15.5 million youth or 29.4% of all U.S. children living in two-parent homes (McDonald, Jouriles, Ramisetty-Mikler, Caetano, & Green, 2006).
The link between family status and witnessing/indirect victimization and child maltreatment may be explained by the higher risk for the child to be exposed to suffer from traumatic experiences in single-parenthood due to the parental conflicts that triggered the family rupture and/or limited protection, supervision, and care in a single-parent household. As single-parenthood is an increasing reality in developed societies, it is advisable to increase sensitivity in both evaluations and interventions.
Our results suggest that experiences of victimization are associated with higher scores on ADHD symptoms, such as inattention, hyperactivity, impulsivity, and dysexecutive symptoms in children and adolescents. Exposure to violence, particularly during sensitive developmental periods, may affect the normal development of the brain structures responsible for regulating behaviors, and hence, such traumatic experiences may lead to neurobiological changes in response to the activation of physiological stress response systems (Humphreys & Zeanah, 2015; Shonkoff et al., 2012; Teicher & Samson, 2013). In other instances, certain disorders may be a high-risk condition for experiencing maltreatment (Finkelhor, Ormrod et al., 2009; Finkelhor, Turner et al., 2009), which in turns affects structures responsible for regulating behaviors that are deficient or maladaptive in children with ADHD.
In summary, there are several suggestions that can be deduced from our study. First, a more integrated biopsychosocial approach to ADHD is necessary. The role of psychosocial factors in promoting and perpetuating the development of ADHD symptoms has been neglected within the field of child mental health. Our study supports the growing literature that indicates that we must take into account the experiences of victimization during the evaluation of patients with ADHD. Clinicians, when told that a child has a diagnosis of ADHD, have underestimated the presence of psychosocial factors, and thus, they are less likely to ask about the possibility of neglect or abuse (Richards, 2012). Second, the consequences of the victimization episodes must be included within the treatment of ADHD. However, such multimodal treatment may be limited to motivated families with good support and may not be available to or good for families usually referred to community mental health centers, as these facilities often have more children suffering from social adversity, for example, adoptive families, experiences of abuse, neglect and visualization of domestic violence, parents with mental disorders, or addictions, and so on, and comorbidity with behavioral disorders.
Another interesting result is that scores of children with problems related to inattention, learning and social issues also have more problems with bullying. This subgroup could be a risk profile for this type of victimization and could require specific attention to prevent these situations.
A final reflection from our study concerns the stigma on the population that suffers from mental health problems. This population is sometimes perceived as aggressive, and this is even more evident in the case of ADHD. This and other studies indicate that children with ADHD are also frequently victims of situations of direct and indirect abuse.
Limitations
The main limitations of the present study are sampling type and the relatively small sample size. We also used a cross-sectional design, which could be considered a limitation, and the retrospective and correlational methodology used in our study cannot establish a causality link between variables. To accomplish this, we need longitudinal methodology and complex models that integrate environmental and biological influences that lead to disorders. As we have used a clinical sample, the results are not generalizable to the general population. For example, some types of abuse, such as sexual abuse, may be underrepresented because of the lower proportion of women in the sample, and it is much more common for this type of abuse to occur in the female gender. In a representative Spanish community sample using the JVQ, found that an experience of sexual victimization was reported by 8.8% of the sample and was more prevalent in girls (14.2%) and in older adolescents (10.6%; Pereda, Abad, & Guilera, 2016),
The Conners questionnaires were completed by parents, and thus, the victimization questionnaires may have recall bias. In the case of the questionnaires for children below 12 years of age, it is possible that the parents did not know all of the experiences of victimization or were affected by their own experiences, as could be the case for indirect victimization. In addition, parents may have hidden the presence of familial maltreatment. Nonetheless, in their study of the psychometric properties of the JVQ, Finkelhor, Hamby, Ormrod, and Turner (2005) believed that the evaluation performed suggested that caregivers generally provided adequate and comparable information to child self-reports when caregivers were interviewed as proxies regarding the experiences of children aged 2 to 9 years.
Another limitation is that the period and duration of the experiences of abuse were not defined in this study and that these data should be considered in future studies. Both factors are necessary to determine the possible impact on neurodevelopment and on the severity and persistence of symptoms, which may be crucial when making decisions regarding the types of interventions to be implemented, as some authors have noted (Teicher & Parigger, 2015).
Despite these limitations, our study may be the first to analyze specific types of victimization in a clinical sample of Spanish children and adolescents with ADHD. It is also noted that there are few studies in the international literature that have evaluated different types of victimization in children and adolescents with ADHD as most studies are limited to assessing a specific type of victimization (Becker et al., 2017; Bejerot & Humble, 2013; Chou, Liu, Yang, Yen, & Hu, 2014) or to assessing only adolescent or adult ADHD (Ferrer et al., 2016). Accordingly, we contend that by examining multiple types of victimization and by including both children and adolescents with ADHD, we enhance the value of our study.
Similarly, clinical samples may be more representative of the users we treat in the mental health centers for children and adolescents. Thus, it is necessary to integrate assessment and intervention frameworks that respond to the clinical and social realities of which we are a part (Shonkoff et al., 2012).
Conclusion
In conclusion, our study indicates a high percentage of victimization in patients treated for ADHD. In addition, we have demonstrated a differential profile between hyperactive/impulsive symptoms and behavioral disorders associated with child maltreatment and symptoms of inattention and dysexecutive and learning problems that are more associated with peer victimization.
Both findings emphasize the importance of the systematic detection of different types of victimization in children and adolescents with ADHD and the development of strategies that minimize the impact of victimization on the clinical population treated.
Footnotes
Author's Note
Fernando Lopez-Seco, Elisabet Vilella and Adela Masana-Marín are also affiliated to IISPV and CIBERSAM.
Acknowledgements
The authors are grateful to all of the children and mothers who participated in this study.
Human and Animal Rights
Research involving human participants.
Informed Consent
All families and all children above 12 years of age signed an informed consent form that was specifically designed for the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.