
Abstract
Recent studies have shown that couples’ reports of intimate partner violence (IPV) are not necessarily consistent. This study investigated the associations between patterns of partner victimization and perpetration reports and health and perceived wellbeing. Using household survey data from a probabilistic urban sample of adults aged 25 to 50 years and their partners, we identified 1,467 heterosexual pairs who completed the modified Japanese version of the Conflict Tactics Scale 2 Short Form. We classified responses into four categories: congruent report of no IPV, incongruent respondent victimization report, incongruent partner perpetration report, and congruent report of IPV. We used analysis of covariance to compare physical and mental health (measured by the SF-8 Health Survey Questionnaire) and life satisfaction among the four groups. The results showed that 22.4% of respondents were involved in IPV, and approximately 75% of them had incongruent reports. Compared with congruent reports of no IPV, respondents with an incongruent victimization report and an incongruent partner perpetration report scored significantly lower on physical health (−0.96, p = .03 and −1.16, p = .04, respectively). Those with an incongruent victimization report and congruent report of IPV had lower mental health scores (−2.32, p = .00 and −2.21, p = .00, respectively) and lower life satisfaction (−0.32, p = .00 and −0.21, p = .01, respectively). The results indicated that the respondent’s victimization report was associated with worse mental health regardless of their partner’s perpetration report, and physical health was worse only in cases with incongruent reports. Cases with a partner perpetration report but no respondent victimization report showed worse physical health but no negative effects on mental health and perceived wellbeing. These results indicate that research and practice regarding IPV should consider both partners’ experiences of violence when assessing the impact of health and wellbeing on victims.
Keywords
Introduction
Intimate partner violence (IPV) can include physical, psychological, and sexual violence. IPV has been a public health issue for decades in both developed and developing countries, with recognition of its prevalence and the severe, lifelong impact it has on victims’ physical and mental state (Campbell, 2002; Coker et al., 2002; Desmarais, Reeves, Nicholls, Telford, & Fiebert, 2012; Ellsberg, Jansen, Heise, Watts, & García-Moreno, 2008). Previous studies have mainly treated male-to-female IPV as a consequence of gender-biased power distribution in paternal societies, although recent studies have recognized that female-to-male IPV is not uncommon and that IPV can be reciprocal between couple partners (Archer, 2000; Dixon & Graham-Kevan, 2011; Johnson, 1995; McHugh, Livingston, & Ford, 2005; Straus, 2011; Whitaker, Haileyesus, Swahn, & Saltzman, 2007). Some studies have shown between-partner disagreement in IPV reports of perpetration and victimization (Caetano, Field, Ramisetty-Mikler, & Lipsky, 2009; Margolin, 1987; Schafer, Caetano, & Clark, 1998).
The identification of IPV often relies on self-reports from victims and/or perpetrators, and third-person observation (e.g., medical examination) is limited to overt cases. Although self-reports may be susceptible to report bias owing to socially desirable responses (Sugarman & Hotaling, 1997), fear of stigma (Overstreet & Quinn, 2013; Rodriguez, Szkupinski Quiroga, & Bauer, 1996), or other psychosocial reactions (Henderson, Bartholomew, Trinke, & Kwong, 2005), they are likely to reflect an individual’s perception of the quality of the inter-partner relationship.
There are several mechanisms that determine the different responses of victims to the experience of violence. Some disregard the victimized experience as a means of psychological defense (Cramer, 1987; Dollinger & Cramer, 2007). If victims recognize the violence, they may feel embarrassed and afraid of social stigma, remain silent to fit in with gender norms, experience emotional and economic dependence, or feel helpless to speak out without appropriate support resources (Bornstein, 2006; Hien & Ruglass, 2009; McCauley, Yurk, Jenckes, & Ford, 1998; Rodriguez et al., 1996; Strube & Barbour, 1983, 1984) Others may intentionally or unintentionally rely on an intimate relationship with the perpetrator partner to feel secure in their sociopsychological identity (Henderson, Bartholomew, & Dutton, 1997; Henderson et al., 2005). In all cases, victims’ recognition of, and reaction to, IPV will be influenced by how their perpetrator partner recognizes and reacts to IPV (Overstreet & Quinn, 2013).
These different patterns of recognition of victimization may further result in different psychological and behavioral responses and health consequences. However, previous studies on the health consequences of IPV examined victim-reported IPV, and a broader view of the different patterns of IPV reports between partners remains elusive owing to limitations of data and/or scope of the studies. As recent studies have started to reveal, inter-partner disagreement about reports of perpetration and victimization is not uncommon (Margolin, 1987), and focusing solely on recognized and reported victimization may overlook IPV victims who do not speak out and their unique requirements in terms of public health intervention. Although public health practitioners and hospital clinicians can support victims who report IPV victimization, they may not effectively screen and support silent victims. Furthermore, current practice in Japan generally ignores treatment of perpetrators.
To address this knowledge gap, the present study aimed to explore whether patterns of IPV reports between partners were differently associated with victimization respondents’ health and psychological wellbeing.
Method
Data Source
We utilized data from the Japanese Study on Stratification, Health, Income, and Neighborhood (J-SHINE), a Japanese household panel study of randomly selected adults aged between25 and 50 years and their partners/spouses in a metropolitan area of Japan (Takada, Kondo, & Hashimoto, 2014), approved by the Data Control Committee of the J-SHINE research group for secondary data analysis use. Wave 2 followed 2,971 respondents between July and December 2012 and 1,799 of their spouses/partners in the following year in a spouse supplement survey. Both surveys used the same set of IPV question items (see below).
We excluded 161 subjects who had missing partner reports, 132 pairs with inconsistent demographic data referring to residential registry information, and 39 pairs who had not fully completed the IPV questionnaire battery. We, therefore, analyzed data for 1,467 pairs (2,934 individuals).
Measurements
IPV
The J-SHINE wave 2 and spouse survey included four subscales of the Japanese version of the Conflict Tactics Scale 2 Short Form (JCTS2SF) to measure IPV over the past 12 months; psychological aggression (minor/severe), physical assault (minor/severe), injury (minor/severe), and minor sexual coercion (Straus & Douglas, 2004; Umeda & Kawakami, 2014) with minor wording modification in some items to better reflect original meaning (Umeda, Kawakami, & Miller, 2017). In addition, two items were included in the questionnaire battery to assess social isolation (“Have you restricted your spouse/partner in contacting or meeting with his or her family or friends?”) and financial restriction (“Have you prevented your spouse/partner from knowing about or using your shared money?”).
The modified JCTS2SF in this study measures both perpetration and victimization for each of nine types of partner violence with three-level response Likert-type scales (none, once, or more than twice). As the original CTS2SF scale does not require standardized scoring, but allows flexible scoring for research purposes (Straus, 2004; Straus & Douglas, 2004), we obtained a dichotomized score by classing self-report of any type of IPV perpetration/victimization more than twice as a positive IPV case. The rationale was that IPV is a chronic phenomenon and multiple types of IPV mostly overlap (Coker, Smith, McKeown, & King, 2000; García-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006).
In this study, each respondent was counted twice, once as a victim and once as a perpetrator (and vice versa for her or his partner), as the JCTS2SF measures both types of experiences. We then classified each episode into four categories based on targeted respondents’ own reports of victimization experiences and their partners’ reports of perpetration experiences: (1) congruent report of no IPV (respondent reported no victimization and his or her partner reported no perpetration), (2) incongruent respondent victimization report (respondent reported victimization and his or her partner reported no perpetration), (3) incongruent partner perpetration report (respondent reported no victimization and his or her partner reported perpetration), and (4) congruent report of IPV (respondent reported victimization and his or her partner reported perpetration; see Table 1).
Between-Partner Matches in Reported IPV.

Note. IPV = intimate partner violence.
Health and wellbeing of respondent
We used health and wellbeing status of respondents as an outcome variable. We used the SF-8 Health Survey Questionnaire to measure physical and mental health in the past month of the survey. Following the recommended scoring algorithm, Physical Component Summary and Mental Component Summary scores were calculated (Fukuhara & Suzukamo, 2004). The Physical Component Summary and Mental Component Summary are derived from subjective evaluations of characteristics such as physical function, bodily pain, and role limitations owing to physical/mental health problems; scores are supposed to follow a normal distribution (Fukuhara & Suzukamo, 2004). To assess wellbeing status, we used a one-item questionnaire on life satisfaction (“How satisfied are you with your current life in general?”) with a five-level response Likert-type scale (satisfied, somewhat satisfied, indifferent, somewhat dissatisfied, and dissatisfied); this was based on an item from a national survey of Social Stratification and Mobility in Japan (Hara, 2011).
Demographic variables
With reference to previous studies on IPV, we included the following demographic variables of respondents as potential confounders (Capaldi, Knoble, Shortt, & Kim, 2012; Thompson et al., 2006; World Health Organization/London School of Hygiene and Tropical Medicine, 2010): gender, age, educational attainment (lower than high school, vocational school/junior college, or higher than university), annual household income (in US$1,000; less than 45, 45-67.4, 67.5-90, more than 90, or “do not know”), employment status (regular employee, non-regular employee, self-employed, or unemployed), and experience of child maltreatment under age 15 years. In addition, we included the age gap between partners (within 1 year, 2-3 years, 4-6 years, or more than 7 years) and the educational attainment gap between partners (both equal to or above university [High], both lower than university [Low], or a combination of High and Low).
Statistical analyses
First, we compared the baseline characteristics of the respondents across the four categories using the chi-squared test and/or one-way analysis of variance as appropriate. Then we compared Physical Component Summary scores, Mental Component Summary scores, and life satisfaction scores using analysis of covariance, adjusting for the confounders listed earlier. Taking into account clustering within couples which could lead to underestimation of error, we used robust error estimation to control for potential high intra-class correlations within couples.
Results
Table 2 shows the prevalence of between-partner matches in reported IPV: 22.4% of respondents were involved in IPV during the previous 12 months. Approximately 75% of the respondents who had any IPV report from the respondent and/or his or her partner had incongruent reports between the couple.
Proportion of Between-Partner Matches in Reported IPV.
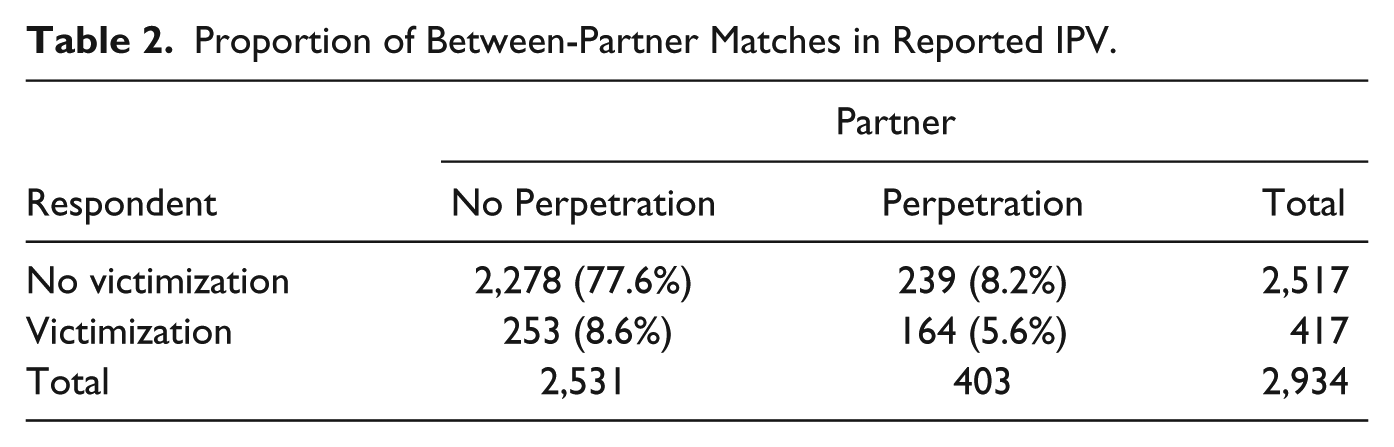
Table 3 presents demographic data for the respondents. Those who reported IPV victimization (e.g., incongruent respondent victimization + congruent IPV report) were younger and more likely to have had childhood experience of maltreatment than those who had not experienced IPV.
Baseline Characteristics of Respondents by IPV Report Category.

Note. IPV = intimate partner violence.
Chi-square test or one-way analysis of variance.
Low: lower than university, High: equal to or higher than university
Table 4 shows the analysis of covariance results, after adjusting for gender, age, educational attainment, annual household income, experience of child maltreatment, age gap between couples, and educational gap between couples, using robust error estimation. The Physical Component Summary was significantly lower in those with an incongruent victimization report (−0.96, p = .03) and with an incongruent partner perpetration report (−1.16, p = .04), compared with the reference group. The Mental Component Summary was significantly lower in those with an incongruent victimization report (−2.32, p = .00) and with a congruent report of IPV (−2.21, p = .00). The same tendency was observed for life satisfaction (incongruent respondent victimization report: −0.32, p = .00, and congruent report of IPV: −0.21, p = .01).
Analysis of Covariance Results for IPV Victims’ Physical and Mental Health.

Note. Adjusted for gender, age, educational attainment, annual household income, experience of child maltreatment, age gap between partners, and educational attainment gap between partners. Robust error estimation using couple as a cluster. IPV = intimate partner violence.
Discussion
Using household survey data from a metropolitan area of Japan, this study revealed that about one-fourth of respondents reported involvement in IPV. Those who reported victimization were younger and more likely to have experience of child maltreatment, which is consistent with previous findings (Capaldi et al., 2012; Thompson et al., 2006). Approximately 75% of those who had any IPV report from the respondent and/or his or her partner had reports that were incongruent with their partners’ reports, a figure compatible with previous findings showing low to moderate kappa coefficients between partner IPV reports (Caetano et al., 2009; Schafer et al., 1998).
A negative and significant association between reporting victimization and poorer mental health and life satisfaction was observed regardless of the perpetration status of partners. Previous reports have also reported a negative association between IPV victimization and mental health (Campbell, 2002; Ellsberg et al., 2008); however, these studies examined victimization reports but did not obtain information about partners’ perpetration status. The results of this study indicate that victims who recognized their victimization experienced impaired mental health and wellbeing although their partners reported no violence. An individual’s recognition of his or her victimized status leads to psychological stress, which may be mediated by lower self-esteem (Bradley, Schwartz, & Kaslow, 2005) or by self-stigma, in which victims stigmatize themselves as IPV victims and internalize negative beliefs about the self (Overstreet & Quinn, 2013).
Respondents with no victimization report and an incongruent partner perpetration report maintained their mental health and life satisfaction. This may be a result of psychological defense mechanisms: a psychological process by which cognitive disharmony is relieved by reconstructing the perception of events in response to perceived threats, which subsequently leads to recovery of psychological equilibrium and maintenance of self-esteem (Cramer, 1987, 2000; Vaillant, 1994). Some researchers have suggested that higher self-esteem is associated with greater life satisfaction (Hong & Giannakopoulos, 1994) and that individuals with greater defense mechanisms have better health outcomes (Dollinger & Cramer, 2007). Another possible explanation is that respondents with incongruent partner perpetration reports recognized their partner’s perpetration as part of social interaction to maintain intimate partnership and their sociopsychological identity through the relationship (Henderson et al., 1997; Henderson et al., 2005). In such cases, a psychological defense mechanism could act to maintain mental health at the cost of physical health.
Poorer physical health was associated with between-partner mismatched IPV reports. In such cases, respondents may have difficulties in negotiating with their partners about IPV because of the contradictory recognition of IPV. Shared problem recognition is an important skill for resolving marital conflict (Scanzoni & Polonko, 1980). By losing the opportunity to negotiate, violence may continue and a respondent may fail to seek effective countermeasures to protect herself or himself, resulting in poorer physical health.
Several limitations of the study should be acknowledged. First, the sample was obtained from a metropolitan area of Japan, and the generalizability of the results needs confirmation by future studies in settings characterized by different sociocultural and gender norms, especially in low- to middle-income countries where IPV against women poses a serious social threat. Second, the limited number and range of items on the CTS2SF and JCTS2SF cannot cover the full range of IPV, as discussed previously (Follingstad & Rogers, 2013; Straus & Douglas, 2004). Thus, a more sophisticated IPV measure is needed to fully capture IPV. Third, IPV prevalence is likely to be underreported (Hamby, 2005; Sugarman & Hotaling, 1997), which possibly affected the observed frequency of IPV in this study. The prevalence of IPV in this study was similar to that of previous Japanese surveys (Gender Equality Division, Department of Citizens’ Affairs, Saitama Prefecture, Japan, 2015; Japanese Cabinet Office, 2002, 2014). However, if both partners underreport perpetration and victimization, their accounts might be misclassified as a congruent report of no IPV, which would result in a biased estimation toward the null. Thus, the non-significant findings in this study may reflect type II error. Fourth, we set an arbitrary cutoff point for the IPV dichotomy, which may have affected the results. When we took any one positive response on the JCTS2SF as a positive IPV case, the Physical Component Summary score of those with their own incongruent victimization report remained negative but became non-significant. However, the other results were robust despite changing the threshold. Finally, the cross-sectional design of the current study precludes causal inferences about possible mechanisms linking report patterns and health outcomes. Additional studies are needed using repeated measures data.
Despite the limitations, this study has some strengths. First, it was a unique population-based, large-scale survey that used paired IPV data. In Japan’s paternalistic society, IPV is traditionally regarded as male-to-female violence (Yoshihama, 2002). However, the prevalence of IPV in this study was neither gender-specific nor unilateral and reflected IPV patterns found in previous studies worldwide (Archer, 2000; Johnson, 1995; McHugh & Frieze, 2006; Straus, 2011). Second, to the best of our knowledge, this is the first study to analyze the association between patterns of couple reports on IPV and their health impact. Third, the finding that victims who do not report their victimization experience have poorer physical health was notable, because the health of silent victims is not usually examined.
The implication for public health practices is that attention should be paid not only to those who report victimization but also to victims who do not speak out. Given the non-ignorable prevalence of IPV, physical health damage relative to reasonable mental health should be taken as a potential message to screen hidden/unrecognized IPV. Another implication for public service providers is that IPV should be recognized as a phenomenon that is constructed through the interaction between partners, rather than simply as either the occurrence/non-occurrence of violence. Current practice in Japan focuses on victims whose reported IPV matches perpetration reports; isolated victimization reports are taken less seriously and are often assumed to represent over-reporting, which leaves victims at risk of both IPV and stigmatization. Those reporting IPV victimization should be supported regardless of the presence of a congruent partner report. In addition, physical problems in the absence of an IPV report can be a sign of an intimate partnership mediated by violence and a cue to screen for underreported IPV, which may enable practitioners and clinicians to identify and treat perpetrators. Public service professionals such as hospital staff, police, and law officials should be aware of the risk of harm to the victim’s health if they only focus on objectively judging and labeling perpetrator/victim statuses, without considering how social interaction between partners is created, maintained, and recognized as inter-personal violence.
Footnotes
Acknowledgments
The authors thank the J-SHINE Data Management Committee for their dedication to collecting and managing the data attentively, and their tolerance regarding data disclosure.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by Health and Labor Sciences Research Grants from the Ministry of Health, Labor and Welfare (Lifestyle disease research; H27-general-002).